
Perceptions of COVID-19 Vaccine, Racism, and Social Vulnerability: An Examination among East Asian Americans, Southeast Asian Americans, South Asian Americans, and Others

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Participants and Procedures
2.3. Measures
2.4. Analyses
3. Results
3.1. Descriptive Statistics
3.2. Racial/Ethnic Differences Regarding Racism
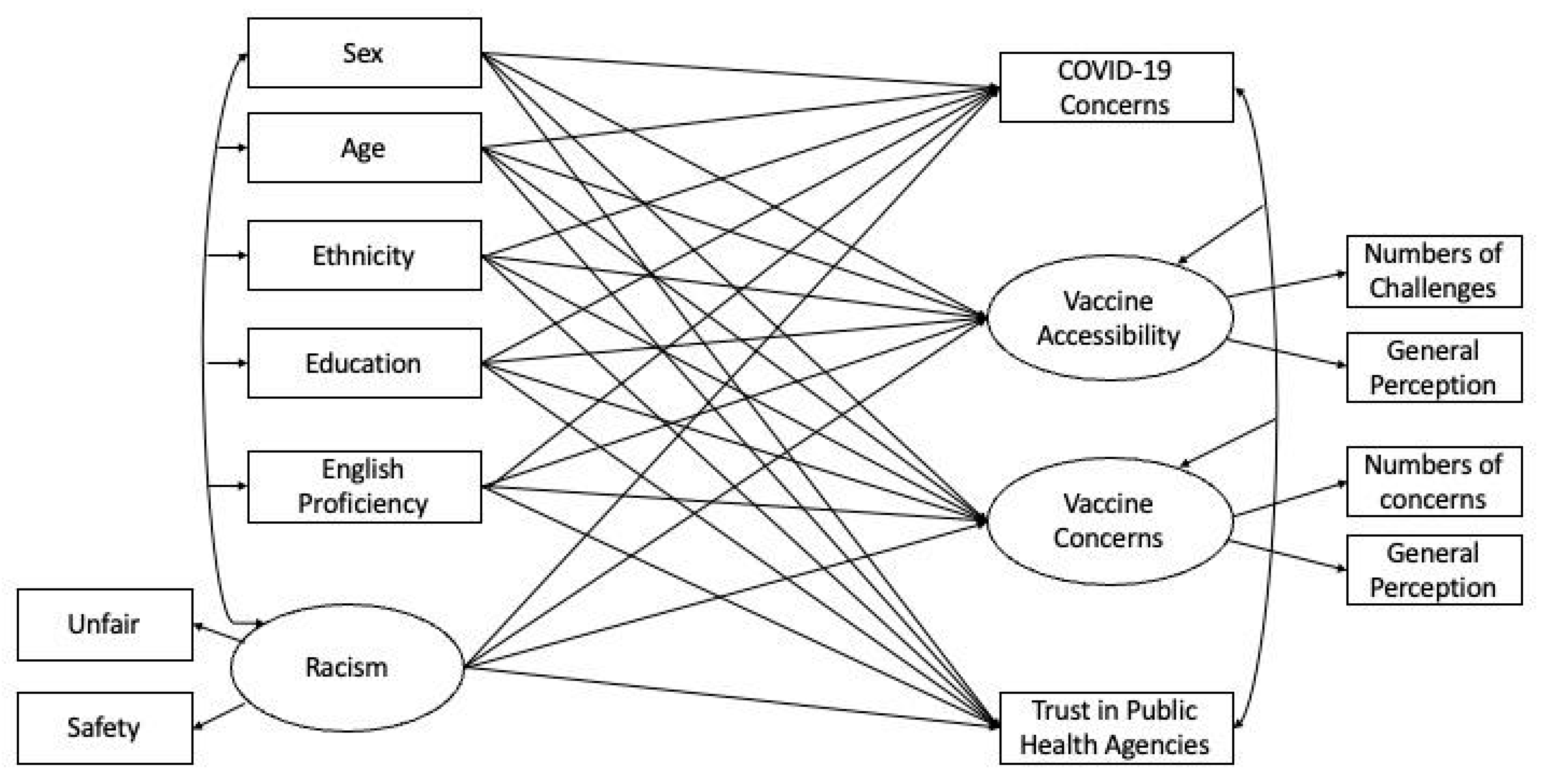
3.3. Predicting COVID-19-Related Concerns with Mediation Effects
