
Durability of Humoral and Cellular Immunity after an Extended Primary Series with Heterologous Inactivated SARS-CoV-2 Prime-Boost and ChAdOx1 nCoV-19 in Dialysis Patients (ICON3)

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
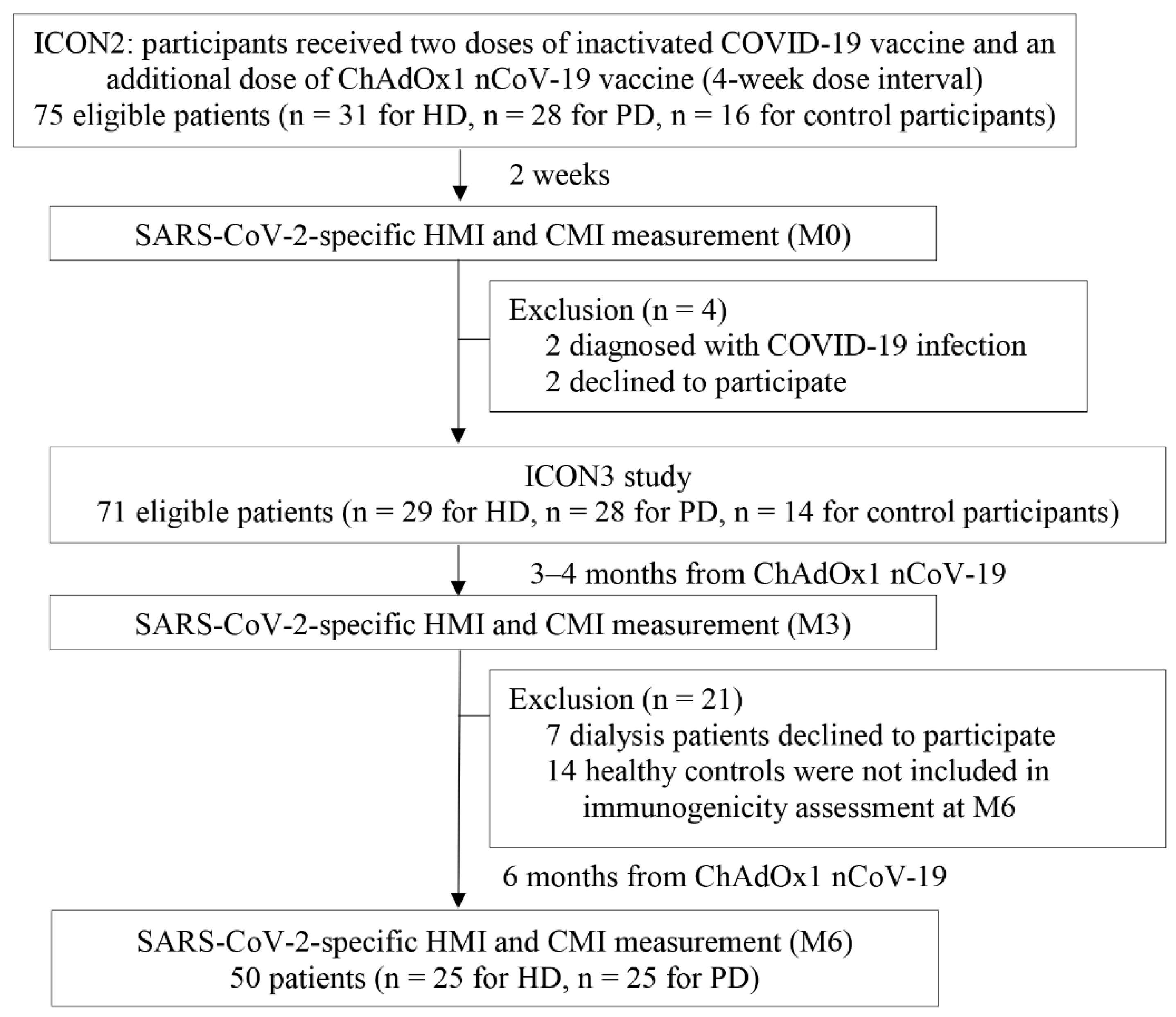
2.1. Study Design
2.2. SARS-CoV-2-Specific Humoral Immunity
2.3. SARS-CoV-2-Specific Cell-Mediated Immunity
2.4. Statistical Analyses
3. Results
3.1. Participant Clinical Characteristics
3.2. SARS-CoV-2-Specific MHI
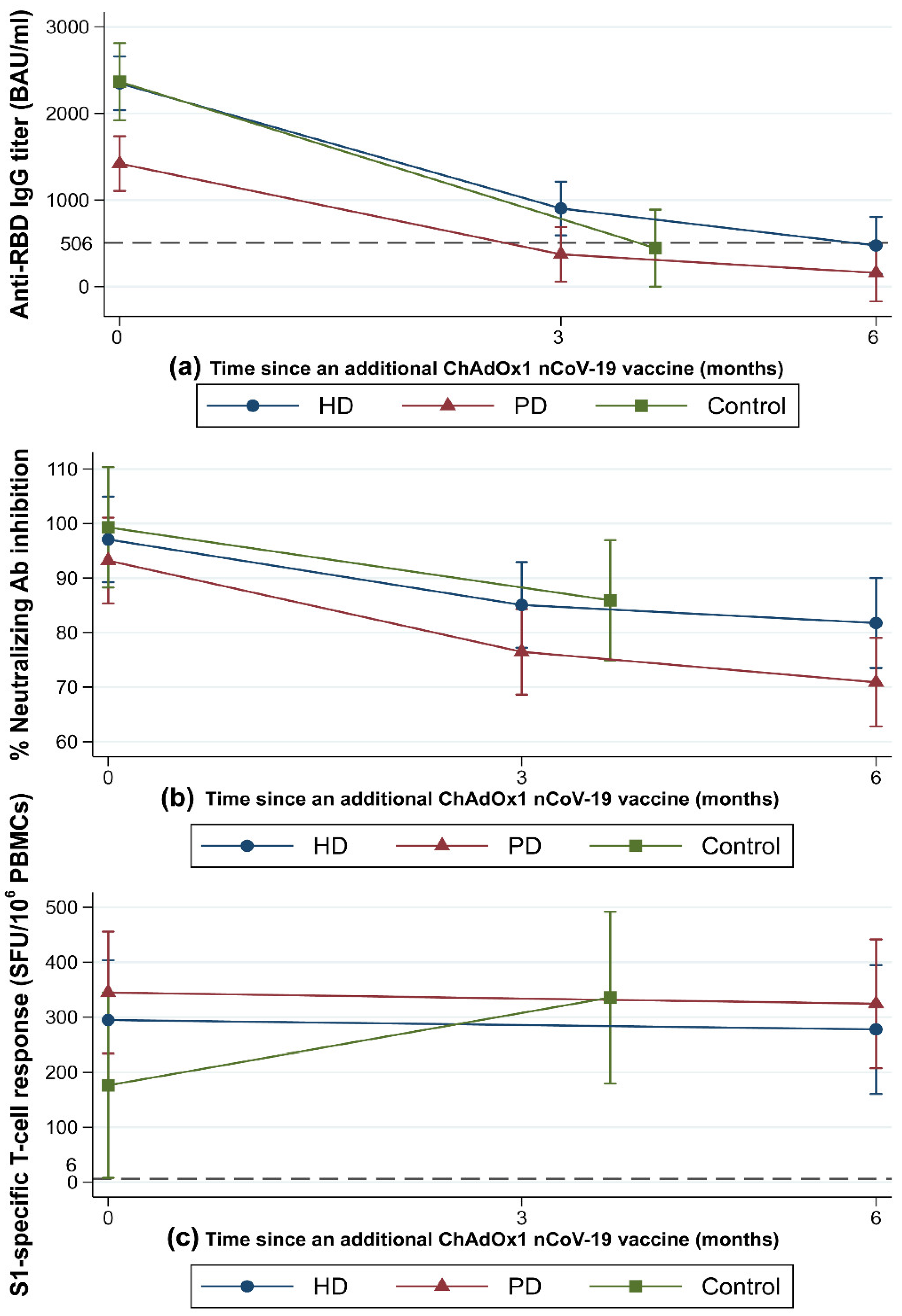
3.2.1. Anti-RBD IgG
3.2.2. Neutralizing Antibody
3.2.3. Predictors of Early Loss of Anti-RBD IgG Seroprotection Status among Dialysis Patients at M3
3.3. SARS-CoV-2-Specific CMI
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Couchoud, C.; Bayer, F.; Ayav, C.; Bechade, C.; Brunet, P.; Chantrel, F.; Frimat, L.; Galland, R.; Hourmant, M.; Laurain, E.; et al. Low incidence of SARS-CoV-2, risk factors of mortality and the course of illness in the French national cohort of dialysis patients. Kidney Int. 2020, 98, 1519–1529. [Google Scholar] [CrossRef] [PubMed]
