
Impact of Vaccine and Immunity Passports in the Context of COVID-19: A Time Series Analysis in Overseas France


{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Scope, Design and Objectives
2.2. Inclusion and Data Collection
2.3. Data Analysis
3. Results
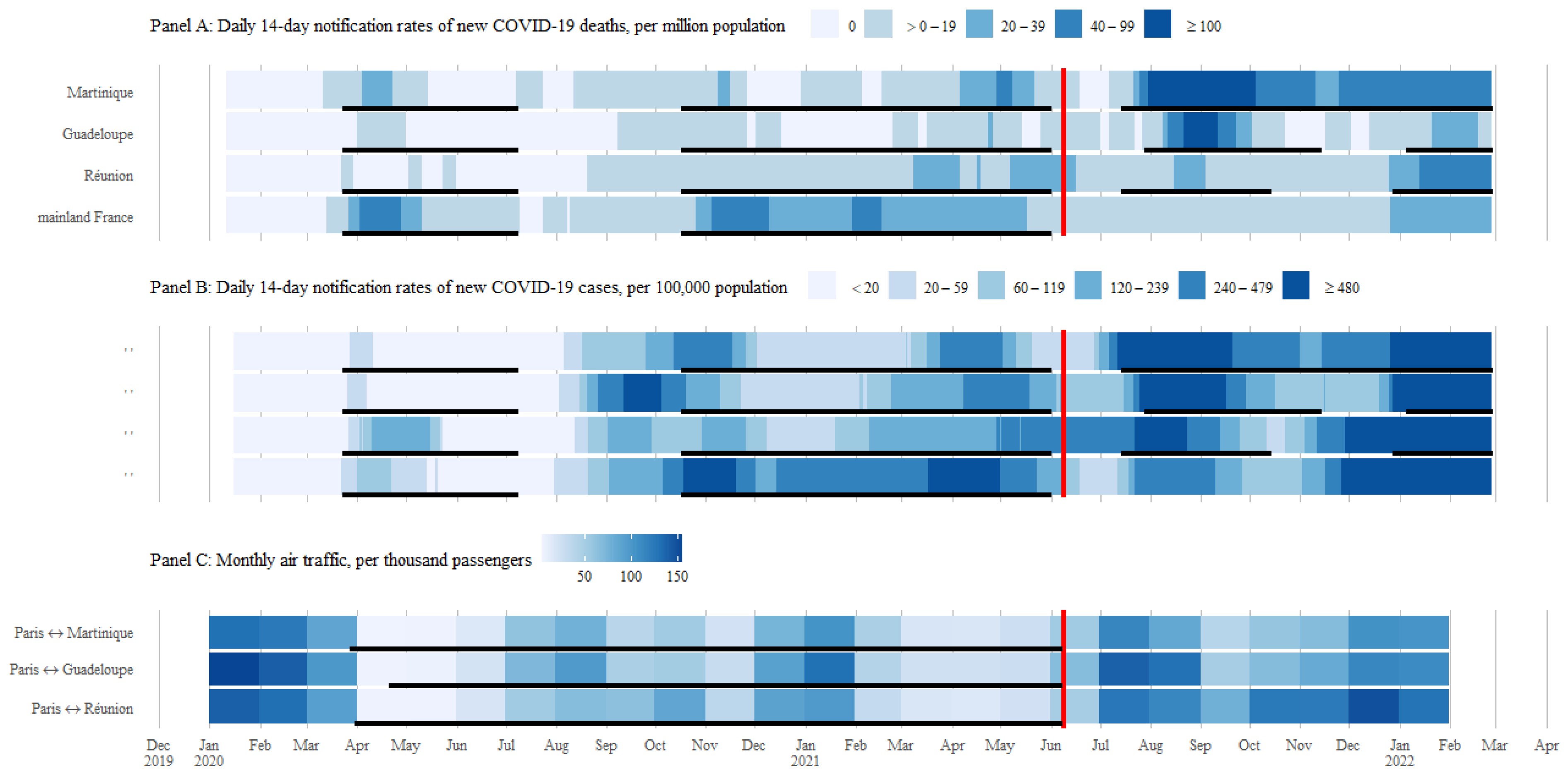
3.1. Description of COVID-19 Transmission and Mortality Compared to the Adoption of Immunity Passports
3.2. Timeline of States of Health Emergency in Relation to the Adoption of Immunity Passports
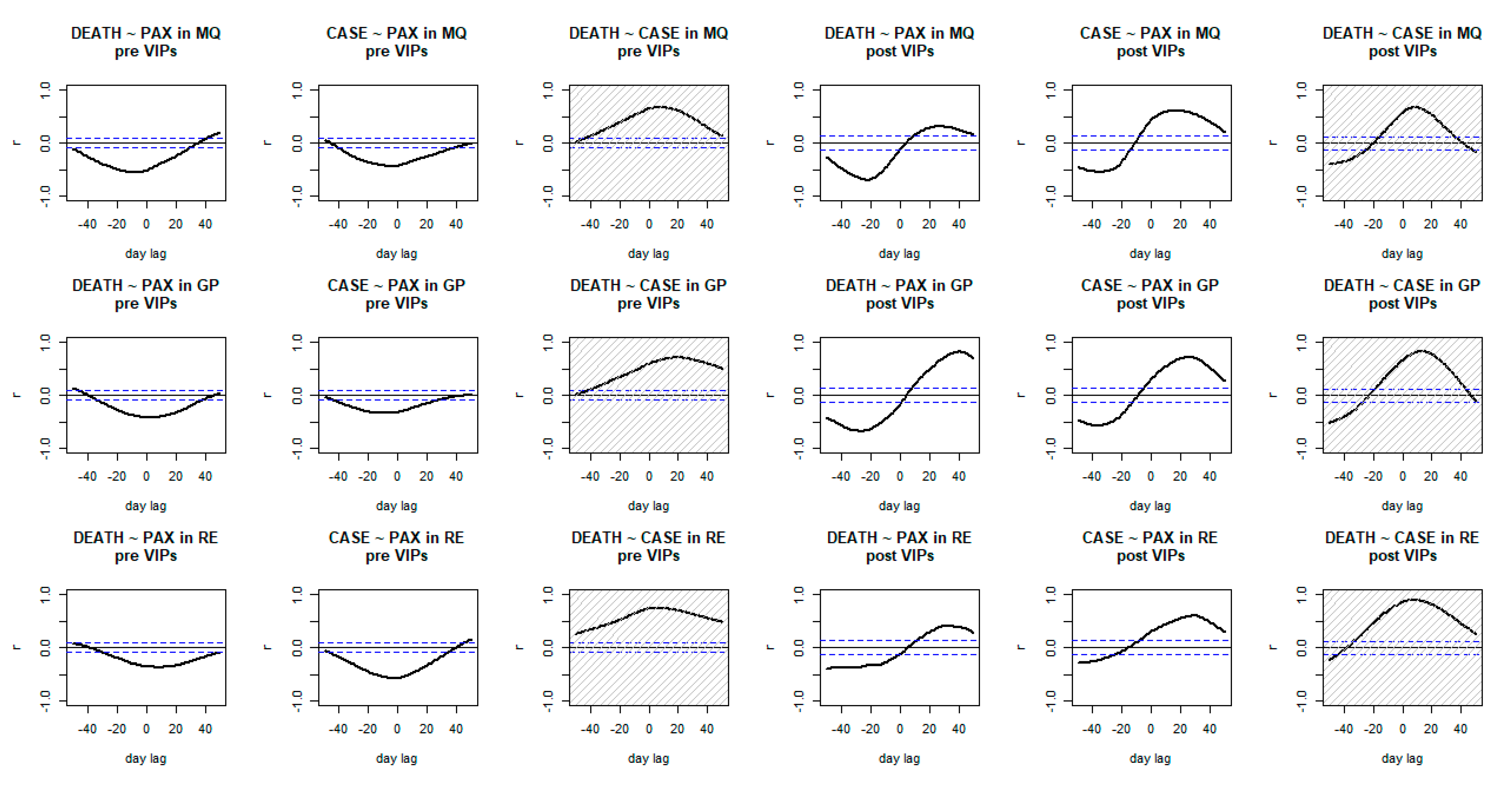
3.3. Time Correlations of COVID-19 and Air Traffic with Paris in Overseas France in Relation to the Adoption of Immunity Passports
4. Discussion
4.1. Breaking the Circle of Blame
4.2. Methods and Results’ Repeatability
4.3. The Practicality of the Cross-Sectoral Routine Surveillance
4.4. Limits of the Study
4.5. Policy Recommendations
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- French Transport Ministry. 2020 Statistical Bulletin—Commercial Air Traffic (Bulletin Statistique 2020—Trafic Aérien Commercial); French Transport Ministry: Paris, France, 2021. [Google Scholar]
- French Transport Ministry. 2019 Statistical Bulletin—Commercial Air Traffic (Bulletin Statistique 2019—Trafic Aérien Commercial); French Transport Ministry: Paris, France, 2020. [Google Scholar]