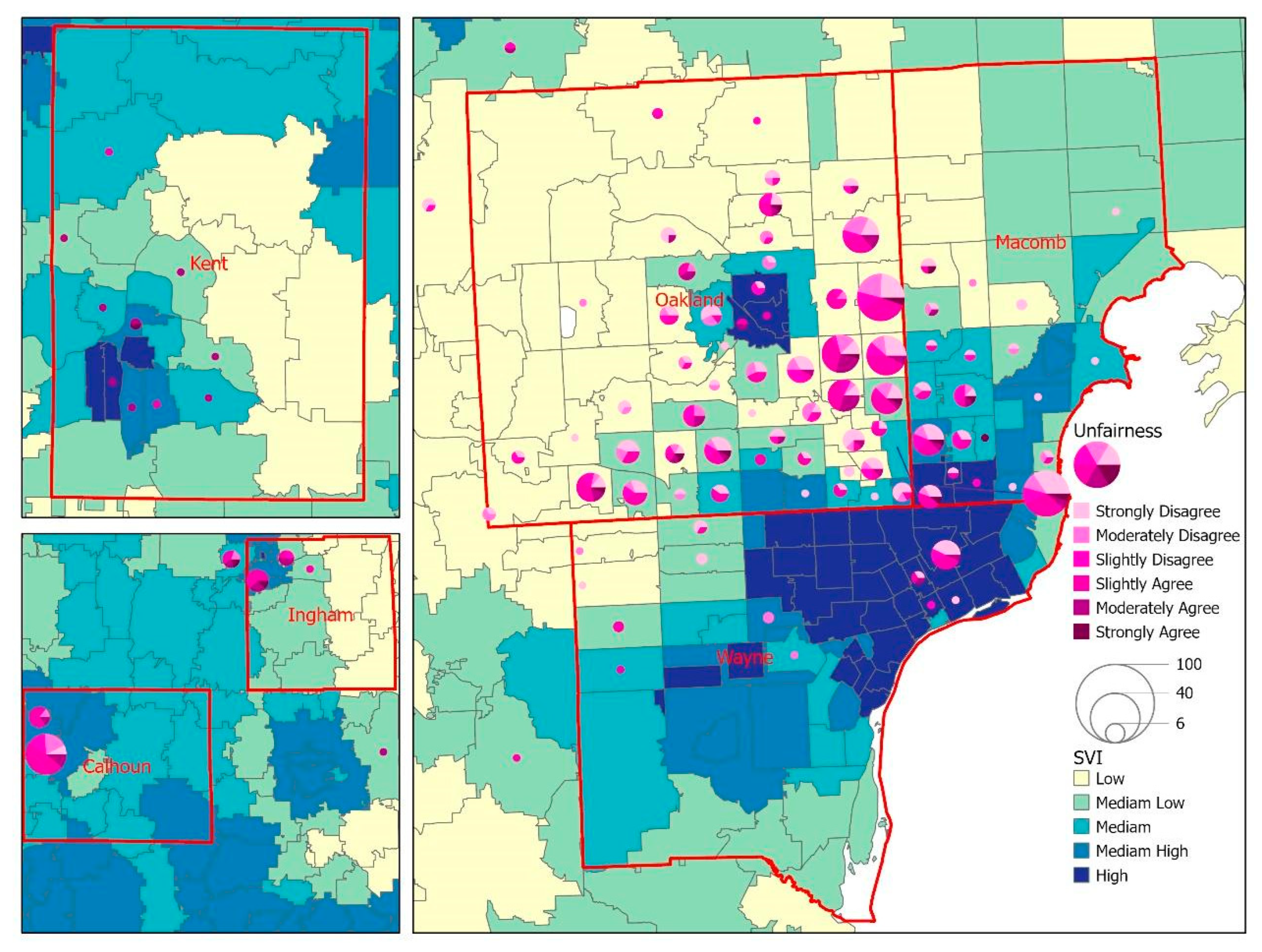
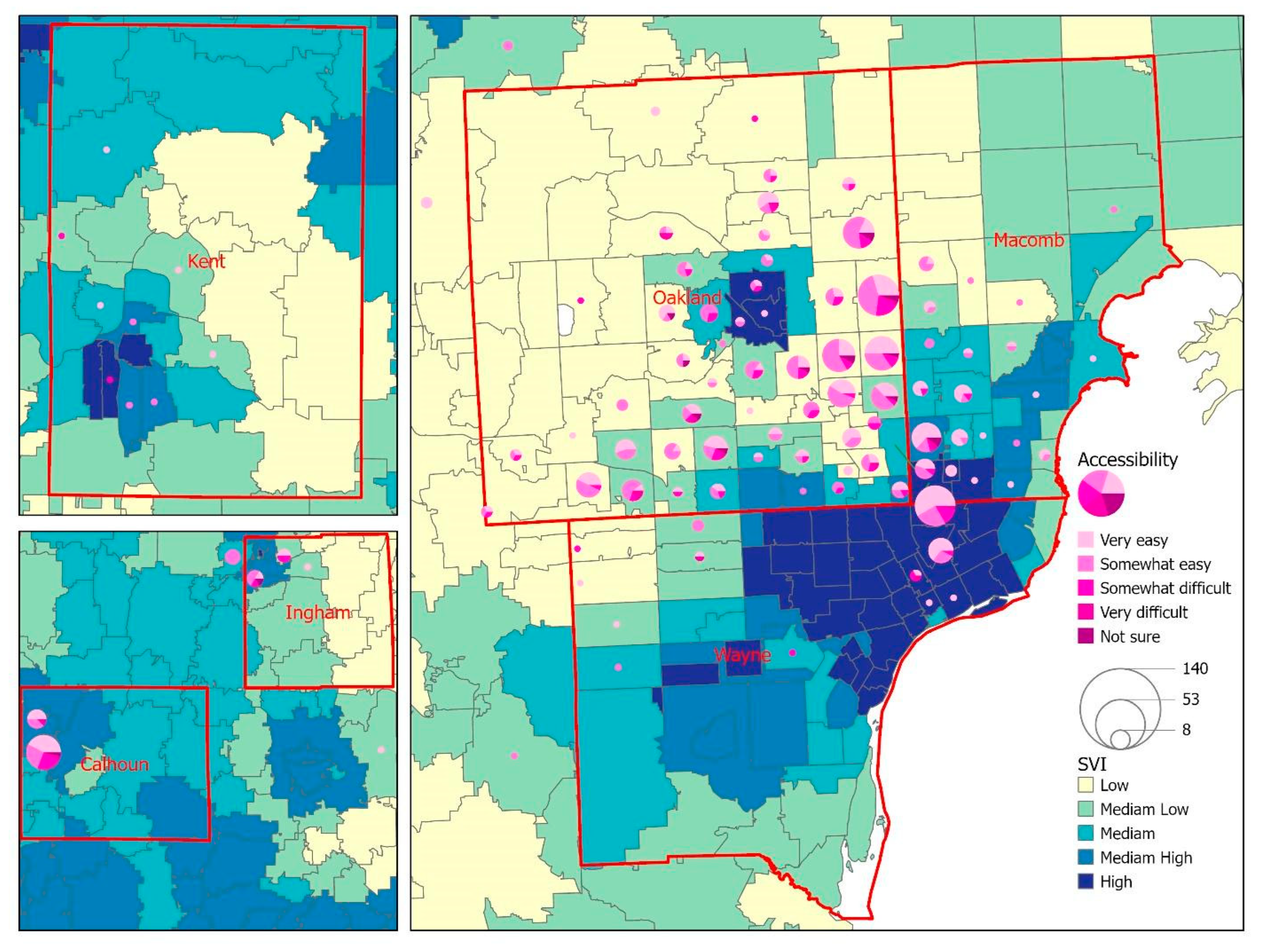
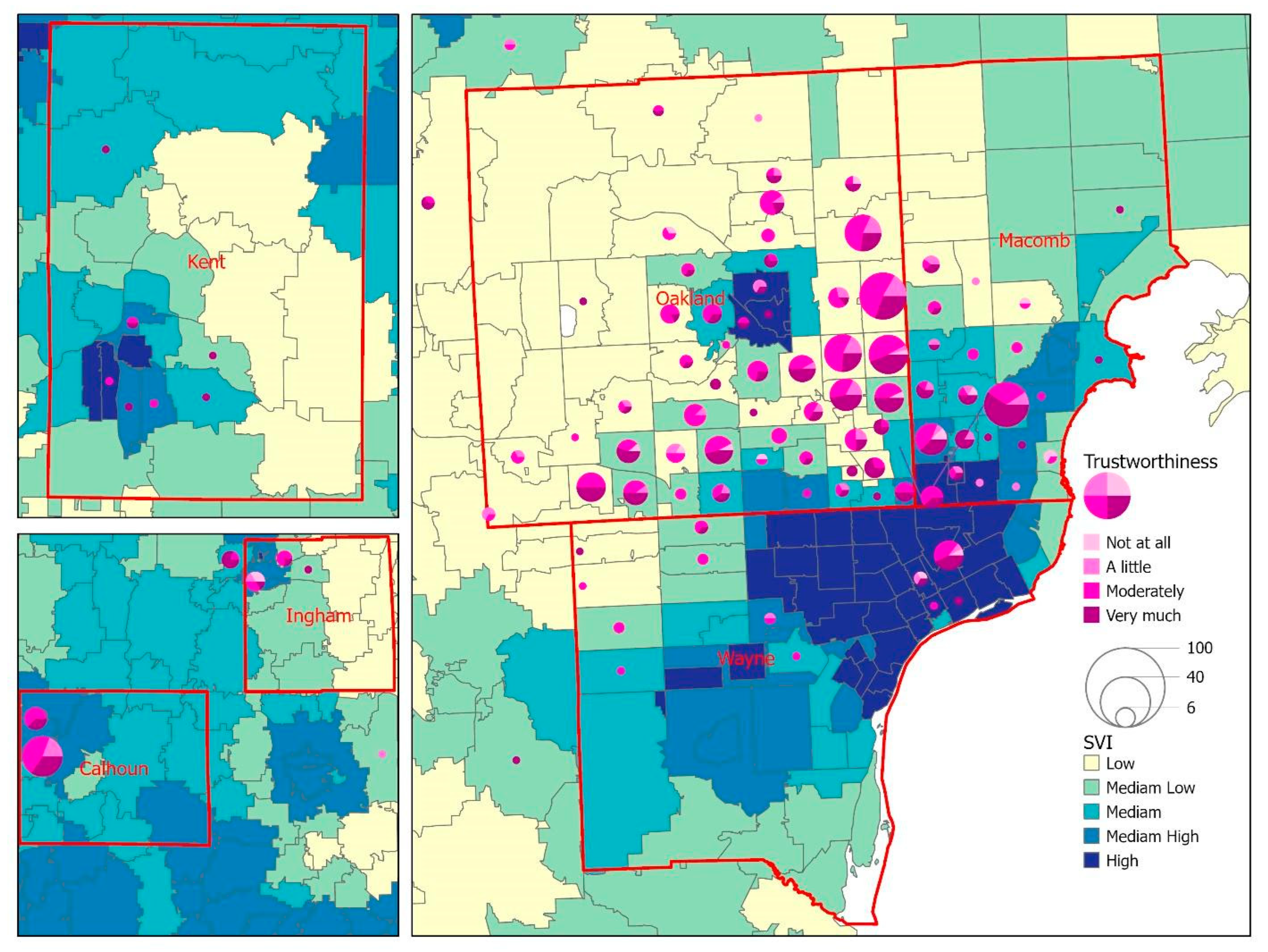
3.4. Social Vulnerability Index and COVID-19 Concerns
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- USAFacts. US Coronavirus Vaccine Tracker. Available online: https://usafacts.org/visualizations/covid-vaccine-tracker-states/?utm_source=usnews&utm_medium=partnership&utm_campaign=fellowship&utm_content=Link (accessed on 8 June 2022).