- Jager, K.J.; Kramer, A.; Chesnaye, N.C.; Couchoud, C.; Sánchez-Álvarez, J.E.; Garneata, L.; Collart, F.; Hemmelder, M.H.; Ambühl, P.; Kerschbaum, J. Results from the ERA-EDTA Registry indicate a high mortality due to COVID-19 in dialysis patients and kidney transplant recipients across Europe. Kidney Int. 2020, 98, 1540–1548. [Google Scholar] [CrossRef] [PubMed]
- El Karoui, K.; Hourmant, M.; Ayav, C.; Glowacki, F.; Couchoud, C.; Lapidus, N.; Registry, R. Vaccination and COVID-19 Dynamics in Dialysis Patients. Clin. J. Am. Soc. Nephrol. 2022, 17, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Van Praet, J.; Reynders, M.; de Bacquer, D.; Viaene, L.; Schoutteten, M.K.; Caluwe, R.; Doubel, P.; Heylen, L.; de Bel, A.V.; van Vlem, B.; et al. Predictors and Dynamics of the Humoral and Cellular Immune Response to SARS-CoV-2 mRNA Vaccines in Hemodialysis Patients: A Multicenter Observational Study. J. Am. Soc. Nephrol. 2021, 32, 12. [Google Scholar] [CrossRef]
- Seija, M.; Rammauro, F.; Santiago, J.; Orihuela, N.; Zulberti, C.; Machado, D.; Recalde, C.; Noboa, J.; Frantchez, V.; Astesiano, R.; et al. Comparison of antibody response to SARS-CoV-2 after two doses of inactivated virus and BNT162b2 mRNA vaccines in kidney transplant. Clin. Kidney J. 2022, 15, 527–533. [Google Scholar] [CrossRef]