- French Ecology Ministry. COVID-19: Mandatory Test and End of Quarantine in July and August in the Overseas Territories (COVID-19: Test Obligatoire et Fin de Quarantaines en Juillet et en Août Dans les Territoires d’Outre-mer). Available online: https://archive.ph/OFdHY (accessed on 2 February 2022).
- French Overseas Ministry. Changes to the Rules Applicable to Passengers to and from Overseas Territories, as of 9th June (Évolution des Règles Applicables Aux Passagers à Destination et en Provenance des Outre-mer, à Compter du 9 Juin). Available online: https://archive.ph/nfilA (accessed on 2 February 2022).
- Dominica Government Cruise Ship to Return to Dominica in June 2021. Available online: https://archive.ph/jFk6s (accessed on 26 February 2022).
- DASPA Cruise Schedule 2021/22. Available online: https://www.domports.daspa.dm/index.php/maritime/daspa-cruise-schedule/ (accessed on 23 February 2022).
- WHO Dominica—WHO Coronavirus (COVID-19) Dashboard with Vaccination Data. Available online: https://covid19.who.int/region/amro/country/dm (accessed on 26 February 2022).
- Ryan, M. COVID-19 Virtual Press Conference Transcript—1 February 2022; WHO Team: Geneva, Switzerland, 2022. [Google Scholar]
- Decoster, K. IHP News 656: On the ‘Fair Share Model’ We Urgently Need for our Pre-Revolutionary Times. Available online: https://www.internationalhealthpolicies.org/wp-content/uploads/2022/02/IHPn656.pdf (accessed on 11 February 2022).
