
Differential Dynamics of Humoral and Cell-Mediated Immunity with Three Doses of BNT162b2 SARS-CoV-2 Vaccine in Healthcare Workers in Japan: A Prospective Cohort Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Cohort, Design, and Sample Processing
2.2. Detection of SARS-CoV-2 Specific Antibodies
2.3. Detection of Neutralizing Antibodies against SARS-CoV-2
2.4. Detection of Cell-Mediated Immunity against SARS-CoV-2
2.5. Other Laboratory Testing
2.6. Statistical Analysis
3. Results
3.1. Demographic and Clinical Data of the Study Participants
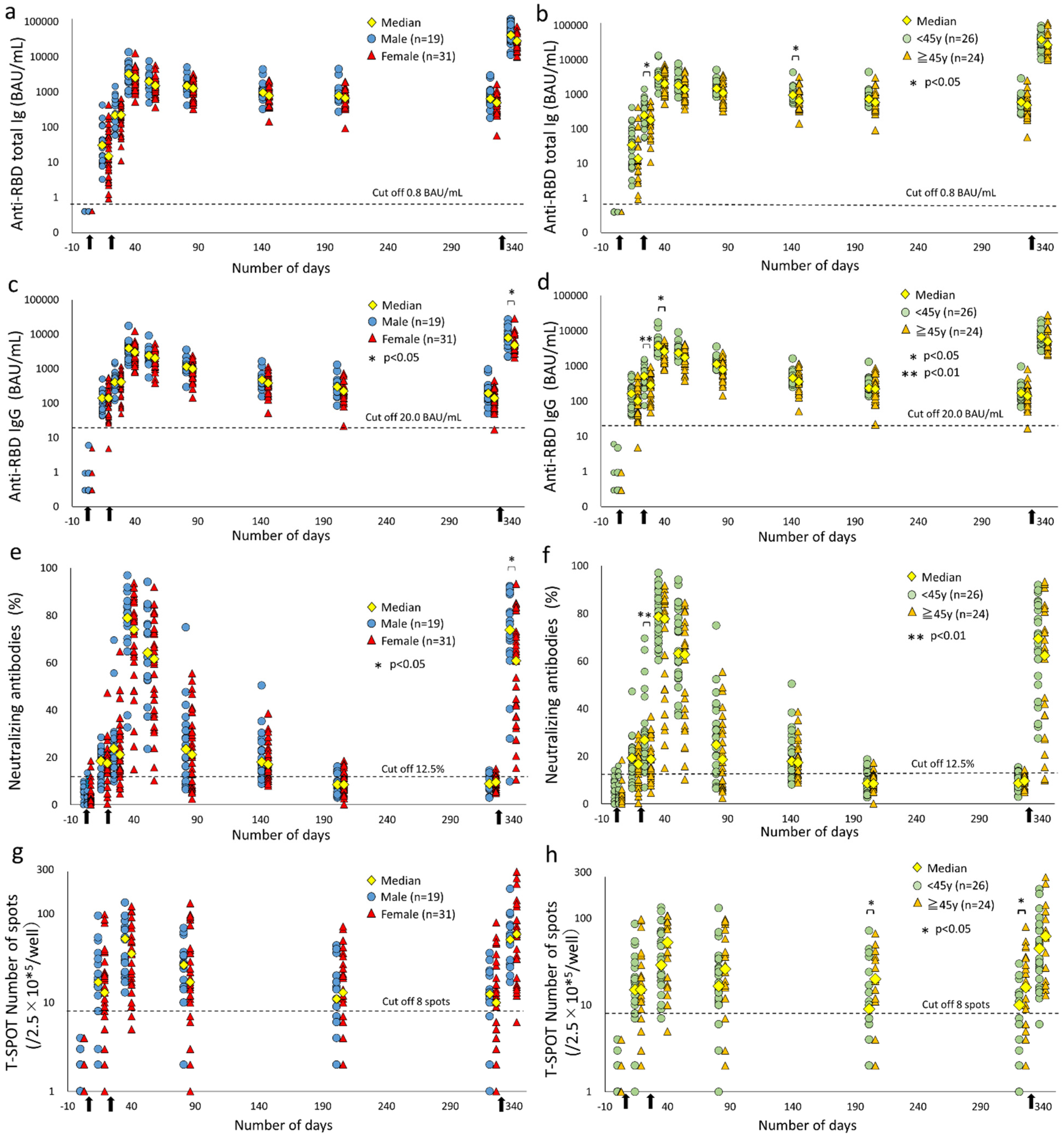
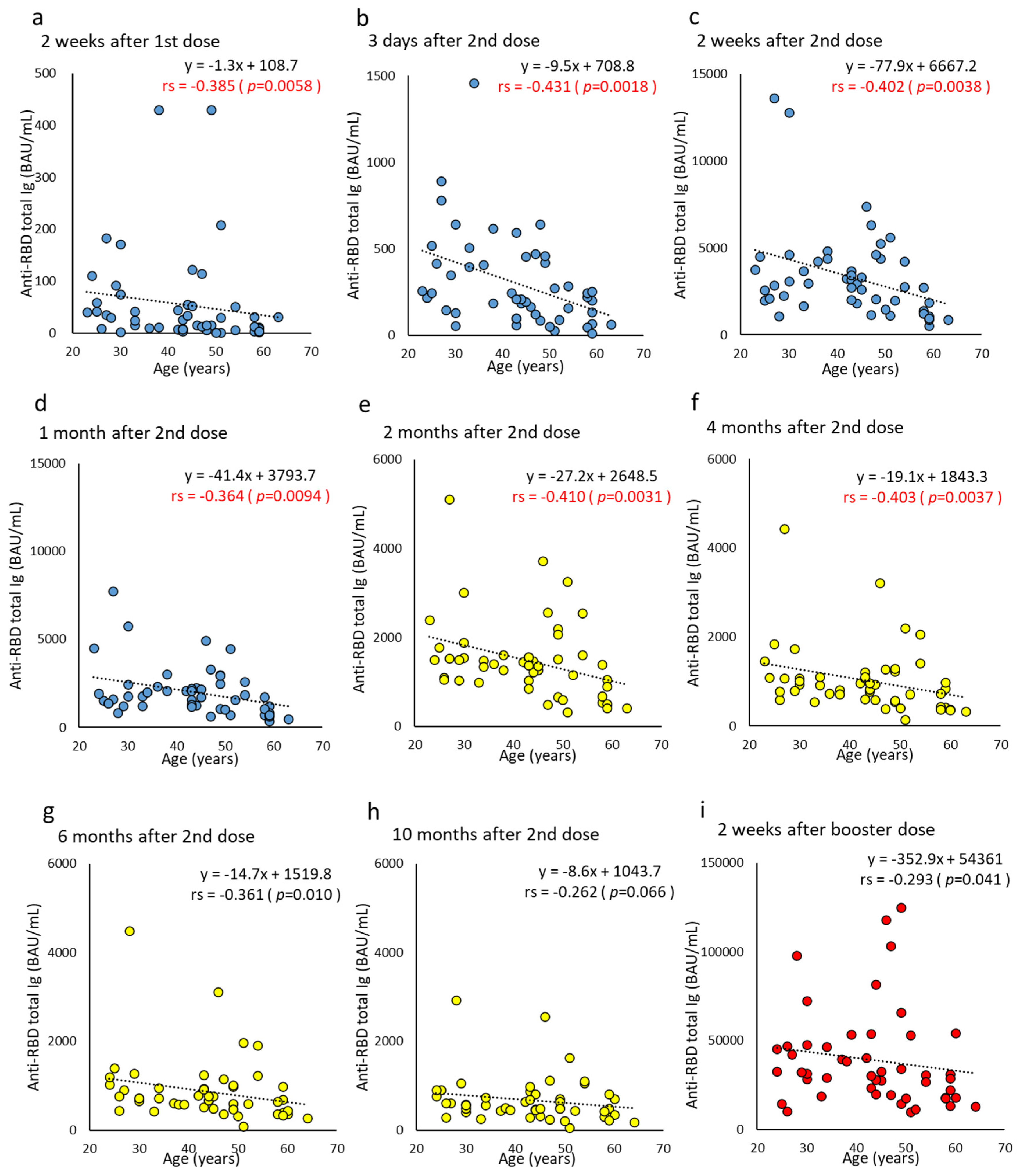
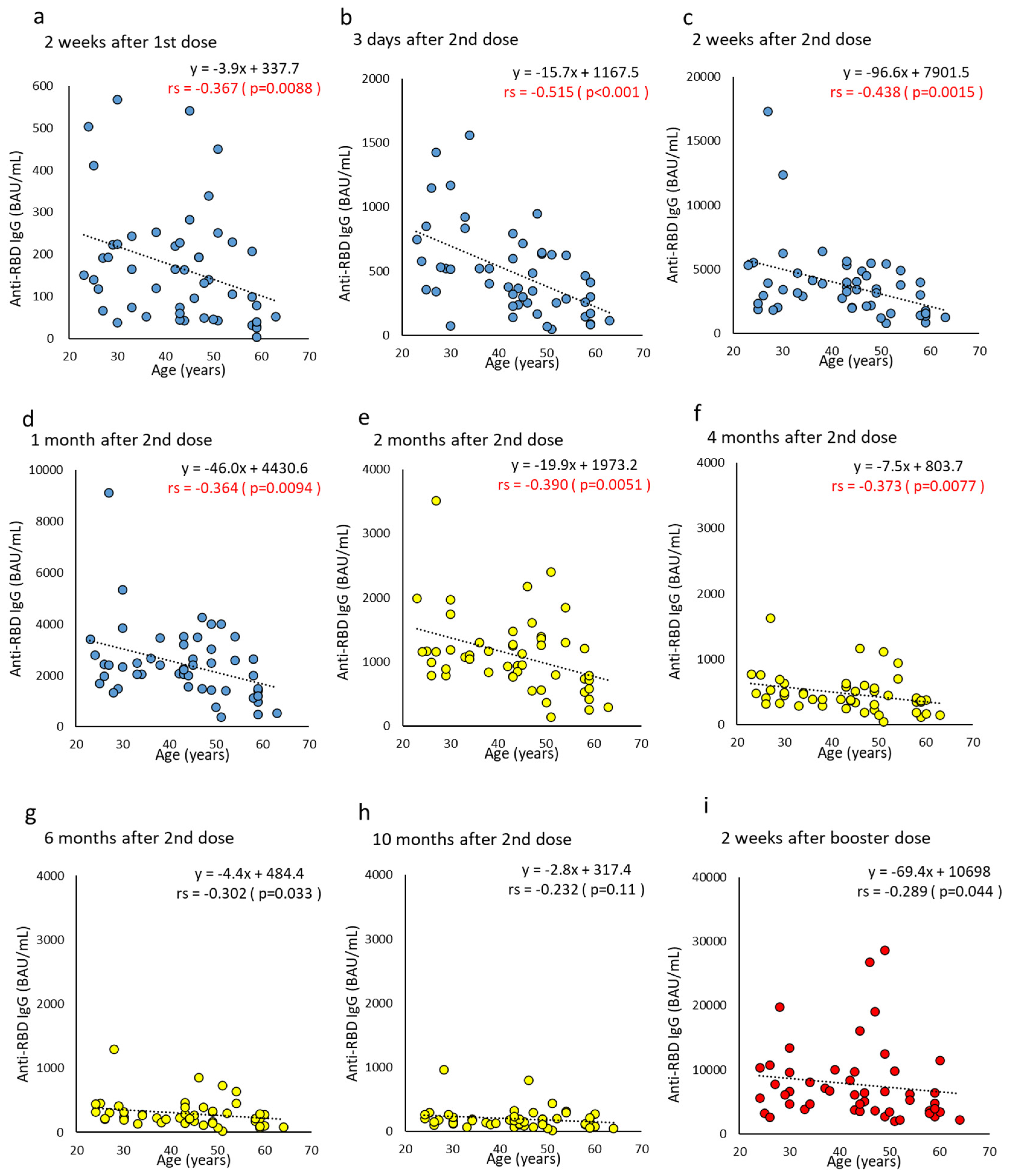
3.2. Time Course of SARS-CoV-2 Anti-RBD Antibodies after COVID-19 Vaccination
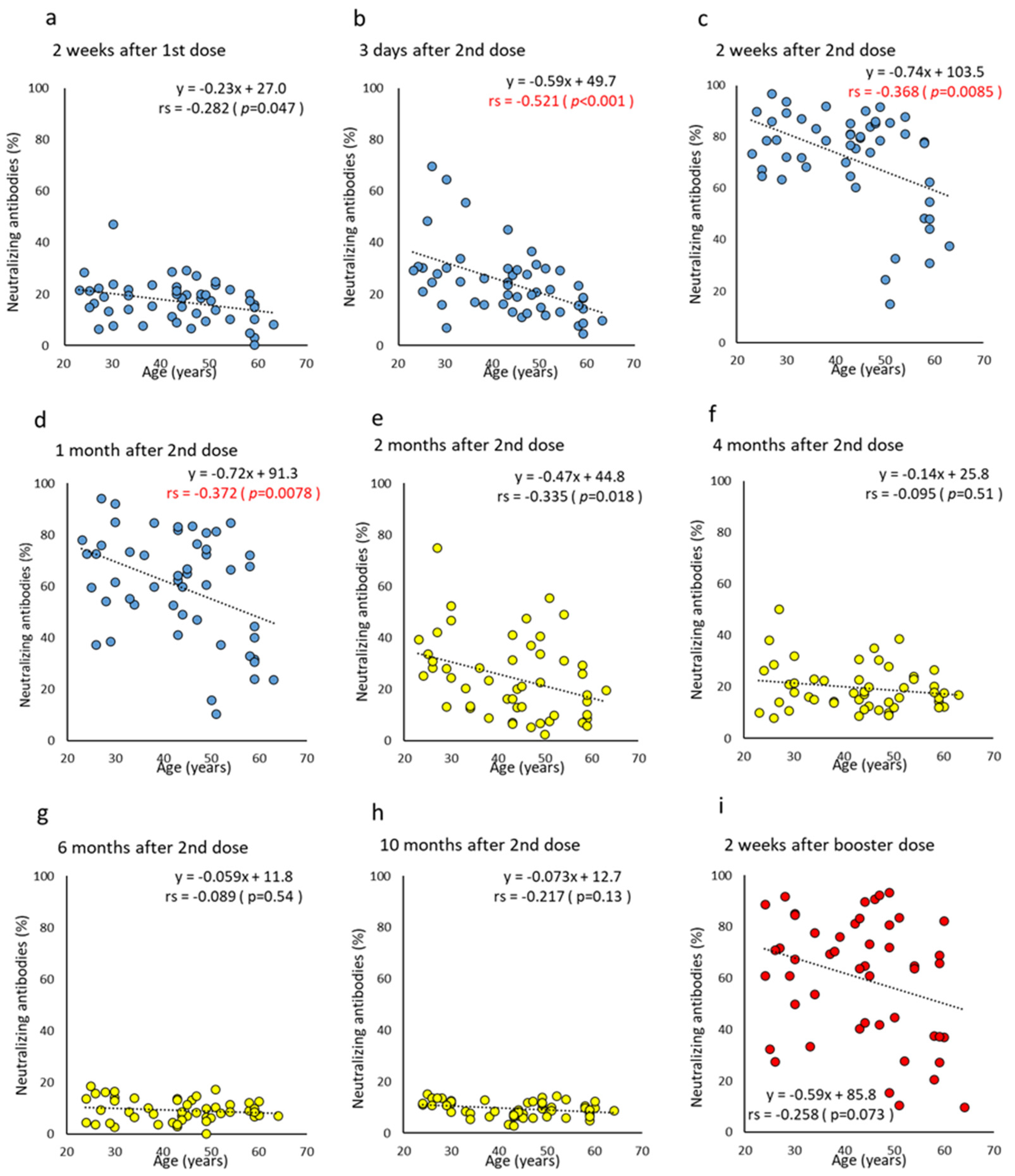
3.3. Time Course of SARS-CoV-2 Neutralizing Antibodies after COVID-19 Vaccination