- Centers for Disease Control and Prevention (CDC). COVID Data Tracker. 2022. Available online: https://covid.cdc.gov/covid-data-tracker/#vaccinations_vacc-people-additional-dose-totalpop (accessed on 6 July 2022).
- Salmon, D.A.; Dudley, M.Z.; Glanz, J.M.; Omer, S.B. Vaccine Hesitancy: Causes, Consequences, and a Call to Action. Am. J. Prev. Med. 2015, 49, S391–S398. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.H.; Shiu, C.S. Race, Ethnicity and COVID-19 Vaccine Concerns: A Latent Class Analysis of Data during Early Phase of Vaccination. SSM-Popul. Health 2022, 18, 101073. [Google Scholar] [CrossRef] [PubMed]
- Bagasra, A.B.; Doan, S.; Allen, C.T. Racial Differences in Institutional Trust and COVID-19 Vaccine Hesitancy and Refusal. BMC Public Health 2021, 21, 2104. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health & Human Services Office of Minority Health. Profile: Asian Americans. 2021. Available online: https://minorityhealth.hhs.gov/omh/browse.aspx?lvl=3&lvlid=63 (accessed on 9 July 2022).
- Pew Research Center. Key Facts about Asian Americans, a Diverse and Growing Population. 2021. Available online: https://www.pewresearch.org/fact-tank/2021/04/29/key-facts-about-asian-americans/ (accessed on 18 May 2022).
- Fridman, A.; Gershon, R.; Gneezy, A. COVID-19 and Vaccine Hesitancy: A Longitudinal Study. PLoS ONE 2021, 16, e0250123. [Google Scholar] [CrossRef] [PubMed]
- Viswanath, K.; Bekalu, M.; Dhawan, D.; Pinnamaneni, R.; Lang, J.; McLoud, R. Individual and Social Determinants of COVID-19 Vaccine Uptake. BMC Public Health 2021, 21, 818. [Google Scholar] [CrossRef] [PubMed]
- Elhadi, M.; Alsoufi, A.; Alhadi, A.; Hmeida, A.; Alshareea, E.; Dokali, M.; Abodabos, S.; Alsadiq, O.; Abdelkabir, M.; Ashini, A.; et al. Knowledge, Attitude, and Acceptance of Healthcare Workers and the Public Regarding the COVID-19 Vaccine: A Cross-sectional Study. BMC Public Health 2021, 21, 955. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.L.; Wileden, L.; Shanks, T.R.; Goold, S.D.; Morenoff, J.D.; Gorin, S.N.S. Mediators of Racial Differences in COVID-19 Vaccine Acceptance and Uptake: A Cohort Study in Detroit, MI. Vaccines 2022, 10, 36. [Google Scholar] [CrossRef] [PubMed]
- Jethwa, H.; Wong, R.; Abraham, S. COVID-19 Vaccine Trials: Ethnic Diversity and Immunogenicity. Vaccine 2021, 39, 3541–3543. [Google Scholar] [CrossRef] [PubMed]
- Pepperrell, T.; Rodgers, F.; Tandon, P.; Sarsfield, K.; Pugh-Jones, M.; Rashid, T.; Keestra, S. Making a COVID-19 Vaccine that Works for Everyone: Ensuring Equity and Inclusivity in Clinical Trials. Glob. Health Action 2021, 14, 1892309. [Google Scholar] [CrossRef] [PubMed]
- Latkin, C.A.; Dayton, L.; Yi, G.; Konstantopoulos, A.; Boodram, B. Trust in a COVID-19 Vaccine in the U.S.: A Social-ecological Perspective. Soc. Sci. Med. 2021, 270, 113684. [Google Scholar] [CrossRef] [PubMed]
- Park, V.M.T.; Dougan, M.; Meyer, O.L.; Nam, B.; Tzuang, M.; Park, L.G.; Vuong, Q.; Tsoh, J.Y. Vaccine Willingness: Findings from the COVID-19 Effects on the Mental and Physical Health of Asian Americans & Pacific Islanders Survey Study (COMPASS). Prev. Med. Rep. 2021, 23, 101480. [Google Scholar] [CrossRef]