- WHO Interim Position Paper: Considerations Regarding proof of COVID-19 Vaccination for International Travellers. Available online: https://archive.ph/8XLog (accessed on 22 February 2022).
- World Health Organization. Digital Documentation of COVID-19 Certificates: Vaccination Status—Technical Specifications and Implementation Guidances; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- WHO. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—24 November 2021. Available online: https://archive.ph/BvEaD (accessed on 11 February 2022).
- World Travel & Tourism Council. Tourism & Travel Economic Impact 2021; World Travel & Tourism Council: London, UK, 2021. [Google Scholar]
- European Commission. Study on the Impact of the COVID-19 Pandemic on the Outermost Regions: Factsheet—Martinique; Publications Office: Luxembourg, 2022.
- PAHO Low Vaccination Rates in the Caribbean must Be Urgently Addressed to Stop the Spread of COVID-19 Says PAHO Director. Available online: https://archive.ph/hd6Cn (accessed on 25 February 2022).
- INSEE. Tourism in the Caribbean: Winning Back a Larger Clientele (Le Tourisme Aux Antilles: À la Reconquête d’une plus Large Clientèle); INSEE: Paris, France, 2018.
- European Commission. Study on the Impact of the COVID-19 Pandemic on the Outermost Regions: Factsheet—Réunion; Publications Office: Luxembourg, 2022.