- Boongird, S.; Chuengsaman, P.; Setthaudom, C.; Nongnuch, A.; Assanatham, M.; Phanprasert, S.; Kitpermkiat, R.; Kiertiburanakul, S.; Malathum, K.; Phuphuakrat, A.; et al. Short-Term Immunogenicity Profiles and Predictors for Suboptimal Immune Responses in Patients with End-Stage Kidney Disease Immunized with Inactivated SARS-CoV-2 Vaccine. Infect. Dis. Ther. 2022, 11, 351–365. [Google Scholar] [CrossRef]
- Carr, E.J.; Wu, M.; Harvey, R.; Wall, E.C.; Kelly, G.; Hussain, S.; Howell, M.; Kassiotis, G.; Swanton, C.; Gandhi, S.; et al. Neutralising antibodies after COVID-19 vaccination in UK haemodialysis patients. Lancet 2021, 398, 1038–1041. [Google Scholar] [CrossRef]
- Speer, C.; Goth, D.; Benning, L.; Buylaert, M.; Schaier, M.; Grenz, J.; Nusshag, C.; Kalble, F.; Kreysing, M.; Reichel, P.; et al. Early Humoral Responses of Hemodialysis Patients after COVID-19 Vaccination with BNT162b2. Clin. J. Am. Soc. Nephrol 2021, 16, 1073–1082. [Google Scholar] [CrossRef]
- Interim Recommendations for an Extended Primary Series with an Additional Vaccine Dose for COVID-19 Vaccination in Immunocompromised Persons. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-vaccines-SAGE_recommendation-immunocompromised-persons (accessed on 26 October 2021).
