
Two Pediatric Cases of Multisystem Inflammatory Syndrome with Overlapping Neurological Involvement Following SARS-CoV-2 Vaccination and Unknown SARS-CoV2 Infection: The Importance of Pre-Vaccination History

 , ,
, ,  and
and
Abstract
:1. Introduction
1.1. Case Report 1
1.2. Case Report 2
2. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| SARS-CoV-2 | severe acute respiratory syndrome coronavirus 2 |
| MIS-C | multisystem Inflammatory Syndrome in children |
| MIS-V | multisystem inflammatory syndrome following SARS-CoV-2 vaccination |
| MERS | mild encephalitis/encephalopathy with reversible splenial lesion |
References
- Feldstein, L.R.; Tenforde, M.W.; Friedman, K.G.; Newhams, M.; Rose, E.B.; Dapul, H.; Soma, V.L.; Maddux, A.B.; Mourani, P.M.; Bowens, C.; et al. Characteristics and outcomes of US children and adolescents with multisystem inflammatory syndrome in children (MIS-C) compared with severe acute COVID-19. JAMA 2021, 325, 1074–1087. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Mannan, O.; Eyre, M.; Löbel, U.; Bamford, A.; Eltze, C.; Hameed, B.; Hemingway, C.; Hacohen, Y. Neurologic and Radiographic Findings Associated With COVID-19 Infection in Children. JAMA Neurol. 2020, 77, 1440–1445. [Google Scholar] [CrossRef] [PubMed]
- Bektas, G.; Akcay, N.; Boydag, K.; Sevketoglu, E. Reversible splenial lesion syndrome associated withSARS-CoV-2 infection in two children. Brain Dev. 2021, 43, 230–233. [Google Scholar] [CrossRef] [PubMed]
- Walter, E.B.; Talaat, K.R.; Sabharwal, C.; Gurtman, A.; Lockhart, S.; Paulsen, G.C.; Barnett, E.D.; Muñoz, F.M.; Maldonado, Y.; Pahud, B.A.; et al. Evaluation of the BNT162b2 COVID-19 Vaccine in Children 5 to 11 Years of Age. N. Engl. J. Med. 2022, 386, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Garg, R.K.; Paliwal, V.K. Spectrum of neurological complications following COVID-19 vaccination. Neurol. Sci 2022, 43, 3–40. [Google Scholar] [CrossRef] [PubMed]
