
Access to Vaccination among Disadvantaged, Isolated and Difficult-to-Reach Communities in the WHO European Region: A Systematic Review

 , , ,
, , ,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
2.3. Study Selection
2.4. Data Extraction and Analysis
2.5. Study Appraisal
3. Results
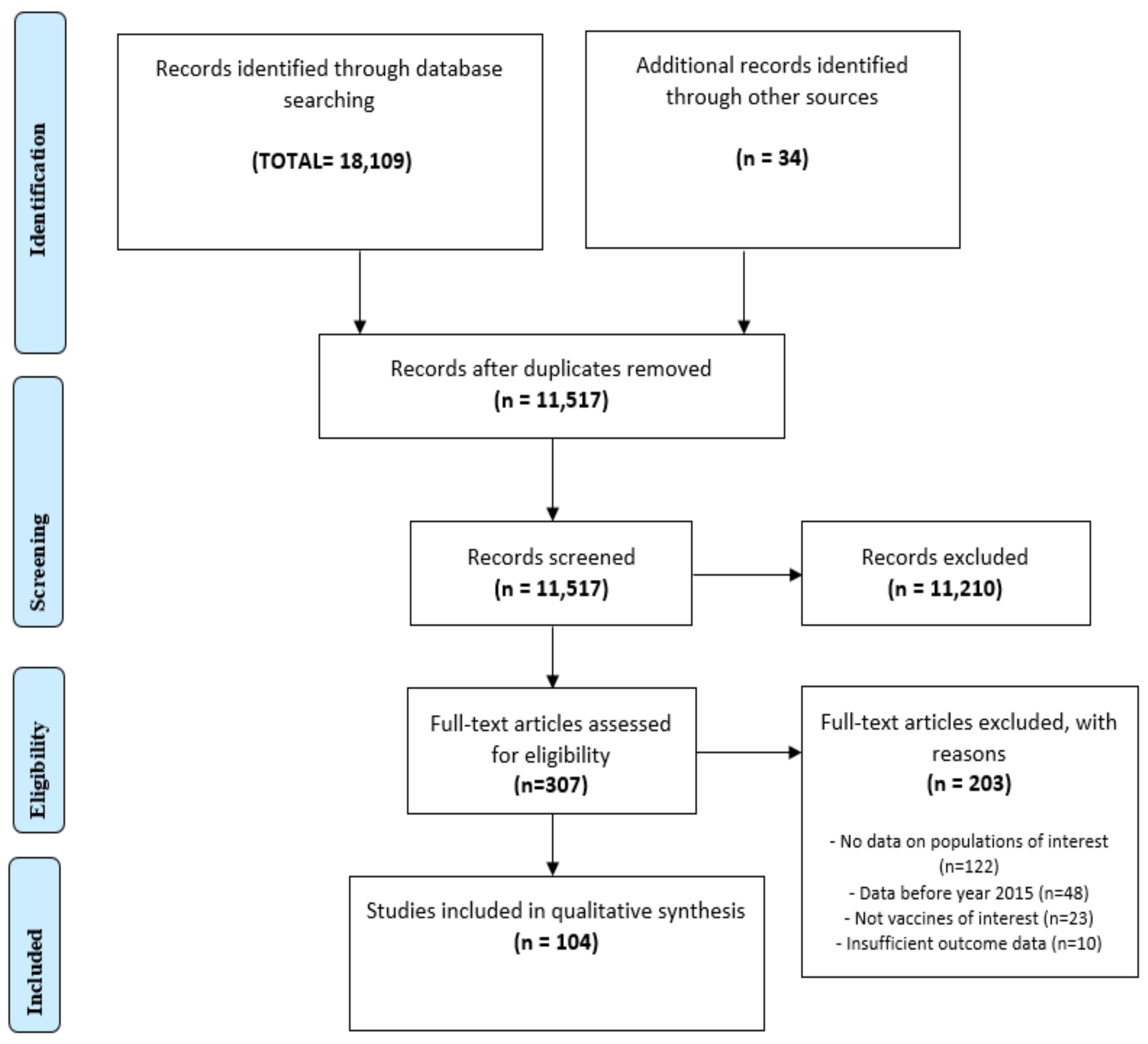
3.1. Study Selection
3.2. Characteristics of Included Studies
3.2.1. Coverage for Non-COVID-19 Vaccines
3.2.2. COVID-19 Vaccine Coverage
3.2.3. Vaccine Coverage Population-Level Insight
3.3. Factors That Influence Considerations around Vaccination
3.3.1. Access to Immunisation Services
3.3.2. Vaccination Awareness and Health Literacy
3.3.3. Barriers
3.3.4. Facilitators
4. Discussion
- Identification of strategies for effectively reaching isolated populations with information about vaccinations;
- Providing early screenings, testing and immediate vaccination for migrant and traveller communities;
- Improving health monitoring by establishing secure databases, implementing vaccination policies that take into consideration the unique factors influencing specific population groups;
- Improving knowledge and understanding of vaccines by providing more information about personal benefits and risks;
- Using new communication techniques (social media) in the active and effective reaching of isolated groups with vaccine information establishing secure immunisation databases that can be frequently updated;
- Supporting vaccine literacy by providing more information to both health providers and isolated, disadvantaged and difficult-to-reach population groups;
- Enhancing community intervention strategies and involvement;
- Strengthening advocacy with community leaders and representatives.
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization Regional Office for Europe. Measles in Europe: Record Number of Both Sick and Immunized; WHO Europe: Geneva, Switzerland, 2019. [Google Scholar]
- European Centre for Disease Prevention and Control. Monthly Measles and Rubella Monitoring Report, April 2019; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2019.
- Doornekamp, L.; Van Leeuwen, L.; Van Gorp, E.; Voeten, H.; Goeijenbier, M. Determinants of Vaccination Uptake in Risk Populations: A Comprehensive Literature Review. Vaccines 2020, 8, 480. [Google Scholar] [CrossRef] [PubMed]
- Villa, S.; Raviglione, M.C. Migrants’ health: Building migrant-sensitive health systems. J. Public Health Res. 2019, 8, 1592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mipatrini, D.; Stefanelli, P.; Severoni, S.; Rezza, G. Vaccinations in migrants and refugees: A challenge for European health systems. A systematic review of current scientific evidence. Pathog. Glob. Health 2017, 111, 59–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Loenen, T.; van den Muijsenbergh, M.; Hofmeester, M.; Dowrick, C.; Van Ginneken, N.; Mechili, E.A.; Angelaki, A.; Ajdukovic, D.; Bakic, H.; Pavlic, D.R.; et al. Primary care for refugees and newly arrived migrants in Europe: A qualitative study on health needs, barriers and wishes. Eur. J. Public Health 2018, 28, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Europe WHO. European Vaccine Action Plan 2015. Available online: https://www.euro.who.int/__data/assets/pdf_file/0007/255679/WHO_EVAP_UK_v30_WEBx.pdf (accessed on 26 April 2022).