- Bruminhent, J.; Setthaudom, C.; Kitpermkiat, R.; Kiertiburanakul, S.; Malathum, K.; Assanatham, M.; Nongnuch, A.; Phuphuakrat, A.; Chaumdee, P.; Janphram, C.; et al. Immunogenicity of ChAdOx1 nCoV-19 vaccine after a two-dose inactivated SARS-CoV-2 vaccination of dialysis patients and kidney transplant recipients. Sci. Rep. 2022, 12, 3587. [Google Scholar] [CrossRef]
- Bensouna, I.; Caudwell, V.; Kubab, S.; Acquaviva, S.; Pardon, A.; Vittoz, N.; Bozman, D.F.; Hanafi, L.; Faucon, A.L.; Housset, P. SARS-CoV-2 Antibody Response After a Third Dose of the BNT162b2 Vaccine in Patients Receiving Maintenance Hemodialysis or Peritoneal Dialysis. Am. J. Kidney Dis. 2022, 79, 185–192.e1. [Google Scholar] [CrossRef]
- Thompson, M.G.; Natarajan, K.; Irving, S.A.; Rowley, E.A.; Griggs, E.P.; Gaglani, M.; Klein, N.P.; Grannis, S.J.; DeSilva, M.B.; Stenehjem, E.; et al. Effectiveness of a Third Dose of mRNA Vaccines Against COVID-19-Associated Emergency Department and Urgent Care Encounters and Hospitalizations among Adults During Periods of Delta and Omicron Variant Predominance-VISION Network, 10 States, August 2021–January 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 139–145. [Google Scholar] [PubMed]
- Atmar, R.L.; Lyke, K.E.; Deming, M.E.; Jackson, L.A.; Branche, A.R.; El Sahly, H.M.; Rostad, C.A.; Martin, J.M.; Johnston, C.; Rupp, R.E.; et al. Homologous and Heterologous COVID-19 Booster Vaccinations. N. Engl. J. Med. 2022, 386, 1046–1057. [Google Scholar] [CrossRef] [PubMed]
- Ferdinands, J.M.; Rao, S.; Dixon, B.E.; Mitchell, P.K.; DeSilva, M.B.; Irving, S.A.; Lewis, N.; Natarajan, K.; Stenehjem, E.; Grannis, S.J.; et al. Waning 2-Dose and 3-Dose Effectiveness of mRNA Vaccines Against COVID-19-Associated Emergency Department and Urgent Care Encounters and Hospitalizations Among Adults During Periods of Delta and Omicron Variant Predominance-VISION Network, 10 States, August 2021–January 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 255–263. [Google Scholar] [PubMed]
- Anand, S.; Montez-Rath, M.E.; Han, J.; Garcia, P.; Cadden, L.; Hunsader, P.; Morgan, C.; Kerschmann, R.; Beyer, P.; Dittrich, M.; et al. SARS-CoV-2 Vaccine Antibody Response and Breakthrough Infection in Patients Receiving Dialysis. Ann. Intern. Med. 2022, 175, 371–378. [Google Scholar] [CrossRef]
- Davidovic, T.; Schimpf, J.; Abbassi-Nik, A.; Stockinger, R.; Sprenger-Mahr, H.; Lhotta, K.; Zitt, E. Waning humoral response 6 months after SARS-CoV-2 vaccination with the mRNA-BNT162b2 vaccine in hemodialysis patients: Time for a boost. Kidney Int. 2021, 100, 1334–1335. [Google Scholar] [CrossRef]
- Dheir, H.; Tocoglu, A.; Toptan, H.; Pinar, M.; Demirci, T.; Koroglu, M.; Yaylaci, S.; Genc, A.B.; Genc, A.C.; Firat, N.; et al. Short and mid-term SARS-CoV-2 antibody response after inactivated COVID-19 vaccine in hemodialysis and kidney transplant patients. J. Med. Virol. 2022, 94, 3176–3183. [Google Scholar] [CrossRef]
- Chew, K.L.; Tan, S.S.; Saw, S.; Pajarillaga, A.; Zaine, S.; Khoo, C.; Wang, W.; Tambyah, P.; Jureen, R.; Sethi, S.K. Clinical evaluation of serological IgG antibody response on the Abbott Architect for established SARS-CoV-2 infection. Clin. Microbiol. Infect. 2020, 26, 1256.e9–1256.e11. [Google Scholar] [CrossRef]
- Abbott Core Laboratory. Abbott Architect i SARS-CoV-2 IgG II Quant Reagent Instructions for Use. Available online: https://www.corelaboratory.abbott/int/en/offerings/segments/infectious-disease/sars-cov-2- (accessed on 12 April 2022).
