
Vaccine Resistance and Hesitancy among Older Adults Who Live Alone or Only with an Older Partner in Community in the Early Stage of the Fifth Wave of COVID-19 in Hong Kong


 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Participants and Data Collection
2.2. Measures
2.3. Statistical Methods
3. Results
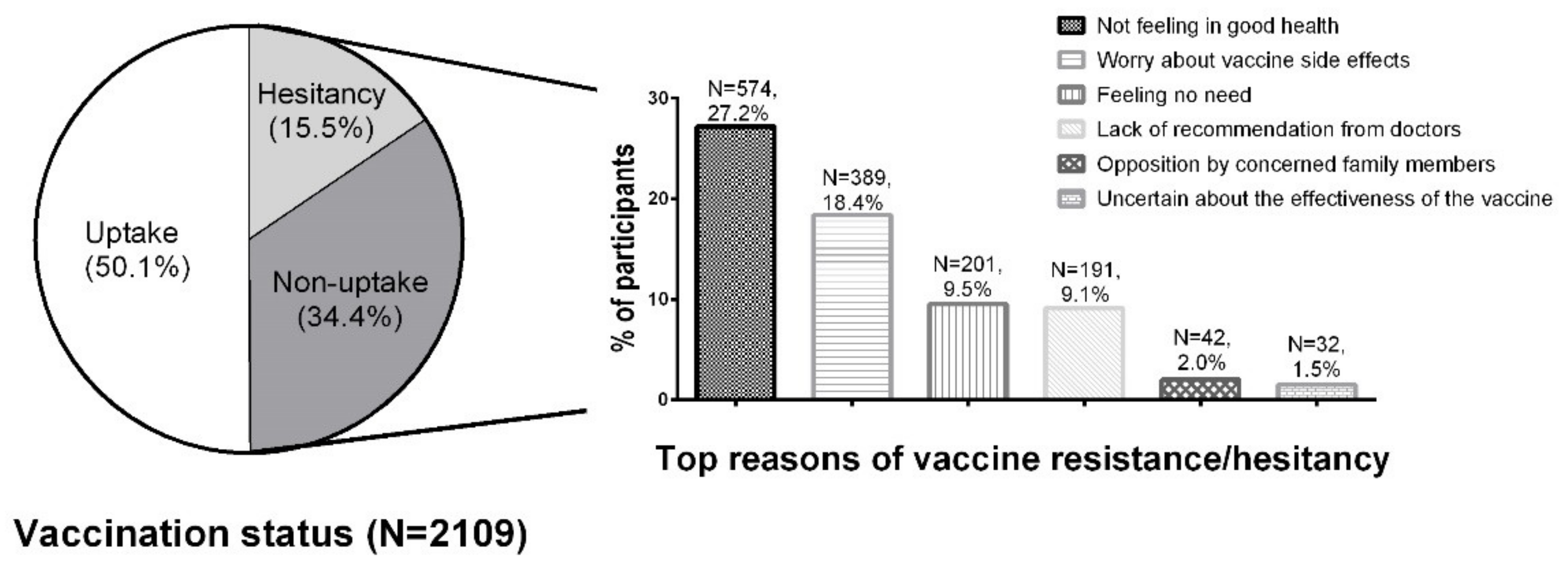
3.1. Participants’ Characteristics and Reasons for Vaccine Resistance or Hesitancy
3.2. Univariate Analysis on Factors Associated with Vaccine Resistance and Hesitancy
3.3. Multivariate Analysis on Factors Associated with Vaccine Resistance and Hesitancy

{kind=link}
| Characteristics | Crude OR | 95% CI | p-Value | Adjusted OR * | 95 % CI | p-Value | ||
|---|---|---|---|---|---|---|---|---|
| Age (years) | ||||||||
| Mean (SD) | 1.04 | 1.03 | 1.05 | <0.001 | 1.03 | 1.02 | 1.04 | <0.001 |
| Sex | ||||||||
| Male | Ref | Ref | ||||||
| Female | 0.94 | 0.78 | 1.13 | 0.493 | 0.91 | 0.74 | 1.11 | 0.343 |
| Living status | ||||||||
| Live with an older partner | Ref | Ref | ||||||
| Live alone | 1.38 | 1.16 | 1.65 | <0.001 | 1.32 | 1.08 | 1.61 | 0.007 |
| Occupational status | ||||||||
| Retirement | Ref | Ref | ||||||
| Caring family/full-time/part-time/unemployed | 0.47 | 0.30 | 0.74 | 0.001 | 0.63 | 0.39 | 1.02 | 0.062 |
| Social security support | ||||||||
| No | Ref | Ref | ||||||
| Yes (CSSA or OALA) | 1.22 | 0.99 | 1.49 | 0.057 | 1.00 | 0.81 | 1.25 | 0.978 |
| Number of doctor-diagnosed chronic conditions | ||||||||
| 0–1 | Ref | Ref | ||||||
| 2–3 | 1.17 | 0.97 | 1.42 | 0.110 | 1.03 | 0.84 | 1.28 | 0.764 |
| >3 | 1.89 | 1.49 | 2.39 | <0.001 | 1.55 | 1.17 | 2.04 | 0.002 |
| Ever hospital admission over the past 6 months | ||||||||
| No | Ref | Ref | ||||||
| Yes | 1.51 | 1.18 | 1.93 | 0.001 | 1.24 | 0.95 | 1.60 | 0.114 |
| Medical appointment in the next 6 months | ||||||||
| No | Ref | |||||||
| Yes | 1.14 | 0.91 | 1.42 | 0.265 | ||||
| Regular measurement of blood pressure | ||||||||
| No hypertension | Ref | |||||||
| Yes | 1.13 | 0.85 | 1.50 | 0.396 | ||||
