1. Introduction
The global COVID-19 pandemic caused by SARS-CoV-2 has infected an estimated 500 million people worldwide, as of April 2022 [
1]. Vaccination is one of the most effective strategies to reduce the severity and mortality caused by COVID-19; currently, inactivated, adenovirus-vectored, and mRNA are globally the most widely used vaccine platforms. Evidence has shown that these vaccines are effective and safe in healthy populations [
2]; however, impaired vaccine responses have been observed in autoimmune rheumatic disease (AIRD) patients. This has been attributed to the interplay between autoimmune activities along with the patients being on immunosuppressive therapies [
3].
Despite strong evidence that AIRD patients elicit a different response to COVID-19 vaccines compared to healthy individuals, data regarding this group of population are limited. Patients with AIRD are often excluded from vaccine studies, leading to limited data available to develop an appropriate vaccination guideline for this vulnerable group of the population. This leads to an important question: “Which type of COVID-19 vaccine is the most suitable for patients with AIRD?” Previous studies have shown that in normal individuals, mRNA vaccine elicits a robust humoral and cellular immune response when compared to the inactivated and adenovirus-vectored vaccines [
4], potentially making it an ideal choice for those on immunosuppressive drugs. Nevertheless, there has been no head-to-head comparison of immunogenicity and safety between vaccine types in AIRD patients thus far. The majority of existing studies only examined immune responses to a single vaccine type, either mRNA or inactivated vaccines [
5,
6,
7,
8], thus lacking a direct comparison. In addition, despite being one of the most widely used vaccines in the world, data on adenovirus-vectored vaccines in AIRD patients are still lacking.
Vaccine types vary across nations, depending on politics, national health programs, and availability. In Thailand, inactivated and adenovirus-vectored vaccines were the first to become available during the pandemic, followed by the mRNA vaccine. Leveraging the variety of vaccine types used in Thailand, we are able to study the heterogeneity among the immune response towards different types of vaccine types in AIRD patients. In this study, we compared both the humoral and cellular immune responses induced by inactivated, adenovirus-vectored, and heterogeneous adenovirus-vectored/mRNA vaccinated patients with systemic lupus erythematosus (SLE) and rheumatoid arthritis (RA).
2. Methods
This is a prospective cohort study investigating the safety and immunogenicity of an inactivated SARS-CoV-2 COVID-19 vaccine (CoronaVac or COVILO), an adenovirus-vectored vaccine (AZD1222, AstraZeneca, Cambridge, UK), and a heterologous regimen of adenovirus-vectored/mRNA vaccine (BNT162b2, Pfizer–BioNTech, New York, NY, USA) in SLE and RA patients. The Institutional Review Board of Chulalongkorn University’s Faculty of Medicine reviewed and approved the trial (882/2021), and it was registered in the Thai Clinical Trial Registry (TCTR20210917003).
2.1. Participants
Consecutively, SLE and RA patients aged 18–65 years who met the SLE or RA classification criteria were enrolled. Those with a history of SARS-CoV-2 infection, prior immunization with any SARS-CoV-2 vaccine, allergy to a vaccine component, pregnancy, and active disease at the time of enrollment were excluded. Participants meeting eligibility criteria were invited to participate in the study and provided written informed consent.
2.2. Procedure
At baseline, demographic information, current medications, disease activity, and relevant blood samples were collected. The SELENA-SLEDAI and Disease Activity Score 28 ESR (DAS28-ESR) were used to evaluate disease activity for patients with SLE and RA, respectively.
To standardize the various immunosuppressive treatment regimens used in our cohort, the Vasudev score was adopted and modified to calculate the total immunosuppressive load [
9]. One unit of immunosuppression was assigned for each of the following doses of immunosuppressive medications: prednisone 5 mg/day, mycophenolate mofetil (MMF) 500 mg/day, azathioprine 100 mg/day, cyclosporine 100 mg/day, tacrolimus 2 mg/day, leflunomide 10 mg/day, and methotrexate 15 mg/week (
Table 1). The immunosuppressive unit scale was calculated using the average doses of immunosuppressive medication from baseline to 30 days after the second vaccination.