- De Vito, E.; Parente, P.; De Waure, C.; Poscia, A.; Ricciardi, W. A Review of Evidence on Equitable Delivery, Access and Utilization of Immunization Services for Migrants and Refugees in the WHO European Region; Health Evidence Network Synthesis Report, No. 53; WHO Regional Office for Europe: Copenhagen, Denmark, 2017. [Google Scholar]
- Ravensbergen, S.J.; Nellums, L.B.; Hargreaves, S.; Stienstra, Y.; Friedland, J.S. National approaches to the vaccination of recently arrived migrants in Europe: A comparative policy analysis across 32 European countries. Travel Med. Infect. Dis. 2019, 27, 33–38. [Google Scholar] [CrossRef]
- Sheikh, S.; Biundo, E.; Courcier, S.; Damm, O.; Launay, O.; Maes, E.; Marcos, C.; Matthews, S.; Meijer, C.; Poscia, A.; et al. A report on the status of vaccination in Europe. Vaccine 2018, 36, 4979–4992. [Google Scholar] [CrossRef]
- Carrasco-Sanz, A.; Leiva-Gea, I.; Martin-Alvarez, L.; Del Torso, S.; Van Esso, D.; Hadjipanayis, A.; Kadir, A.; Ruiz-Canela, J.; Perez-Gonzalez, O.; Grossman, Z. Migrant children’s health problems, care needs, and inequalities: European primary care paediatricians’ perspective. Child Care Health Dev. 2018, 44, 183–187. [Google Scholar] [CrossRef]
- Socha, A.; Klein, J. What are the challenges in the vaccination of migrants in Norway from healthcare provider perspectives? A qualitative, phenomenological study. BMJ Open 2020, 10, e040974. [Google Scholar] [CrossRef]
- Mills, E.; Jadad, A.R.; Ross, C.; Wilson, K. Systematic review of qualitative studies exploring parental beliefs and attitudes toward childhood vaccination identifies common barriers to vaccination. J. Clin. Epidemiol. 2005, 58, 1081–1088. [Google Scholar] [CrossRef]
- Rath, B.; Ekezie, W.; Romaine, C.; Harrabi, M. Access to Vaccination among Disadvantaged, Isolated and Difficult-to-Reach Communities in the WHO-European Region: A Mixed-Method Systematic Review. PROSPERO 2020 CRD42020192530. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020192530 (accessed on 16 April 2022).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- JBI. Critical Appraisal Tools. Available online: https://jbi.global/critical-appraisal-tools (accessed on 16 March 2022).
- Bell, S.; Saliba, V.; Ramsay, M.E.; Mounier-Jack, S. What have we learnt from measles outbreaks in 3 English cities? A qualitative exploration of factors influencing vaccination uptake in Romanian and Roma Romanian communities. BMC Public Health 2020, 20, 381. [Google Scholar] [CrossRef]
- Boukamel, M.; Fougère, Y.; Gehri, M.; Suris, J.C.; Rochat, I.; Miletto, D.; Kyrilli, S.; Fouriki, A.; Crisinel, P.A. Prevalence of tuberculosis in migrant children in Switzerland and relevance of current screening guidelines. Swiss Med. Wkly. 2020, 150, w20253. [Google Scholar] [CrossRef] [PubMed]
- Ergönül, Ö.; Tülek, N.; Kayı, I.; Irmak, H.; Erdem, O.; Dara, M. Profiling infectious diseases in Turkey after the influx of 3.5 million Syrian refugees. Clin. Microbiol. Infect. 2020, 26, 307–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorman, D.R.; Bielecki, K.; Willocks, L.J.; Pollock, K.G. A qualitative study of vaccination behaviour amongst female Polish migrants in Edinburgh, Scotland. Vaccine 2019, 37, 2741–2747. [Google Scholar] [CrossRef] [Green Version]
- Mueller-Hermelink, M.; Kobbe, R.; Methling, B.; Rau, C.; Schulze-Sturm, U.; Auer, I.; Ahrens, F.; Brinkmann, F. Universal screening for latent and active tuberculosis (TB) in asylum seeking children, Bochum and Hamburg, Germany, September 2015 to November 2016. Eurosurveillance 2018, 23, 17-00536. [Google Scholar] [CrossRef] [Green Version]
- Öztaş, D.; Kurt, B.; Akbaba, M.; Akyol, M.; Mollahaliloğlu, S.; Topaç, O. Vaccination rates for Syrian population under temporary protection in Turkey. Cent. Eur. J. Public Health 2020, 28, 130–134. [Google Scholar] [CrossRef]
- Ali-Saleh, O.; Bord, S.; Basis, F. Low Response to the COVID-19 Vaccine Among the Arab Population in Israel: Is It a Cultural Background, or a Systemic Failure, or Maybe Both? J. Racial Ethn. Health Disparities 2022. [Google Scholar] [CrossRef]
- Bentivegna, E.; Di Meo, S.; Carriero, A.; Capriotti, N.; Barbieri, A.; Martelletti, P. Access to COVID-19 Vaccination during the Pandemic in the Informal Settlements of Rome. Int. J. Environ. Res. Public Health 2022, 19, 719. [Google Scholar] [CrossRef]
- Blakeway, H.; Prasad, S.; Kalafat, E.; Heath, P.T.; Ladhani, S.N.; Le Doare, K.; Magee, L.A.; O’Brien, P.; Rezvani, A.; von Dadelszen, P.; et al. COVID-19 vaccination during pregnancy: Coverage and safety. Am. J. Obstet. Gynecol. 2022, 226, 236.e1–236.e14. [Google Scholar] [CrossRef]
- Cook, E.J.; Elliott, E.; Gaitan, A.; Nduka, I.; Cartwright, S.; Egbutah, C.; Randhawa, G.; Waqar, M.; Ali, N. Vaccination against COVID-19: Factors That Influence Vaccine Hesitancy among an Ethnically Diverse Community in the UK. Vaccines 2022, 10, 106. [Google Scholar] [CrossRef] [PubMed]
- Gaughan, C.H.; Razieh, C.; Khunti, K.; Banerjee, A.; Chudasama, Y.V.; Davies, M.J.; Dolby, T.; Gillies, C.L.; Lawson, C.; Mirkes, E.M.; et al. COVID-19 vaccination uptake amongst ethnic minority communities in England: A linked study exploring the drivers of differential vaccination rates. J. Public Health 2022, fdab400. [Google Scholar] [CrossRef] [PubMed]
- Glampson, B.; Brittain, J.; Kaura, A.; Mulla, A.; Mercuri, L.; Brett, S.J.; Aylin, P.; Sandall, T.; Goodman, I.; Redhead, J.; et al. Assessing COVID-19 Vaccine Uptake and Effectiveness Through the North West London Vaccination Program: Retrospective Cohort Study. JMIR Public Health Surveill. 2021, 7, e30010. [Google Scholar] [CrossRef] [PubMed]
- Gorelik, Y.; Anis, E.; Edelstein, M. Inequalities in initiation of COVID19 vaccination by age and population group in Israel- December 2020–July 2021. Lancet Reg. Health Eur. 2022, 12, 100234. [Google Scholar] [CrossRef] [PubMed]
- Hall, V.J.; Foulkes, S.; Saei, A.; Andrews, N.; Oguti, B.; Charlett, A.; Wellington, E.; Stowe, J.; Gillson, N.; Atti, A.; et al. COVID-19 vaccine coverage in health-care workers in England and effectiveness of BNT162b2 mRNA vaccine against infection (SIREN): A prospective, multicentre, cohort study. Lancet 2021, 397, 1725–1735. [Google Scholar] [CrossRef]