- European Commission. Study on the Impact of the COVID-19 Pandemic on the Outermost Regions: Factsheet—Guadeloupe; Publications Office: Luxembourg, 2022.
- WHO. Evidence to Recommendations: Methods Used for Assessing Health Equity and Human Rights Considerations in COVID-19 and Aviation; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- UNWTO. Exploring Safe Travel in the Age of Vaccines. Available online: https://archive.ph/8pQbK (accessed on 11 February 2022).
- World Travel & Tourism Council. #SafeTravels: Global Protocols & Stamp for the New Normal. Available online: https://archive.ph/tOK7i (accessed on 11 February 2022).
- UNWTO. World Tourism Remains at a Standstill as 100% of Countries Impose Restrictions on Travel. Available online: https://archive.ph/ieZ9Y (accessed on 25 February 2022).
- UNWTO. “Blanket Travel Restrictions Don’t Work”: UNWTO Adds Its Voice to WHO Statement. Available online: https://archive.ph/bOMO5 (accessed on 11 February 2022).
- UNWTO. WHO, UNWTO and WHO: Travel Measures Should be Based on Risk Assessment. Available online: https://archive.ph/2gAr7 (accessed on 25 February 2022).
- WHO. Evidence review: Public health measures in the aviation sector in the context of COVID-19: Quarantine and isolation: Tables and figures for ethical and equity considerations, 21 May 2021. Wkly. Epidemiol. Rec. 2021, 96, 165–172. [Google Scholar]
- UNWTO Committee on Tourism Ethics. Recommendation on COVID-19 Certificates for International Travel; UNWTO Committee on Tourism Ethics: Madrid, Spain, 2021. [Google Scholar]
- European Council. COVID-19: Council Updates Recommendation on Restrictions to Travel from Third Countries. Available online: https://archive.ph/kXcfj (accessed on 2 February 2022).
- French COVID-19 Scientific Council. Reacting now to Limit a New Wave Associated with the Delta Variant (Réagir Maintenant Pour Limiter une Nouvelle Vague Associée au Variant Delta); French COVID-19 Scientific Council: Paris, France, 2021.
- INSEE. Evolution of the Number of Deaths Between 1st June and 31st December 2021 (Évolution du Nombre de décès Entre le 1er Juin et le 31 Décembre 2021). Available online: https://archive.ph/AqR8Z (accessed on 13 February 2022).
- WHO French Polynesia: WHO Coronavirus Disease (COVID-19) Dashboard with Vaccination Data. Available online: https://archive.ph/sDatO (accessed on 8 April 2022).
- WHO Western Pacific. COVID-19 Situation Report for the Western Pacific Region—25th August 2021; WHO Western Pacific: Manila, Philippines, 2021. [Google Scholar]
- Prefect of Martinique. Press Communiqué—Urban Violence (Communiqué de Presse—Violences Urbaines); Prefect of Martinique: Martinique, France, 2021. [Google Scholar]
- French Overseas Ministry. Speech by Sébastien Lecornu on Guadeloupe (Allocution de Sébastien Lecornu sur la Guadeloupe). Available online: https://archive.ph/5ONXY (accessed on 8 April 2022).
- Ward, J.K.; Gauna, F.; Gagneux-Brunon, A.; Botelho-Nevers, E.; Cracowski, J.-L.; Khouri, C.; Launay, O.; Verger, P.; Peretti-Watel, P. The French health pass holds lessons for mandatory COVID-19 vaccination. Nat. Med. 2022, 28, 232–235. [Google Scholar] [CrossRef]
- France 24. France Postpones Vaccine Mandate after Violent Unrest in Martinique and Guadeloupe; France 24: Paris, France, 2021. [Google Scholar]
- Cruse, R. Frustration in the French Antilles. Available online: https://archive.ph/6zmKF (accessed on 22 February 2022).
- French Government Health Pass (Pass Sanitaire). Available online: https://archive.ph/vPytf (accessed on 9 April 2022).
- Santé Publique France. COVID-19: Weekly Epidemiological Update n° 68 of 17th June 2021 (COVID-19: Point Épidémiologique Hebdomadaire n° 68 du 17 Juin 2021); Santé Publique France: Paris, France, 2021.
