
BNT162b2 mRNA COVID-19 Vaccine Does Not Impact the Honeymoon Phase in Type 1 Diabetes: A Case Report

 ,
,  , , , , ,
, , , , , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Presentation
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pal, R.; Bhadada, S.K.; Misra, A. COVID-19 vaccination in patients with diabetes mellitus: Current concepts, uncertainties and challenges. Diabetes Metab. Syndr. 2021, 15, 505–508. [Google Scholar] [CrossRef] [PubMed]
- Gregory, J.M.; Moore, D.J. The Dual Burden of Type 1 Diabetes and COVID-19. Ann. Intern. Med. 2021, 174, 703–704. [Google Scholar] [CrossRef] [PubMed]
- Drucker, D.J. Diabetes, obesity, metabolism, and SARS-CoV-2 infection: The end of the beginning. Cell Metab. 2021, 33, 479–498. [Google Scholar] [CrossRef] [PubMed]
- Powers, A.C.; Aronoff, D.M.; Eckel, R.H. COVID-19 vaccine prioritisation for type 1 and type 2 diabetes. Lancet Diabetes Endocrinol. 2021, 9, 140–141. [Google Scholar] [CrossRef]
- DiMeglio, L.A. COVID-19 and Type 1 Diabetes: Addressing Concerns and Maintaining Control. Diabetes Care 2021, 44, 1924–1928. [Google Scholar] [CrossRef]
- Suthar, A.B.; Wang, J.; Seffren, V.; Wiegand, R.E.; Griffing, S.; Zell, E. Public health impact of Covid-19 vaccines in the US: Observational study. BMJ 2022, 377, e069317. [Google Scholar] [CrossRef]
- Samuel, S.M.; Varghese, E.; Triggle, C.R.; Büsselberg, D. COVID-19 Vaccines and Hyperglycemia-Is There a Need for Postvaccination Surveillance? Vaccines 2022, 10, 454. [Google Scholar] [CrossRef]
- Abu-Rumaileh, M.A.; Gharaibeh, A.M.; Gharaibeh, N.E. COVID-19 Vaccine and Hyperosmolar Hyperglycemic State. Cureus 2021, 13, e14125. [Google Scholar] [CrossRef]
- Heald, A.H.; Stedman, M.; Horne, L.; Rea, R.; Whyte, M.; Gibson, J.M.; Livingston, M.; Anderson, S.G.; Ollier, W. Analysis of Continuous Blood Glucose Data in People with Type 1 Diabetes (T1DM) After COVID-19 Vaccination Indicates a Possible Link Between the Immune and the Metabolic Response. J. Diabetes Sci. Technol. 2021, 15, 1204–1205. [Google Scholar] [CrossRef]
- Heald, A.H.; Stedman, M.; Horne, L.; Rea, R.; Whyte, M.; Gibson, J.M.; Anderson, S.G.; Ollier, W. The change in glycaemic control immediately after COVID-19 vaccination in people with type 1 diabetes. Diabet Med. 2022, 39, e14774. [Google Scholar] [CrossRef]