- Iacoella, C.; Ralli, M.; Maggiolini, A.; Arcangeli, A.; Ercoli, L. Acceptance of COVID-19 vaccine among persons experiencing homelessness in the City of Rome, Italy. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 3132–3135. [Google Scholar]
- Kraft, K.B.; Godøy, A.A.; Vinjerui, K.H.; Kour, P.; Kjøllesdal, M.K.R.; Indseth, T. COVID-19 vaccination coverage by immigrant background.Vaksinasjonsdekning mot covid-19 etter innvandrerbakgrunn. Tidsskr. Nor. Legeforening 2021, 141. [Google Scholar] [CrossRef]
- Martin, C.A.; Marshall, C.; Patel, P.; Goss, C.; Jenkins, D.R.; Ellwood, C.; Barton, L.; Price, A.; Brunskill, N.J.; Khunti, K.; et al. SARS-CoV-2 vaccine uptake in a multi-ethnic UK healthcare workforce: A cross-sectional study. PLOS Med. 2021, 18, e1003823. [Google Scholar] [CrossRef]
- Muhsen, K.; Na’Aminh, W.; Lapidot, Y.; Goren, S.; Amir, Y.; Perlman, S.; Green, M.S.; Chodick, G.; Cohen, D. A nationwide analysis of population group differences in the COVID-19 epidemic in Israel, February 2020–February 2021. Lancet Reg. Health Eur. 2021, 7, 100130. [Google Scholar] [CrossRef]
- Nafilyan, V.; Dolby, T.; Razieh, C.; Gaughan, C.H.; Morgan, J.; Ayoubkhani, D.; Walker, S.; Khunti, K.; Glickman, M.; Yates, T. Sociodemographic inequality in COVID-19 vaccination coverage among elderly adults in England: A national linked data study. BMJ Open 2021, 11, e053402. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Joshi, A.D.; Drew, D.A.; Merino, J.; Ma, W.; Lo, C.-H.; Kwon, S.; Wang, K.; Graham, M.S.; Polidori, L.; et al. Self-reported COVID-19 vaccine hesitancy and uptake among participants from different racial and ethnic groups in the United States and United Kingdom. Nat. Commun. 2022, 13, 1–9. [Google Scholar] [CrossRef]
- Perry, M.; Akbari, A.; Cottrell, S.; Gravenor, M.B.; Roberts, R.; Lyons, R.A.; Bedston, S.; Torabi, F.; Griffiths, L. Inequalities in coverage of COVID-19 vaccination: A population register based cross-sectional study in Wales, UK. Vaccine 2021, 39, 6256–6261. [Google Scholar] [CrossRef] [PubMed]
- Saban, M.; Myers, V.; Ben-Shetrit, S.; Wilf-Miron, R. Socioeconomic gradient in COVID-19 vaccination: Evidence from Israel. Int. J. Equity Health 2021, 20, 242. [Google Scholar] [CrossRef] [PubMed]
- Taubman-Ben-Ari, O.; Weiss, E.; Abu-Sharkia, S.; Khalaf, E.; Msw, E.W.; Msw, S.A.S.; Ma, E.K. A comparison of COVID-19 vaccination status among pregnant Israeli Jewish and Arab women and psychological distress among the Arab women. Nurs. Health Sci. 2022, 24, 360–367. [Google Scholar] [CrossRef]
- Tessier, E.; Rai, Y.; Clarke, E.; Lakhani, A.; Tsang, C.; Makwana, A.; Heard, H.; Rickeard, T.; Lakhani, S.; Roy, P.; et al. Characteristics associated with COVID-19 vaccine uptake among adults aged 50 years and above in England (8 December 2020–17 May 2021): A population-level observational study. BMJ Open 2022, 12, e055278. [Google Scholar] [CrossRef]
- Watkinson, R.E.; Williams, R.; Gillibrand, S.; Sanders, C.; Sutton, M. Ethnic inequalities in COVID-19 vaccine uptake and comparison to seasonal influenza vaccine uptake in Greater Manchester, UK: A cohort study. PLoS Med. 2022, 19, e1003932. [Google Scholar] [CrossRef]
- Dixon, K.C.; Mullis, R.; Blumenfeld, T. Vaccine uptake in the Irish Travelling community: An audit of general practice records. J. Public Health 2017, 39, e235–e241. [Google Scholar] [CrossRef] [Green Version]
- Freidl, G.S.; Tostmann, A.; Curvers, M.; Ruijs, W.L.; Smits, G.; Schepp, R.; Duizer, E.; Boland, G.; de Melker, H.; van der Klis, F.R.; et al. Immunity against measles, mumps, rubella, varicella, diphtheria, tetanus, polio, hepatitis A and hepatitis B among adult asylum seekers in The Netherlands, 2016. Vaccine 2018, 36, 1664–1672. [Google Scholar] [CrossRef]
- Jablonka, A.; Behrens, G.M.N.; Stange, M.; Dopfer, C.; Grote, U.; Hansen, G.; Schmidt, R.E.; Happle, C. Tetanus and diphtheria immunity in refugees in Europe in 2015. Infection 2017, 45, 157–164. [Google Scholar] [CrossRef]
- Jackson, C.; Bedford, H.; Cheater, F.M.; Condon, L.; Emslie, C.; Ireland, L.; Kemsley, P.; Kerr, S.; Lewis, H.J.; Mytton, J.; et al. Needles, Jabs and Jags: A qualitative exploration of barriers and facilitators to child and adult immunisation uptake among Gypsies, Travellers and Roma. BMC Public Health 2017, 17, 254. [Google Scholar] [CrossRef] [Green Version]
- Louka, C.; Chandler, E.; Ranchor, A.V.; Broer, H.; Pournaras, S.; Ravensbergen, S.J.; Stienstra, Y. Asylum seekers’ perspectives on vaccination and screening policies after their arrival in Greece and The Netherlands. PLoS ONE 2019, 14, e0226948. [Google Scholar] [CrossRef] [PubMed]
- Mellou, K.; Silvestros, C.; Saranti-Papasaranti, E.; Koustenis, A.; Pavlopoulou, I.D.; Georgakopoulou, T.; Botsi, C.; Terzidis, A. Increasing childhood vaccination coverage of the refugee and migrant population in Greece through the European programme PHILOS, April 2017 to April 2018. Eurosurveillance 2019, 24, 1800326. [Google Scholar] [CrossRef] [PubMed]
- Nakken, C.S.; Skovdal, M.; Nellums, L.B.; Friedland, J.S.; Hargreaves, S.; Norredam, M. Vaccination status and needs of asylum-seeking children in Denmark: A retrospective data analysis. Public Health 2018, 158, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Perry, M.; Townson, M.; Cottrell, S.; Fagan, L.; Edwards, J.; Saunders, J.; O’Hare, R.; Richardson, G. Inequalities in vaccination coverage and differences in follow-up procedures for asylum-seeking children arriving in Wales, UK. Eur. J. Pediatr. 2020, 179, 171–175. [Google Scholar] [CrossRef]
- Sane, J.; Sorvari, T.; Widerström, M.; Kauma, H.; Kaukoniemi, U.; Tarkka, E.; Puumalainen, T.; Kuusi1, M.; Salminen, M.; Lyytikäinen, O. Respiratory diphtheria in an asylum seeker from Afghanistan arriving to Finland via Sweden, December 2015. Eurosurveillance 2016, 21, 14–17. [Google Scholar] [CrossRef]
- Staehelin, C.; Chernet, A.; Sydow, V.; Piso, R.J.; Suter-Riniker, F.; Funez, S.; Nickel, B.; Paris, D.H.; Labhardt, N.D. Seroprotection rates of vaccine-preventable diseases among newly arrived Eritrean asylum seekers in Switzerland: A cross-sectional study. J. Travel Med. 2019, 26, taz035. [Google Scholar] [CrossRef]