| Not measure regularly | 1.28 | 0.93 | 1.74 | 0.126 | ||||
| Regular measurement of blood glucose | ||||||||
| No diabetes | Ref | Ref | ||||||
| Yes | 1.21 | 0.97 | 1.51 | 0.091 | 1.08 | 0.85 | 1.39 | 0.521 |
| Not measure regularly | 1.17 | 0.88 | 1.55 | 0.294 | 0.98 | 0.71 | 1.33 | 0.879 |
| Help available when needed | ||||||||
| Yes | Ref | Ref | ||||||
| No | 1.24 | 1.01 | 1.53 | 0.038 | 1.13 | 0.90 | 1.42 | 0.279 |
| Number of social media use in the past 2 weeks | ||||||||
| 0 | Ref | Ref | ||||||
| 1 | 0.62 | 0.50 | 0.76 | <0.001 | 0.69 | 0.55 | 0.86 | 0.001 |
| >1 | 0.39 | 0.29 | 0.52 | <0.001 | 0.48 | 0.36 | 0.65 | <0.001 |
| Self-rated Health status in score | ||||||||
| High (67–100) | Ref | Ref | ||||||
| Middle (34–66) | 1.42 | 1.14 | 1.76 | 0.002 | 1.51 | 1.20 | 1.91 | <0.001 |
| Low (0–33) | 1.76 | 1.43 | 2.17 | <0.001 | 1.57 | 1.24 | 1.99 | <0.001 |
| Meaning of life | ||||||||
| High (5–7) | Ref | Ref | ||||||
| Middle (3–4) | 1.41 | 1.16 | 1.72 | 0.001 | 1.10 | 0.89 | 1.37 | 0.391 |
| Low (1–2) | 1.62 | 1.02 | 2.57 | 0.039 | 1.08 | 0.65 | 1.79 | 0.771 |
| Missing | 1.43 | 1.11 | 1.84 | 0.005 | 1.34 | 1.02 | 1.77 | 0.036 |
| Loneliness (measured by UCLA-3) | ||||||||
| 0–5 | Ref | Ref | ||||||
| ≥6 | 1.44 | 1.14 | 1.81 | 0.002 | 1.11 | 0.85 | 1.46 | 0.433 |
| Memory loss | ||||||||
| No | Ref | Ref | ||||||
| Yes, but not worry | 1.02 | 0.84 | 1.25 | 0.817 | 0.91 | 0.73 | 1.12 | 0.375 |
| Yes, and worry | 1.44 | 1.10 | 1.89 | 0.009 | 1.08 | 0.80 | 1.46 | 0.620 |
| Depression (measured by PHQ-2) | ||||||||
| 0–2 | Ref | Ref | ||||||
| ≥3 | 1.58 | 1.13 | 2.20 | 0.007 | 1.07 | 0.66 | 1.75 | 0.785 |
| Anxiety (measured by GAD-2) | ||||||||
| 0–2 | Ref | Ref | ||||||
| ≥3 | 1.61 | 1.11 | 2.33 | 0.012 | 1.27 | 0.74 | 2.19 | 0.380 |
3.4. Additional Separate Analysis on Factors Associated with Vaccine Resistance and Factors Associated with Vaccine Hesitancy
4. Discussion
4.1. Major Findings
4.2. Strengths and Limitations
4.3. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 1 June 2022).