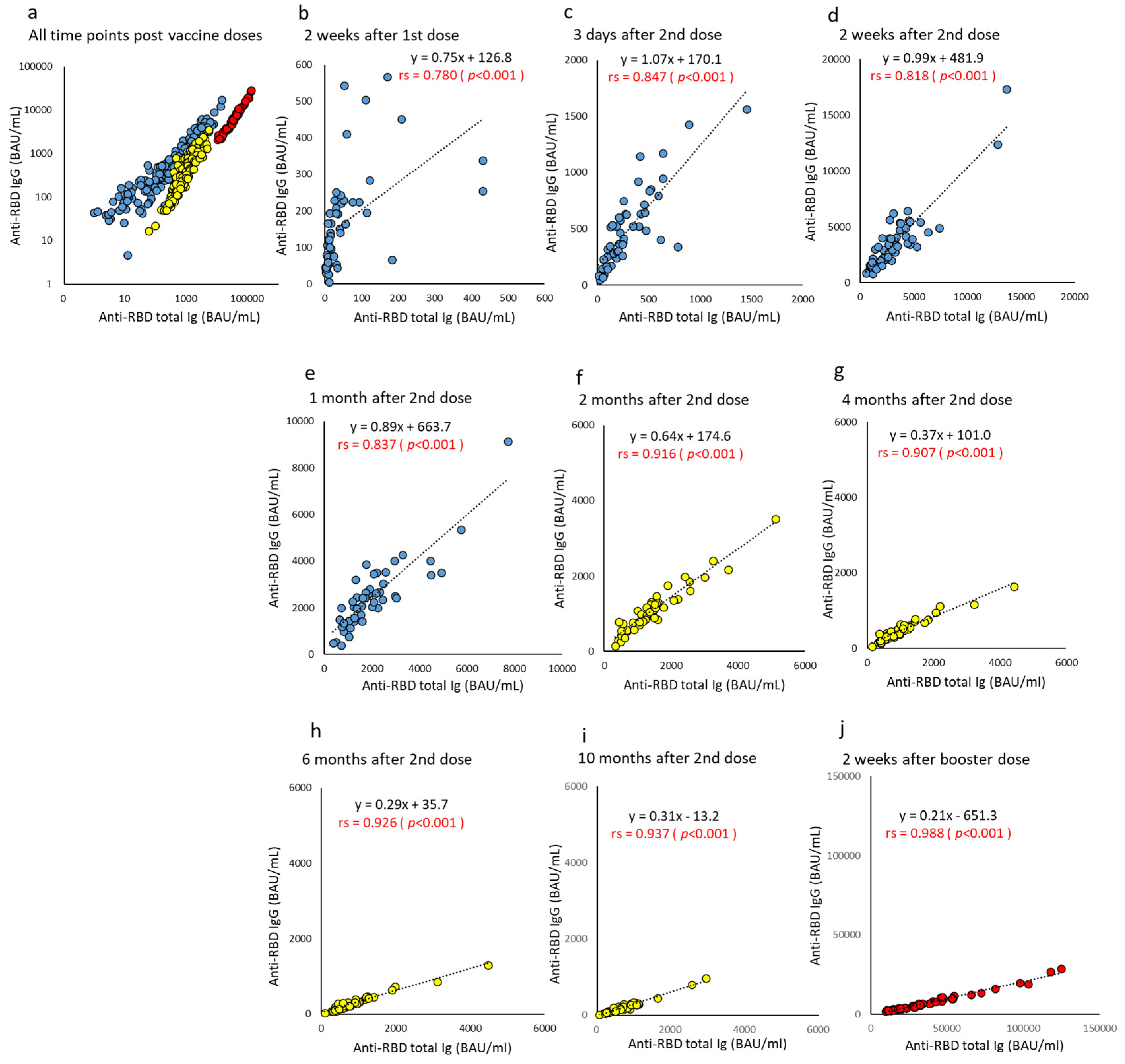
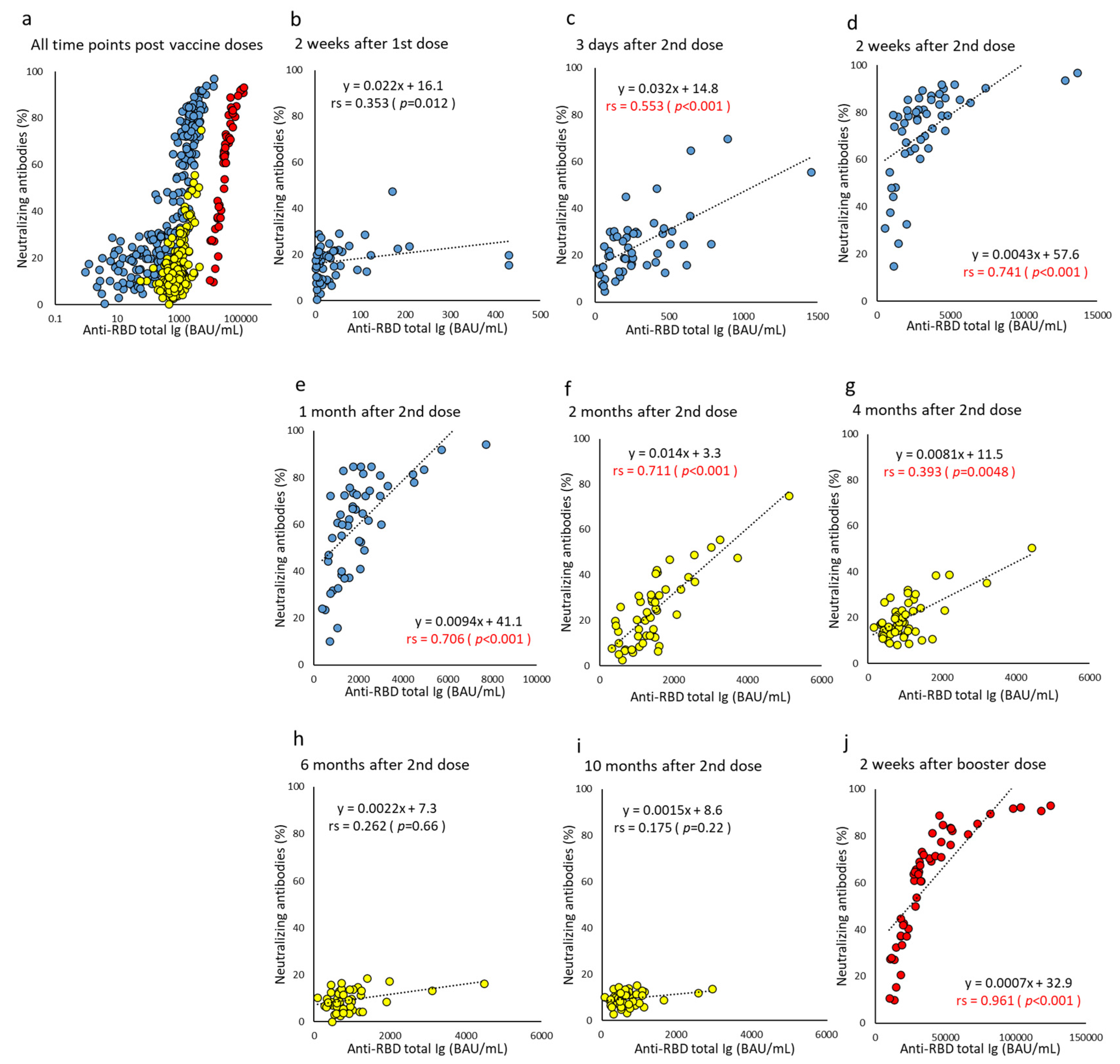
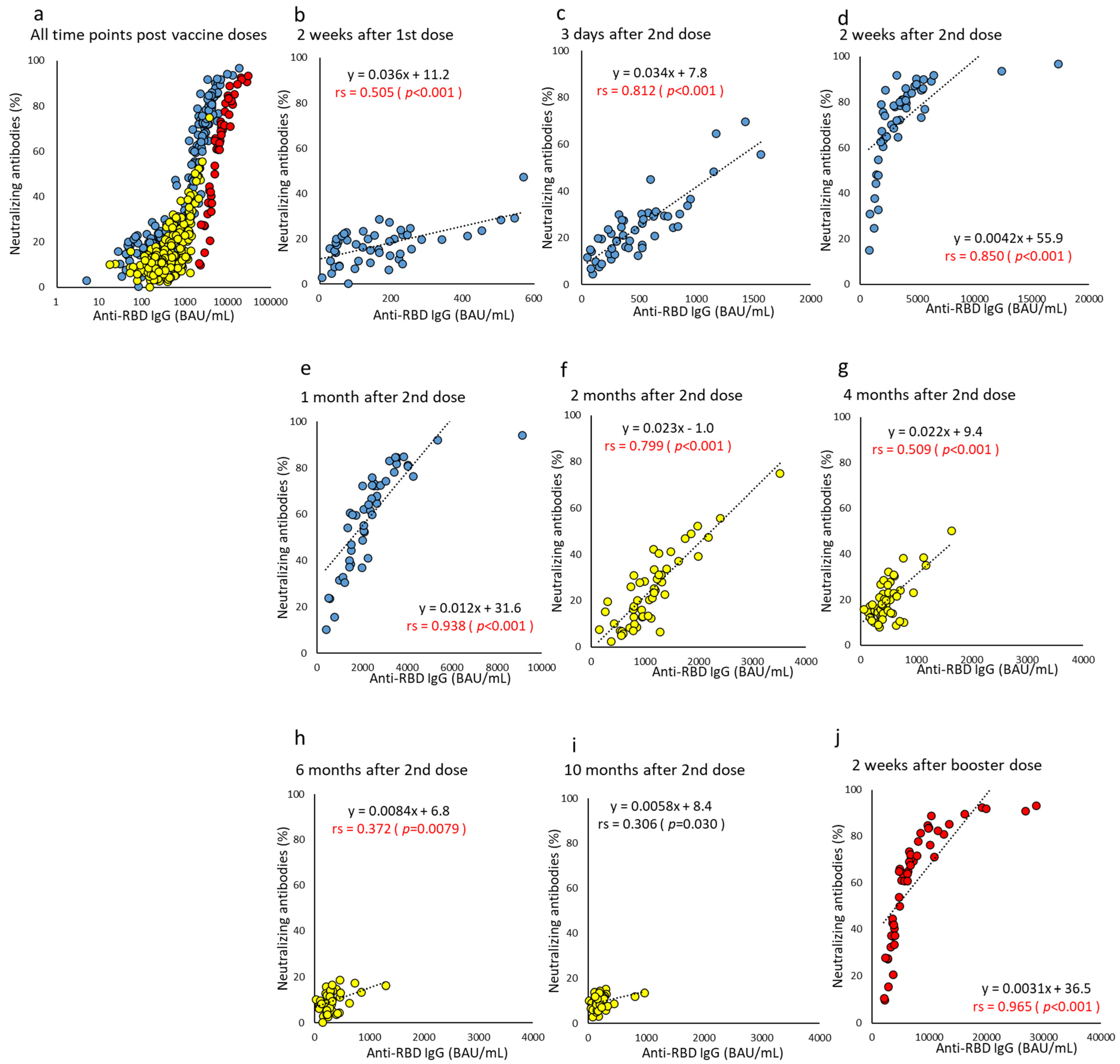
3.4. Correlation of Each Humoral Immunity Parameter for Different Time Points after Vaccine Doses
3.5. Cell-Mediated Immunity, T-SPOT Numbers, and Relation with Humoral Immunity Parameters
3.6. Factors Affecting the Neutralizing Antibody Peak by the Third Dose
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Naaber, P.; Tserel, L.; Kangro, K.; Sepp, E.; Jürjenson, V.; Adamson, A.; Haljasmägi, L.; Rumm, A.P.; Maruste, R.; Kärner, J.; et al. Dynamics of Antibody Response to BNT162b2 Vaccine After Six Months: A Longitudinal Prospective Study. Lancet Reg. Health Eur. 2021, 10, 100208. [Google Scholar] [CrossRef]