- Feng, S.; Phillips, D.J.; White, T.; Sayal, H.; Aley, P.K.; Bibi, S.; Dold, C.; Fuskova, M.; Gilbert, S.C.; Hirsch, I.; et al. Correlates of protection against symptomatic and asymptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 2032–2040. [Google Scholar] [CrossRef]
- Coronavirus Diagnostics by Euroimmun. SARS-CoV-2 NeutraLISA. Available online: https://www.coronavirus-diagnostics.com/documents/Indications/Infections/Coronavirus/EI_2606_D_UK_F.pdf (accessed on 12 April 2022).
- Tan, C.W.; Chia, W.N.; Qin, X.; Liu, P.; Chen, M.I.; Tiu, C.; Hu, Z.; Chen, V.C.; Young, B.E.; Sia, W.R.; et al. A SARS-CoV-2 surrogate virus neutralization test based on antibody-mediated blockage of ACE2-spike protein-protein interaction. Nat. Biotechnol. 2020, 38, 1073–1078. [Google Scholar] [CrossRef]
- Bruminhent, J.; Setthaudom, C.; Chaumdee, P.; Boongird, S.; Kiertiburanakul, S.; Malathum, K.; Nongnuch, A.; Phuphuakrat, A.; Jirasiritham, S.; Janphram, C.; et al. SARS-CoV-2-specific humoral and cell-mediated immune responses after immunization with inactivated COVID-19 vaccine in kidney transplant recipients (CVIM 1 study). Am. J. Transpl. 2022, 22, 813–822. [Google Scholar] [CrossRef]
- Package Insert. T-SPOT.COVID. Available online: https://www.tspotcovid.com/wp-content/uploads/sites/5/2021/03/PI-T-SPOT.COVID-IVD-UK-v3.pdf (accessed on 12 April 2022).
- Schwarzkopf, S.; Krawczyk, A.; Knop, D.; Klump, H.; Heinold, A.; Heinemann, F.M.; Thummler, L.; Temme, C.; Breyer, M.; Witzke, O.; et al. Cellular Immunity in COVID-19 Convalescents with PCR-Confirmed Infection but with Undetectable SARS-CoV-2-Specific IgG. Emerg. Infect. Dis. 2021, 27, 122–129. [Google Scholar] [CrossRef]
- Angel-Korman, A.; Peres, E.; Bryk, G. Diminished and waning immunity to COVID-19 vaccination among hemodialysis patients in Israel: The case for a third vaccine dose. Clin. Kidney J. 2021, 15, 226–234. [Google Scholar] [CrossRef] [PubMed]
- De Vriese, A.S.; van Praet, J.; Reynders, M.; Heylen, L.; Viaene, L.; Caluwe, R.; Schoutteten, M.; de Bacquer, D. Longevity and clinical effectiveness of the humoral and cellular response to SARS-CoV-2 vaccination in hemodialysis patients. Kidney Int. Rep. 2022, 7, 1103–1107. [Google Scholar] [CrossRef]
- Anand, S.; Montez-Rath, M.E.; Han, J.; Garcia, P.; Cadden, L.; Hunsader, P.; Kerschmann, R.; Beyer, P.; Dittrich, M.; Block, G.A.; et al. Antibody Response to COVID-19 Vaccination in Patients Receiving Dialysis. J. Am. Soc. Nephrol. 2021, 32, 2435–2438. [Google Scholar] [CrossRef]
- Hsu, C.M.; Weiner, D.E.; Aweh, G.N.; Manley, H.J.; Ladik, V.; Frament, J.; Miskulin, D.; Argyropoulos, C.; Abreo, K.; Chin, A.; et al. Seroresponse to SARS-CoV-2 Vaccines Among Maintenance Dialysis Patients. Am. J. Kidney Dis. 2022, 79, 307–310. [Google Scholar] [CrossRef] [PubMed]