A vaccine regimen was provided based on patient preference, availability, and hospital policy. For inactivated vaccines, there were two brands available in Thailand, CoronaVac (Sinovac Life Sciences, Beijing, China) and COVILO (Beijing Institute of Biological Products, Beijing, China). Each dose (0.5 mL) of CoronaVac and COVILO contains 600 SU and 3.9–10.4 U of inactivated SARS-CoV-2 virus, respectively. Two doses of vaccine were administered intramuscularly at a 4 week interval. For the adenovirus-vectored vaccine, two doses of AZD1222 (5 × 1010 viral particles, 0.5 mL each) were administered intramuscularly with an 8–12 week interval. For heterologous regimen, AZD1222 followed by 30 ug of BNT162b2 were administered intramuscularly with a 4–8 week interval.
2.3. Immunogenicity Assessment
On day 28 after completion of the regimen, blood samples were collected to assess immune responses and disease activities. The humoral responses were measured by total serum binding antibody levels against receptor-binding domain (RBD) of the SARS-CoV-2 spike (S) protein (Roche Diagnostics, Basel, Switzerland). Positive values were defined as 0.4 arbitrary U/mL (AU/mL).
The human IFN-γ ELISpot assay (ELISpot) was used to assess cellular immune responses in a random subset of patients in each vaccine group according to the instruction manual (Mabtech, Stockholm, Sweden) [
10]. In brief, pre-coated ELISpot plates were washed with phosphate-buffered saline (PBS) and blocked with RPMI1640 medium (Gibco, Waltham, MA, USA) containing 10% heat-inactivated fetal bovine serum (FBS) (Gibco, Waltham, MA, USA) (R10 medium) for 30 min at room temperature. A quantity of 2.5 × 10
5 PBMCs/well was stimulated for 40 h with SARS-CoV-2 spike peptide pools (S1 and S2) (Mimotopes, Victoria, Australia). Tests were performed in duplicate and with negative control (R10 medium) and positive control (phytohemagglutinin (PHA), Sigma-Aldrich, Burlington, MA, USA). After incubation, the plates were washed with PBS, and a secondary anti-IFN-γ antibody directly conjugated with alkaline phosphatase (7-B6-ALP) was added at the ratio of 1:200 in filtered PBS containing 0.5% FBS for 2 h at room temperature. After washing, the plates were incubated with 100 µL/well of substrate solution (BCIP/NBT-plus) until distinct spots emerged. The reaction was stopped by extensively washing in tap water and rinsing the underside of the membrane, and the plates were left to dry. Inspection and spots counting was performed in the ELISpot reader (ImmunoSpot
® Analyzer, Bonn, Germany). Results are expressed as spot-forming cells (SFCs)/10
6 PBMCs following the subtraction of negative controls. More than 50 spots per 10
6 peripheral blood mononuclear cells (PBMC) were considered positive.
2.4. Safety Assessment
Local and systemic reactogenicity was reviewed on day 7 following each vaccination. Assessment of disease activity was repeated on day 28 after the second vaccination by the previously mentioned scoring system.
2.5. Statistical Analyses
Baseline characteristics were reported as mean and standard deviations (SD), or median and interquartile range (IQR), as appropriate. The antibody titer was natural log(ln) transformed as an outcome measure to ensure normality, and was also presented as geometric mean titers (GMT) with a 95% confidence interval (CI). The normalized titer between vaccine groups was analyzed by one-way analysis of variance (one-way ANOVA) and post hoc multiple comparisons by Tukey’s method. Univariable, multivariable linear regression, and multivariable logistic regression analyses were performed to demonstrate the associations between immunogenicity and age, sex, AIRD diagnosis, and dosage of immunosuppressants. Disease activity scores before and after vaccination were compared using paired T-test. The percentage of cellular responsiveness and reactogenicity were compared among vaccine types using the chi-square statistic. All statistical analyses had α levels of <0.05 for defining significance. Data were statistically analyzed using JMP software V.13.2.1 (SAS Institute, Cary, NC, USA) and graphs were created using GraphPad Prism V.4.03 (GraphPad Software, La Jolla, CA, USA).