- Patone, M.; Handunnetthi, L.; Saatci, D.; Pan, J.; Katikireddi, S.V.; Razvi, S.; Hunt, D.; Mei, X.W.; Dixon, S.; Zaccardi, F.; et al. Neurological complications after first dose of COVID-19 vaccines and SARS-CoV-2 infection. Nat. Med. 2021, 27, 2144–2153. [Google Scholar] [CrossRef] [PubMed]
- Belay, E.D.; Godfred Cato, S.; Rao, A.K.; Abrams, J.; Wilson, W.W.; Lim, S.; Newton-Cheh, C.; Melgar, M.; DeCuir, J.; Webb, B.; et al. Multisystem Inflammatory Syndrome in Adults after SARS-CoV-2 infection and COVID-19 vaccination. Clin. Infect. Dis. 2021, ciab936. [Google Scholar] [CrossRef] [PubMed]
- Yousaf, A.R.; Cortese, M.M.; Taylor, A.W.; Broder, K.R.; Oster, M.E.; Wong, J.M.; Guh, A.Y.; McCormick, D.W.; Kamidani, S.; Schlaudecker, E.P.; et al. Reported cases of multisystem inflammatory syndrome in children aged 12–20 years in the USA who received a COVID-19 vaccine, December, 2020, through August, 2021: A surveillance investigation. Lancet Child Adolesc. Health 2022, 6, 303–312. [Google Scholar] [CrossRef]
- Karatzios, C.; Scuccimarri, R.; Chèdeville, G.; Basfar, W.; Bullard, J.; Stein, D.R. Multisystem Inflammatory Syndrome Following SARS-CoV-2 Vaccination in Two Children. Pediatrics 2022. [Google Scholar] [CrossRef] [PubMed]
- Buchhorn, R.; Meyer, C.; Schulze-Forster, K.; Junker, J.; Heidecke, H. Autoantibody Release in Children after Corona Virus mRNA Vaccination: A Risk Factor of Multisystem Inflammatory Syndrome? Vaccines 2021, 9, 1353. [Google Scholar] [CrossRef] [PubMed]