- Fonolleda, M.; Murillo, M.; Vázquez, F.; Bel, J.; Vives-Pi, M. Remission Phase in Paediatric Type 1 Diabetes: New Understanding and Emerging Biomarkers. Horm. Res. Paediatr. 2017, 88, 307–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhong, T.; Tang, R.; Xie, Y.; Liu, F.; Li, X.; Zhou, Z. Frequency, clinical characteristics, and determinants of partial remission in type 1 diabetes: Different patterns in children and adults. J. Diabetes 2020, 12, 761–768. [Google Scholar] [CrossRef] [PubMed]
- Passanisi, S.; Salzano, G.; Gasbarro, A.; Urzì Brancati, V.; Mondio, M.; Pajno, G.B.; Alibrandi, A.; Lombardo, F. Influence of Age on Partial Clinical Remission among Children with Newly Diagnosed Type 1 Diabetes. Int. J. Environ. Res. Public Health 2020, 17, 4801. [Google Scholar] [CrossRef] [PubMed]
- Pinkey, J.H.; Bingley, P.J.; Sawtell, P.A.; Dunger, D.B.; Gale, E.A. Presentation and progress of childhood diabetes mellitus: A prospective population-based study. The Bart’s-Oxford Study Group. Diabetologia 1994, 37, 70–74. [Google Scholar] [CrossRef]
- Wallensteen, M.; Dahlquist, G.; Persson, B.; Landin-Olsson, M.; Lernmark, Å.; Sundkvist, G.; Thalme, B. Factors influencing the magnitude, duration, and rate of fall of B-cell function in type 1 (insulin-dependent) diabetic children followed for two years from their clinical diagnosis. Diabetologia 1988, 31, 664–669. [Google Scholar] [CrossRef] [Green Version]
- Abdul-Rasoul, M.; Habib, H.; Al-Khouly, M. ‘The honeymoon phase’ in children with type 1 diabetes mellitus: Frequency, duration, and influential factors. Pediatr. Diabetes 2006, 7, 101–107. [Google Scholar] [CrossRef]
- Yazidi, M.; Mahjoubi, S.; Oueslati, I.; Chaker, F.; Chihaoui, M. The remission phase in adolescents and young adults with newly diagnosed type 1 diabetes mellitus: Prevalence, predicting factors and glycemic control during follow-up. Arch. Endocrinol. Metab. 2022, 66, 222–228. [Google Scholar] [CrossRef]
- Niedzwiecki, P.; Pilacinski, S.; Uruska, A.; Adamska, A.; Naskret, D.; Zozulinska-Ziolkiewicz, D. Influence of remission and its duration on development of early microvascular complications in young adults with type 1 diabetes. J. Diabetes Complicat. 2015, 29, 1105–1111. [Google Scholar] [CrossRef]