- Veronese, N.; Saccaro, C.; Demurtas, J.; Smith, L.; Dominguez, L.J.; Maggi, S.; Barbagallo, M. Prevalence of unwillingness and uncertainty to vaccinate against COVID-19 in older people: A systematic review and meta-analysis. Ageing Res. Rev. 2021, 72, 101489. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef] [PubMed]
- Gallè, F.; Sabella, E.A.; Roma, P.; Ferracuti, S.; Da Molin, G.; Diella, G.; Montagna, M.T.; Orsi, G.B.; Liguori, G.; Napoli, C.; et al. Knowledge and Lifestyle Behaviors Related to COVID-19 Pandemic in People over 65 Years Old from Southern Italy. Int. J. Environ. Res. Public Health 2021, 18, 10872. [Google Scholar] [CrossRef]
- Gallant, A.J.; Nicholls, L.A.B.; Rasmussen, S.; Cogan, N.; Young, D.; Williams, L. Changes in attitudes to vaccination as a result of the COVID-19 pandemic: A longitudinal study of older adults in the UK. PLoS ONE 2021, 16, e0261844. [Google Scholar] [CrossRef]
- Wu, L.; Wang, X.; Li, R.; Huang, Z.; Guo, X.; Liu, J.; Yan, H.; Sun, X. Willingness to Receive a COVID-19 Vaccine and Associated Factors among Older Adults: A Cross-Sectional Survey in Shanghai, China. Vaccines 2022, 10, 654. [Google Scholar] [CrossRef]
- Huang, C.Y.; Lin, C.C.; Hsieh, C.Y.; Lin, C.Y.; Chen, T.T.; Wu, P.C.; Liu, D.H.; Tou, S.I.; Yen, H.R. The Willingness of Elderly Taiwanese Individuals to Accept COVID-19 Vaccines after the First Local Outbreak. Vaccines 2022, 10, 520. [Google Scholar] [CrossRef]
- Xiao, J.; Cheung, J.K.; Wu, P.; Ni, M.Y.; Cowling, B.J.; Liao, Q. Temporal changes in factors associated with COVID-19 vaccine hesitancy and uptake among adults in Hong Kong: Serial cross-sectional surveys. Lancet Reg. Health West. Pac. 2022, 23, 100441. [Google Scholar] [CrossRef]
- MacDonald, N.E.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; Goldstein, S.; Larson, H.; Manzo, M.L.; Reingold, A.; et al. Vaccine Hesitancy: Definition, Scope and Determinants. Vaccine 2015, 33, 4161. [Google Scholar] [CrossRef]
- Sallam, M.; Al-Sanafi, M.; Sallam, M. A Global Map of COVID-19 Vaccine Acceptance Rates per Country: An Updated Concise Narrative Review. J. Multidiscip. Healthc. 2022, 15, 21–45. [Google Scholar] [CrossRef]
- Smith, D.J.; Hakim, A.J.; Leung, G.M.; Xu, W.; Schluter, W.W.; Novak, R.T.; Marston, B.; Hersh, B.S. COVID-19 Mortality and Vaccine Coverage—Hong Kong Special Administrative Region, China, January 6, 2022–March 21, 2022. Morb. Mortal. Wkly. Rep. 2022, 71, 545. [Google Scholar] [CrossRef]
- Kwan, R. How Hong Kong’s vaccination missteps led to the world’s highest Covid-19 death rate. BMJ 2022, 377, 1127. [Google Scholar] [CrossRef]