3. Results
The cohort consisted of 94 patients, with 64 (68%) having SLE and 30 (32%) having RA. Ninety-three percent of the patients were female. The inactivated, AZD1222, and AZD1222/BNT162b2 vaccines were administered to 23 (8 CoronaVac and 15 COVILO), 43, and 28 patients, respectively. The baseline characteristics, such as gender, disease duration, underlying autoimmune disease, and disease activity, were comparable between the vaccine groups. AZD1222 was primarily administered to the elderly in Thailand, reflected by the average age of those who received it being the highest among the vaccine types (
Table 2). In addition, the immunosuppressive load among those who received AZD1222 was less than those with other vaccine types.
3.1. Humoral Immune Responses
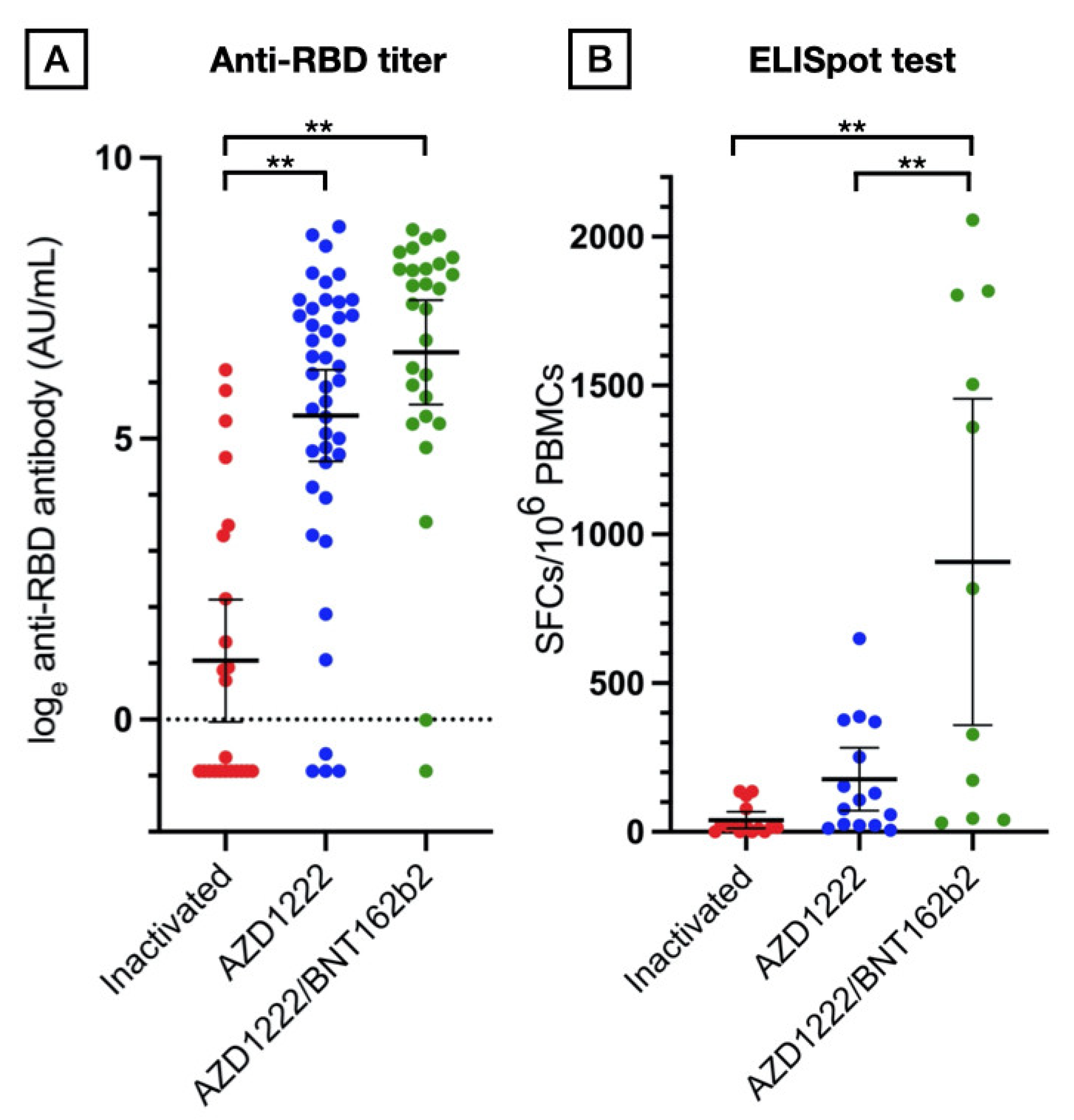
The inactivated vaccine group had the lowest seroconversion rate (52%) compared to AZD1222 (93%) and AZD1222/BNT162b2 (96%),
p < 0.0001. The anti-RBD titers were also lowest in the inactivated vaccine group (GMT 2.84 AU/mL; 95% CI 0.96 to 8.44), followed by AZD1222 (GMT 233.7 AU/mL; 95% CI 99.0 to 505.5), and AZD1222/BNT162b2 (GMT 688.6 AU/mL; 95% CI 271 to 1745),
p < 0.0001 (
Figure 1A). After adjusting for age, gender, diagnosis, and immunosuppressive load, the vaccine regimen remained an independent predictor of anti-RBD titer (
Table 3). The inactivated vaccine was associated with the lowest humoral response, while AZD1222/BNT162b2 was the highest. The immunosuppressive load was also negatively associated with anti-RBD titer (beta = −0.38; 95%CI −0.66 to −1.0,
p = 0.008) (
Figure 2).
3.2. Cellular Responses
The cellular immune response was assessed in 41 patients. In the inactivated vaccine, AZD1222, and AZD1222/BNT162b2 groups, there were 15, 15, and 11 patients, respectively. The baseline characteristics, including age, gender, underlying rheumatologic disease, and immunosuppressive load, were comparable between the vaccine groups (
