
Cellular Immune Response after Vaccination with an Adjuvanted, Recombinant Zoster Vaccine in Allogeneic Hematopoietic Stem Cell Transplant Recipients


Abstract
:1. Introduction
2. Materials and Methods
2.1. Volunteers
2.2. Vaccine and Vaccination
2.3. ELISpot Assay
2.4. Statistical Analysis
3. Results
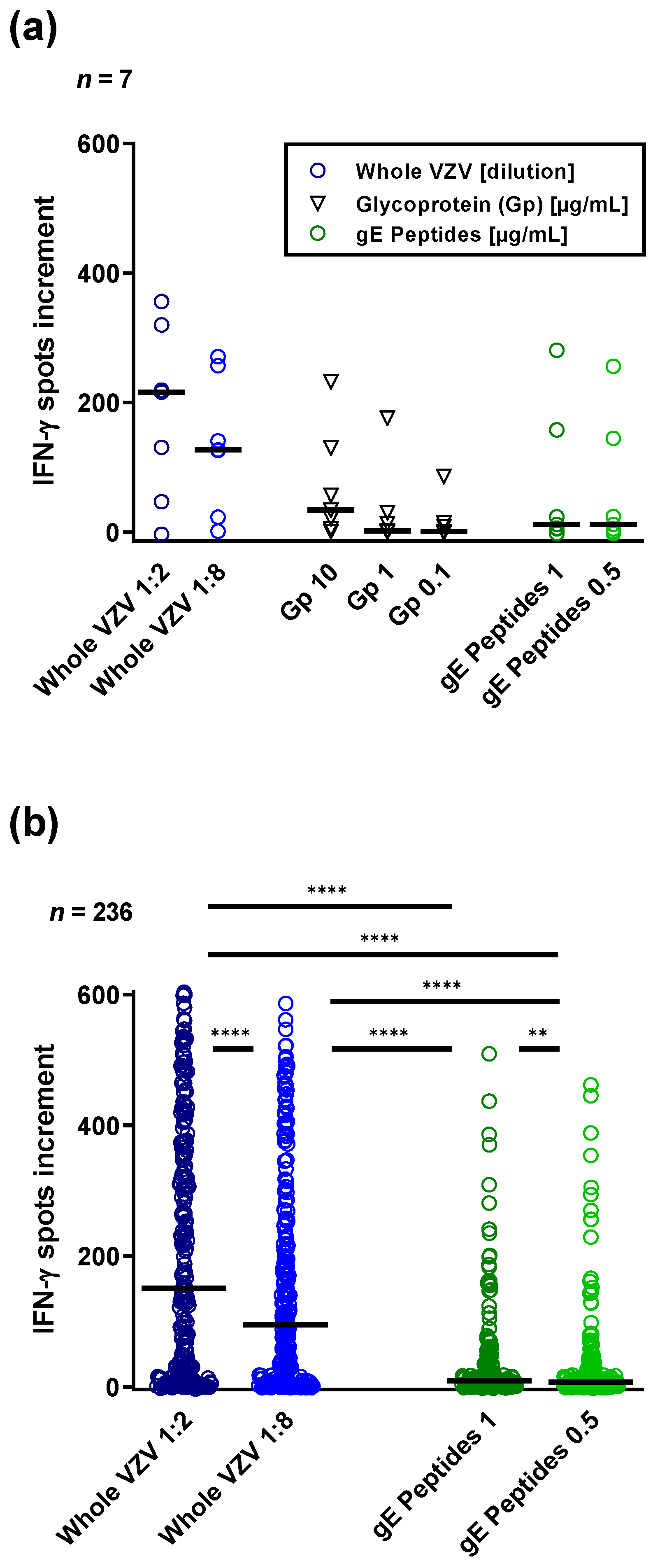
3.1. ELISpot Responses to Three Different VZV Antigens
3.2. Comparison of VZV-Specific Immunity in Stem Cell Transplant Recipients Prior to and Post Vaccination
3.3. Correlation of VZV-Specific Immunity Measured with Various VZV Antigens and at Various Time Points
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sauerbrei, A. Diagnosis, antiviral therapy, and prophylaxis of varicella-zoster virus infections. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 723–734. [Google Scholar] [CrossRef]
- Hillebrand, K.; Bricout, H.; Schulze-Rath, R.; Schink, T.; Garbe, E. Incidence of herpes zoster and its complications in Germany, 2005-2009. J. Infect. 2015, 70, 178–186. [Google Scholar] [CrossRef]
- Gershon, A.A.; Mervish, N.; LaRussa, P.; Steinberg, S.; Lo, S.H.; Hodes, D.; Fikrig, S.; Bonagura, V.; Bakshi, S. Varicella-zoster virus infection in children with underlying human immunodeficiency virus infection. J. Infect. Dis. 1997, 176, 1496–1500. [Google Scholar] [CrossRef]
- Arvin, A. Aging, immunity, and the varicella-zoster virus. N. Engl. J. Med. 2005, 352, 2266–2267. [Google Scholar] [CrossRef]
- Whitley, R.J.; Siebenhaar, F.; Sterry, W. Varicella-Zoster-Virus Infections. In Harrison’s Principles of Internal Medicine (Deutsche Ausgabe), 16th ed.; Dietel, M., Suttrop, N., Zeitz, M., Eds.; Union Druckerei: Weimar, Germany, 2005; Volume 1, pp. 1121–1124. [Google Scholar]