- Wang, K.; Wong, E.L.Y.; Cheung, A.W.L.; Yau, P.S.Y.; Chung, V.C.H.; Wong, C.H.L.; Dong, D.; Wong, S.Y.S.; Yeoh, E.K. Influence of Vaccination Characteristics on COVID-19 Vaccine Acceptance Among Working-Age People in Hong Kong, China: A Discrete Choice Experiment. Front. Public Health 2021, 9, 793533. [Google Scholar] [CrossRef]
- Kwok, K.O.; Li, K.K.; Wei, W.I.; Tsoi, M.T.F.; Tang, A.; Lam, H.S.; McNeil, E.B.; Wong, S.Y.S. Likelihood of COVID-19 vaccination among primary school students in Hong Kong. Clin. Microbiol. Infect. 2021, 28, 142–144. [Google Scholar] [CrossRef]
- Kharicha, K.; Harari, D.; Swift, C.; Stuck, G.G.E. Health risk appraisal in older people 1: Are older people living alone an ‘at-risk’ group? Br. J. Gen. Pract. 2007, 57, 271. [Google Scholar]
- Wong, K.; Yeung, M. Population ageing trend of Hong Kong. Population 2019, 18, 64. [Google Scholar]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Zhang, D.; Sit, R.W.S.; Wong, C.; Zou, D.; Mercer, S.W.; Johnston, M.C.; Wong, S.Y.S. Cohort profile: The prospective study on Chinese elderly with multimorbidity in primary care in Hong Kong. BMJ Open 2020, 10, e027279. [Google Scholar] [CrossRef] [Green Version]
- Poon, P.K.M.; Zhou, W.; Chan, D.C.C.; Kwok, K.O.; Wong, S.Y.S. Recommending COVID-19 Vaccines to Patients: Practice and Concerns of Frontline Family Doctors. Vaccines 2021, 9, 1319. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The Patient Health Questionnaire-2: Validity of a two-item depression screener. Med. Care 2003, 41, 1284–1292. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.; Monahan, P.O.; Löwe, B. Anxiety Disorders in Primary Care: Prevalence, Impairment, Comorbidity, and Detection. Ann. Intern. Med. 2007, 146, 317–325. [Google Scholar] [CrossRef]
- Russell, D. UCLA Loneliness Scale (Version 3): Reliability, Validity, and Factor Structure. J. Pers. Assess. 1996, 66, 20–40. [Google Scholar] [CrossRef]
- Shek, D. Reliability and factorial structure of the Chinese version of the purpose in life questionnaire. J. Clin. Psychol. 1988, 44, 384–392. [Google Scholar] [CrossRef]
- Stevens, J. Applied Multivariate Statistics for the Social Sciences; Routledge: Abingdon, UK, 2002. [Google Scholar]
- Siu, J.Y.M.; Cao, Y.; Shum, D.H. Perceptions of and hesitancy toward COVID-19 vaccination in older Chinese adults in Hong Kong: A qualitative study. BMC Geriatr. 2022, 22, 288. [Google Scholar] [CrossRef]
- Fieselmann, J.; Annac, K.; Erdsiek, F.; Yilmaz-Aslan, Y.; Brzoska, P. What are the reasons for refusing a COVID-19 vaccine? A qualitative analysis of social media in Germany. BMC Public Health 2022, 22, 846. [Google Scholar] [CrossRef]