- Health Department of French Polynesia. Weekly Epidemiological Bulletin COVID-19 #47 from 31/05 to 06/06/2021 (Bulletin Épidémiologique Hebdomadaire COVID-19 #47 du 31/05 au 06/06/2021); Health Department of French Polynesia: Papeete, France, 2021. [Google Scholar]
- Santé Publique France. COVID-19: Epidemiological Update of 7th April 2022 (COVID-19: Point Épidémiologique du 7 Avril 2022); Santé Publique France: Paris, France, 2022.
- Santé Publique France. COVID-19 and Other Respiratory Viruses in Réunion. Update as of 8th April 2022 (COVID-19 et Autres Virus Respiratoires à La Réunion. Point au 08 Avril 2022); Santé Publique France: Paris, France, 2022.
- Health Department of French Polynesia. Weekly Epidemiological Bulletin COVID-19 #88 from 21/03 to 27/03/2022 (Bulletin Épidémiologique Hebdomadaire COVID-19 #88 du 21/03 au 27/03/2022); Health Department of French Polynesia: Papeete, France, 2022; p. 6. [Google Scholar]
- Santé Publique France. COVID-19 Guadeloupe, St Martin, St Barth—Regional Epidemiological Point N°97 (COVID-19 Guadeloupe, St Martin, St Barth—Point Épidémio Régional N°97); Santé Publique France: Paris, France, 2022.
- Santé Publique France. COVID-19 Martinique—Regional Epidemiological Point N°94 (COVID-19 Martinique—Point Épidémio Régional N°94); Santé Publique France: Paris, France, 2022.
- French Overseas Ministry; French Health Ministry. For Better Protection of the Overseas Territories, Sébastien Lecornu and Olivier Véran Broaden the Target of the Vaccination Strategy in Several Territories (Pour une Meilleure Protection des Outre-mer, Sébastien Lecornu et Olivier Véran élargissent la Cible de la Stratégie de Vaccination dans Plusieurs Territoires). Available online: https://archive.ph/yrDBM (accessed on 8 April 2022).
- French COVID-19 Scientific Council. Extension of the State of Health Emergency in the Overseas Territories until November 15, 2021 (Prolongation de l’État d’Urgence Sanitaire dans les Territoires d’Outre-Mer Jusqu’au 15 Novembre 2021); French COVID-19 Scientific Council: Paris, France, 2021. [Google Scholar]
- Santé Publique France. Géodes. Available online: https://geodes.santepubliquefrance.fr/#c=indicator&selcodgeo=02&view=map1 (accessed on 10 February 2022).
- French Ministry of Transport. TendanCIEL—Air Traffic Statistics (Statistiques du Trafic Aérien); French Ministry of Transport: Paris, France, 2022. [Google Scholar]
- Redon, M. Migrations and Border: The Case of Saint Martin (Migrations et Frontière: Le cas de Saint-Martin). Études Caribéennes 2007. [Google Scholar] [CrossRef]
- Marie, C.-V. Reference point—Sociodemographic changes in the overseas departments: New societies, new issues, new challenges (Point de repère—Mutations sociodémographiques dans les Dom: Nouvelles sociétés, nouveaux enjeux, nouveaux défis). Inf. Soc. 2014, 186, 10–15. [Google Scholar]
- Santé Publique France. COVID-19 Regional Epidemiological Point n°100-2022—French Guiana (Point Épidémio Régional COVID-19 n°100-2022—Guyane); Santé Publique France: Paris, France, 2022.
- Pison, G. The population of France in 2005 (La population de la France en 2005). Popul. Soc. 2006, 421, 1–4. [Google Scholar]
- Santé Publique France. Public Health Bulletin COVID-19 in Martinique, December 2021 (Bulletin de Santé Publique COVID-19 en Martinique, Décembre 2021); Santé Publique France: Paris, France, 2021.