- Iyengar, K.P.; Nune, A.; Ish, P.; Botchu, R.; Shashidhara, M.K.; Jain, V.K. Multisystem inflammatory syndrome after SARS-CoV-2 vaccination (MIS-V), to interpret with caution. Postgrad. Med. J. 2021, 98, e91. [Google Scholar] [CrossRef] [PubMed]
- Salzman, M.B.; Huang, C.W.; O’Brien, C.M.; Castillo, R.D. Multisystem Inflammatory Syndrome after SARS-CoV-2 Infection and COVID-19 Vaccination. Emerg. Infect. Dis. 2021, 27, 1944–1948. [Google Scholar] [CrossRef] [PubMed]
- Consiglio, C.R.; Cotugno, N.; Sardh, F.; Pou, C.; Amodio, D.; Rodriguez, L.; Tan, Z.; Zicari, S.; Ruggiero, A.; Pascucci, G.R.; et al. The Immunology of Multisystem Inflammatory Syndrome in Children with COVID-19. Cell 2020, 183, 968–981. [Google Scholar] [CrossRef] [PubMed]
- Vogel, T.P.; Top, K.A.; Karatzios, C.; Hilmers, D.C.; Tapia, L.I.; Moceri, P.; Giovannini-Chami, L.; Wood, N.; Chandler, R.E.; Klein, N.P.; et al. Multisystem inflammatory syndrome in children and adults (MIS-C/A): Case definition & guidelines for data collection, analysis, and presentation of immunization safety data. Vaccine 2021, 39, 3037–3049. [Google Scholar] [PubMed]
- Sacco, K.; Castagnoli, R.; Vakkilainen, S.; Liu, C.; Delmonte, O.M.; Oguz, C.; Kaplan, I.M.; Alehashemi, S.; Burbelo, P.D.; Bhuyan, F.; et al. Immunopathological signatures in multisystem inflammatory syndrome in children and pediatric COVID-19. Nat. Med. 2022, 28, 1050–1062. [Google Scholar] [CrossRef] [PubMed]
- Dennis-Heyward, E. Disparities in Susceptibility to Multisystem Inflammatory Syndrome in Children. JAMA Pediatr. 2021, 175, 892–893. [Google Scholar] [CrossRef] [PubMed]
- Takanashi, J.; Tada, H.; Maeda, M.; Suzuki, M.; Terada, H.; Barkovich, A.J. Encephalopathy with a reversible splenial lesion is associated with hyponatremia. Brain Dev. 2009, 31, 217–220. [Google Scholar] [CrossRef] [PubMed]