- Harvey, W.T.; Carabelli, A.M.; Jackson, B.; Gupta, R.K.; Thomson, E.C.; Harrison, E.M.; Ludden, C.; Reeve, R.; Rambaut, A.; COVID-19 Genomics UK (COG-UK) Consortium; et al. SARS-CoV-2 Variants, Spike Mutations and Immune Escape. Nat. Rev. Microbiol. 2021, 19, 409–424. [Google Scholar] [CrossRef]
- Mlcochova, P.; Kemp, S.A.; Dhar, M.S.; Papa, G.; Meng, B.; Ferreira, I.A.T.M.; Datir, R.; Collier, D.A.; Albecka, A.; Singh, S.; et al. SARS-CoV-2 B.1.617.2 Delta Variant Replication and Immune Evasion. Nature 2021, 599, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Karim, S.S.A.; Karim, Q.A.; Omicron, S.-C. Omicron SARS-CoV-2 Variant: A New Chapter in the COVID-19 Pandemic. Lancet 2021, 398, 2126–2128. [Google Scholar] [CrossRef]
- Tarke, A.; Coelho, C.H.; Zhang, Z.; Dan, J.M.; Yu, E.D.; Methot, N.; Bloom, N.I.; Goodwin, B.; Phillips, E.; Mallal, S.; et al. SARS-CoV-2 Vaccination Induces