- Pierri, F.; Perry, B.L.; DeVerna, M.R.; Yang, K.C.; Flammini, A.; Menczer, F.; Bryden, J. Online misinformation is linked to early COVID-19 vaccination hesitancy and refusal. Sci. Rep. 2022, 12, 5966. [Google Scholar] [CrossRef] [PubMed]
- Lai, F.T.T.; Huang, L.; Chui, C.S.L.; Wan, E.Y.F.; Li, X.; Wong, C.K.H.; Chan, E.W.W.; Ma, T.; Lum, D.H.; Leung, J.C.N.; et al. Multimorbidity and adverse events of special interest associated with Covid-19 vaccines in Hong Kong. Nat. Commun. 2022, 13, 411. [Google Scholar] [CrossRef] [PubMed]
- Wilson-Genderson, M.; Heid, A.R.; Cartwright, F.; Collins, A.L.; Pruchno, R. Change in Loneliness Experienced by Older Men and Women Living Alone and With Others at the Onset of the COVID-19 Pandemic. Res. Aging 2022, 44, 369–381. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.; van Hoek, A.; Boccia, D.; Thomas, S.L. Lower vaccine uptake amongst older individuals living alone: A systematic review and meta-analysis of social determinants of vaccine uptake. Vaccine 2017, 35, 2315–2328. [Google Scholar] [CrossRef]
- Yuan, S. Zero COVID in China: What next? Lancet 2022, 399, 1856–1857. [Google Scholar] [CrossRef]
- Kwok, K.O.; Li, K.K.; Tang, A.; Tsoi, M.T.F.; Chan, E.Y.Y.; Tang, J.W.T.; Wong, A.; Wei, W.I.; Wong, S.Y.S. Psychobehavioral Responses and Likelihood of Receiving COVID-19 Vaccines during the Pandemic, Hong Kong. Emerg. Infect. Dis. 2021, 27, 1802–1810. [Google Scholar] [CrossRef]
- The Government of the Hong Kong SAR. Hong Kong Vaccination Dashboard. Available online: https://www.covidvaccine.gov.hk/en/dashboard (accessed on 7 June 2022).
- Minstry of Health, Singapore. Vaccination Statistics. Available online: https://www.moh.gov.sg/covid-19/vaccination/statistics (accessed on 7 June 2022).
- Census and Statistics Department Hong Kong SAR. Thematic Report: Older Persons. Available online: https://www.statistics.gov.hk/pub/B11201052016XXXXB0100.pdf (accessed on 8 July 2022).
- Hong Kong Monthly Digest of Statistics. Statistics on Comprehensive Social Security Assistance Scheme, 2010 to 2020. Available online: https://www.censtatd.gov.hk/en/data/stat_report/product/FA100078/att/B72109FB2021XXXXB0100.pdf (accessed on 8 July 2022).

| Variables | All Participants | Vaccinated or Intention to Be Vaccinated * | Hesitated to Be Vaccinated | Unvaccinated | ||||
|---|---|---|---|---|---|---|---|---|
| N = 2109 | % | N = 1057 | % | N = 327 | % | N = 725 | % | |
| Age (years) | ||||||||
| Mean (SD) | 79.3 | 7.6 | 78.2 | 7.2 | 79.7 | 7.5 | 80.8 | 8.0 |
| Sex | ||||||||
| Male | 649 | 30.8 | 318 | 30.1 | 91 | 27.8 | 240 | 33.1 |
