
Adverse Reactions after Booster SARS-CoV-2 Vaccination Have Less Impact on Antibody Response than after Basic Vaccination Scheme

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. SARS-CoV-2 Antibody Measurements
2.3. Ethics Statement
2.4. Statistical Analysis
3. Results
3.1. Participants Characteristics
3.2. Frequency of Adverse Reactions after 1st, 2nd and 3rd Dose of Vaccination
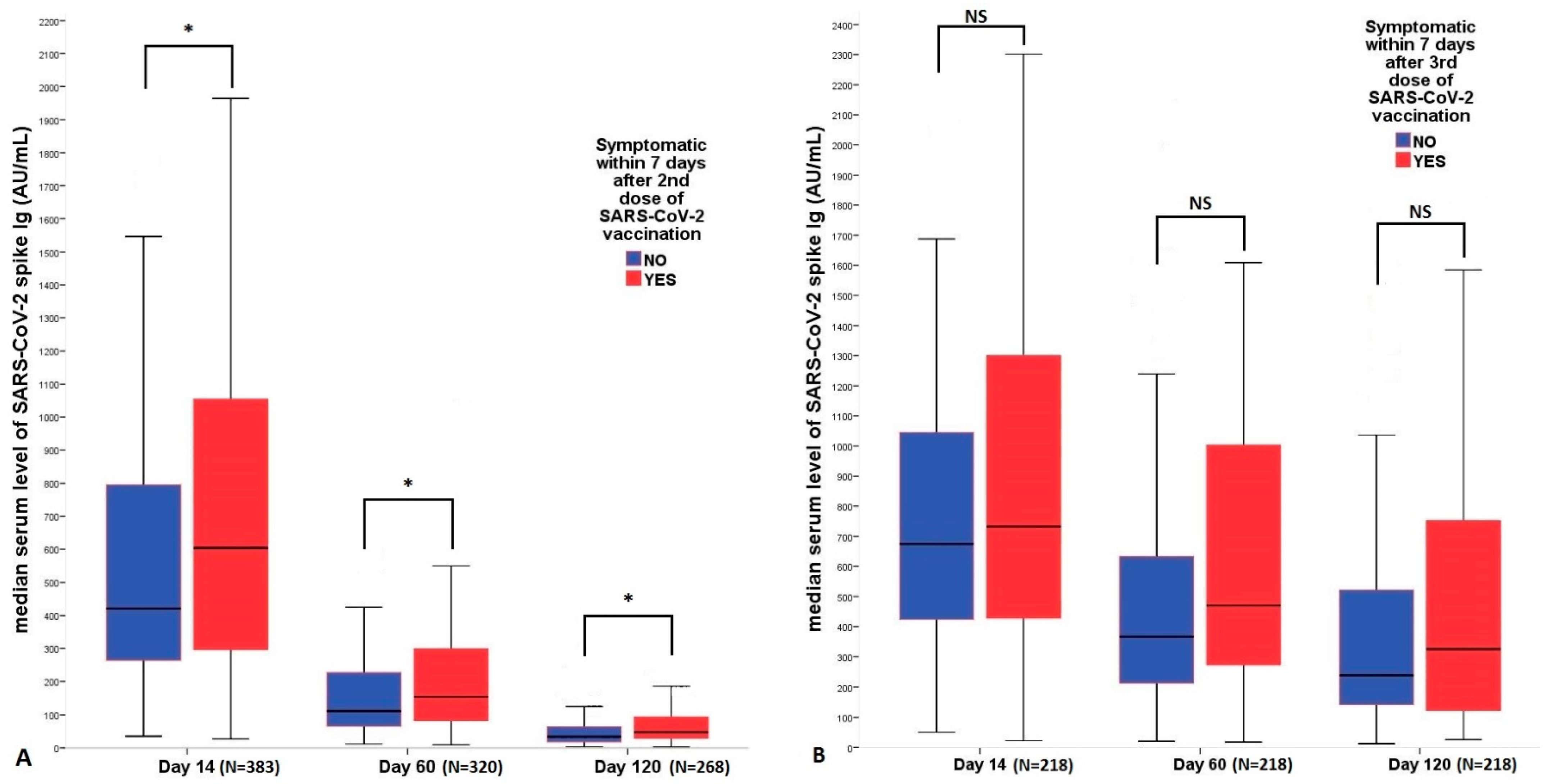
3.3. Correlation of Antibody Titers with Adverse Reactions after the 2nd and 3rd Vaccinations
3.4. Factors Related to SARS-CoV-2 Positivity after the 3rd Vaccination
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Dighriri, I.M.; Alhusayni, K.M.; Mobarki, A.Y.; Aljerary, I.S.; Alqurashi, K.A.; Aljuaid, F.A.; Alamri, K.A.; Mutwalli, A.A.; Maashi, N.A.; Aljohani, A.M.; et al. Pfizer-BioNTech COVID-19 Vaccine (BNT162b2) Side Effects: A Systematic Review. Cureus 2022, 14, e23526. [Google Scholar] [CrossRef]
- Menni, C.; May, A.; Polidori, L.; Louca, P.; Wolf, J.; Capdevila, J.; Hu, C.; Ourselin, S.; Steves, C.J.; Valdes, A.M.; et al. COVID-19 vaccine waning and effectiveness and side-effects of boosters: A prospective community study from the ZOE COVID Study. Lancet Infect. Dis. 2022, 22, 1002–1010. [Google Scholar] [CrossRef]
- Kanizsai, A.; Molnar, T.; Varnai, R.; Zavori, L.; Tőkés-Füzesi, M.; Szalai, Z.; Berecz, J.; Csecsei, P. Fever after Vaccination against SARS-CoV-2 with mRNA-Based Vaccine Associated with Higher Antibody Levels during 6 Months Follow-Up. Vaccines 2022, 10, 447. [Google Scholar] [CrossRef]
- Levy, I.; Levin, E.G.; Olmer, L.; Regev-Yochay, G.; Agmon-Levin, N.; Wieder-Finesod, A.; Indenbaum, V.; Herzog, K.; Doolman, R.; Asraf, K.; et al. Correlation between Adverse Events and Antibody Titers among Healthcare Workers Vaccinated with BNT162b2 mRNA COVID-19 Vaccine. Vaccines 2022, 10, 1220. [Google Scholar] [CrossRef]
- Koike, R.; Sawahata, M.; Nakamura, Y.; Nomura, Y.; Katsube, O.; Hagiwara, K.; Niho, S.; Masuda, N.; Tanaka, T.; Sugiyama, K. Systemic Adverse Effects Induced by the BNT162b2 Vaccine Are Associated with Higher Antibody Titers from 3 to 6 Months after Vaccination. Vaccines 2022, 10, 451. [Google Scholar] [CrossRef]
- Wise, J. COVID-19: People who have had infection might only need one dose of mRNA vaccine. BMJ (Clin. Res. Ed.) 2021, 372, n308. [Google Scholar] [CrossRef]
- Krammer, F.; Srivastava, K.; Simon, V. Robust spike antibody responses and increased reactogenicity in seropositive individuals after a single dose of SARS-CoV-2 mRNA vaccine. medRxiv 2021. [Google Scholar] [CrossRef]