Immunological T Cell Memory Able to Cross-Recognize Variants from Alpha to Omicron. Cell 2022, 185, 847–859.e11. [Google Scholar] [CrossRef] [PubMed]
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R.; Asraf, K.; Mendelson, E.; Ziv, A.; et al. Waning Immune Humoral Response to BNT162b2 COVID-19 Vaccine Over 6 Months. N. Engl. J. Med. 2021, 385, e84. [Google Scholar] [CrossRef]
- Muench, P.; Jochum, S.; Wenderoth, V.; Ofenloch-Haehnle, B.; Hombach, M.; Strobl, M.; Sadlowski, H.; Sachse, C.; Torriani, G.; Eckerle, I.; et al. Development and Validation of the Elecsys Anti-SARS-CoV-2 Immunoassay as a Highly Specific Tool for Determining past Exposure to SARS-CoV-2. J. Clin. Microbiol. 2020, 58, e01694-20. [Google Scholar] [CrossRef]
- Higgins, V.; Fabros, A.; Kulasingam, V. Quantitative Measurement of Anti-SARS-CoV-2 Antibodies: Analytical and Clinical Evaluation. J. Clin. Microbiol. 2021, 59, e03149-20. [Google Scholar] [CrossRef]
- Giavarina, D.; Carta, M. Improvements and Limits of Anti SARS-CoV-2 Antibodies Assays by WHO (NIBSC 20/136) Standardization. Diagnosis 2022, 9, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Noda, K.; Matsuda, K.; Yagishita, S.; Maeda, K.; Akiyama, Y.; Terada-Hirashima, J.; Matsushita, H.; Iwata, S.; Yamashita, K.; Atarashi, Y.; et al. A Novel Highly Quantitative and Reproducible Assay for the Detection of Anti-SARS-CoV-2 IgG and IgM Antibodies. Sci. Rep. 2021, 11, 5198. [Google Scholar] [CrossRef] [PubMed]
- Shang, J.; Wan, Y.; Luo, C.; Ye, G.; Geng, Q.; Auerbach, A.; Li, F. Cell Entry Mechanisms of SARS-CoV-2. Proc. Natl. Acad. Sci. USA 2020, 117, 11727–11734. [Google Scholar] [CrossRef]
- Takeshita, M.; Nishina, N.; Moriyama, S.; Takahashi, Y.; Uwamino, Y.; Nagata, M.; Aoki, W.; Masaki, K.; Ishii, M.; Saya, H.; et al. Incomplete Humoral Response Including Neutralizing Antibodies in Asymptomatic to Mild COVID-19 Patients in Japan. Virology 2021, 555, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Prendecki, M.; Clarke, C.; Brown, J.; Cox, A.; Gleeson, S.; Guckian, M.; Randell, P.; Dalla Pria, A.D.; Lightstone, L.; Xu, X.N.; et al. Effect of Previous SARS-CoV-2 Infection on Humoral and T-Cell Responses to Single-Dose BNT162b2 Vaccine. Lancet 2021, 397, 1178–1181. [Google Scholar] [CrossRef]
- Oxford Immunotec. Package Insert for Oxford Immunotec, PI-T-SPOT.COVID-IVD-US v3 T-SPOT-COVID-US-PI-v3-1. Available online: https://www.tspotcovid.com/wp-content/uploads/sites/5/2021/03/T-SPOT-COVID-US-PI-v3-1.pdf (accessed on 20 April 2022).