- Napoles, A.M.; Stewart, A.L.; Strassle, P.D.; Quintero, S.; Bonilla, J.; Alhomsi, A.; Santana-Ufret, V.; Maldonado, A.I.; Perez-Stable, E.J. Racial/ethnic Disparities in Intent to Obtain a COVID-19 Vaccine: A Nationally Representative United States Survey. Prev. Med. Rep. 2021, 24, 101653. [Google Scholar] [CrossRef] [PubMed]
- Jacobi, C.J.; Vaidyanathan, B. Racial Differences in Anticipated COVID-19 Vaccine Acceptance Among Religious Populations in the US. Vaccine 2021, 39, 6351–6355. [Google Scholar] [CrossRef] [PubMed]
- Misra, S.; Le, P.D.; Goldmann, E.; Yang, L.H. Psychological Impact of Anti-Asian Stigma due to the COVID-19 Pandemic: A Call for Research, Practice, and Policy Responses. Psychol. Trauma 2020, 12, 461–464. [Google Scholar] [CrossRef] [PubMed]
- Park, V.M.T.; Dougan, M.; Meyer, O.L.; Nam, B.; Tzuang, M.; Park, L.G.; Vuong, Q.; Tsoh, J. Differences in COVID-19 Vaccine Concerns Among Asian Americans and Pacific Islanders: The COMPASS Survey. J. Racial Ethn. Health Disparit. 2021, 9, 979–991. [Google Scholar] [CrossRef] [PubMed]
- Agency for Toxic Substances and Disease Registry. At A Glance: CDC/ATSDR Social Vulnerability Index. 2021. Available online: https://www.atsdr.cdc.gov/placeandhealth/svi/at-a-glance_svi.html (accessed on 3 August 2022).
- Agency for Toxic Substances and Disease Registry. CDC/ATSDR Social Vulnerability Index. 2022. Available online: https://www.atsdr.cdc.gov/placeandhealth/svi/index.html (accessed on 3 August 2022).
- US Census Bureau. 2018 American Community Survey 1-Year Estimates. 2019. Available online: https://www.census.gov/newsroom/press-kits/2019/acs-1year.html (accessed on 16 May 2022).
- US Census Bureau. 2019 American Community Survey 1-Year Estimates. 2020. Available online: https://www2.census.gov/about/training-workshops/2020/2020-09-10-acs-presentation.pdf (accessed on 16 May 2022).
- US Census Bureau. 2014 American Community Survey 1-Year Estimates. 2015. Available online: https://www.census.gov/newsroom/press-kits/2015/acs_oneyear.html (accessed on 16 May 2022).
- Centers for Disease Control and Prevention (CDC). How to Conduct a Rapid Community Assessment. 2022. Available online: https://www.cdc.gov/vaccines/covid-19/vaccinate-with-confidence/rca-guide/index.html (accessed on 21 June 2022).
- Gonzalez, D.; Kenney, G.M.; McDaniel, M.; Skopec, L. Perceptions of Unfair Treatment or Judgment Due to Race or Ethnicity in Five Settings. 2021. Available online: https://www.urban.org/sites/default/files/publication/104565/perceptions-of-unfair-treatment-or-judgment-due-to-race-or-ethnicity-in-five-settings_0.pdf (accessed on 9 August 2022).
- SMARTLING. What Is Back Translation and Why Is It Important? Available online: https://www.smartling.com/resources/101/what-is-back-translation-and-why-is-it-important/ (accessed on 9 July 2022).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022; Available online: https://www.r-project.org/ (accessed on 8 June 2022).