- Stein-Zamir, C.; Israeli, A. Knowledge, Attitudes and Perceptions About Routine Childhood Vaccinations Among Jewish Ultra-Orthodox Mothers Residing in Communities with Low Vaccination Coverage in the Jerusalem District. Matern. Child Health J. 2017, 21, 1010–1017. [Google Scholar] [CrossRef]
- Stein-Zamir, C.; Israeli, A. Timeliness and completeness of routine childhood vaccinations in young children residing in a district with recurrent vaccine-preventable disease outbreaks, Jerusalem, Israel. Eurosurveillance 2019, 24, 1800004. [Google Scholar] [CrossRef]
- Vita, S.; Sinopoli, M.T.; Sulekova, L.F.; Morucci, L.; Lopalco, M.; Spaziante, M.; Pacifici, L.E.; Bazzardi, R.; Angeletti, S.; Ciccozzi, M.; et al. Vaccination campaign strategies in recently arrived migrants: Experience of an Italian reception centre. J. Infect. Dev. Ctries. 2019, 13, 1159–1164. [Google Scholar] [CrossRef]
- Cuomo, G.; Franconi, I.; Riva, N.; Bianchi, A.; Digaetano, M.; Santoro, A.; Codeluppi, M.; Bedini, A.; Guaraldi, G.; Mussini, C. Migration and health: A retrospective study about the prevalence of HBV, HIV, HCV, tuberculosis and syphilis infections amongst newly arrived migrants screened at the Infectious Diseases Unit of Modena, Italy. J. Infect. Public Health 2019, 12, 200–204. [Google Scholar] [CrossRef]
- Fougère, Y.; El Houss, S.; Surís, J.-C.; Rouvenaz-Defago, S.; Miletto, D.; Von Der Weid, L.; Willen, F.; Williams-Smith, J.A.; Gehri, M.; Crisinel, P.A. High coverage of hepatitis B vaccination and low prevalence of chronic hepatitis B in migrant children dictate a new catch-up vaccination strategy. Vaccine 2018, 36, 4501–4506. [Google Scholar] [CrossRef] [PubMed]
- Führer, A.; Eichner, F.; Stang, A. Morbidity of asylum seekers in a medium-sized German city. Eur. J. Epidemiol. 2016, 31, 703–706. [Google Scholar] [CrossRef] [PubMed]
- Karasahin, E.F.; Karasahin, O.; Kalkan, I.A. Results of Viral Hepatitis and Human Immunodeficiency Virus Screening in Afghan Irregular Migrants: A Cross-sectional Study (2011–2019). Viral Hepatit Derg. Viral Hepat. J. 2021, 27, 98–102. [Google Scholar] [CrossRef]
- Köse, Ş.; Ödemiş, I.; Çelik, D.; Gireniz Tatar, B.; Akbulut, I.; Çiftdoğan, D.Y. Hepatitis A, B, C and HIV seroprevalence among Syrian refugee children admitted to outpatient clinics. Infez. Med. 2017, 25, 339–343. [Google Scholar]
- Mazzitelli, M.; Greco, G.; Serapide, F.; Scaglione, V.; Morrone, H.; Marascio, N.; Giancotti, A.; Liberto, M.; Matera, G.; Trecarichi, E.; et al. Outcome of HBV screening and vaccination in a migrant population in southern Italy. Infez. Med. 2021, 29, 236–241. [Google Scholar]
- Mellou, K.; Chrisostomou, A.; Sideroglou, T.; Georgakopoulou, T.; Kyritsi, M.; Hadjichristodoulou, C.; Tsiodras, S. Hepatitis A among refugees, asylum seekers and migrants living in hosting facilities, Greece, April to December 2016. Eurosurveillance 2017, 22, 30448. [Google Scholar] [CrossRef]
- Norman, F.F.; Comeche, B.; Martínez-Lacalzada, M.; Pérez-Molina, J.-A.; Gullón, B.; Monge-Maillo, B.; Chamorro, S.; López-Vélez, R. Seroprevalence of vaccine-preventable and non-vaccine-preventable infections in migrants in Spain. J. Travel Med. 2021, 28, taab025. [Google Scholar] [CrossRef]
- Serre-Delcor, N.; Treviño-Maruri, B.; Collazos-Sanchez, F.; Pou-Ciruelo, D.; Soriano-Arandes, A.; Sulleiro, E.; Molina-Romero, I.; Ascaso, C.; Bocanegra-Garcia, C. Health Status of Asylum Seekers, Spain. Am. J. Trop. Med. Hyg. 2018, 98, 300–307. [Google Scholar] [CrossRef] [Green Version]
- Taylor, J.E.B.; Surey, J.; MacLellan, J.; Francis, M.; Abubakar, I.; Stagg, H.R. Hepatitis B vaccination uptake in hard-to-reach populations in London: A cross-sectional study. BMC Infect. Dis. 2019, 19, 372. [Google Scholar] [CrossRef]
- Vu, F.; Cavassini, M.; D’Acremont, V.; Greub, G.; Jaton, K.; Masserey, E.; Pongelli, S.; Bouche, L.; Ngarambe, C.; Bize, R.; et al. Epidemiology of sexually transmitted infections among female sex workers in Switzerland: A local, exploratory, cross-sectional study. Swiss Med. Wkly. 2020, 150, w20357. [Google Scholar] [CrossRef]
- Bechini, A.; Pieralli, F.; Chellini, E.; Martini, A.; Dugheri, G.; Crescioli, F.; Scatena, T.; Baggiani, L.; Lillini, R.; Fiaschi, P.; et al. Application of socio-economic-health deprivation index, analysis of mortality and influenza vaccination coverage in the elderly population of Tuscany. J. Prev. Med. Hyg. 2019, 59, E18–E25. [Google Scholar] [CrossRef] [PubMed]
- Bielecki, K.; Kirolos, A.; Willocks, L.; Pollock, K.; Gorman, D. Low uptake of nasal influenza vaccine in Polish and other ethnic minority children in Edinburgh, Scotland. Vaccine 2019, 37, 693–697. [Google Scholar] [CrossRef]
- Bielecki, K.; Craig, J.; Willocks, L.J.; Pollock, K.G.; Gorman, D.R. Impact of an influenza information pamphlet on vaccination uptake among Polish pupils in Edinburgh, Scotland and the role of social media in parental decision making. BMC Public Health 2020, 20, 1381. [Google Scholar] [CrossRef] [PubMed]
- Boddington, N.L.; Warburton, F.; Zhao, H.; Andrews, N.; Ellis, J.; Donati, M.; Pebody, R.G. Influenza vaccine effectiveness against hospitalisation due to laboratory-confirmed influenza in children in England in the 2015–2016 influenza season—A test-negative case-control study. Epidemiol. Infect. 2019, 147, e201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fortunato, F.; Iannelli, G.; Cozza, A.; Del Prete, M.; Pollidoro, F.; Cocciardi, S.; Di Trani, M.; Martinelli, D.; Prato, R. Local deprivation status and seasonal influenza vaccination coverage in adults ≥65 years residing in the Foggia municipality, Italy, 2009–2016. J. Prev. Med. Hyg. 2019, 59, E51–E64. [Google Scholar] [CrossRef] [PubMed]
- Glatman-Freedman, A.; Amir, K.; Dichtiar, R.; Zadka, H.; Vainer, I.; Karolinsky, D.; Enav, T.; Shohat, T. Factors associated with childhood influenza vaccination in Israel: A cross-sectional evaluation. Isr. J. Health Policy Res. 2019, 8, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Gorman, D.R.; Bielecki, K.; Larson, H.J.; Willocks, L.J.; Craig, J.; Pollock, K.G. Comparing vaccination hesitancy in Polish migrant parents who accept or refuse nasal flu vaccination for their children. Vaccine 2020, 38, 2795–2799. [Google Scholar] [CrossRef]