- Manisty, C.; Otter, A.D.; Treibel, T.A.; McKnight, Á.; Altmann, D.M.; Brooks, T.; Noursadeghi, M.; Boyton, R.J.; Semper, A.; Moon, J.C. Antibody response to first BNT162b2 dose in previously SARS-CoV-2-infected individuals. Lancet 2021, 397, 1057–1058. [Google Scholar] [CrossRef]
- Chu, L.; Vrbicky, K.; Montefiori, D.; Huang, W.; Nestorova, B.; Chang, Y.; Carfi, A.; Edwards, D.K.; Oestreicher, J.; Legault, H.; et al. Immune response to SARS-CoV-2 after a booster of mRNA-1273: An open-label phase 2 trial. Nat. Med. 2022, 28, 1042–1049. [Google Scholar] [CrossRef]
- Mise-Omata, S.; Ikeda, M.; Takeshita, M.; Uwamino, Y.; Wakui, M.; Arai, T.; Yoshifuji, A.; Murano, K.; Siomi, H.; Nakagawara; et al. Memory B Cells and Memory T Cells Induced by SARS-CoV-2 Booster Vaccination or Infection Show Different Dynamics and Responsiveness to the Omicron Variant. J. Immunol. 2022, 209, 2104–2113. [Google Scholar] [CrossRef]
- Goel, R.R.; Painter, M.M.; Apostolidis, S.A.; Mathew, D.; Meng, W.; Rosenfeld, A.M.; Lundgreen, K.A.; Reynaldi, A.; Khoury, D.S.; Pattekar, A.; et al. mRNA vaccines induce durable immune memory to SARS-CoV-2 and variants of concern. Science 2021, 374, abm0829. [Google Scholar] [CrossRef]
- Gaebler, C.; Wang, Z.; Lorenzi, J.C.C.; Muecksch, F.; Finkin, S.; Tokuyama, M.; Cho, A.; Jankovic, M.; Schaefer-Babajew, D.; Oliveira, T.Y.; et al. Evolution of antibody immunity to SARS-CoV-2. Nature 2021, 591, 639–644. [Google Scholar] [CrossRef]
- Jara, A.; Undurraga, E.A.; Zubizarreta, J.R.; González, C.; Pizarro, A.; Acevedo, J.; Leo, K.; Paredes, F.; Bralic, T.; Vergara, V.; et al. Effectiveness of homologous and heterologous booster doses for an inactivated SARS-CoV-2 vaccine: A large-scale prospective cohort study. Lancet. Glob. Health 2022, 10, e798–e806. [Google Scholar] [CrossRef]
- Atmar, R.L.; Lyke, K.E.; Deming, M.E.; Jackson, L.A.; Branche, A.R.; El Sahly, H.M.; Rostad, C.A.; Martin, J.M.; Johnston, C.; Rupp, R.E.; et al. Homologous and Heterologous Covid-19 Booster Vaccinations. N. Engl. J. Med. 2022, 386, 1046–1057. [Google Scholar] [CrossRef]
- El Yousfi, M.; Mercier, S.; Breuillé, D.; Denis, P.; Papet, I.; Mirand, P.P.; Obled, C. The inflammatory response to vaccination is altered in the elderly. Mech. Ageing Dev. 2005, 126, 874–881. [Google Scholar] [CrossRef]
- Hervé, C.; Laupèze, B.; Del Giudice, G.; Didierlaurent, A.M.; Tavares Da Silva, F. The how’s and what’s of vaccine reactogenicity. NPJ Vaccines 2019, 4, 39. [Google Scholar] [CrossRef] [Green Version]
- Powell, A.A.; Power, L.; Westrop, S.; McOwat, K.; Campbell, H.; Simmons, R.; Ramsay, M.E.; Brown, K.; Ladhani, S. Real-world data shows increased reactogenicity in adults after heterologous compared to homologous prime-boost COVID-19 vaccination, March-June 2021, England. Eur. Commun. Dis. Bull. 2021, 26, 2100634. [Google Scholar] [CrossRef]