- Infante, M.; Ricordi, C. Editorial—Moving forward on the pathway of targeted immunotherapies for type 1 diabetes: The importance of disease heterogeneity. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 8702–8704. [Google Scholar]
- Aly, H.; Gottlieb, P. The honeymoon phase: Intersection of metabolism and immunology. Curr. Opin. Endocrinol. Diabetes Obes. 2009, 16, 286–292. [Google Scholar] [CrossRef]
- Mortensen, H.B.; Hougaard, P.; Swift, P.; Hansen, L.; Holl, R.W.; Hoey, H.; Bjoerndalen, H.; De Beaufort, C.; Chiarelli, F.; Danne, T.; et al. New definition for the partial remission period in children and adolescents with type 1 diabetes. Diabetes Care 2009, 32, 1384–1390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitabchi, A.E.; Umpierrez, G.E.; Miles, J.M.; Fisher, J.N. Hyperglycemic crises in adult patients with diabetes. Diabetes Care 2009, 32, 1335–1343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saisho, Y. Postprandial C-Peptide to Glucose Ratio as a Marker of β Cell Function: Implication for the Management of Type 2 Diabetes. Int. J. Mol. Sci. 2016, 17, 744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caprio, M.; Infante, M.; Calanchini, M.; Mammi, C.; Fabbri, A. Vitamin D: Not just the bone. Evidence for beneficial pleiotropic extraskeletal effects. Eat Weight Disord. 2017, 22, 27–41. [Google Scholar] [CrossRef]
- Caprio, M.; Mammi, C.; Rosano, G.M. Vitamin D: A novel player in endothelial function and dysfunction. Arch. Med. Sci. 2012, 8, 4–5. [Google Scholar] [CrossRef]
- Maia Pinheiro, M.; Moura Maia Pinheiro, F.; Pires Amaral Resende, L.L.; Nogueira Diniz, S.; Fabbri, A.; Infante, M. Improvement of pure sensory mononeuritis multiplex and IgG1 deficiency with sitagliptin plus Vitamin D3. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 8151–8159. [Google Scholar]
- Maia Pinheiro, M.; Maia Pinheiro, F.M.; Amaral Resende, L.L.P.; Diniz, S.N.; Fabbri, A.; Infante, M. 36-month follow-up of a pure sensory mononeuritis multiplex and IgG1 deficiency improved after treatment with sitagliptin and Vitamin D3. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 1768–1769. [Google Scholar]
- Infante, M.; Sears, B.; Rizzo, A.M.; Mariani Cerati, D.; Caprio, M.; Ricordi, C.; Fabbri, A. Omega-3 PUFAs and vitamin D co-supplementation as a safe-effective therapeutic approach for core symptoms of autism spectrum disorder: Case report and literature review. Nutr. Neurosci. 2018, 23, 779–790. [Google Scholar] [CrossRef]