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R.; Asraf, K.; Mendelson, E.; Ziv, A.; et al. Waning Immune Humoral Response to BNT162b2 COVID-19 Vaccine over 6 Months. N. Engl. J. Med. 2021, 385, e84. [Google Scholar] [CrossRef]
- Speer, C.; Schaier, M.; Nusshag, C.; Tollner, M.; Buylaert, M.; Kalble, F.; Reichel, P.; Grenz, J.; Susal, C.; Zeier, M.; et al. Longitudinal Humoral Responses after COVID-19 Vaccination in Peritoneal and Hemodialysis Patients over Twelve Weeks. Vaccines 2021, 9, 1130. [Google Scholar] [CrossRef]
- Nacasch, N.; Cohen-Hagai, K.; Benchetrit, S.; Zitman-Gal, T.; Einbinder, Y.; Erez, D.; Hornik-Lurie, T.; Goldman, S.; Tanasiychuk, T.; Frajewicki, V.; et al. Comparison of long-term antibody response to mRNA SARS-CoV-2 vaccine among peritoneal dialysis and hemodialysis patients. Nephrol. Dial. Transpl. 2022, 37, 602–604. [Google Scholar] [CrossRef]
- Ghamar-Chehreh, M.E.; Agah, S.; Khedmat, H.; Aghaei, A.; Alavian, S.M. Serum albumin level as an indicator of response to Hepatitis B vaccination in dialysis patients: A systematic review and meta-analysis. Casp. J. Intern. Med. 2017, 8, 250–257. [Google Scholar]
- COVID-19 Vaccines for Moderately or Severely Immunocompromised People. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations/immuno.html (accessed on 12 April 2022).
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Boedecker-Lips, S.C.; Lautem, A.; Runkel, S.; Klimpke, P.; Kraus, D.; Keil, P.; Holtz, S.; Tomalla, V.; Marczynski, P.; Boedecker, C.B.; et al. Six-Month Follow-Up after Vaccination with BNT162b2: SARS-CoV-2 Antigen-Specific Cellular and Humoral Immune Responses in Hemodialysis Patients and Kidney Transplant Recipients. Pathogens 2022, 11, 67. [Google Scholar] [CrossRef] [PubMed]
- Primorac, D.; Brlek, P.; Matisic, V.; Molnar, V.; Vrdoljak, K.; Zadro, R.; Parcina, M. Cellular Immunity-The Key to Long-Term Protection in Individuals Recovered from SARS-CoV-2 and after Vaccination. Vaccines 2022, 10, 442. [Google Scholar] [CrossRef] [PubMed]
- Mazzoni, A.; di Lauria, N.; Maggi, L.; Salvati, L.; Vanni, A.; Capone, M.; Lamacchia, G.; Mantengoli, E.; Spinicci, M.; Zammarchi, L.; et al. First-dose mRNA vaccination is sufficient to reactivate immunological memory to SARS-CoV-2 in subjects who have recovered from COVID-19. J. Clin. Invest. 2021, 131, 12. [Google Scholar]
- Pozzetto, B.; Legros, V.; Djebali, S.; Barateau, V.; Guibert, N.; Villard, M.; Peyrot, L.; Allatif, O.; Fassier, J.B.; Massardier-Pilonchery, A.; et al. Immunogenicity and efficacy of heterologous ChAdOx1-BNT162b2 vaccination. Nature 2021, 600, 701–706. [Google Scholar] [CrossRef]