p > 0.05). The proportion of patients who had a positive ELISpot test was lowest in the inactivated vaccine group, followed by the AZD1222 and the AZD1222/BNT162b2 vaccine groups (27%, 67%, and 73%, respectively,
p = 0.03). The mean ELISpot levels of each vaccine group also followed a similar trend (inactivated vaccine 39.73 (95% CI 11.41 to 68.06), AZD1222 176.7 (95% CI 70.98 to 282.4), and AZD1222/BNT162b2 907.1 (95% CI 358.9 to 1445),
p < 0.0001) (
Figure 1B). ELISpot level was weakly correlated with anti-RBD titer (r-square = 0.37,
p < 0.0001,
Supplemental Figure S1).
3.3. Safety, Reactogenicity, and Disease Activity
Most patients (90%) experienced at least one non-serious adverse reaction in both injections. Overall, the most reported adverse reaction was injection site pain (36%), followed by fatigue (21%) and fever (21%). Patients who had AZD1222 and AZD1222/BNT162b2 reported more injection site pain than for the inactivated vaccine (41.3%, 58.6% and 10.8%, respectively; p < 0.001).
A total of 34 SLE (48%) and 30 RA patients (90%) had complete data on disease activity scores pre- and post-vaccination. There was no difference in the change of SLEDAI score across the vaccine regimens in patients with SLE (95%CI −0.94 to 0.94;
p > 0.999). DAS28-ESR was lower in patients with RA after vaccination (95%CI −1.12 to −0.17;
p = 0.01) (
Supplemental Figure S2).
During the study period, two patients were infected with COVID-19. One patient was given AZD1222/BNT162b2 and developed COVID-19 infection one day after the second dose. The other received AZD1222 and had COVID-19 infection 29 days after the first dose.
4. Discussion
Despite the global strategy to use vaccination to limit the spread of COVID-19, data on their efficacy and adverse effects in individuals with AIRD are under-reported, because the individuals were often omitted from clinical studies that led to the vaccines’ approval [
11,
12,
13,
14]. In AIRD patients, an effective COVID-19 vaccine strategy is critical because altered vaccine responsiveness makes this population vulnerable to COVID-19 infection and severe complications [
15].