- Infante, M.; Ricordi, C.; Sanchez, J.; Clare-Salzler, M.J.; Padilla, N.; Fuenmayor, V.; Chavez, C.; Alvarez, A.; Baidal, D.; Alejandro, R.; et al. Influence of Vitamin D on Islet Autoimmunity and Beta-Cell Function in Type 1 Diabetes. Nutrients 2019, 11, 2185. [Google Scholar] [CrossRef] [Green Version]
- Federico, G.; Focosi, D.; Marchi, B.; Randazzo, E.; De Donno, M.; Vierucci, F.; Bugliani, M.; Campi, F.; Scatena, F.; Saggese, G.; et al. Administering 25-hydroxyvitamin D3 in vitamin D-deficient young type 1A diabetic patients reduces reactivity against islet autoantigens. Clin. Nutr. 2014, 33, 1153–1156. [Google Scholar] [CrossRef]
- Pinheiro, M.M.; Pinheiro, F.M.M.; Diniz, S.N.; Fabbri, A.; Infante, M. Combination of vitamin D and dipeptidyl peptidase-4 inhibitors (VIDPP-4i) as an immunomodulation therapy for autoimmune diabetes. Int. Immunopharmacol. 2021, 95, 107518. [Google Scholar] [CrossRef] [PubMed]
- Infante, M.; Buoso, A.; Pieri, M.; Lupisella, S.; Nuccetelli, M.; Bernardini, S.; Fabbri, A.; Iannetta, M.; Andreoni, M.; Colizzi, V.; et al. Low Vitamin D Status at Admission as a Risk Factor for Poor Survival in Hospitalized Patients With COVID-19: An Italian Retrospective Study. J. Am. Coll. Nutr. 2021, 41, 250–265. [Google Scholar] [CrossRef] [PubMed]
- Nogues, X.; Ovejero, D.; Pineda-Moncusí, M.; Bouillon, R.; Arenas, D.; Pascual, J.; Ribes, A.; Guerri-Fernandez, R.; Villar-Garcia, J.; Rial, A.; et al. Calcifediol Treatment and COVID-19–Related Outcomes. J. Clin. Endocrinol. Metab. 2021, 106, e4017–e4027. [Google Scholar] [CrossRef] [PubMed]
- Infante, M.; Pieri, M.; Lupisella, S.; D’Amore, L.; Bernardini, S.; Fabbri, A.; Morello, M. Low testosterone levels and high estradiol to testosterone ratio are associated with hyperinflammatory state and mortality in hospitalized men with COVID-19. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 5889–5903. [Google Scholar] [PubMed]
- Velikova, T.; Fabbri, A.; Infante, M. The role of vitamin D as a potential adjuvant for COVID-19 vaccines. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 5323–5327. [Google Scholar]
- Charoenngam, N.; Shirvani, A.; Holick, M.F. Vitamin D and Its Potential Benefit for the COVID-19 Pandemic. Endocr. Pract. 2021, 27, 484–493. [Google Scholar] [CrossRef]