| Female | 1460 | 69.2 | 739 | 69.9 | 236 | 72.2 | 485 | 66.9 |
| Living status | ||||||||
| Living with an older partner | 775 | 36.7 | 428 | 40.5 | 111 | 33.9 | 236 | 32.6 |
| Living alone | 1334 | 63.3 | 629 | 59.5 | 216 | 66.1 | 489 | 67.4 |
| Occupational status | ||||||||
| Retirement | 2007 | 95.2 | 990 | 93.7 | 316 | 96.6 | 701 | 96.7 |
| Caring family/Full-time/part-time/unemployed | 92 | 4.4 | 62 | 5.9 | 9 | 2.8 | 21 | 2.9 |
| Missing | 10 | 0.5 | 5 | 0.5 | 2 | 0.6 | 3 | 0.4 |
| Social security support | ||||||||
| No | 488 | 23.1 | 263 | 24.9 | 74 | 22.6 | 151 | 20.8 |
| Yes (CSSA or OALA) | 1621 | 76.9 | 794 | 75.1 | 253 | 77.4 | 574 | 79.2 |
| Number of doctor-diagnosed chronic conditions | ||||||||
| 0–1 | 749 | 35.5 | 414 | 39.2 | 105 | 32.1 | 230 | 31.7 |
| 2–3 | 904 | 42.9 | 464 | 43.9 | 148 | 45.3 | 292 | 40.3 |
| >3 | 447 | 21.2 | 177 | 16.7 | 74 | 22.6 | 196 | 27.0 |
| Missing | 9 | 0.4 | 2 | 0.2 | 0 | 0.0 | 7 | 1.0 |
| Ever hospital admission over the past 6 months | ||||||||
| No | 1787 | 84.7 | 925 | 87.5 | 266 | 81.3 | 596 | 82.2 |
| Yes | 306 | 14.5 | 127 | 12.0 | 59 | 18.0 | 120 | 16.6 |
| Missing | 16 | 0.8 | 5 | 0.5 | 2 | 0.6 | 9 | 1.2 |
| Medical appointment in the next 6 months | ||||||||
| No | 375 | 17.8 | 198 | 18.7 | 46 | 14.1 | 131 | 18.1 |
| Yes | 1721 | 81.6 | 854 | 80.8 | 280 | 85.6 | 587 | 81.0 |
| Missing | 13 | 0.6 | 5 | 0.5 | 1 | 0.3 | 7 | 1.0 |
| Regular measurement of blood pressure | ||||||||
| No hypertension | 226 | 10.7 | 121 | 11.4 | 25 | 7.6 | 80 | 11.0 |
| Yes | 1335 | 63.3 | 674 | 63.8 | 215 | 65.7 | 446 | 61.5 |
| Not measure regularly | 533 | 25.3 | 253 | 23.9 | 86 | 26.3 | 194 | 26.8 |
| Missing | 15 | 0.7 | 9 | 0.9 | 1 | 0.3 | 5 | 0.7 |
| Regular measurement of blood glucose | ||||||||
| No diabetes | 1452 | 68.8 | 748 | 70.8 | 236 | 72.2 | 468 | 64.6 |
| Yes | 398 | 18.9 | 186 | 17.6 | 60 | 18.3 | 152 | 21.0 |
| Not measure regularly | 216 | 10.2 | 103 | 9.7 | 23 | 7.0 | 90 | 12.4 |
| Missing | 43 | 2.0 | 20 | 1.9 | 8 | 2.4 | 15 | 2.1 |
| Help available when needed | ||||||||
| Yes | 1623 | 77.0 | 831 | 78.6 | 254 | 77.7 | 538 | 74.2 |
| No | 472 | 22.4 | 216 | 20.4 | 71 | 21.7 | 185 | 25.5 |
| Missing | 14 | 0.7 | 10 | 0.9 | 2 | 0.6 | 2 | 0.3 |
| Types of social media use in the past 2 weeks | ||||||||
| 0 | 1339 | 63.5 | 595 | 56.3 | 220 | 67.3 | 524 | 72.3 |
| 1 | 506 | 24.0 | 286 | 27.1 | 74 | 22.6 | 146 | 20.1 |
| >1 | 253 | 12.0 | 170 | 16.1 | 32 | 9.8 | 51 | 7.0 |
| Missing | 11 | 0.5 | 6 | 0.6 | 1 | 0.3 | 4 | 0.6 |
| Self-rated Health status | ||||||||
| High (score 67–100) | 686 | 32.5 | 397 | 37.6 | 88 | 26.9 | 201 | 27.7 |