The anti-RBD titer is a valuable measure for estimating individual resistance to COVID-19 infection [
16]. A high anti-RBD titer also provides cross-protection against SARS-CoV2 variants of concern [
16]. In comparison, among the three vaccine regimens, we found that only half of the AIRD patients who received inactivated vaccines had seroconversion, whereas almost all of the patients who received AZD1222 and AZD1222/BNT162b2 were seroconverted. The mean anti-RBD titer of inactivated vaccine recipients was also lower than AZD1222 and AZD1222/BNT162b2 by 82 and 242 fold, respectively. Our findings were consistent with studies performed on the healthy population, where lower humoral response was reported in inactivated vaccine when compared to adenovirus-vectored or mRNA vaccine [
17,
18]. The other studies also found that heterologous adenovirus-vectored/mRNA vaccination was more immunogenic than homologous adenovirus-vectored vaccination [
19,
20]. Vaccine type remains to be a strong independent predictor of humoral immune response in AIRD patients, even when it is adjusted for other potential confounders, including baseline characteristics and immunosuppressive load.
Cellular immunity plays a pivotal role in long-term protection as well as reducing the severity of COVID-19 infection, while antibody titers wane over time [
21]. It also cross-reacts with the variants of concern that can evade neutralizing antibodies [
22,
23]. Nevertheless, there were only a few studies regarding cellular immunogenicity to mRNA vaccines in AIRD patients [
6] and none for the inactivated and adenovirus-vectored vaccines. Our study demonstrated that there was a weak association between anti-RBD titer and ELISpot level, and the pattern of cellular immune response of each vaccine type followed that of the humoral immune response. The proportion of patients with positive cellular immunity was lowest in inactivated vaccine recipients when compared to AZD1222 and AZD1222/BNT162b2.
Apart from the above findings, we also demonstrated an independent association between high immunosuppressive load and poor humoral immune response. A high potency vaccine should be strongly considered in AIRD patients to provide adequate humoral and cellular protection, especially for those who received a high immunosuppressive load.
Overall, every type of vaccine is well tolerated with only mild adverse reactions such as injection site pain or fever. The inactivated vaccine had the least local and systemic adverse reaction compared to the others. A finding from a cross-sectional study in Mexico evaluating adverse events of six COVID-19 vaccines in 225 AIRD patients was consistent with our study [
24]. There was no evidence of disease flares upon using any type of vaccine in our cohort, and no change in disease activity score was observed. Similar to our findings, other studies reported low incidence of AIRD flares in those receiving inactivated, adenovirus-vectored, and mRNA vaccines [
8,
25,
26,
27].
Limitations regarding the subject of our study include the number of participants, focusing primarily on SLE and RA patients and excluding other immunosuppressive regimens. Consequently, our results may not apply to other autoimmune diseases or those who received different types of immunosuppressive regimens, such as immunomodulatory biologic agents. Due to the limited sample size, we combined two brands of inactivated vaccines in the analysis, although their efficacy may not be equivalent. Our results may also not be applicable to those receiving homologous mRNA vaccines. It is also important to note that the immunosuppressive load calculation used within this research was adapted from a previous study that was based on arbitrary criteria. Furthermore, using anti-RBD seroconversion and ELISpot for T cell response might not fully reflect protection against the disease. However, there is mounting evidence that the levels of antibodies directed against the RBD domain of the spike protein measured in our study are a good predictor of vaccine efficacy [
28].
5. Conclusions
Different regimens of the COVID-19 vaccine are not equal in terms of immunogenicity. Most of them are safe and well-tolerated with no flare of autoimmune disease post-vaccination. Our study highlighted the urgent need for a booster dose of a high potency vaccine in patients with AIRD, particularly those who have previously received an inactivated vaccine or received high doses of immunosuppressants.
Supplementary Materials
The following supporting information can be downloaded at:
https://www.mdpi.com/article/10.3390/vaccines10060853/s1, Figure S1: Relationship between total anti-RBD Ig level and ELISpot after the second vaccination; Figure S2: Estimation plot of the difference in disease activity scores between pre- and post-vaccination, grouped by (A) Systemic lupus erythematosus and (B) Rheumatoid arthritis; Table S1: Number of participants according to the number of immunosuppressive drug used.