- Kruse, M.; Dark, C.; Aspden, M.; Cochrane, D.; Competiello, R.; Peltz, M.; Torres, L.; Wrighton-Smith, P.; Dudek, M. Performance of the T-SPOT®.COVID Test for Detecting SARS-CoV-2-responsive T Cells. Int. J. Infect. Dis. 2021, 113, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the Freely Available Easy-to-Use Software ‘EZR’ for Medical Statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [Green Version]
- Sourij, C.; Tripolt, N.J.; Aziz, F.; Aberer, F.; Forstner, P.; Obermayer, A.M.; Kojzar, H.; Kleinhappl, B.; Pferschy, P.N.; Mader, J.K.; et al. Humoral Immune Response to COVID-19 Vaccination in Diabetes Is Age-Dependent but Independent of Type of Diabetes and Glycaemic Control: The Prospective COVAC-DM Cohort Study. Diabetes Obes. Metab. 2022, 24, 849–858. [Google Scholar] [CrossRef]
- Kageyama, T.; Ikeda, K.; Tanaka, S.; Taniguchi, T.; Igari, H.; Onouchi, Y.; Kaneda, A.; Matsushita, K.; Hanaoka, H.; Nakada, T.A.; et al. Antibody Responses to BNT162b2 mRNA COVID-19 Vaccine and Their Predictors Among Healthcare Workers in a Tertiary Referral Hospital in Japan. Clin. Microbiol. Infect. 2021, 27, 1861.e1–1861.e5. [Google Scholar] [CrossRef]
- Liu, Y.; Soh, W.T.; Kishikawa, J.I.; Hirose, M.; Nakayama, E.E.; Li, S.; Sasai, M.; Suzuki, T.; Tada, A.; Arakawa, A.; et al. An Infectivity-Enhancing Site on the SARS-CoV-2 Spike Protein Targeted by Antibodies. Cell 2021, 184, 3452–3466.e18. [Google Scholar] [CrossRef]
- Amanat, F.; Stadlbauer, D.; Strohmeier, S.; Nguyen, T.H.O.; Chromikova, V.; McMahon, M.; Jiang, K.; Arunkumar, G.A.; Jurczyszak, D.; Polanco, J.; et al. A Serological Assay to Detect SARS-CoV-2 Seroconversion in Humans. Nat. Med. 2020, 26, 1033–1036. [Google Scholar] [CrossRef] [PubMed]
- Nakagama, Y.; Nitahara, Y.; Kaku, N.; Tshibangu-Kabamba, E.; Kido, Y. A Dual-Antigen SARS-CoV-2 Serological Assay Reflects Antibody Avidity. J. Clin. Microbiol. 2022, 60, e0226221. [Google Scholar] [CrossRef] [PubMed]
- Matusali, G.; Sberna, G.; Meschi, S.; Gramigna, G.; Colavita, F.; Lapa, D.; Francalancia, M.; Bettini, A.; Capobianchi, M.R.; Puro, V.; et al. Differential Dynamics of SARS-CoV-2 Binding and Functional Antibodies upon BNT162b2 Vaccine: A 6-Month Follow-Up. Viruses 2022, 14, 312. [Google Scholar] [CrossRef] [PubMed]
- Moriyama, S.; Adachi, Y.; Sato, T.; Tonouchi, K.; Sun, L.; Fukushi, S.; Yamada, S.; Kinoshita, H.; Nojima, K.; Kanno, T.; et al. Temporal Maturation of Neutralizing Antibodies in COVID-19 Convalescent Individuals Improves Potency and Breadth to Circulating SARS-CoV-2 Variants. Immunity 2021, 54, 1841–1852.e4. [Google Scholar] [CrossRef]
- Victora, G.D.; Nussenzweig, M.C. Germinal Centers. Annu. Rev. Immunol. 2012, 30, 429–457. [Google Scholar] [CrossRef]
- Müller, L.; Andrée, M.; Moskorz, W.; Drexler, I.; Walotka, L.; Grothmann, R.; Ptok, J.; Hillebrandt, J.; Ritchie, A.; Rabl, D.; et al. Age-Dependent Immune Response to the Biontech/Pfizer BNT162b2 Coronavirus Disease 2019 Vaccination. Clin. Infect. Dis. 2021, 73, 2065–2072. [Google Scholar] [CrossRef]
- Kato, H.; Miyakawa, K.; Ohtake, N.; Yamaoka, Y.; Yajima, S.; Yamazaki, E.; Shimada, T.; Goto, A.; Nakajima, H.; Ryo, A. Vaccine-Induced Humoral Response Against SARS-CoV-2 Dramatically Declined but Cellular Immunity Possibly Remained at 6 Months Post BNT162b2 Vaccination. Vaccine 2022, 40, 2652–2655. [Google Scholar] [CrossRef]
- Fujigaki, H.; Yamamoto, Y.; Koseki, T.; Banno, S.; Ando, T.; Ito, H.; Fujita, T.; Naruse, H.; Hata, T.; Moriyama, S.; et al. Antibody Responses to BNT162b2 Vaccination in Japan: Monitoring Vaccine Efficacy by Measuring IgG Antibodies against the Receptor-Binding Domain of SARS-CoV-2. Microbiol. Spectr. 2022, 10, e0118121. [Google Scholar] [CrossRef]
- Gilbert, P.B.; Montefiori, D.C.; McDermott, A.B.; Fong, Y.; Benkeser, D.; Deng, W.; Zhou, H.; Houchens, C.R.; Martins, K.; Jayashankar, L.; et al. Immune Correlates Analysis of the mRNA-1273 COVID-19 Vaccine Efficacy Clinical Trial. Science 2022, 375, 43–50. [Google Scholar] [CrossRef]
- Spitzer, A.; Angel, Y.; Marudi, O.; Zeltser, D.; Saiag, E.; Goldshmidt, H.; Goldiner, I.; Stark, M.; Halutz, O.; Gamzu, R.; et al. Association of a Third Dose of BNT162b2 Vaccine with Incidence of SARS-CoV-2 Infection Among Health Care Workers in Israel. JAMA 2022, 327, 341–349. [Google Scholar] [CrossRef]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing Antibody Levels Are Highly Predictive of Immune Protection from Symptomatic SARS-CoV-2 Infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef] [PubMed]
- Lustig, Y.; Sapir, E.; Regev-Yochay, G.; Cohen, C.; Fluss, R.; Olmer, L.; Indenbaum, V.; Mandelboim, M.; Doolman, R.; Amit, S.; et al. BNT162b2 COVID-19 Vaccine and Correlates of Humoral Immune Responses and Dynamics: A Prospective, Single-Centre, Longitudinal Cohort Study in Health-Care Workers. Lancet Respir. Med. 2021, 9, 999–1009. [Google Scholar] [CrossRef]