- Warkentin, L.; Zeschick, N.; Kühlein, T.; Steininger, P.; Überla, K.; Kaiser, I.; Gall, C.; Sebastião, M.; Hueber, S. Reactogenicity after heterologous and homologous COVID-19 prime-boost vaccination regimens: Descriptive interim results of a comparative observational cohort study. BMC Infect. Dis. 2022, 22, 504. [Google Scholar] [CrossRef]
- Schmidt, T.; Klemis, V.; Schub, D.; Mihm, J.; Hielscher, F.; Marx, S.; Abu-Omar, A.; Ziegler, L.; Guckelmus, C.; Urschel, R.; et al. Immunogenicity and reactogenicity of heterologous ChAdOx1 nCoV-19/mRNA vaccination. Nat. Med. 2021, 27, 1530–1535. [Google Scholar] [CrossRef]
- Wu, K.; Yang, S.; Li, X.; Xia, B.; Ma, S.; Chen, X. MA09.03 Peripheral CD8+ T Cells Predicts Immune-Related Adverse Events and Survival in Advanced Non-Small Cell Lung Cancer Treated With Immunotherapy. J. Thorac. Oncol. 2021, 16, S911–S912. [Google Scholar] [CrossRef]
- Klingel, H.; Lauen, M.; Krüttgen, A.; Imöhl, M.; Kleines, M. Severity of adverse reactions is associated with T-cell response in mRNA-1273 vaccinated health care workers. Clin. Exp. Vaccine Res. 2022, 11, 121–124. [Google Scholar] [CrossRef]
- Stosic, M.; Milic, M.; Markovic, M.; Kelic, I.; Bukumiric, Z.; Veljkovic, M.; Kisic Tepavcevic, D.; Saponjic, V.; Plavsa, D.; Jovanovic, S. Immunogenicity and Reactogenicity of the Booster Dose of COVID-19 Vaccines and Related Factors: A Panel Study from the General Population in Serbia. Vaccines 2022, 10, 838. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Asymptomatic (N = 141) | Symptomatic (N = 77) | p-Value | |
|---|---|---|---|
| Age, (mean ± SD) | 49.6 ± 11 | 44 ± 11 | 0.001 |
| Female, (N, %) | 116 (82%) | 57 (74%) | 0.151 |
| BMI, (mean ± SD) | 28 ± 7 | 27 ± 5 | 0.474 |
| Smoking, (N, %) | 45 (33%) | 23 (32%) | 0.947 |
| Time lag between 2nd and 3rd vaccine dose, days, (mean ± SD) | 250 ± 45 | 247 ± 41 | 0.827 |
| Pfizer BioNTech vaccine, 3rd dose, (N, %) | 136 (97%) | 65 (84%) | 0.002 |
| Hypertension, (N, %) | 40 (29%) | 17 (23%) | 0.359 |
| Diabetes, type II, (N,%) | 10 (7%) | 5 (7%) | 0.904 |
| Allergy, (N, %) | 32 (23%) | 28 (38%) | 0.022 |
| Autoimmune disease, (N, %) | 10 (7%) | 3 (4%) | 0.361 |
| Symptomatic after 1st dose, (N, %) | 43 (31%) | 43 (56%) | <0.001 |
| Symptomatic after 2nd dose, (N, %) | 40 (28%) | 45 (58%) | <0.001 |
| SARS-CoV-2 positivity before 3rd dose, (N, %) | 45 (32%) | 17 (22%) | 0.124 |
| SARS-CoV-2 positivity after 3rd dose, (N, %) | 31 (22%) | 23 (30%) | 0.197 |
| Fever | Minimum | 25% | Median | 75% | Maximum | p-Value |
|---|---|---|---|---|---|---|
| After 2nd dose | ||||||
| Day 14 (N = 383) | ||||||
| + (N = 56) | 266 | 689 | 986 | 1402 | 7785 | <0.001 |