- Hu, L.T.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria Versus New Alternatives. Struc. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Karras, D.J. Statistical Methodology: II. Reliability and Variability Assessment in Study Design, Part A. Acad. Emerg. Med. 1997, 4, 64–71. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). CDC/ATSDR Social Vulnerability Index. Available online: https://www.atsdr.cdc.gov/placeandhealth/svi/index.html (accessed on 16 May 2022).
- Din, A.; Wilson, R. Crosswalking ZIP codes to census geographies: Geoprocessing the U.S. Department of Housing & Urban Development’s ZIP code crosswalk files. Cityscape 2020, 22, 293–314. [Google Scholar]
- US Census Bureau. 2015–2019 American Community Survey 5-year Estimates. 2019. Available online: https://www.census.gov/programs-surveys/acs/technical-documentation/table-and-geography-changes/2019/5-year.html (accessed on 18 May 2022).
- ESRI. ArcGIS Pro. Available online: https://www.esri.com/en-us/arcgis/products/arcgis-pro/overview (accessed on 6 July 2022).
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and Receptivity for COVID-19 Vaccines: A Rapid Systematic Review. Vaccines 2020, 9, 16. [Google Scholar] [CrossRef] [PubMed]
- Kaiser Family Foundation (KFF). COVID-19 Racial Disparities in Testing, Infection, Hospitalization, and Death: Analysis of Epic Patient Data. 2020. Available online: https://www.kff.org/coronavirus-covid-19/issue-brief/covid-19-racial-disparities-testing-infection-hospitalization-death-analysis-epic-patient-data/ (accessed on 5 June 2022).
- U.S. Department of Health and Human Services Office of Minority Health. Using the Minority Health Social Vulnerability Index to Drive Equitable Public Health Efforts—Blog Post. Available online: https://minorityhealth.hhs.gov/Blog/BlogPost.aspx?BlogID=3288 (accessed on 21 June 2022).
- World Health Organization (WHO). Improving Vaccination Demand and Addressing Hesitancy. Available online: https://www.who.int/immunization/programmes_systems/vaccine_hesitancy/en/ (accessed on 3 November 2020).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Categorical Variables | Available N | % |
| Gender | ||
| Male | 231 | 41.18 |
| Female | 330 | 58.82 |
| Ethnicity | ||
| East Asian | 260 | 42.76 |
| South Asian | 100 | 16.45 |
| Southeast Asian | 179 | 29.44 |
| Non-Asian | 69 | 11.35 |
| Education | ||
| High school or less | 44 | 20.87 |
| High school graduate | 110 | 18.36 |
| Some college | 125 | 20.87 |
| Bachelor’s or higher | 320 | 53.42 |
| Employment status | ||
| Employed | 414 | 69.70 |
| Unemployed | 180 | 30.30 |
| Continuous Variables | Available N | M (SD) |
| Age | 570 | 40.91 (14.23) |
| English proficiency | 607 | 3.23 (0.83) |
| Accessibility of COVID-19 vaccination | ||
| Number of difficulties | 601 | 0.80 (0.63) |
| General perceived difficulty | 588 | 1.80 (0.80) |
| General concerns about COVID-19 | 589 | 2.32 (1.01) |
| COVID-19 vaccine concerns | ||
| Number of concerns | 593 | 0.90 (0.79) |
| General safety concerns | 592 | 3.15 (0.74) |
| Trust in public health agencies | 573 | 3.21 (0.76) |
| Racism | ||
| Being treated unfairly | 585 | 2.92 (1.53) |