- Infante, M.; Ricordi, C.; Baidal, D.A.; Alejandro, R.; Lanzoni, G.; Sears, B.; Fabbri, A. VITAL study: An incomplete picture? Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 3142–3147. [Google Scholar]
- Sourij, C.; Tripolt, N.J.; Aziz, F.; Aberer, F.; Forstner, P.; Obermayer, A.M.; Kojzar, H.; Kleinhappl, B.; Pferschy, P.N.; Mader, J.K.; et al. Humoral immune response to COVID-19 vaccination in diabetes is age-dependent but independent of type of diabetes and glycaemic control: The prospective COVAC-DM cohort study. Diabetes Obes. Metab. 2022, 24, 849–858. [Google Scholar] [CrossRef]
- Pieralice, S.; Monte, L.; Defeudis, G.; Tabacco, G.; Napoli, N.; Pozzilli, P. 677-P: Impact of Third Dose COVID-Vaccination on Glycaemic Control in Individuals with Type 1 Diabetes Using Flash Glucose Monitoring. Diabetes 2022, 71 (Suppl. 1), 677. [Google Scholar] [CrossRef]
- Cieślewicz, A.; Dudek, M.; Krela-Kaźmierczak, I.; Jabłecka, A.; Lesiak, M.; Korzeniowska, K. Pancreatic Injury after COVID-19 Vaccine-A Case Report. Vaccines 2021, 9, 576. [Google Scholar] [CrossRef]
- Parkash, O.; Sharko, A.; Farooqi, A.; Ying, G.W.; Sura, P. Acute Pancreatitis: A Possible Side Effect of COVID-19 Vaccine. Cureus 2021, 13, e14741. [Google Scholar] [CrossRef] [PubMed]
- Walter, T.; Connor, S.; Stedman, C.; Doogue, M. A case of acute necrotising pancreatitis following the second dose of Pfizer-BioNTech COVID-19 mRNA vaccine. Br. J. Clin. Pharmacol. 2022, 88, 1385–1386. [Google Scholar] [CrossRef] [PubMed]
- Eguchi, K.; Nagai, R. Islet inflammation in type 2 diabetes and physiology. J. Clin. Investig. 2017, 127, 14–23. [Google Scholar] [CrossRef] [Green Version]
- Infante, M.; Padilla, N.; Alejandro, R.; Caprio, M.; Della-Morte, D.; Fabbri, A.; Ricordi, C. Diabetes-Modifying Antirheumatic Drugs: The Roles of DMARDs as Glucose-Lowering Agents. Medicina 2022, 58, 571. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Fan, J.; Su, Q.; Yang, Z. Cytokines and Abnormal Glucose and Lipid Metabolism. Front. Endocrinol. 2019, 10, 703. [Google Scholar] [CrossRef] [PubMed]
- Rehman, K.; Akash, M.S. Mechanisms of inflammatory responses and development of insulin resistance: How are they interlinked? J. Biomed. Sci. 2016, 23, 87. [Google Scholar] [CrossRef] [Green Version]