- INSEE. Economic Report 2020—Martinique (Bilan Économique 2020—Martinique). Available online: https://archive.ph/NSppC (accessed on 6 March 2022).
- INSEE. Economic Report 2020—Guadeloupe (Bilan Économique 2020—Guadeloupe). Available online: https://archive.ph/zzSkg (accessed on 9 March 2022).
- INSEE. Economic Report 2020—Réunion (Bilan Économique 2020—La Réunion). Available online: https://www.insee.fr/fr/statistiques/5017208?sommaire=5017385 (accessed on 2 April 2022).
- INSEE. Economic Report (Bilan Économique) 2019—Guadeloupe. Available online: https://archive.ph/juKhS (accessed on 6 March 2022).
- INSEE. Tourist Attendance 2015—Réunion (Fréquentation Touristique 2015—La Réunion). Available online: https://archive.ph/aNe9W (accessed on 2 April 2022).
- INSEE. Population Estimate as of 1st January 2022 (Estimation de la Population au 1er Janvier 2022). Available online: https://archive.ph/UH39o (accessed on 9 March 2022).
- Presidency of the French Republic Coronavirus COVID-19. Available online: https://archive.ph/rnZOl (accessed on 9 April 2022).
- Prefecture of Guadeloupe COVID-19: Prefectural Decrees (COVID-19: Les Arrêtés Préfectoraux). Available online: https://archive.ph/y194d (accessed on 9 April 2022).
- Prefecture of Martinique Prefectural Decrees Relating to the Management of COVID-19 (Arrêtés Préfectoraux Relatifs à la Gestion du COVID-19). Available online: https://archive.ph/TAFdJ (accessed on 9 April 2022).
- Prefecture of Réunion Logbook of Administrative Acts (Recueil des Actes Administratifs). Available online: https://archive.ph/dNDce (accessed on 9 April 2022).
- Mintz, J.; Huntley, K.; Wahood, W.; Raine, S.; Hardigan, P.; Haffizulla, F. Early Government Interventions are Correlated to Lower Peak COVID-19 Outcomes. Ann. Epidemiol. 2020, 52, 107. [Google Scholar] [CrossRef]
- Arumugam, M.; Haja Najimudeen, R.B.; Vijayan, A.; Sathyamoorthy, B.; Patole, P.S. A cross-sectional study of COVID-19 outbreak in Indian population. Ann. Med. Surg. 2022, 76, 103554. [Google Scholar] [CrossRef]
- Whittemore, P.B. COVID-19 fatalities, latitude, sunlight, and vitamin D. Am. J. Infect. Control 2020, 48, 1042–1044. [Google Scholar] [CrossRef]
- Pearson, E.S.; Adyanthāya, N.K. The Distribution of Frequency Constants in Small Samples from Non-Normal Symmetrical and Skew Populations. Biometrika 1929, 21, 259–286. [Google Scholar] [CrossRef]
- Havlicek, L.L.; Peterson, N.L. Robustness of the Pearson Correlation against Violations of Assumptions. Percept. Mot. Ski. 1976, 43, 1319–1334. [Google Scholar] [CrossRef]
- Badr, H.S.; Du, H.; Marshall, M.; Dong, E.; Squire, M.M.; Gardner, L.M. Association between mobility patterns and COVID-19 transmission in the USA: A mathematical modelling study. Lancet Infect. Dis. 2020, 20, 1247–1254. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- Kucharski, A.J.; Jit, M.; Logan, J.G.; Cotten, M.; Clifford, S.; Quilty, B.J.; Russell, T.W.; Peeling, R.W.; Antonio, M.; Heymann, D.L. Travel measures in the SARS-CoV-2 variant era need clear objectives. Lancet 2022, 399, 1367–1369. [Google Scholar] [CrossRef]
- PAHO. An increase in COVID-19 Cases and Hospitalization in the Eastern Caribbean Countries and Circulation of Variant of Concern (VOC) Delta. Available online: https://archive.ph/kbcgb (accessed on 7 March 2022).
- WHO. WHO Advice for International Traffic in Relation to the SARS-CoV-2 Omicron Variant (B.1.1.529). Available online: https://archive.ph/1cWkm (accessed on 25 February 2022).