- Stuart, A.S.V.; Shaw, R.H.; Liu, X.; Greenland, M.; Aley, P.K.; Andrews, N.J.; Cameron, J.C.; Charlton, S.; Clutterbuck, E.A.; Collins, A.M.; et al. Immunogenicity, safety, and reactogenicity of heterologous COVID-19 primary vaccination incorporating mRNA, viral-vector, and protein-adjuvant vaccines in the UK (Com-COV2): A single-blind, randomised, phase 2, non-inferiority trial. Lancet 2022, 399, 36–49. [Google Scholar] [CrossRef]
- Moss, P. The T cell immune response against SARS-CoV-2. Nat. Immunol. 2022, 23, 186–193. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Demographic Data n (%) or Mean (SD) | HD (n = 29) | PD (n = 28) | Controls (n = 14) | p-Value |
|---|---|---|---|---|
| Age [years], mean (SD) | 44.3 (9.7) | 41.0 (11.5) | 43.6 (8.0) | 0.46 |
| Male sex, n (%) | 22 (76%) * | 17 (61%) | 5 (36%) | 0.04 |
| Body mass index [kg/m2], mean (SD) | 25.4 (5.2) | 23.6 (4.4) | 26.5 (6.1) | 0.20 |
| Age-adjusted Charlson Comorbidity Index, median (IQR) | 3 (3–5) | 2.5 (2–4) | N/A | 0.06 |
| Comorbidities, n (%) | ||||
| Diabetes mellitus | 13 (45%) * | 7 (25%) | 1 (8%) | 0.05 a |
| Hypertension | 22 (76%) * | 25 (89%) * | 2 (17%) | <0.01 a |
| Dyslipidemia | 11 (38%) | 9 (32%) | 4 (33%) | 0.94 a |
| Ischemic heart disease | 7 (24%) | 2 (7%) | 0 (0%) | 0.07 |
| Etiologies of ESKD, n (%) | 0.15 | |||
| Diabetes | 6 (21%) | 5 (18%) | N/A | |
| Hypertension | 3 (10%) | 8 (29%) | N/A | |
| Chronic glomerulonephritis | 5 (17%) | 7 (25%) | N/A | |
| Other | 3 (10%) | 0 (0%) | N/A | |
| Unknown | 12 (41%) | 7 (25%) | N/A | |
| Immunosuppressive drugs | 0 (0%) | 1 (3%) | 0 (0) | |
| Dialysis vintage, months, median (IQR) | 32.6 (19.0–83.5) | 34.1 (7.2–57.2) | N/A | 0.18 |
| Total Kt/Vurea | 1.6 (0.3%) | 2.0 (0.4%) | N/A | N/A |
| Anuria, n (%) | 16 (55%) | 9 (32%) | N/A | 0.04 |
| Smoking, n (%) | 13 (45%) | 10 (36%) | 0 (0) | 0.60 |
| Baseline lab results | ||||
| White blood cell count [×109 cells/L], mean (SD) | 7.0 (1.9) | 7.3 (2.8) | 7.8 (2.7) b | 0.69 |
| Absolute lymphocyte count [×109 cells/L], mean (SD) | 1.6 (0.5) * | 1.5 (0.8) * | 2.3 (0.9) b | 0.03 |
| Hemoglobin [g/dL], mean (SD) | 11.1 (2.1) * | 10.0 (2.3) * | 13.5 (1.1) b | <0.01 |
| Calcium [mg/dL], mean (SD) | 8.8 (1.0) | 8.6 (1.0) | N/A | 0.45 |
| Phosphorus [mg/dL], mean (SD) | 5.5 (1.9) | 5.4 (1.9) | N/A | 0.87 |
| Albumin [g/L], mean (SD) | 40.1 (4.3) | 33.1 (4.1) | N/A | <0.001 |
| Ferritin [ng/mL], median (IQR) | 304 (119–441) | 367 (156–751) | N/A | 0.04 |
| Time interval between vaccination and immunogenicity evaluation | ||||
| Time interval from M0 to M3 [months], mean (SD) | 3.5 (0.2) * | 3.4 (0.2) * | 4.2 (0.3) | <0.01 |