- Hardelid, P.; Rait, G.; Gilbert, R.; Petersen, I. Factors associated with influenza vaccine uptake during a universal vaccination programme of preschool children in England and Wales: A cohort study. J. Epidemiol. Community Health 2016, 70, 1082–1087. [Google Scholar] [CrossRef] [Green Version]
- Hungerford, D.; Ibarz-Pavon, A.; Cleary, P.; French, N. Influenza-associated hospitalisation, vaccine uptake and socioeconomic deprivation in an English city region: An ecological study. BMJ Open 2018, 8, e023275. [Google Scholar] [CrossRef] [Green Version]
- Loiacono, M.M.; Mahmud, S.M.; Chit, A.; van Aalst, R.; Kwong, J.C.; Mitsakakis, N.; Skinner, L.; Thommes, E.; Bricout, H.; Grootendorst, P. Patient and practice level factors associated with seasonal influenza vaccine uptake among at-risk adults in England, 2011 to 2016: An age-stratified retrospective cohort study. Vaccine X 2020, 4, 100054. [Google Scholar] [CrossRef]
- Ben Natan, M.; Kabha, S.; Yehia, M.; Hamza, O. Factors That Influence Israeli Muslim Arab Parents’ Intention to Vaccinate Their Children Against Influenza. J. Pediatr. Nurs. 2016, 31, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Perniciaro, S.; Imöhl, M.; Van Der Linden, M. Invasive Pneumococcal Disease in Refugee Children, Germany. Emerg. Infect. Dis. 2018, 24, 1934–1936. [Google Scholar] [CrossRef] [PubMed]
- Shahbari, N.A.E.; Gesser-Edelsburg, A.; Davidovitch, N.; Brammli-Greenberg, S.; Grifat, R.; Mesch, G.S. Factors associated with seasonal influenza and HPV vaccination uptake among different ethnic groups in Arab and Jewish society in Israel. Int. J. Equity Health 2021, 20, 201. [Google Scholar] [CrossRef]
- Yakut, N.; Soysal, S.; Soysal, A.; Bakir, M. Knowledge and acceptance of influenza and pertussis vaccinations among pregnant women of low socioeconomic status in Turkey. Hum. Vaccines Immunother. 2020, 16, 1101–1108. [Google Scholar] [CrossRef] [PubMed]
- Brockmann, S.O.; Wjst, S.; Zelmer, U.; Carollo, S.; Schmid, M.; Roller, G.; Eichner, M. ÖGD-Initiative zur Verbesserung der Durchimpfung bei Asylsuchenden [Public Health initiative for improved vaccination for asylum seekers. Bundesgesundheitsblatt Gesundh. Gesundh. 2016, 59, 592–598. [Google Scholar] [CrossRef]
- Burström, B.; Mellblom, J.; Marttila, A.; Kulane, A.; Martin, H.; Lindberg, L.; Burström, K. Healthcare utilisation and measles, mumps and rubella vaccination rates among children with an extended postnatal home visiting programme in a disadvantaged area in Stockholm, Sweden—A 3-year follow-up. Acta Paediatr. 2020, 109, 1847–1853. [Google Scholar] [CrossRef]
- Ceccarelli, G.; Vita, S.; Riva, E.; Cella, E.; Lopalco, M.; Antonelli, F.; De Cesaris, M.; Fogolari, M.; Dicuonzo, G.; Ciccozzi, M.; et al. Susceptibility to measles in migrant population: Implication for policy makers. J. Travel Med. 2018, 25, tax080. [Google Scholar] [CrossRef] [Green Version]
- Fabiani, M.; Ferrante, G.; Minardi, V.; Giambi, C.; Riccardo, F.; Declich, S.; Masocco, M. Comparison of rubella immunization rates in immigrant and Italian women of childbearing age: Results from the Italian behavioral surveillance system PASSI (2011–2015). PLoS ONE 2017, 12, e0178122. [Google Scholar] [CrossRef] [Green Version]
- Fozouni, L.; Weber, C.; Lindner, A.K.; Rutherford, G.W. Immunization coverage among refugee children in Berlin. J. Glob. Health 2019, 9, 010432. [Google Scholar] [CrossRef]
- Georgakopoulou, T.; Horefti, E.; Vernardaki, A.; Pogka, V.; Gkolfinopoulou, K.; Triantafyllou, E.; Tsiodras, S.; Theodoridou, M.; Mentis, A.; Panagiotopoulos, T. Ongoing measles outbreak in Greece related to the recent European-wide epidemic. Epidemiol. Infect. 2018, 146, 1692–1698. [Google Scholar] [CrossRef] [Green Version]
- Habersaat, K.B.; Pistol, A.; Stanescu, A.; Hewitt, C.; Grbic, M.; Butu, C.; Jackson, C. Measles outbreak in Romania: Understanding factors related to suboptimal vaccination uptake. Eur. J. Public Health 2020, 30, 986–992. [Google Scholar] [CrossRef] [PubMed]
- Hagstam, P.; Böttiger, B.; Winqvist, N. Measles and rubella seroimmunity in newly arrived adult immigrants in Sweden. Infect. Dis. 2019, 51, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Haider, E.A.; Willocks, L.J.; Anderson, N. Identifying inequalities in childhood immunisation uptake and timeliness in southeast Scotland, 2008–2018: A retrospective cohort study. Vaccine 2019, 37, 5614–5624. [Google Scholar] [CrossRef] [PubMed]
- Hudečková, H.; Stašková, J.; Mikas, J.; Mečochová, A.; Staroňová, E.; Polčičová, A.; Baška, T.; Novák, M.; Malinovská, N.; Zibolenová, J.; et al. Measles outbreak in a Roma community in the Eastern region of Slovakia, May to October 2018. Zdr. Varst. 2020, 59, 219–226. [Google Scholar] [CrossRef]
- Jablonka, A.; Happle, C.; Wetzke, M.; Dopfer, C.; Merkesdal, S.; Schmidt, R.E.; Behrens, G.M.N.; Solbach, P. Measles, Rubella and Varicella IgG Seroprevalence in a Large Refugee Cohort in Germany in 2015: A Cross-Sectional Study. Infect Dis Ther. 2017, 6, 487–496. [Google Scholar] [CrossRef] [Green Version]
- Suppli, C.H.; Dreier, J.W.; Rasmussen, M.; Andersen, A.-M.N.; Valentiner-Branth, P.; Mølbak, K.; Krause, T.G. Sociodemographic predictors are associated with compliance to a vaccination-reminder in 9692 girls age 14, Denmark 2014–2015. Prev. Med. Rep. 2018, 10, 93–99. [Google Scholar] [CrossRef]
- van den Heuvel, R.; Stammnitz, A. Masern-Impfung bei Asylsuchenden in der Erstaufnahmeeinrichtung (EAE) Bielefeld: Impfquote 73%, Impfablehnung 21 [Immunization Against Measles at the Asylum Center Bielefeld, Germany: Vaccination Rate 73%, Refusal Rate 21]. Gesundheitswesen 2020, 82, e67–e71. [Google Scholar] [CrossRef]
- Werber, D.; Hoffmann, A.; Santibanez, S.; Mankertz, A.; Sagebiel, D. Large measles outbreak introduced by asylum seekers and spread among the insufficiently vaccinated resident population, Berlin, October 2014 to August 2015. Eurosurveillance 2017, 22, 30599. [Google Scholar] [CrossRef] [Green Version]
- Byrne, L.; Ward, C.; White, J.M.; Amirthalingam, G.; Edelstein, M. Predictors of coverage of the national maternal pertussis and infant rotavirus vaccination programmes in England. Epidemiol. Infect. 2018, 146, 197–206. [Google Scholar] [CrossRef] [Green Version]