- Mendelson, M.; Venter, F.; Moshabela, M.; Gray, G.; Blumberg, L.; de Oliveira, T.; Madhi, S.A. The political theatre of the UK’s travel ban on South Africa. Lancet 2021, 398, 2211–2213. [Google Scholar] [CrossRef]
- Atout France. Tourist Attendance and Attractiveness of Réunion, Martinique, Guadeloupe (La Fréquentation et Attractivité Touristique de la Réunion, la Martinique, la Guadeloupe); Atout France: Paris, France, 2021.
- WHO. New Caledonia: WHO Coronavirus Disease (COVID-19) Dashboard with Vaccination Data. Available online: https://archive.ph/bv83V (accessed on 10 April 2022).
- WHO. Barbados: WHO Coronavirus Disease (COVID-19) Dashboard with Vaccination Data. Available online: https://archive.ph/4BbUR (accessed on 10 April 2022).
- WHO. Seychelles: WHO Coronavirus Disease (COVID-19) Dashboard with Vaccination Data. Available online: https://archive.ph/wK3dA (accessed on 10 April 2022).
- Devonish, D.; Dulal-Arthur, T. Perceived COVID-19 Vaccine Pressure in the Caribbean: Exploring a New Stressor–Strain Phenomenon in the Pandemic. Vaccines 2022, 10, 238. [Google Scholar] [CrossRef] [PubMed]
- The Lancet COVID-19: The next phase and beyond. Lancet 2022, 399, 1753. [CrossRef]
- Weiss, C.H. The Many Meanings of Research Utilization. Public Adm. Rev. 1979, 39, 426. [Google Scholar] [CrossRef]
- Bertrand, C.; Lecarpentier, E. COVID-19: A disaster. Méd. Catastr. Urgences Collect. 2022, 6, 45–48. [Google Scholar] [CrossRef]
- Portecop, P.; Chavet, F.; Haegaert, V.; Pujo, J.-M.; Gueye, P.; Kallel, H. Naval aviation contribution to COVID 19 evacuation in French overseas territories (Contribution aéronavale à l’évacuation COVID-19 en outre-mer). Méd. Catastr. Urgences Collect. 2022, 6, 7–11. [Google Scholar] [CrossRef]
- French Health Ministry. End of the Mediation Mission at the Martinique University Hospital (Fin de la Mission de Médiation au CHU de Martinique). Available online: https://archive.ph/XMMFo (accessed on 10 April 2022).
- Boutonnet, M.; Turc, J.; Dupre, H.-L.; Paris, R.; Muller, V. “MoRPHEE” fighting COVID-19. Anaesth. Crit. Care Pain Med. 2020, 39, 363–364. [Google Scholar] [CrossRef]
- Bast, E.; Tang, F.; Dahn, J.; Palacio, A. Increased risk of hospitalisation and death with the delta variant in the USA. Lancet Infect. Dis. 2021, 21, 1629–1630. [Google Scholar] [CrossRef]
- Alizon, S.; Haim-Boukobza, S.; Foulongne, V.; Verdurme, L.; Trombert-Paolantoni, S.; Lecorche, E.; Roquebert, B.; Sofonea, M.T. Rapid spread of the SARS-CoV-2 Delta variant in some French regions, June 2021. Eurosurveillance 2021, 26, 2100573. [Google Scholar] [CrossRef] [PubMed]
- Filipovic-Pierucci, A.; Rigault, A.; Fagot-Campagna, A.; Tuppin, P. Health status of populations living in French overseas territories in 2012, compared with metropolitan France: An analysis of the national health insurance database. Rev. Epidemiol. Sante Publique 2016, 64, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Cour des Comptes. Health in the Overseas Territories, a Responsibility of the Republic (La Santé dans les Outre-Mer, une Responsabilité de la République); Cour des Comptes: Paris, France, 2014.