- Nemet, I.; Kliker, L.; Lustig, Y.; Zuckerman, N.; Erster, O.; Cohen, C.; Kreiss, Y.; Alroy-Preis, S.; Regev-Yochay, G.; Mendelson, E.; et al. Third BNT162b2 Vaccination Neutralization of SARS-CoV-2 Omicron Infection. N. Engl. J. Med. 2022, 386, 492–494. [Google Scholar] [CrossRef] [PubMed]
- Costa Clemens, S.A.; Weckx, L.; Clemens, R.; Almeida Mendes, A.V.; Ramos Souza, A.; Silveira, M.B.V.; da Guarda, S.N.F.; de Nobrega, M.M.; de Moraes Pinto, M.I.; Gonzalez, I.G.S.; et al. Heterologous Versus Homologous COVID-19 Booster Vaccination in Previous Recipients of Two Doses of CoronaVac COVID-19 Vaccine in Brazil (RHH-001): A phase 4, Non-Inferiority, Single Blind, Randomised Study. Lancet 2022, 399, 521–529. [Google Scholar] [CrossRef]
- Çağlayan, D.; Süner, A.F.; Şiyve, N.; Güzel, I.; Irmak, Ç.; Işik, E.; Appak, Ö.; Çelik, M.; Öztürk, G.; Alp Çavuş, S.; et al. An Analysis of Antibody Response Following the Second Dose of CoronaVac and Humoral Response After Booster Dose with BNT162b2 or CoronaVac Among Healthcare Workers in Turkey. J. Med. Virol. 2022, 94, 2212–2221. [Google Scholar] [CrossRef] [PubMed]
- Re, D.; Seitz-Polski, B.; Brglez, V.; Carles, M.; Graça, D.; Benzaken, S.; Liguori, S.; Zahreddine, K.; Delforge, M.; Bailly-Maitre, B.; et al. Humoral and Cellular Responses After a Third Dose of SARS-CoV-2 BNT162b2 Vaccine in Patients with Lymphoid Malignancies. Nat. Commun. 2022, 13, 864. [Google Scholar] [CrossRef]
- Sun, S.; Cai, X.; Wang, H.; He, G.; Lin, Y.; Lu, B.; Chen, C.; Pan, Y.; Hu, X. Abnormalities of Peripheral Blood System in Patients with COVID-19 in Wenzhou, China. Clin. Chim. Acta 2020, 507, 174–180. [Google Scholar] [CrossRef]
- Cañete, P.F.; Vinuesa, C.G. COVID-19 Makes B Cells Forget, but T Cells Remember. Cell 2020, 183, 13–15. [Google Scholar] [CrossRef]
- Nordström, P.; Ballin, M.; Nordström, A. Risk of Infection, Hospitalisation, and Death up to 9 Months After a Second Dose of COVID-19 Vaccine: A Retrospective, Total Population Cohort Study in Sweden. Lancet 2022, 399, 814–823. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Data | |
|---|---|---|
| Age-years, Median (IQR, range) | Female (n = 31) | 48 (32–56, 23–59) |
| Male (n = 19) | 42 (35–45, 24–63) | |
| Job—no. (%) | Nurse | 12 (24) |
| Physician | 2 (4) | |
| Medical laboratory scientist | 20 (40) | |
| Medical office staff | 16 (32) | |
| Vaccine adverse reactions at 2 doses—no. (%) | Fever (238 °C) | 7 (14) |
| Pain at the injection site | 46 (92) | |
| Fatigue/tiredness | 35 (70) | |
| Headache | 12 (24) | |
| Vaccine adverse reactions at 3 doses—no. (%) | Fever (238 °C) | 14 (28) |
| Pain at the injection site | 43 (86) | |
| Fatigue/tiredness | 38 (76) | |
| Headache | 24 (48) | |
| Antibody (IgG) titers for another virus-COI * median (IQR) | Chickenpox | 17.6 (9.9–23.6) |
| Rubella | 17.8 (8.8–33.7) | |
| Measles | 16.5 (111–31.3) | |
| Mumps | 5.3 (3.3–8.2) | |
| Factor (Unit) | Time Point after 2 Doses | NAb < 65% Inhibition Group: n = 25 Median (IQR) | NAb ≥ 65% Inhibition Group: n = 24 Median (IQR) | p-Value | Odds Ratio (95% Cl) |
|---|---|---|---|---|---|
| Total Ig (BAU/mL) | 2 weeks (peak) | 7.6 (7.0–7.9) * | 8.3 (7.9–8.4) * | 0.0085 | 18.8 (2.12–167) |
| T-SPOT (2.5 × 105/well) | 6 months | 11 (6–20) | 14 (8–41) | 0.011 | 1.13 (1.03–1.24) |
| Eosinophils (%) | 2 months | 3.1 (1.7–6.1) | 1.9 (1.2–3.1) | 0.048 | 0.4 (0.17–0.99) |
| Red blood cells (×106/μL) | 2 months | 4.41 (4.26–4.70) | 4.73 (4.52–5.11) | 0.048 | 1.03 (1.00–1.07) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamashita, K.; Suzuki, A.; Takebayashi, S.; Toguchi, A.; Ogitani, K.; Niizeki, N.; Nagura, O.; Furuhashi, K.; Iwaizumi, M.; Maekawa, M. Differential Dynamics of Humoral and Cell-Mediated Immunity with Three Doses of BNT162b2 SARS-CoV-2 Vaccine in Healthcare Workers in Japan: A Prospective Cohort Study. Vaccines 2022, 10, 1050. https://doi.org/10.3390/vaccines10071050
Yamashita K, Suzuki A, Takebayashi S, Toguchi A, Ogitani K, Niizeki N, Nagura O, Furuhashi K, Iwaizumi M, Maekawa M. Differential Dynamics of Humoral and Cell-Mediated Immunity with Three Doses of BNT162b2 SARS-CoV-2 Vaccine in Healthcare Workers in Japan: A Prospective Cohort Study. Vaccines. 2022; 10(7):1050. https://doi.org/10.3390/vaccines10071050
Chicago/Turabian StyleYamashita, Keita, Akira Suzuki, Shiori Takebayashi, Akihiro Toguchi, Kenya Ogitani, Noriyasu Niizeki, Osanori Nagura, Kazuki Furuhashi, Moriya Iwaizumi, and Masato Maekawa. 2022. "Differential Dynamics of Humoral and Cell-Mediated Immunity with Three Doses of BNT162b2 SARS-CoV-2 Vaccine in Healthcare Workers in Japan: A Prospective Cohort Study" Vaccines 10, no. 7: 1050. https://doi.org/10.3390/vaccines10071050