Author Contributions
T.A., T.L., S.S., N.O. and W.K. contributed to the conception and design of the work; acquisition, analysis, interpretation of data; drafting and revising the work. Y.P., Y.A., P.V., N.A., N.W. and S.B. contributed to data acquisition and final approval of the version to be published. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by a Rajadapisek Sompot, the Second Century Fund (C2F) Chulalongkorn University, Health Systems Research Institute (62-034), and National Science and Technology Development Agency (FDA-CO-2562-9090-TH).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Chulalongkorn University’s Faculty of Medicine (882/2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
The authors thank Mahachakri Sirindhorn Clinical Research Center, Faculty of Medicine, Chulalongkorn University for facility support, and Jariya Pongsaisopon and Sukanlaya Yoosomsuk for coordinating the study. Thanks are also due to Sasiwimol Ubolyam for enzyme-linked immunosorbent spot testing, and Sutthinee Lapchai for sample preparation and coding. Study data were collected and managed using REDCap electronic data capture tools hosted at Chula Data Management Center, Faculty of Medicine, Chulalongkorn University. We thank Chula Data Management Center, Faculty of Medicine, Chulalongkorn University for the REDCap administrative support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Worldometer. COVID-19 Pandemic. Available online: https://www.worldometers.info/coronavirus/ (accessed on 19 April 2022).
- Kyriakidis, N.C.; López-Cortés, A.; González, E.V.; Grimaldos, A.B.; Prado, E.O. SARS-CoV-2 vaccines strategies: A comprehensive review of phase 3 candidates. NPJ Vaccines 2021, 6, 28. [Google Scholar] [CrossRef] [PubMed]
- Bin Lee, A.R.Y.; Wong, S.Y.; Chai, L.Y.A.; Lee, S.C.; Lee, M.X.; Muthiah, M.D.; Tay, S.H.; Teo, C.B.; Tan, B.K.J.; Chan, Y.H.; et al. Efficacy of covid-19 vaccines in immunocompromised patients: Systematic review and meta-analysis. BMJ 2022, 376, e068632. [Google Scholar]
- Rotshild, V.; Hirsh-Raccah, B.; Miskin, I.; Muszkat, M.; Matok, I. Comparing the clinical efficacy of COVID-19 vaccines: A systematic review and network meta-analysis. Sci. Rep. 2021, 11, 22777. [Google Scholar] [CrossRef] [PubMed]
- Deepak, P.; Kim, W.; Paley, M.A.; Yang, M.; Carvidi, A.B.; Demissie, E.G.; El-Qunniet, A.A.; Haile, A.; Huang, K.; Kinnett, B.; et al. Effect of Immunosuppression on the Immunogenicity of mRNA Vaccines to SARS-CoV-2: A Prospective Cohort Study. Ann. Intern. Med. 2021, 174, 1572–1585. [Google Scholar] [CrossRef]
- Hadjadj, J.; Planas, D.; Ouedrani, A.; Buffier, S.; Delage, L.; Nguyen, Y.; Bruel, T.; Stolzenberg, M.-C.; Staropoli, I.; Ermak, N.; et al. Immunogenicity of BNT162b2 vaccine against the Alpha and Delta variants in immunocompromised patients with systemic inflammatory diseases. Ann. Rheum. Dis. 2022, 81, 720–728. [Google Scholar] [CrossRef]
- Tang, K.-T.; Hsu, B.-C.; Chen, D.-Y. Immunogenicity, Effectiveness, and Safety of COVID-19 Vaccines in Rheumatic Patients: An Updated Systematic Review and Meta-Analysis. Biomedicines 2022, 10, 834. [Google Scholar] [CrossRef]
- Yuki, E.F.N.; Borba, E.F.; Pasoto, S.G.; Seguro, L.P.; Lopes, M.; Saad, C.G.S.; Medeiros-Ribeiro, A.C.; Silva, C.A.; de Andrade, D.C.O.; de Vinci, K.; et al. Impact of Distinct Therapies on Antibody Response to SARS-CoV-2 Vaccine in Systemic Lupus Erythematosus. Arthritis Care Res. 2022, 74, 562–571. [Google Scholar] [CrossRef]
- Vasudev, B.; Hariharan, S.; Hussain, S.A.; Zhu, Y.R.; Bresnahan, B.A.; Cohen, E.P. BK virus nephritis: Risk factors, timing, and outcome in renal transplant recipients. Kidney Int. 2005, 68, 1834–1839. [Google Scholar] [CrossRef] [Green Version]
- Mabtech. Human IFN-γ ELISpot PRO kit Datasheet/Protocol [19 April 2022]. Available online: https://www.mabtech.com/sites/default/files/datasheets/3420-2APT-2.pdf (accessed on 19 April 2022).