- Perry, M.; McGowan, A.; Roberts, R.; Cottrell, S. Timeliness and equity of infant pertussis vaccination in wales: Analysis of the three dose primary course. Vaccine 2020, 38, 1402–1407. [Google Scholar] [CrossRef]
- Hvass, A.M.F.; Wejse, C. High coverage of polio immunization program in refugees resettling in Denmark. A cross-sectional study of polio serology in newly arrived refugees. Expert Rev. Vaccines 2019, 18, 1317–1322. [Google Scholar] [CrossRef] [PubMed]
- Tayfur, I.; Günaydin, M.; Suner, S. Healthcare Service Access and Utilization among Syrian Refugees in Turkey. Ann. Glob. Health 2019, 85, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veronesi, L.; Colucci, M.E.; Capobianco, E.; Bracchi, M.T.; Zoni, R.; Palandri, L.; Affanni, P. Immunity status against poliomyelitis in young migrants: A seroprevalence study. Acta Biomed. 2020, 90, 28–34. [Google Scholar] [CrossRef]
- Hungerford, D.; Vivancos, R.; Read, J.M.; Iturriza-Gόmara, M.; French, N.; Cunliffe, N.A. Rotavirus vaccine impact and socioeconomic deprivation: An interrupted time-series analysis of gastrointestinal disease outcomes across primary and secondary care in the UK. BMC Med. 2018, 16, 1–14. [Google Scholar] [CrossRef]
- Ward, C.; Byrne, L.; White, J.M.; Amirthalingam, G.; Tiley, K.; Edelstein, M. Sociodemographic predictors of variation in coverage of the national shingles vaccination programme in England, 2014/15. Vaccine 2017, 35, 2372–2378. [Google Scholar] [CrossRef]
- Affanni, P.; Colucci, M.E.; Capobianco, E.; Bracchi, M.T.; Zoni, R.; Viani, I.; Caruso, L.; Carlone, L.; Arcuri, C.; Veronesi, L. Immunity status against tetanus in young migrants: A seroprevalence study. Acta Biomed. 2020, 91, 77–84. [Google Scholar] [CrossRef]
- Ahmad, B.B.; Kristensen, K.L.; Glenthoej, J.P.; Poulsen, A.; Bryld, A.-G.; Huber, F.G.; Andersen, E.M.; Ravn, P. Latent tuberculosis infection among minor asylum seekers in Denmark. Eur. Respir. J. 2020, 55, 1901688. [Google Scholar] [CrossRef]
- Fritschi, N.; Schmidt, A.J.; Hammer, J.; Ritz, N.; Unit, S.P.S. Pediatric Tuberculosis Disease during Years of High Refugee Arrivals: A 6-Year National Prospective Surveillance Study. Respiration 2021, 100, 1050–1059. [Google Scholar] [CrossRef]
- Larsen, F.D.; Jespersen, S.; Wejse, C.; Petersen, E.; Larsen, C.S. One-sixth of inpatients in a Danish infectious disease ward have imported diseases: A cross-sectional analysis. Travel Med. Infect. Dis. 2017, 20, 43–48. [Google Scholar] [CrossRef]
- Decuyper, I.I.; Van Damme, P.; Soentjens, P.; Wojciechowski, M. Low adherence with national travel medicine recommendations in Belgian expatriate children: A retrospective analysis. Travel Med. Infect. Dis. 2019, 32, 101424. [Google Scholar] [CrossRef]
- Ganczak, M.; Bielecki, K.; Drozd-Dąbrowska, M.; Topczewska, K.; Biesiada, D.; Molas-Biesiada, A.; Dubiel, P.; Gorman, D. Vaccination concerns, beliefs and practices among Ukrainian migrants in Poland: A qualitative study. BMC Public Health 2021, 21, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Pohl, C.; Mack, I.; Schmitz, T.; Ritz, N. The spectrum of care for pediatric refugees and asylum seekers at a tertiary health care facility in Switzerland in 2015. Eur. J. Pediatr. 2017, 176, 1681–1687. [Google Scholar] [CrossRef] [PubMed]
- Letley, L.; Rew, V.; Ahmed, R.; Habersaat, K.B.; Paterson, P.; Chantler, T.; Saavedra-Campos, M.; Butler, R. Tailoring immunisation programmes: Using behavioural insights to identify barriers and enablers to childhood immunisations in a Jewish community in London, UK. Vaccine 2018, 36, 4687–4692. [Google Scholar] [CrossRef]
- Jenness, S.M.; Aavitsland, P.; White, R.A.; Winje, B.A. Measles vaccine coverage among children born to Somali immigrants in Norway. BMC Public Health 2021, 21, 1–8. [Google Scholar] [CrossRef]
- Elran, B.; Yaari, S.; Glazer, Y.; Honovich, M.; Grotto, I.; Anis, E. Parents’ perceptions of childhood immunization in Israel: Information and concerns. Vaccine 2018, 36, 8062–8068. [Google Scholar] [CrossRef]
- Tessier, E.; Warburton, F.; Tsang, C.; Rafeeq, S.; Boddington, N.; Sinnathamby, M.A.; Pebody, R. Population-level factors predicting variation in influenza vaccine uptake among adults and young children in England, 2015/16 and 2016/17. Vaccine 2018, 36, 3231–3238. [Google Scholar] [CrossRef]
- Klok-Nentjes, S.; Tramper-Stranders, G.A.; van Dam-Bakker, E.D.M.; Beldman, J. Undocumented children in the Amsterdam region: An analysis of health, school, and living circumstances. Eur. J. Pediatr. 2018, 177, 1057–1062. [Google Scholar] [CrossRef]
- Ellis, N.; Walker-Todd, E.; Heffernan, C. Influences on childhood immunisation decision-making in London’s Gypsy and Traveller communities. Br. J. Nurs. 2020, 29, 822–826. [Google Scholar] [CrossRef]
- Kundi, M.; Obermeier, P.; Helfert, S.; Oubari, H.; Fitzinger, S.; Yun, J.; Brix, M.; Rath, B. The Impact of the Parent-Physician Relationship on Parental Vaccine Safety Perceptions. Curr. Drug Saf. 2015, 10, 16–22. [Google Scholar] [CrossRef]
- Godefroy, R.; Chaud, P.; Ninove, L.; Dina, J.; Decoppet, A.; Casha, P.; Hraiech, S.; Brouqui, P.; Cassir, N. Measles outbreak in a French Roma community in the Provence-Alpes-Côte d’Azur region, France, May to July 2017. Int. J. Infect. Dis. 2018, 76, 97–101. [Google Scholar] [CrossRef] [Green Version]
- Thomson, A.; Robinson, K.; Vallée-Tourangeau, G. The 5As: A practical taxonomy for the determinants of vaccine uptake. Vaccine 2016, 34, 1018–1024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Habersaat, K.B.; Jackson, C. Understanding vaccine acceptance and demand—and ways to increase them. Bundesgesundheitsblatt Gesundh. Gesundh. 2020, 63, 32–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giambi, C.; Del Manso, M.; Dente, M.G.; Napoli, C.; Montaño-Remacha, C.; Riccardo, F.; Declich, S. Network for the control of cross-border health threats in the Mediterranean Basin and Black Sea for the ProVacMed project Immunization Strategies Targeting Newly Arrived Migrants in Non-EU Countries of the Mediterranean Basin and Black Sea. Int. J. Environ. Res. Public Health 2017, 14, 459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seeber, L.; Conrad, T.; Hoppe, C.; Obermeier, P.; Chen, X.; Karsch, K.; Muehlhans, S.; Tief, F.; Boettcher, S.; Diedrich, S.; et al. Educating parents about the vaccination status of their children: A user-centered mobile application. Prev. Med. Rep. 2017, 5, 241–250. [Google Scholar] [CrossRef]