- Okada, T.; Fujita, Y.; Imataka, G.; Takase, N.; Tada, H.; Sakuma, H.; Takanashi, J.I. Increased cytokines/chemokines and hyponatremia as a possible cause of clinically mild encephalitis/encephalopathy with a reversible splenial lesion associated with acute focal bacterial nephritis. Brain Dev. 2022, 44, 30–35. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Title | Patient 1 | Patient 2 |
|---|---|---|
| Age (years) | 14 | 9 |
| Sex | F | M |
| Initial central nervous system Manifestations | Episode of unresponsiveness to stimuli, catatonia, inability to move followed by agitation and confusion | Agitation and headache, followed by drowsiness |
| Others symptoms | Fever, vomit | Fever, conjunctivitis, palmar rash, vomiting, diarrhea, abdominal pain |
| Laboratory findings | ||
| White blood cell (103/uL) | 11.87 | 5.06 |
| Neutrophils (103/uL) | 10.03 | 4.20 |
| Lymphocytes (103/uL) | 0.74 | 0.44 |
| Platelet (103/uL) | 314 | 55 |
| CRP (mg/dL) (N < 0.50) | 26.77 | 16 |
| Procalcitonin (ng/mL)(N: 0–0.5) | 4.18 | 9.96 |
| Ferritin (mg/L)(N: 13–150) | 501 | 1374 |
| Troponin I (pg/mL)(N: <14) | 25.7 | 66.1 |
| Pro-BNP (pg/L)(N: <217) | 320 | 9865 |
| Fibrinogen (mg/dL)(N: 212–433) | 700 | 552 |
| D-dimer (mcg/mL) | 8.18 | 5.35 |
| Albumin (g/dl) | 3.1 | 3.3 |
| Natrium (mEq/L) | 127 | 129 |
| AST (U/L) | 46 | 70 |
| ALT (U/L) | 54 | 32 |
| Creatinine (mg/dl) | 1.26 | 1.17 |
| ACTH (pg/mL) | 228 | |
| CSF | ||
| Glucose (mg/dL) | 97 | |
| Protein (mg/dL) | 20 | |
| Cell count (/mm3) | 2 | |
| Echocardiogram | Normal ventricular systolic functions | Left ventricular ejection fraction 44% |
| Chest X-ray | Normal at the admission Day 3: right pleural effusion | Mild accentuation of the broncovascular texture |
| EEG | global slowing | global slowing |
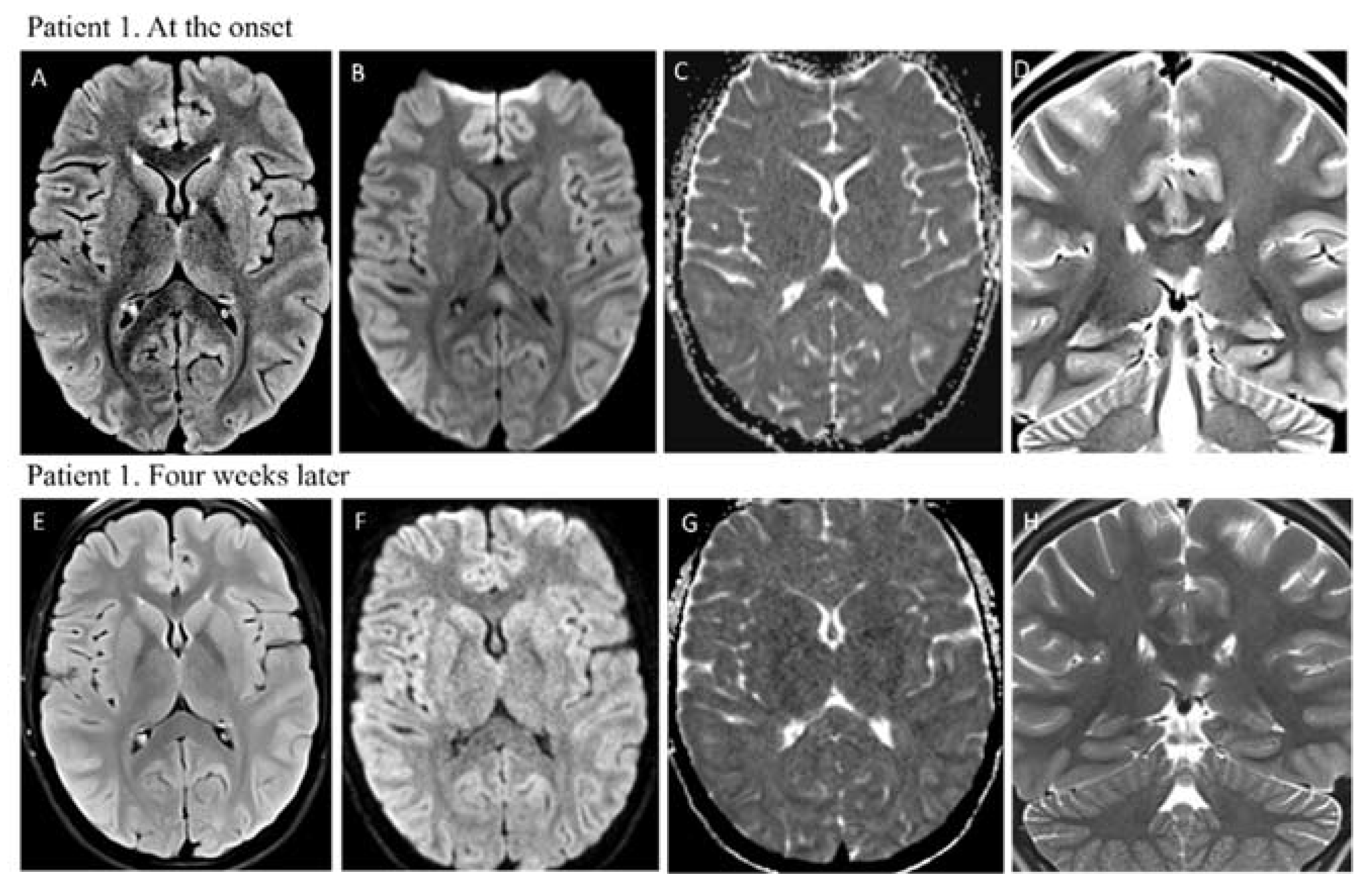
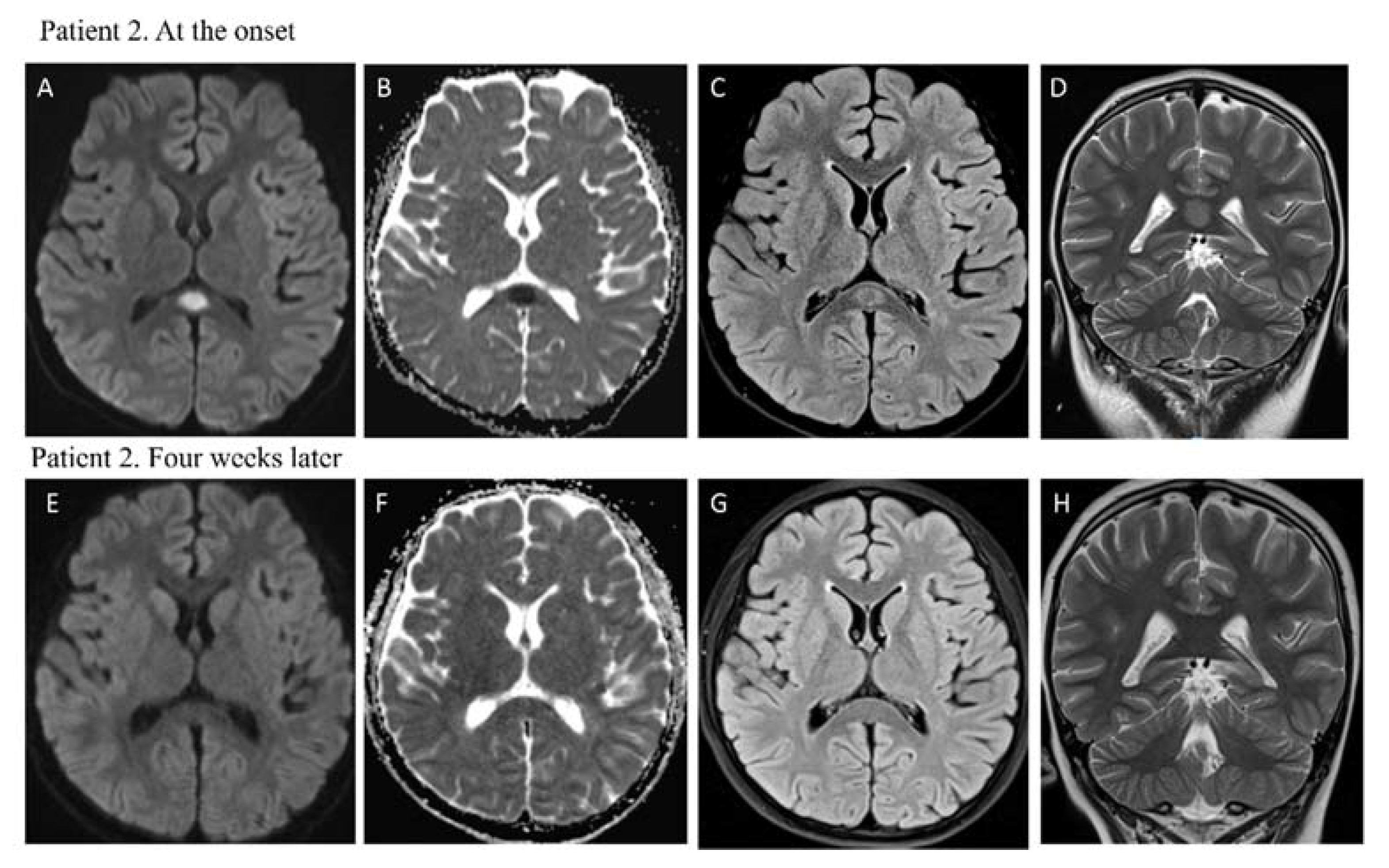