- Palacios, R.; Patino, E.G.; de Oliveira Piorelli, R.; Conde, M.; Batista, A.P.; Zeng, G.; Xin, Q.; Kallas, E.G.; Flores, J.; Ockenhouse, C.F.; et al. Double-Blind, Randomized, Placebo-Controlled Phase III Clinical Trial to Evaluate the Efficacy and Safety of treating Healthcare Professionals with the Adsorbed COVID-19 (Inactivated) Vaccine Manufactured by Sinovac—PROFISCOV: A structured summary of a study protocol for a randomised controlled trial. Trials 2020, 21, 853. [Google Scholar]
- Thomas, S.J.; Moreira, E.D., Jr.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Polack, F.P.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine through 6 Months. N. Engl. J. Med. 2021, 385, 1761–1773. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillieet, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Zhang, Y.; Zeng, G.; Pan, H.; Li, C.; Hu, Y.; Chu, K.; Hanet, W.; Chen, Z.; Tang, R.; Yin, W.; et al. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine in healthy adults aged 18–59 years: A randomised, double-blind, placebo-controlled, phase 1/2 clinical trial. Lancet Infect. Dis. 2021, 21, 181–192. [Google Scholar] [CrossRef]
- Papagoras, C.; Fragoulis, G.E.; Zioga, N.; Simopoulou, T.; Deftereou, K.; Kalavri, E.; Zampeli, E.; Gerolymatou, N.; Kataxaki, E.; Melissaropoulos, K.; et al. Better outcomes of COVID-19 in vaccinated compared to unvaccinated patients with systemic rheumatic diseases. Ann. Rheum. Dis. 2021; ahead of print. [Google Scholar]
- Feng, S.; Phillips, D.J.; White, T.; Sayal, H.; Aley, P.K.; Bibi, S.; Dold, C.; Fuskova, M.; Gilbert, S.C.; Hirsch, I.; et al. Correlates of protection against symptomatic and asymptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 2032–2040. [Google Scholar] [CrossRef] [PubMed]
- Sughayer, M.A.; Souan, L.; Abu Alhowr, M.M.; Al Rimawi, D.; Siag, M.; Albadr, S.; Owdeh, M.; Al Atrash, T. Comparison of the effectiveness and duration of anti-RBD SARS-CoV-2 IgG antibody response between different types of vaccines: Implications for vaccine strategies. Vaccine 2022, 40, 2841–2847. [Google Scholar] [CrossRef]
- Wanlapakorn, N.; Suntronwong, N.; Phowatthanasathian, H.; Yorsaeng, R.; Vichaiwattana, P.; Thongmee, T.; Auphimai, C.; Srimuan, D.; Thatsanatorn, T.; Assawakosri, S.; et al. Safety and immunogenicity of heterologous and homologous inactivated and adenoviral-vectored COVID-19 vaccine regimens in healthy adults: A prospective cohort study. Hum. Vaccin Immunother. 2022, 18, 2029111. [Google Scholar] [CrossRef]
- Kang, C.-M.; Lee, N.-Y.; Lin, C.-H.; Hsu, Y.-S.; Chang, Y.-C.; Chung, M.-Y.; Lee, Y.-F.; Tseng, W.-P.; Wu, J.-L.; Chen, S.-Y.; et al. Immunogenicity and safety of homologous and heterologous ChAdOx1-S and mRNA-1273 vaccinations in healthy adults in Taiwan. J. Clin. Virol. 2022, 150–151, 105156. [Google Scholar] [CrossRef]