- Lindemann, M.; Schuett, P.; Moritz, T.; Ottinger, H.D.; Opalka, B.; Seeber, S.; Nowrousian, M.R.; Grosse-Wilde, H. Cellular in vitro immune function in multiple myeloma patients after high-dose chemotherapy and autologous peripheral stem cell transplantation. Leukemia 2005, 19, 490–492. [Google Scholar] [CrossRef]
- Gross, G. Zoster-Manifestationsformen an der Haut, Komplikationen und Therapie. Dtsch. Med. Wochenschr. 1997, 122, 132–139. [Google Scholar] [CrossRef]
- Koc, Y.; Miller, K.B.; Schenkein, D.P.; Griffith, J.; Akhtar, M.; DesJardin, J.; Snydman, D.R. Varicella zoster virus infections following allogeneic bone marrow transplantation: Frequency, risk factors, and clinical outcome. Biol. Blood Marrow Transplant. 2000, 6, 44–49. [Google Scholar] [CrossRef] [Green Version]
- Ullmann, A.J.; Schmidt-Hieber, M.; Bertz, H.; Heinz, W.J.; Kiehl, M.; Kruger, W.; Mousset, S.; Neuburger, S.; Neumann, S.; Penack, O.; et al. Infectious diseases in allogeneic haematopoietic stem cell transplantation: Prevention and prophylaxis strategy guidelines 2016. Ann. Hematol. 2016, 95, 1435–1455. [Google Scholar] [CrossRef] [Green Version]
- Jamani, K.; MacDonald, J.; Lavoie, M.; Williamson, T.S.; Brown, C.B.; Chaudhry, A.; Jimenez-Zepeda, V.H.; Duggan, P.; Tay, J.; Stewart, D.; et al. Zoster prophylaxis after allogeneic hematopoietic cell transplantation using acyclovir/valacyclovir followed by vaccination. Blood Adv. 2016, 1, 152–159. [Google Scholar] [CrossRef]
- Robert-Koch-Institute. Empfehlungen der Ständigen Impfkommission beim Robert Koch-Institut 2021. Epid. Bull. 2021, 34, 4–38. [Google Scholar]
- U.S. Department of Health & Human Services. HHS.gov Immunization. Available online: https://www.hhs.gov/immunization/diseases/chickenpox/index.html (accessed on 24 March 2022).