| Safety concern due to one’s race | 586 | 3.16 (1.78) |
| Non-Asian | East Asian | South Asian | Southeast Asian | F | MSerror | p | η² | |
|---|---|---|---|---|---|---|---|---|
| Being treated unfairly | 1.54 (1.18) b | 3.21 (1.44) a | 2.97 (1.63) a | 3.00 (1.45) a | 24.21 | 2.08 | <0.001 | 0.11 |
| Safety concern due to one’s race | 1.26 (0.73) c | 3.74 (1.61) a | 2.91 (1.93) b | 3.21 (1.72) b | 42.46 | 2.62 | <0.001 | 0.18 |
| COVID-19 Concerns | Vaccine Accessibility | Vaccine Safety Concerns | Trustworthiness | |||||
|---|---|---|---|---|---|---|---|---|
| B (SE) | p | B (SE) | p | B (SE) | p | B (SE) | p | |
| Sex at birth (ref.: female) | ||||||||
| Male | −0.332 (0.087) | <0.001 | −0.036 (0.063) | 0.567 | −0.043 (0.047) | 0.363 | −0.013 (0.067) | 0.849 |
| Age * | −0.012 (0.003) | <0.001 | −0.004 (0.002) | 0.065 | −0.001 (0.002) | 0.545 | 0.004 (0.003) | 0.145 |
| Ethnicity (ref.: Non-Asian) | ||||||||
| East Asian | −0.351 (0.171) | 0.040 | 0.320 (0.121) | 0.008 | 0.176 (0.093) | 0.059 | −0.001 (0.133) | 0.994 |
| South Asian | −0.036 (0.181) | 0.842 | 0.161 (0.124) | 0.194 | 0.226 (0.097) | 0.020 | 0.172 (0.139) | 0.218 |
| Southeast Asian | 0.038 (0.164) | 0.817 | 0.115 (0.112) | 0.304 | 0.128 (0.088) | 0.145 | −0.004 (0.126) | 0.974 |
| Education (ref: <high school) | ||||||||
| High school or equivalent (GED) | −0.399 (0.189) | 0.035 | −0.068 (0.128) | 0.594 | 0.092 (0.102) | 0.368 | −0.114 (0.154) | 0.459 |
| Some college | −0.082 (0.191) | 0.667 | 0.037 (0.131) | 0.776 | 0.194 (0.104) | 0.062 | −0.345 (0.155) | 0.026 |
| Bachelor’s degree or higher | 0.010 (0.182) | 0.956 | 0.179 (0.132) | 0.174 | 0.164 (0.099) | 0.098 | −0.169 (0.148) | 0.255 |
| Employment status (ref.: unemployed) | ||||||||
| Employed | −0.071 (0.097) | 0.464 | −0.069 (0.067) | 0.306 | −0.035 (0.052) | 0.503 | 0.118 (0.074) | 0.111 |
| English proficiency | 0.119 (0.060) | 0.046 | −0.053 (0.041) | 0.195 | −0.076 (0.032) | 0.017 | 0.028 (0.046) | 0.546 |
| Racism experience | 0.092 (0.060) | 0.127 | 0.042 (0.042) | 0.313 | 0.067 (0.032) | 0.038 | −0.069 (0.047) | 0.147 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, T.-Y.; Ford, O.; Rainville, A.J.; Yang, X.; Chow, C.M.; Lally, S.; Bessire, R.; Donnelly, J. Perceptions of COVID-19 Vaccine, Racism, and Social Vulnerability: An Examination among East Asian Americans, Southeast Asian Americans, South Asian Americans, and Others. Vaccines 2022, 10, 1333. https://doi.org/10.3390/vaccines10081333
Wu T-Y, Ford O, Rainville AJ, Yang X, Chow CM, Lally S, Bessire R, Donnelly J. Perceptions of COVID-19 Vaccine, Racism, and Social Vulnerability: An Examination among East Asian Americans, Southeast Asian Americans, South Asian Americans, and Others. Vaccines. 2022; 10(8):1333. https://doi.org/10.3390/vaccines10081333
Chicago/Turabian StyleWu, Tsu-Yin, Olivia Ford, Alice Jo Rainville, Xining Yang, Chong Man Chow, Sarah Lally, Rachel Bessire, and Jessica Donnelly. 2022. "Perceptions of COVID-19 Vaccine, Racism, and Social Vulnerability: An Examination among East Asian Americans, Southeast Asian Americans, South Asian Americans, and Others" Vaccines 10, no. 8: 1333. https://doi.org/10.3390/vaccines10081333