- Sheng, W.-H.; Chang, S.-Y.; Lin, P.-H.; Hsieh, M.-J.; Chang, H.-H.; Cheng, C.-Y.; Yanget, H.-C.; Pan, C.-F.; Ieong, S.-M.; Chao, T.-L.; et al. Immune response and safety of heterologous ChAdOx1-nCoV-19/mRNA-1273 vaccination compared with homologous ChAdOx1-nCoV-19 or homologous mRNA-1273 vaccination. J. Formos. Med. Assoc. 2022, 121, 766–777. [Google Scholar] [CrossRef]
- Sadarangani, M.; Marchant, A.; Kollmann, T.R. Immunological mechanisms of vaccine-induced protection against COVID-19 in humans. Nat. Rev. Immunol. 2021, 21, 475–484. [Google Scholar] [CrossRef]
- Geers, D.; Shamier, M.C.; Bogers, S.; den Hartog, G.; Gommers, L.; Nieuwkoop, N.N.; Schmitz, K.S.; Rijsbergen, L.C.; Van Osch, J.A.T.; Dijkhuizen, E.; et al. SARS-CoV-2 variants of concern partially escape humoral but not T-cell responses in COVID-19 convalescent donors and vaccinees. Sci. Immunol. 2021, 6, eabj1750. [Google Scholar] [CrossRef]
- Redd, A.D.; Nardin, A.; Kared, H.; Bloch, E.M.; Pekosz, A.; Laeyendecker, O.; Abel, B.; Fehlings, M.; Quinn, T.C.; Tobianet, A.A.R. CD8+ T-Cell Responses in COVID-19 Convalescent Individuals Target Conserved Epitopes from Multiple Prominent SARS-CoV-2 Circulating Variants. Open Forum Infect. Dis. 2021, 8, ofab143. [Google Scholar] [CrossRef]
- Esquivel-Valerio, J.A.; Skinner-Taylor, C.M.; Moreno-Arquieta, I.A.; Cardenas-de la Garza, J.A.; Garcia-Arellano, G.; Gonzalez-Garcia, P.L.; del Rocio Almaraz-Juarez, F.; Galarza-Delgado, D.A. Adverse events of six COVID-19 vaccines in patients with autoimmune rheumatic diseases: A cross-sectional study. Rheumatol. Int. 2021, 41, 2105–2108. [Google Scholar] [CrossRef] [PubMed]
- Cherian, S.; Paul, A.; Ahmed, S.; Alias, B.; Manoj, M.; Santhosh, A.K.; Varghese, D.R.; Krishnan, N.; Shenoy, P. Safety of the ChAdOx1 nCoV-19 and the BBV152 vaccines in 724 patients with rheumatic diseases: A post-vaccination cross-sectional survey. Rheumatol. Int. 2021, 41, 1441–1445. [Google Scholar] [CrossRef] [PubMed]
- Connolly, C.M.; Ruddy, J.A.; Boyarsky, B.J.; Barbur, I.; Werbel, W.A.; Geetha, D.; Garonzik-Wang, J.M.; Segev, D.L.; Christopher-Stine, L.; Paik, J.J. Disease Flare and Reactogenicity in Patients with Rheumatic and Musculoskeletal Diseases Following Two-Dose SARS-CoV-2 Messenger RNA Vaccination. Arthritis Rheumatol. 2022, 74, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Watad, A.; De Marco, G.; Mahajna, H.; Druyan, A.; Eltity, M.; Hijazi, N.; Haddad, A.; Elias, M.; Zisman, D.; Naffaa, M.E.; et al. Immune-Mediated Disease Flares or New-Onset Disease in 27 Subjects Following mRNA/DNA SARS-CoV-2 Vaccination. Vaccines 2021, 9, 435. [Google Scholar] [CrossRef] [PubMed]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccaset, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 


{kind=link}
{kind=link}