| Time interval from M0 to M6 [months], mean (SD) | 6.6 (0.3) c | 6.4 (0.3) c | N/A | 0.28 |
| Variable n (%) or Mean (SD) | Anti-RBD IgG Titer ≥ 506 BAU/mL at M3 (Seroprotection) (n = 26) | Anti-RBD IgG Titer < 506 BAU/mL at M3 (Non-Sero Protection) (n = 31) | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|---|---|
| OR (95%CI) | p-Value | OR (95%CI) | p-Value | |||
| Age [years], mean (SD) | 39.6 (9.2) | 45.3 (11.3) | 1.05 (1.00–1.11) | 0.05 | 1.10 (1.02–1.18) | 0.01 |
| Peritoneal dialysis, n (%) | 9 (35%) | 19 (61%) | 2.99 (1.01–8.84) | 0.05 | 5.23 (0.87–31.50) | 0.07 |
| Dialysis duration [months], median (IQR) | 45.0 (25.0–85.1) | 32.0 (7.46–53.3) | 0.98 (0.98–1.00) | 0.06 | 0.99 (0.98–1.00) | 0.15 |
| Anti-RBD IgG titer at M0 [BAU/mL], mean (SD) Tertile 1 (ref.) Tertile 2 Tertile 3 | 2216 (1540–4172) 1045 (89) 1746 (328) 4336 (820) | 1010 (510–1364) 612 (320) 1490 (419) 2658 (171) | 1.0 0.17 (0.04–0.70) 0.07 (0.15–0.34) | 0.01 <0.01 | 1.0 0.15 (0.03–0.77) 0.06 (0.01–0.38) | 0.02 <0.01 |
| Number(s) of patients with an absolute lymphocyte count of ≥1.5 × 109 cells/L, n (%) | 15 (58%) | 15 (48%) | 0.69 (0.24–1.96) | 0.48 | ||
| Albumin [g/L], mean (SD) | 37.7 (5.6) | 35.9 (5.4) | 0.94 (0.85–1.04) | 0.23 | 1.10 (0.94–1.30) | 0.23 |
| Number(s) of patients with serum ferritin of ≥500 ng/mL, n (%) | 5 (19%) | 10 (32%) | 2.0 (0.58–6.86) | 0.27 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boongird, S.; Setthaudom, C.; Kitpermkiat, R.; Prasongtanakij, S.; Srisala, S.; Chuengsaman, P.; Nongnuch, A.; Assanatham, M.; Kiertiburanakul, S.; Malathum, K.; et al. Durability of Humoral and Cellular Immunity after an Extended Primary Series with Heterologous Inactivated SARS-CoV-2 Prime-Boost and ChAdOx1 nCoV-19 in Dialysis Patients (ICON3). Vaccines 2022, 10, 1064. https://doi.org/10.3390/vaccines10071064
Boongird S, Setthaudom C, Kitpermkiat R, Prasongtanakij S, Srisala S, Chuengsaman P, Nongnuch A, Assanatham M, Kiertiburanakul S, Malathum K, et al. Durability of Humoral and Cellular Immunity after an Extended Primary Series with Heterologous Inactivated SARS-CoV-2 Prime-Boost and ChAdOx1 nCoV-19 in Dialysis Patients (ICON3). Vaccines. 2022; 10(7):1064. https://doi.org/10.3390/vaccines10071064
Chicago/Turabian StyleBoongird, Sarinya, Chavachol Setthaudom, Rungthiwa Kitpermkiat, Somsak Prasongtanakij, Supanart Srisala, Piyatida Chuengsaman, Arkom Nongnuch, Montira Assanatham, Sasisopin Kiertiburanakul, Kumthorn Malathum, and et al. 2022. "Durability of Humoral and Cellular Immunity after an Extended Primary Series with Heterologous Inactivated SARS-CoV-2 Prime-Boost and ChAdOx1 nCoV-19 in Dialysis Patients (ICON3)" Vaccines 10, no. 7: 1064. https://doi.org/10.3390/vaccines10071064