| Middle (score 34–66) | 624 | 29.6 | 307 | 29.0 | 113 | 34.6 | 204 | 28.1 |
| Low (score 0–33) | 760 | 36.0 | 333 | 31.5 | 121 | 37.0 | 306 | 42.2 |
| Missing | 39 | 1.8 | 20 | 1.9 | 5 | 1.5 | 14 | 1.9 |
| Meaning of life | ||||||||
| High (5–7) | 1075 | 51.0 | 586 | 55.4 | 166 | 50.8 | 323 | 44.6 |
| Middle (3–4) | 638 | 30.3 | 293 | 27.7 | 90 | 27.5 | 255 | 35.2 |
| Low (1–2) | 80 | 3.8 | 34 | 3.2 | 12 | 3.7 | 34 | 4.7 |
| Missing | 316 | 15.0 | 144 | 13.6 | 59 | 18.0 | 113 | 15.6 |
| Loneliness (measured by UCLA-3) | ||||||||
| 0–5 | 1748 | 82.9 | 902 | 85.3 | 268 | 82.0 | 578 | 79.7 |
| ≥6 | 355 | 16.8 | 151 | 14.3 | 59 | 18.0 | 145 | 20.0 |
| Missing | 6 | 0.3 | 4 | 0.4 | 0 | 0.0 | 2 | 0.3 |
| Memory loss | ||||||||
| No | 560 | 26.6 | 291 | 27.5 | 78 | 23.9 | 191 | 26.3 |
| Yes, but not worry | 1201 | 56.9 | 617 | 58.4 | 187 | 57.2 | 397 | 54.8 |
| Yes, and worry | 340 | 16.1 | 146 | 13.8 | 61 | 18.7 | 133 | 18.3 |
| Missing | 8 | 0.4 | 3 | 0.3% | 1 | 0.3 | 4 | 0.6 |
| Depression (measured by PHQ-2) | ||||||||
| 0–2 | 1929 | 91.5 | 984 | 93.1 | 307 | 93.9 | 638 | 88.0 |
| ≥3 | 156 | 7.4 | 62 | 5.9 | 18 | 5.5 | 76 | 10.5 |
| Missing | 24 | 1.1 | 11 | 1.0 | 2 | 0.6 | 11 | 1.5 |
| Anxiety (measured by GAD-2) | ||||||||
| 0–2 | 1957 | 92.8 | 996 | 94.2 | 307 | 93.9 | 654 | 90.2 |
| ≥3 | 125 | 5.9 | 49 | 4.6 | 16 | 4.9 | 60 | 8.3 |
| Missing | 27 | 1.3 | 12 | 1.1 | 4 | 1.2 | 11 | 1.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, D.; Zhou, W.; Poon, P.K.-M.; Kwok, K.O.; Chui, T.W.-S.; Hung, P.H.Y.; Ting, B.Y.T.; Chan, D.C.-C.; Wong, S.Y.-S. Vaccine Resistance and Hesitancy among Older Adults Who Live Alone or Only with an Older Partner in Community in the Early Stage of the Fifth Wave of COVID-19 in Hong Kong. Vaccines 2022, 10, 1118. https://doi.org/10.3390/vaccines10071118
Zhang D, Zhou W, Poon PK-M, Kwok KO, Chui TW-S, Hung PHY, Ting BYT, Chan DC-C, Wong SY-S. Vaccine Resistance and Hesitancy among Older Adults Who Live Alone or Only with an Older Partner in Community in the Early Stage of the Fifth Wave of COVID-19 in Hong Kong. Vaccines. 2022; 10(7):1118. https://doi.org/10.3390/vaccines10071118
Chicago/Turabian StyleZhang, Dexing, Weiju Zhou, Paul Kwok-Ming Poon, Kin On Kwok, Tracy Wai-Sze Chui, Phoebe Hoi Yi Hung, Bonny Yin Tung Ting, Dicken Cheong-Chun Chan, and Samuel Yeung-Shan Wong. 2022. "Vaccine Resistance and Hesitancy among Older Adults Who Live Alone or Only with an Older Partner in Community in the Early Stage of the Fifth Wave of COVID-19 in Hong Kong" Vaccines 10, no. 7: 1118. https://doi.org/10.3390/vaccines10071118