- Shoelson, S.E.; Lee, J.; Goldfine, A.B. Inflammation and insulin resistance. J. Clin. Investig. 2006, 116, 1793–1801. [Google Scholar] [CrossRef]
- Edwards, A.E.; Vathenen, R.; Henson, S.M.; Finer, S.; Gunganah, K. Acute hyperglycaemic crisis after vaccination against COVID-19: A case series. Diabet. Med. 2021, 38, e14631. [Google Scholar] [CrossRef]
- Lee, H.J.; Sajan, A.; Tomer, Y. Hyperglycemic Emergencies Associated With COVID-19 Vaccination: A Case Series and Discussion. J. Endocr. Soc. 2021, 5, bvab141. [Google Scholar] [CrossRef]
- Mifsud, S.; Schembri, E.L.; Gruppetta, M. Stress-induced hyperglycaemia. Br. J. Hosp. Med. 2018, 79, 634–639. [Google Scholar] [CrossRef]
- Lager, I. The insulin-antagonistic effect of the counterregulatory hormones. J. Intern. Med. Suppl. 1991, 735, 41–47. [Google Scholar] [PubMed]
- Ganakumar, V.; Jethwani, P.; Roy, A.; Shukla, R.; Mittal, M.; Garg, M.K. Diabetic ketoacidosis (DKA) in type 1 diabetes mellitus (T1DM) temporally related to COVID-19 vaccination. Diabetes Metab. Syndr. 2022, 16, 102371. [Google Scholar] [CrossRef] [PubMed]
- Zilbermint, M.; Demidowich, A.P. Severe Diabetic Ketoacidosis after the Second Dose of mRNA-1273 COVID-19 Vaccine. J. Diabetes Sci. Technol. 2022, 16, 248–249. [Google Scholar] [CrossRef] [PubMed]
- Yakou, F.; Saburi, M.; Hirose, A.; Akaoka, H.; Hirota, Y.; Kobayashi, T.; Matsushita, T. A Case Series of Ketoacidosis after Coronavirus Disease 2019 Vaccination in Patients with Type 1 Diabetes. Front. Endocrinol. 2022, 13, 840580. [Google Scholar] [CrossRef] [PubMed]
- Sprague, J.E.; Arbeláez, A.M. Glucose counterregulatory responses to hypoglycemia. Pediatr. Endocrinol. Rev. 2011, 9, 463–473, quiz 74-5. [Google Scholar]
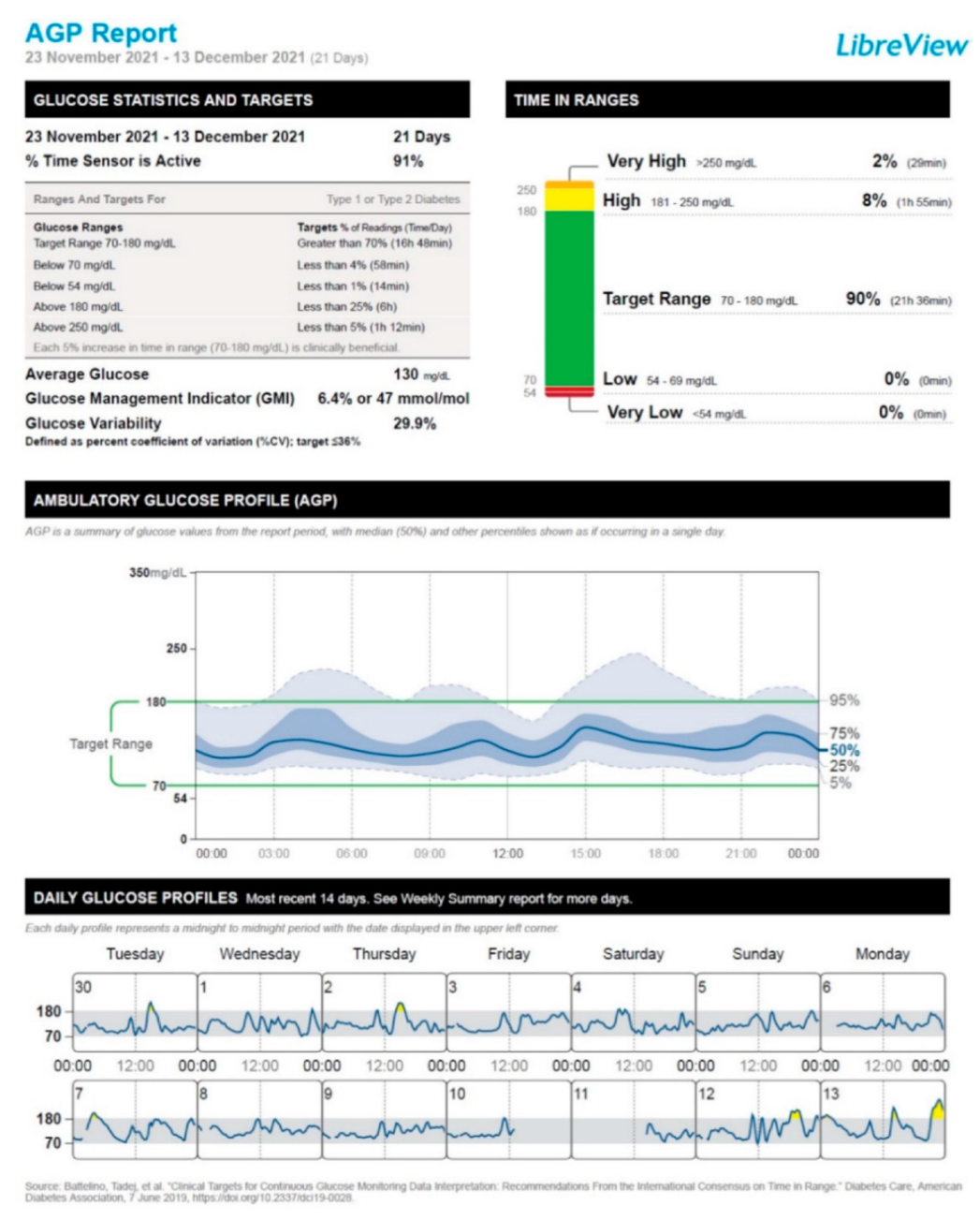
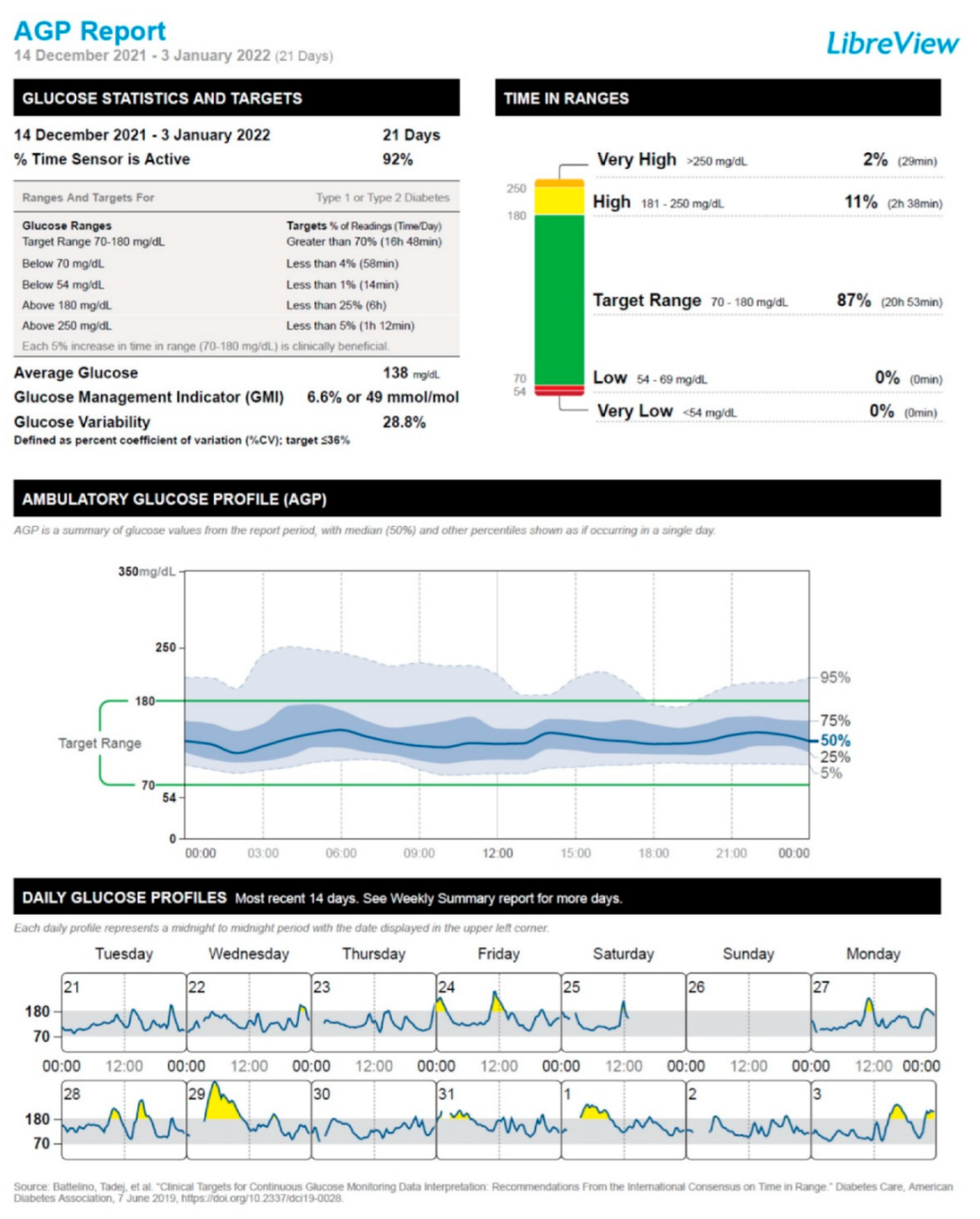
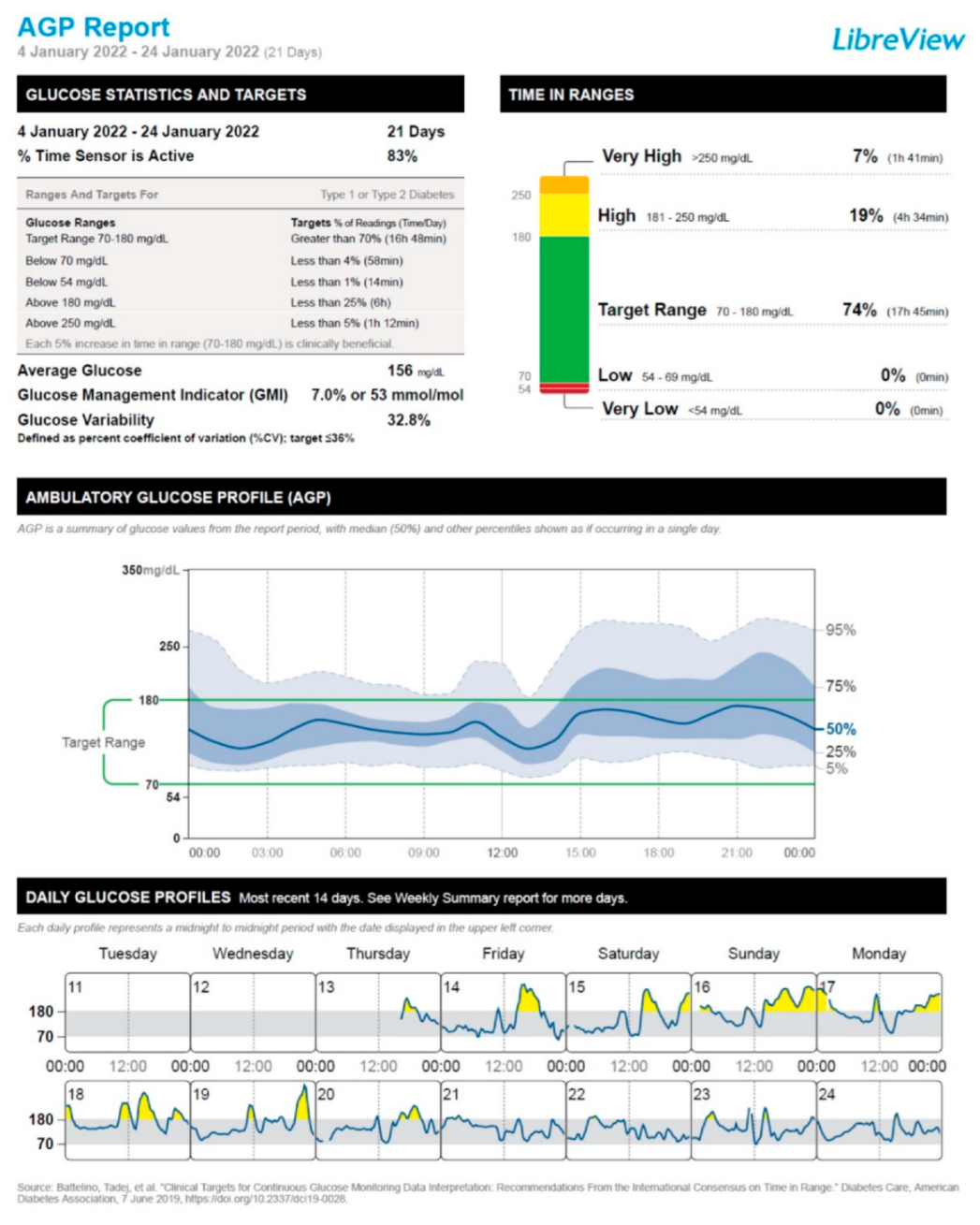
- Battelino, T.; Danne, T.; Bergenstal, R.M.; Amiel, S.A.; Beck, R.; Biester, T.; Bosi, E.; Buckingham, B.A.; Cefalu, W.T.; Close, K.L.; et al. Clinical Targets for Continuous Glucose Monitoring Data Interpretation: Recommendations From the International Consensus on Time in Range. Diabetes Care 2019, 42, 1593–1603. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Xu, Z.; Wang, P.; Li, X.M.; Shuai, Z.W.; Ye, D.Q.; Pan, H.F. New-onset autoimmune phenomena post-COVID-19 vaccination. Immunology 2022, 165, 386–401. [Google Scholar] [CrossRef]