- Chiesa, V.; Chiarenza, A.; Mosca, D.; Rechel, B. Health records for migrants and refugees: A systematic review. Health Policy 2019, 123, 888–900. [Google Scholar] [CrossRef] [PubMed]
- Shet, A.; Carr, K.; Danovaro-Holliday, M.C.; Sodha, S.V.; Prosperi, C.; Wunderlich, J.; Wonodi, C.; Reynolds, H.W.; Mirza, I.; Gacic-Dobo, M.; et al. Impact of the SARS-CoV-2 pandemic on routine immunisation services: Evidence of disruption and recovery from 170 countries and territories. Lancet Glob. Health 2022, 10, e186–e194. [Google Scholar] [CrossRef]
- World Health Organization. Correlates of Vaccine-Induced Protection: Methods and Implications; Contract No.: WHO/IVB/13.01; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Earle, K.A.; Ambrosino, D.M.; Fiore-Gartland, A.; Goldblatt, D.; Gilbert, P.B.; Siber, G.R.; Dull, P.; Plotkin, S.A. Evidence for antibody as a protective correlate for COVID-19 vaccines. Vaccine 2021, 39, 4423–4428. [Google Scholar] [CrossRef]
- Plotkin, S.A. Complex correlates of protection after vaccination. Clin. Infect. Dis. 2013, 56, 1458–1465. [Google Scholar] [CrossRef]
- De Gomensoro, E.; Del Giudice, G.; Doherty, T.M. Challenges in adult vaccination. Ann. Med. 2018, 50, 181–192. [Google Scholar] [CrossRef]
- Kamal, A.; Hodson, A.; Pearce, J.M. A Rapid Systematic Review of Factors Influencing COVID-19 Vaccination Uptake in Minority Ethnic Groups in the UK. Vaccines 2021, 9, 1121. [Google Scholar] [CrossRef]
- Lorini, C.; Santomauro, F.; Donzellini, M.; Capecchi, L.; Bechini, A.; Boccalini, S.; Bonanni, P.; Bonaccorsi, G. Health literacy and vaccination: A systematic review. Hum. Vaccines Immunother. 2018, 14, 478–488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prins, W.; Butcher, E.; Hall, L.L.; Puckrein, G.; Rosof, B. Improving adult immunization equity: Where do the published research literature and existing resources lead? Vaccine 2017, 35, 3020–3025. [Google Scholar] [CrossRef] [PubMed]
- Crocker-Buque, T.; Edelstein, M.; Mounier-Jack, S. Interventions to reduce inequalities in vaccine uptake in children and adolescents aged <19 years: A systematic review. J. Epidemiol. Community Health 2017, 71, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Cheng, I.-H.; Wahidi, S.; Vasi, S.; Samuel, S. Importance of community engagement in primary health care: The case of Afghan refugees. Aust. J. Prim. Health 2015, 21, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Wångdahl, J.; Lytsy, P.; Mårtensson, L.; Westerling, R. Health literacy among refugees in Sweden—A cross-sectional study. BMC Public Health 2014, 14, 1030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, L.E.; Amlôt, R.; Weinman, J.A.; Yiend, J.; Rubin, G.J. A systematic review of factors affecting vaccine uptake in young children. Vaccine 2017, 35, 6059–6069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McFadden, A.; Siebelt, L.; Gavine, A.; Atkin, K.; Bell, K.; Innes, N.; Jones, H.; Jackson, C.; Haggi, H.; MacGillivray, S. Gypsy, Roma and Traveller access to and engagement with health services: A systematic review. Eur. J. Public Health 2018, 28, 74–81. [Google Scholar] [CrossRef]
- Jarrett, C.; Wilson, R.; O’Leary, M.; Eckersberger, E.; Larson, H.J.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; et al. Strategies for Addressing Vaccine Hesitancy-A Systematic Review. Vaccine 2015, 33, 4180–4190. [Google Scholar] [CrossRef] [Green Version]
- Zuanna, T.D.; Del Manso, M.; Giambi, C.; Riccardo, F.; Bella, A.; Caporali, M.G.; Dente, M.G.; Declich, S. The Italian Survey CARE Working Group Immunization Offer Targeting Migrants: Policies and Practices in Italy. Int. J. Environ. Res. Public Health 2018, 15, 968. [Google Scholar] [CrossRef] [Green Version]
- Odone, A.; Fara, G.M.; Giammaco, G.; Blangiardi, F.; Signorelli, C. The future of immunization policies in Italy and in the European Union: The Declaration of Erice. Hum. Vaccines Immunother. 2015, 11, 1268–1271. [Google Scholar] [CrossRef] [Green Version]
- European Centre for Disease Prevention and Control. Monitoring and Evaluation Framework for COVID-19 Response Activities in the EU/EEA and the UK, 17 June 2020; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2020.


{kind=link}
| Vaccine Types | Countries Represented | No. of Studies | Included Studies (Authors, Year) |
|---|---|---|---|
| BCG | England, Germany, Scotland, Switzerland, Turkey | 7 | Bell et al. (2020) [18], Boukamel et al. (2020) [19], Ergönül et al. (2019) [20], Gorman et al. (2019) [21], Mueller-Hermelink et al. (2018) [22], Öztaş et al. (2020) [23], Ergönül et al. (2019) [20] |
| COVID-19 | Israel, Italy, Norway the United Kingdom, Wales | 19 | Ali-Saleh et al. (2022) [24], Bentivegna et al. (2022) [25], Blakeway et al. (2022) [26], Cook et al. (2022) [27], Gaughan et al. (2022) [28], Glampson et al. (2021) [29], Gorelik et al. (2022) [30], Hall et al. (2021) [31], Iacoella et al. (2021) [32], Kraft et al. (2022) [33], Martin et al. (2021) [34], Muhsen et al. (2021) [35], Nafilyan et al. (2021) [36], Nguyen et al. (2022) [37], Perry et al. (2021) [38], Saban et al. (2021) [39], Taubman- Ben-Ari et al. (2022) [40], Tessier et al. (2022) [41], Watksinson et al. (2022) [42] |
| Diphtheria (DTP/DaPT/DTap) | Denmark, England, Finland, Germany, Greece, Israel, Italy, The Netherlands, Switzerland, Turkey, the United Kingdom, Wales | 14 | Dixon et al. (2016) [43], Ergönül et al. (2019) [20], Freidl et al. (2018) [44], Jablonka et al. (2017) [45], Jackson et al. (2017) [46], Louka et al. (2019) [47], Mellou et al. (2019) [48], Nakken et al. (2018) [49], Perry et al. (2020) [50], Sane et al. (2016) [51], Staehelin et al. (2019) [52], Stein-Zamir et al. (2017) [53], Stein-Zamir et al. (2019) [54], Vita et al. (2019) [55] |