| − (N = 327) | 27 | 262 | 442 | 810 | 655 | |
| Day 60 (N = 320) | ||||||
| + (N = 49) | 96 | 164 | 274 | 457 | 998 | <0.001 |
| − (N = 271) | 9 | 70 | 123 | 237 | 655 | |
| Day 120 (N = 268) | ||||||
| + (N = 45) | 28 | 49 | 76 | 148 | 251 | <0.001 |
| − (N = 223) | 2 | 19 | 36 | 68 | 379 | |
| After 3rd dose | ||||||
| Day 14 (N = 218) | ||||||
| + (N = 41) | 47 | 388 | 955 | 1570 | 3209 | 0.045 |
| − (N = 177) | 22 | 425 | 663 | 1014 | 5948 | |
| Day 60 (N = 218) | ||||||
| + (N = 41) | 107 | 331 | 790 | 1190 | 4117 | 0.002 |
| − (N = 177) | 17 | 208 | 379 | 670 | 7101 | |
| Day 120 (N = 218) | ||||||
| + (N = 41) | 56 | 260 | 494 | 815 | 3005 | 0.014 |
| − (N = 177) | 12 | 124 | 240 | 541 | 2706 |
| Variable | Day 0 S-IgG | Day 14 S-IgG | Day 60 S-IgG | Day 120 S-IgG |
|---|---|---|---|---|
| Age | −0.190 ** | −0.030 | −0.028 | −0.089 |
| Smoking | −0.163 * | −0.050 | −0.128 | −0.080 |
| Gender | 0.013 | 0.158 * | 0.134 * | 0.149 * |
| mRNS type vaccine | −0.149 * | −0.317 ** | −0.032 | 0.031 |
| COVID+ before 1st dose | 0.293 ** | 0.004 | −0.024 | −0.042 |
| COVID+between 2nd and 3rd dose | 0.144 * | 0.174 * | 0.204 ** | 0.116 |
| NSAID | −0.163 * | −0.140 * | −0.115 | −0.145 * |
| Hyperlipidaemia | −0.138 * | −0.166 * | −0.157 * | −0.082 |
| Chills after 2nd dose | 0.209 ** | 0.189 ** | 0.138 | 0.091 |
| Fever after 2nd dose | 0.281 ** | 0.261 ** | 0.226 ** | 0.172 ** |
| Chills after 3rd dose | N/A | 0.138 * | 0.203 ** | 0.143 |
| Fever after 3rd dose | N/A | 0.145 * | 0.262 ** | 0.189 ** |
| Use of beta blocker | −0.169 * | −0.054 | −0.123 | −0.019 |
| Time lag between 2nd and 3rd dose | −0.097 | 0.012 | 0.118 | 0.216 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kanizsai, A.; Zavori, L.; Molnar, T.; Tőkés-Füzesi, M.; Szalai, Z.; Berecz, J.; Varnai, R.; Peterfi, Z.; Schwarcz, A.; Csecsei, P. Adverse Reactions after Booster SARS-CoV-2 Vaccination Have Less Impact on Antibody Response than after Basic Vaccination Scheme. Vaccines 2023, 11, 182. https://doi.org/10.3390/vaccines11010182
Kanizsai A, Zavori L, Molnar T, Tőkés-Füzesi M, Szalai Z, Berecz J, Varnai R, Peterfi Z, Schwarcz A, Csecsei P. Adverse Reactions after Booster SARS-CoV-2 Vaccination Have Less Impact on Antibody Response than after Basic Vaccination Scheme. Vaccines. 2023; 11(1):182. https://doi.org/10.3390/vaccines11010182
Chicago/Turabian StyleKanizsai, Andrea, Laszlo Zavori, Tihamer Molnar, Margit Tőkés-Füzesi, Zoltan Szalai, Janos Berecz, Reka Varnai, Zoltan Peterfi, Attila Schwarcz, and Peter Csecsei. 2023. "Adverse Reactions after Booster SARS-CoV-2 Vaccination Have Less Impact on Antibody Response than after Basic Vaccination Scheme" Vaccines 11, no. 1: 182. https://doi.org/10.3390/vaccines11010182