- Sorci, G.; Faivre, B.; Morand, S. Explaining among-country variation in COVID-19 case fatality rate. Sci. Rep. 2020, 10, 18909. [Google Scholar] [CrossRef] [PubMed]
- Prefecture of Guadeloupe. Prefectural Decree n°2021-380 CAB/BSI of 27th November 2021 Prescribing the Conditions of Entry into Guadeloupe by air (Arrêté Préfectoral n°2021-380 CAB/BSI du 27 Novembre 2021 Prescrivant les Conditions d’Entrée en Guadeloupe par voie Aérienne); Prefecture of Guadeloupe: Guadeloupe, France, 2021.
- Prefecture of Guadeloupe. Prefectural Decree of 27th December 2021 Amending Decree No. 2021-409 CAB/BSI of 23th December 23 2021 Prescribing the Conditions for Entering Guadeloupe by Air (Arrêté Préfectoral du 27 Décembre 2021 Portant Modification de l’arrêté n° 2021-409 CAB/BSI du 23 Décembre 2021 Prescrivant les Conditions d’entrée en Guadeloupe par Voie Aérienne); Prefecture of Guadeloupe: Guadeloupe, France, 2021.
- Foo, C.D.; Grépin, K.A.; Cook, A.R.; Hsu, L.Y.; Bartos, M.; Singh, S.; Asgari, N.; Teo, Y.Y.; Heymann, D.L.; Legido-Quigley, H. Navigating from SARS-CoV-2 elimination to endemicity in Australia, Hong Kong, New Zealand, and Singapore. Lancet 2021, 398, 1547–1551. [Google Scholar] [CrossRef]
- New Zealand Government about Exemptions Managed Isolation and Quarantine. Available online: https://archive.ph/fyqWl (accessed on 9 April 2022).
- Patel, J.; Fernandes, G.; Sridhar, D. How can we improve self-isolation and quarantine for COVID-19? BMJ 2021, 372, n625. [Google Scholar] [CrossRef]
- CépiDc Query Mortality Data (Interroger les Données de Mortalité). Available online: https://archive.ph/x2tvo (accessed on 9 March 2022).
- UNWTO. Tourism Statistics—Country Fact Sheets. Available online: https://www.unwto.org/statistics/country-fact-sheets (accessed on 6 March 2022).
- IMF. Tourism in the Post-Pandemic World: Economic Challenges and Opportunities for Asia-Pacific and the Western Hemisphere; IMF: Washington, DC, USA, 2021. [Google Scholar]
- Watts, N.; Amann, M.; Arnell, N.; Ayeb-Karlsson, S.; Beagley, J.; Belesova, K.; Boykoff, M.; Byass, P.; Cai, W.; Campbell-Lendrum, D.; et al. The 2020 report of The Lancet Countdown on health and climate change: Responding to converging crises. Lancet 2021, 397, 129–170. [Google Scholar] [CrossRef]
- Burki, T.K. COVID-19 in the Caribbean. Lancet Respir. Med. 2021, 9, e46. [Google Scholar] [CrossRef]
- Dominica Government Safe in Nature Accommodation for Travellers from High Risk Countries. Available online: https://archive.ph/EdAM1 (accessed on 18 April 2022).
- Dominica Hotel & Tourism Association Dominica’s Safe in Nature Certification Program Pays Off. Available online: https://archive.ph/iTod4 (accessed on 18 April 2022).
- WHO. The WHO Council on the Economics of Health for All—Manifesto; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
d’Almeida, S. Impact of Vaccine and Immunity Passports in the Context of COVID-19: A Time Series Analysis in Overseas France. Vaccines 2022, 10, 852. https://doi.org/10.3390/vaccines10060852
d’Almeida S. Impact of Vaccine and Immunity Passports in the Context of COVID-19: A Time Series Analysis in Overseas France. Vaccines. 2022; 10(6):852. https://doi.org/10.3390/vaccines10060852
Chicago/Turabian Styled’Almeida, Samuel. 2022. "Impact of Vaccine and Immunity Passports in the Context of COVID-19: A Time Series Analysis in Overseas France" Vaccines 10, no. 6: 852. https://doi.org/10.3390/vaccines10060852