| Hepatitis (A, B, C) | England, Finland, Germany, Greece, Israel, Italy, The Netherlands, Spain, Switzerland, Turkey | 21 | Cuomo et al. (2019) [56], Ergönül et al. (2019) [20], Fougère et al. (2018) [57], Freidl et al. (2018) [44], Führer et al. (2016) [58], Iacoella et al. (2021) [32], Jablonka et al. (2017) [45], Karaşahin et al. (2021) [59], Köse et al. (2017) [60], Louka et al. (2019) [47], Mazzitelli et al. (2021) [61], Mellou et al. (2017) [62], Mellou et al. (2019) [48], Norman et al. (2021) [63], Öztaş et al. (2020) [23], Serre-Delcor et al. (2018) [64], Staehelin et al. (2019) [52], Stein-Zamir et al. (2019) [54], Taylor et al. (2019) [65], Vita et al. (2019) [55], Vu et al. (2020) [66] |
| HiB | Denmark, England, Greece, Israel, Turkey | 5 | Dixon et al. (2016) [43], Ergönül et al. (2019) [20], Mellou et al. (2019) [48], Nakken et al. (2018) [49], Stein-Zamir et al. (2019) [54] |
| Influenza | England, Germany, Greece, Israel, Italy, The Netherlands, Scotland, Turkey, the United Kingdom, Wales | 20 | Bechini et al. (2018) [67], Bell et al. (2020) [18], Bielecki et al. (2019) [68], Bielecki et al. (2020) [69], Boddington et al. (2019) [70], Fortunato et al. (2018) [71], Glatman-Freedman et al. (2019) [72], Gorman et al. (2019) [21], Gorman et al. (2020) [73], Hardelid et al. (2016) [74], Hungerford et al. (2018) [75], Iacoella et al. (2021) [32], Jackson et al. (2017) [46], Loiacono et al. (2020) [76], Louka et al. (2019) [47], Natan et al. (2016) [77], Perniciaro et al. (2018) [78], Shahbabi et al. (2021) [79], Watksinson et al. (2022) [42], Yakut et al. (2020) [80] |
| Measles, Mumps, Rubella (MMR/MMRV/MMRV1/ MMRV2) | Denmark, England, Germany, Greece, Israel, Italy, The Netherlands, Scotland, Slovakia, Spain, Sweden, Switzerland, Turkey, Wales | 29 | Bell et al. (2020) [18], Brockmann et al. (2016) [81], Burström et al. (2020) [82], Ceccarelli et al. (2018) [83], Dixon et al. (2016) [43], Ergönül et al. (2019) [20], Fabiani et al. (2017) [84], Freidl et al. (2018) [44], Fozouni et al. (2019) [85], Georgakopoulou et al. (2018) [86], Habersaat et al. (2020) [87], Hagstam et al. (2019) [88], Haider et al. (2019) [89], Hudečková et al. (2020) [90], Jablonka et al. (2017) [45], Jablonka et al. II (2017) [91], Louka et al. (2019) [47], Mellou et al. (2019) [48], Nakken et al. (2018) [49], Norman et al. (2021) [63], Öztaş et al. (2020) [23], Perry et al. (2020) [50], Staehelin et al. (2019) [52], Stein-Zamir et al. (2017) [53], Stein-Zamir et al. (2019) [54], Suppli et al. (2018) [92], Van Den Heuvel R. et al. (2018) [93], Vita et al. (2019) [55], Werber et al. (2017) [94] |
| Meningococcal/MCV/MenC | England, Greece, Italy, Wales | 4 | Dixon et al. (2016) [43], Georgakopoulou et al. (2018) [86], Perry et al. (2020) [50], Vita et al. (2019) [55] |
| Pertussis | England, Italy, Turkey, Wales | 5 | Byrne et al. (2017) [95], Dixon et al. (2016) [43], Perry et al. II (2020) [96], Vita et al. (2019) [55], Yakut et al. (2020) [80] |
| Pneumonia/PCV/Invasive pneumococcal disease (IPD)/Prevnar/CPV | Denmark, England, Greece, Israel, Italy, Turkey | 6 | Dixon et al. (2016) [43], Ergönül et al. (2019) [20], Mellou et al. (2019) [48], Nakken et al. (2018) [49], Öztaş et al. (2020) [23], Stein-Zamir et al. (2019) [54], Vita et al. (2019) [55] |
| Polio/OPV/IPV | Denmark, England, Germany, Greece, Israel, Italy, The Netherlands, Turkey, the United Kingdom | 13 | Dixon et al. (2016) [43], Fozouni et al. (2019) [85], Freidl et al. (2018) [44], Hvass et al. (2019) [97], Jackson et al. (2017) [46], Louka et al. (2019) [47], Mellou et al. (2019) [48], Nakken et al. (2018) [49], Öztaş et al. (2020) [23], Stein-Zamir et al. (2019) [54], Tayfur et al. (2019) [98], Veronesi et al. (2019) [99], Vita et al. (2019) [55] |
| Rotavirus | England/the United Kingdom | 3 | Byrne et al. (2017) [95], Dixon et al. (2016) [43], Hungerford et al. II (2018) [100] |
| Shingles | The United Kingdom | 1 | Ward et al. (2017) [101] |
| Tetanus | England, Germany, Greece, Italy The Netherlands, Switzerland, Turkey, the United Kingdom | 11 | Affani et al. (2020) [102], Dixon et al. (2016) [43], Ergönül et al. (2019) [20], Fozouni et al. (2019) [85], Freidl et al. (2018) [44], Führer et al. (2016) [58], Jablonka et al. (2017) [45], Jackson et al. (2017) [46], Louka et al. (2019) [47], Staehelin et al. (2019) [52], Vita et al. (2019) [55] |
| Tuberculosis | Denmark, Italy, Switzerland | 3 | Ahmad et al. (2020) [103], Fritschi et al. (2021) [104], Iacoella et al. (2021) [32] |
| Varicella/VZV | Germany, The Netherlands Spain, Switzerland, Turkey, the United Kingdom | 7 | Ergönül et al. (2019) [20], Freidl et al. (2018) [44], Jablonka et al. II (2017) [91], Norman et al. (2021) [63], Öztaş et al. (2020) [23], Staehelin et al. (2019) [52], Ward et al. (2017) [101] |
| Whooping cough | The United Kingdom | 1 | Jackson et al. (2017) [46] |
| General/Multiple vaccines/Combination vaccines | Belgium, Denmark, Italy, Poland, Switzerland, Turkey | 6 | Dam Larsen et al. (2017) [105], Decuyper et al. (2019) [106], Ganczak et al. (2021) [107], Pohl et al. (2017) [108], Vita et al. (2019) [55], Öztaş et al. (2020) [23] |
| Levels | Drivers | Barriers | Facilitators |
|---|---|---|---|
| National |
|
|
|
| Healthcare service |
|
|
|
| Community |
|
|
|
| Individual |
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ekezie, W.; Awwad, S.; Krauchenberg, A.; Karara, N.; Dembiński, Ł.; Grossman, Z.; del Torso, S.; Dornbusch, H.J.; Neves, A.; Copley, S.; et al. Access to Vaccination among Disadvantaged, Isolated and Difficult-to-Reach Communities in the WHO European Region: A Systematic Review. Vaccines 2022, 10, 1038. https://doi.org/10.3390/vaccines10071038
Ekezie W, Awwad S, Krauchenberg A, Karara N, Dembiński Ł, Grossman Z, del Torso S, Dornbusch HJ, Neves A, Copley S, et al. Access to Vaccination among Disadvantaged, Isolated and Difficult-to-Reach Communities in the WHO European Region: A Systematic Review. Vaccines. 2022; 10(7):1038. https://doi.org/10.3390/vaccines10071038
Chicago/Turabian StyleEkezie, Winifred, Samy Awwad, Arja Krauchenberg, Nora Karara, Łukasz Dembiński, Zachi Grossman, Stefano del Torso, Hans Juergen Dornbusch, Ana Neves, Sian Copley, and et al. 2022. "Access to Vaccination among Disadvantaged, Isolated and Difficult-to-Reach Communities in the WHO European Region: A Systematic Review" Vaccines 10, no. 7: 1038. https://doi.org/10.3390/vaccines10071038