- Robert-Koch-Institute. Schutzimpfung Gegen Herpes Zoster (Gürtelrose). Available online: https://www.rki.de/DE/Content/Infekt/Impfen/Materialien/Faktenblaetter/Zoster.html;jsessionid=80F817FC1C302CB2CD1F2D9F5F5641D5.internet071?nn=2375548 (accessed on 24 March 2022).
- Vink, P.; Ramon Torrell, J.M.; Sanchez Fructuoso, A.; Kim, S.J.; Kim, S.I.; Zaltzman, J.; Ortiz, F.; Campistol Plana, J.M.; Fernandez Rodriguez, A.M.; Rebollo Rodrigo, H.; et al. Immunogenicity and Safety of the Adjuvanted Recombinant Zoster Vaccine in Chronically Immunosuppressed Adults Following Renal Transplant: A Phase 3, Randomized Clinical Trial. Clin. Infect. Dis. 2020, 70, 181–190. [Google Scholar] [CrossRef]
- Cohen, J.I.; Straus, S.E.; Arvin, A.M. Varicella-zoster virus replication, pathogenesis, and management. In Fields Virology, 5th ed.; Knipe, D.M., Howley, P.M., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2007; Volume 2, pp. 2773–2818. [Google Scholar]
- Czerkinsky, C.; Andersson, G.; Ekre, H.P.; Nilsson, L.A.; Klareskog, L.; Ouchterlony, O. Reverse ELISPOT assay for clonal analysis of cytokine production. I. Enumeration of gamma-interferon-secreting cells. J. Immunol. Methods 1988, 110, 29–36. [Google Scholar] [CrossRef]
- European Medicines Agency. Shingrix- EPAR -Product Information. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/shingrix (accessed on 24 March 2022).
- Arvin, A.M. Humoral and cellular immunity to varicella-zoster virus: An overview. J. Infect. Dis. 2008, 197 (Suppl. S2), S58–S60. [Google Scholar] [CrossRef] [Green Version]
- White, C.J.; Kuter, B.J.; Ngai, A.; Hildebrand, C.S.; Isganitis, K.L.; Patterson, C.M.; Capra, A.; Miller, W.J.; Krah, D.L.; Provost, P.J.; et al. Modified cases of chickenpox after varicella vaccination: Correlation of protection with antibody response. Pediatr. Infect. Dis. J. 1992, 11, 19–23. [Google Scholar] [CrossRef]
- Feyssaguet, M.; Berthold, V.; Helle, L.; Povey, M.; Ravault, S.; Carryn, S.; Gillard, P.; Di Paolo, E. Comparison of a glycoprotein E-based ELISA with a varicella-zoster whole-virus ELISA for the quantification of varicella vaccine immune responses in young children. Vaccine 2020, 38, 3300–3304. [Google Scholar] [CrossRef]
- Sauerbrei, A.; Schafler, A.; Hofmann, J.; Schacke, M.; Gruhn, B.; Wutzler, P. Evaluation of three commercial varicella-zoster virus IgG enzyme-linked immunosorbent assays in comparison to the fluorescent-antibody-to-membrane-antigen test. Clin. Vaccine Immunol. 2012, 19, 1261–1268. [Google Scholar] [CrossRef] [Green Version]
- Cassaniti, I.; Ferrari, A.; Comolli, G.; Sarasini, A.; Gregorini, M.; Rampino, T.; Lilleri, D.; Baldanti, F. Characterization of Varicella-Zoster (VZV) Specific T Cell Response in Healthy Subjects and Transplanted Patients by Using Enzyme Linked Immunospot (ELISpot) Assays. Vaccines 2021, 9, 875. [Google Scholar] [CrossRef]