| Brain Imaging | MRI: hyperintensity on T2-weighted images in the splenium of the corpus callosum with restricted diffusion | MRI: hyperintensity on T2-weighted images in the splenium of corpus callosum with restricted diffusion |
| Immune treatment | IVIG Steroid therapy | IVIG Steroid therapy Anakinra |
| Other treatment | Oxygen | Milrinone |
| Enoxaparin | Enoxaparin | |
| Diuretic | Diuretic |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santilli, V.; Manno, E.C.; Giancotta, C.; Rossetti, C.; Cotugno, N.; Amodio, D.; Rotulo, G.A.; Deodati, A.; Bianchi, R.; Lucignani, G.; et al. Two Pediatric Cases of Multisystem Inflammatory Syndrome with Overlapping Neurological Involvement Following SARS-CoV-2 Vaccination and Unknown SARS-CoV2 Infection: The Importance of Pre-Vaccination History. Vaccines 2022, 10, 1136. https://doi.org/10.3390/vaccines10071136
Santilli V, Manno EC, Giancotta C, Rossetti C, Cotugno N, Amodio D, Rotulo GA, Deodati A, Bianchi R, Lucignani G, et al. Two Pediatric Cases of Multisystem Inflammatory Syndrome with Overlapping Neurological Involvement Following SARS-CoV-2 Vaccination and Unknown SARS-CoV2 Infection: The Importance of Pre-Vaccination History. Vaccines. 2022; 10(7):1136. https://doi.org/10.3390/vaccines10071136
Chicago/Turabian StyleSantilli, Veronica, Emma Concetta Manno, Carmela Giancotta, Chiara Rossetti, Nicola Cotugno, Donato Amodio, Gioacchino Andrea Rotulo, Annalisa Deodati, Roberto Bianchi, Giulia Lucignani, and et al. 2022. "Two Pediatric Cases of Multisystem Inflammatory Syndrome with Overlapping Neurological Involvement Following SARS-CoV-2 Vaccination and Unknown SARS-CoV2 Infection: The Importance of Pre-Vaccination History" Vaccines 10, no. 7: 1136. https://doi.org/10.3390/vaccines10071136