- Patrizio, A.; Ferrari, S.M.; Antonelli, A.; Fallahi, P. A case of Graves’ disease and type 1 diabetes mellitus following SARS-CoV-2 vaccination. J. Autoimmun. 2021, 125, 102738. [Google Scholar] [CrossRef]
- Taieb, A.; Sawsen, N.; Asma, B.A.; Ghada, S.; Hamza, E.; Yosra, H.; Koussay, A. A rare case of grave’s disease after SARS-CoV-2 vaccine: Is it an adjuvant effect? Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 2627–2630. [Google Scholar]
- Tang, X.; He, B.; Liu, Z.; Zhou, Z.; Li, X. Fulminant type 1 diabetes after COVID-19 vaccination. Diabetes Metab. 2022, 48, 101324. [Google Scholar] [CrossRef]
- Sakurai, K.; Narita, D.; Saito, N.; Ueno, T.; Sato, R.; Niitsuma, S.; Arihara, Z. Type 1 diabetes mellitus following COVID-19 RNA-based vaccine. J. Diabetes Investig. 2022, 13, 1290–1292. [Google Scholar] [CrossRef] [PubMed]
- Yano, M.; Morioka, T.; Natsuki, Y.; Sasaki, K.; Kakutani, Y.; Ochi, A.; Yamazaki, Y.; Shoji, T.; Emoto, M. New-onset Type 1 Diabetes after COVID-19 mRNA Vaccination. Intern. Med. 2022, 61, 1197–1200. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, H.; Itoh, A.; Watanabe, Y.; Nakajima, Y.; Saisho, Y.; Irie, J.; Meguro, S.; Itoh, H. Newly developed type 1 diabetes after coronavirus disease 2019 vaccination: A case report. J. Diabetes Investig. 2022, 13, 1105–1108. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, H.; Itoh, A.; Itoh, H. Could the development of COVID-19 vaccine-induced type 1 diabetes be explained by a simple mechanism? Diabetes Metab. 2022, 48, 101338. [Google Scholar] [CrossRef]
- Shirakawa, J. Pancreatic β-cell fate in subjects with COVID-19. J. Diabetes Investig. 2021, 12, 2126–2128. [Google Scholar] [CrossRef]
- Fignani, D.; Licata, G.; Brusco, N.; Nigi, L.; Grieco, G.E.; Marselli, L.; Dotta, F. SARS-CoV-2 Receptor Angiotensin I-Converting Enzyme Type 2 (ACE2) Is Expressed in Human Pancreatic. Front. Endocrinol. 2020, 11, 596898. [Google Scholar] [CrossRef]
- Pietropaolo, M.; Hotez, P.; Giannoukakis, N. Incidence of an Insulin-Requiring Hyperglycemic Syndrome in SARS CoV-2-Infected Young Individuals: Is it Type 1 Diabetes? Diabetes 2022. Online ahead of print. [Google Scholar] [CrossRef]
- Montefusco, L.; Bolla, A.M.; Fiorina, P. Should we expect a wave of type 1 diabetes following SARS-CoV-2 pandemic? Diabetes Metab. Res. Rev. 2022, 38, e3529. [Google Scholar] [CrossRef]