- Camargo, J.F.; Lin, R.Y.; Natori, Y.; Anderson, A.D.; Alencar, M.C.; Wang, T.P.; Morris, M.I.; Komanduri, K.V. Reduced immunogenicity of the adjuvanted recombinant zoster vaccine after hematopoietic cell transplant: A pilot study. Blood Adv. 2020, 4, 4618–4622. [Google Scholar] [CrossRef]
- Lindemann, M.; Barsegian, V.; Runde, V.; Fiedler, M.; Heermann, K.H.; Schaefer, U.W.; Roggendorf, M.; Grosse-Wilde, H. Transfer of humoral and cellular hepatitis B immunity by allogeneic hematopoietic cell transplantation. Transplantation 2003, 75, 833–838. [Google Scholar] [CrossRef]
- Aoki, T.; Koh, K.; Kawano, Y.; Mori, M.; Arakawa, Y.; Kato, M.; Hanada, R. Safety of Live Attenuated High-Titer Varicella-Zoster Virus Vaccine in Pediatric Allogeneic Hematopoietic Stem Cell Transplantation Recipients. Biol. Blood Marrow Transplant. 2016, 22, 771–775. [Google Scholar] [CrossRef] [Green Version]
- Chun, J.Y.; Kim, K.; Lee, M.K.; Kang, C.K.; Koh, Y.; Shin, D.Y.; Hong, J.; Choe, P.G.; Kim, N.J.; Yoon, S.S.; et al. Immunogenicity and safety of a live herpes zoster vaccine in hematopoietic stem cell transplant recipients. BMC Infect. Dis. 2021, 21, 117. [Google Scholar] [CrossRef]
- Smith, J.G.; Liu, X.; Kaufhold, R.M.; Clair, J.; Caulfield, M.J. Development and validation of a gamma interferon ELISPOT assay for quantitation of cellular immune responses to varicella-zoster virus. Clin. Diagn. Lab. Immunol. 2001, 8, 871–879. [Google Scholar] [CrossRef] [Green Version]
- Baumrin, E.; Izaguirre, N.E.; Bausk, B.; Feeley, M.M.; Bay, C.P.; Yang, Q.; Ho, V.T.; Baden, L.R.; Issa, N.C. Safety and reactogenicity of the recombinant zoster vaccine after allogeneic hematopoietic cell transplantation. Blood Adv. 2021, 5, 1585–1593. [Google Scholar] [CrossRef]
- Klein, S.L. Sex influences immune responses to viruses, and efficacy of prophylaxis and treatments for viral diseases. BioEssays 2012, 34, 1050–1059. [Google Scholar] [CrossRef] [Green Version]
- Bernin, H.; Fehling, H.; Marggraff, C.; Tannich, E.; Lotter, H. The cytokine profile of human NKT cells and PBMCs is dependent on donor sex and stimulus. Med. Microbiol. Immunol. 2016, 205, 321–332. [Google Scholar] [CrossRef] [Green Version]
- Di Benedetto, S.; Derhovanessian, E.; Steinhagen-Thiessen, E.; Goldeck, D.; Muller, L.; Pawelec, G. Impact of age, sex and CMV-infection on peripheral T cell phenotypes: Results from the Berlin BASE-II Study. Biogerontology 2015, 16, 631–643. [Google Scholar] [CrossRef]
- Villacres, M.C.; Longmate, J.; Auge, C.; Diamond, D.J. Predominant type 1 CMV-specific memory T-helper response in humans: Evidence for gender differences in cytokine secretion. Hum. Immunol. 2004, 65, 476–485. [Google Scholar] [CrossRef]
- Lindemann, M.; Korth, J.; Sun, M.; Xu, S.; Struve, C.; Werner, K.; Dornieden, T.; Horn, P.A.; Witzke, O.; Wilde, B. The Cytomegalovirus-Specific IL-21 ELISpot Correlates with Allograft Function of Kidney Transplant Recipients. Int. J. Mol. Sci. 2018, 19, 3945. [Google Scholar] [CrossRef] [Green Version]