- de Sá-Ferreira, C.O.; da Costa, C.H.M.; Guimarães, J.C.W.; Sampaio, N.S.; Silva, L.D.; de Mascarenhas, L.P.; Young, E.C. Diabetic ketoacidosis and COVID-19: What have we learned so far? Am. J. Physiol. Endocrinol. Metab. 2022, 322, E44–E53. [Google Scholar] [CrossRef]
- Teijaro, J.R.; Farber, D.L. COVID-19 vaccines: Modes of immune activation and future challenges. Nat. Rev. Immunol. 2021, 21, 195–197. [Google Scholar] [CrossRef]
- Rickels, M.R.; Evans-Molina, C.; Bahnson, H.T.; Ylescupidez, A.; Nadeau, K.J.; Hao, W.; Clements, M.A.; Sherr, J.L.; Pratley, R.E.; Hannon, T.S.; et al. High residual C-peptide likely contributes to glycemic control in type 1 diabetes. J. Clin. Investig. 2020, 130, 1850–1862. [Google Scholar] [CrossRef] [PubMed]
- Scoccimarro, D.; Panichi, L.; Ragghianti, B.; Silverii, A.; Mannucci, E.; Monami, M. SARS-CoV2 vaccine hesitancy in Italy: A survey on subjects with diabetes. Nutr. Metab. Cardiovasc Dis. 2021, 31, 3243–3246. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Duan, L.; Li, M.; Wang, J.; Yang, J.; Song, C.; Li, J.; Wang, J.; Jia, J.; Xu, J. COVID-19 Vaccine Hesitancy and Associated Factors among Diabetes Patients: A Cross-Sectional Survey in Changzhi, Shanxi, China. Vaccines 2022, 10, 129. [Google Scholar] [CrossRef] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Infante, M.; Fabbri, A.; Padilla, N.; Pacifici, F.; Di Perna, P.; Vitiello, L.; Feraco, A.; Giuliano, M.; Passeri, M.; Caprio, M.; et al. BNT162b2 mRNA COVID-19 Vaccine Does Not Impact the Honeymoon Phase in Type 1 Diabetes: A Case Report. Vaccines 2022, 10, 1096. https://doi.org/10.3390/vaccines10071096
Infante M, Fabbri A, Padilla N, Pacifici F, Di Perna P, Vitiello L, Feraco A, Giuliano M, Passeri M, Caprio M, et al. BNT162b2 mRNA COVID-19 Vaccine Does Not Impact the Honeymoon Phase in Type 1 Diabetes: A Case Report. Vaccines. 2022; 10(7):1096. https://doi.org/10.3390/vaccines10071096
Chicago/Turabian StyleInfante, Marco, Andrea Fabbri, Nathalia Padilla, Francesca Pacifici, Pasquale Di Perna, Laura Vitiello, Alessandra Feraco, Maria Giuliano, Marina Passeri, Massimiliano Caprio, and et al. 2022. "BNT162b2 mRNA COVID-19 Vaccine Does Not Impact the Honeymoon Phase in Type 1 Diabetes: A Case Report" Vaccines 10, no. 7: 1096. https://doi.org/10.3390/vaccines10071096