- Klein, S.L.; Flanagan, K.L. Sex differences in immune responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef]
- Boef, A.G.C.; van der Klis, F.R.M.; Berbers, G.A.M.; Buisman, A.M.; Sanders, E.A.M.; Kemmeren, J.M.; van der Ende, A.; de Melker, H.E.; Rots, N.Y.; Knol, M.J. Differences by sex in IgG levels following infant and childhood vaccinations: An individual participant data meta-analysis of vaccination studies. Vaccine 2018, 36, 400–407. [Google Scholar] [CrossRef]
- Giefing-Kroll, C.; Berger, P.; Lepperdinger, G.; Grubeck-Loebenstein, B. How sex and age affect immune responses, susceptibility to infections, and response to vaccination. Aging Cell 2015, 14, 309–321. [Google Scholar] [CrossRef]
- Lindemann, M.; Klisanin, V.; Thummler, L.; Fisenkci, N.; Tsachakis-Muck, N.; Ditschkowski, M.; Schwarzkopf, S.; Klump, H.; Reinhardt, H.C.; Horn, P.A.; et al. Humoral and Cellular Vaccination Responses against SARS-CoV-2 in Hematopoietic Stem Cell Transplant Recipients. Vaccines 2021, 9, 1075. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Group | Absolute Number or Median (Range) |
|---|---|---|
| Sex | Female | 34 |
| Male | 45 | |
| Age (years) | 60 (28–76) | |
| Underlying disease | Acute leukemia | 33 |
| Myelodysplastic syndrome | 14 | |
| Myeloproliferative neoplasia | 18 | |
| Lymphoma | 11 | |
| Other/not specified | 2 | |
| Acute GvHD | 0 | 4 |
| I | 27 | |
| II | 46 | |
| III | 1 | |
| IV | 1 | |
| Chronic GvHD | None | 4 |
| Limited | 56 | |
| Extensive | 19 | |
| Interval transplantation– 1st vaccination | 37 months (8–402) | |
| Interval 1st vaccination– 2nd vaccination | 3.5 months (1–16) | |
| Interval vaccination– (first) blood sampling | 1st | 2.3 months (0.3–23) |
| 2nd | 2.6 months (0.2–13) |
| Time Points | Antigen for ELISpot | n | p (Shingles) | p (Sex) |
|---|---|---|---|---|
| Pre vacc. | VZV 1:2 | 64 | 0.01 | 0.07 |
| VZV 1:8 | 61 | 0.006 | 0.11 | |
| gE 1 | 32 | 0.30 | 0.69 | |
| gE 0.5 | 32 | 0.11 | 0.09 | |
| Post 1st vacc. | VZV 1:2 | 38 | 0.04 | 0.04 |
| VZV 1:8 | 38 | 0.06 | 0.04 | |
| gE 1 | 24 | 0.03 | 0.04 | |
| gE 0.5 | 24 | 0.26 | 0.09 | |
| Post 2nd vacc. | VZV 1:2 | 43 | 0.02 | 0.02 |
| VZV 1:8 | 43 | 0.03 | 0.04 | |
| gE 1 | 37 | 0.06 | 0.03 | |
| gE 0.5 | 37 | 0.07 | 0.02 |
| Antigen for ELISpot | Dilution or Concentration | r | p |
|---|---|---|---|
| Whole VZV Behring | 1:2 | 0.54 | 0.24 |
| 1:8 | 0.36 | 0.44 | |
| Glycoprotein SERION | 10 µg/mL | −0.07 | 0.91 |
| 1 µg/mL | 0.72 | 0.08 | |
| 0.1 µg/mL | 0.67 | 0.12 | |
| Glycoprotein E Peptides JPT | gE peptides 0.5 µg/mL | 1.00 | 0.0004 |
| All Samples (n = 172–236) | Variable 2 | |||||||
|---|---|---|---|---|---|---|---|---|
| Variable 1 | VZV 1:2 | VZV 1:8 | gE 1 | gE 0.5 | ||||
| r | p **** | r | p **** | r | p **** | r | p **** | |
| VZV 1:2 | 1 | 0.96 | 0.44 | 0.46 | ||||
| VZV 1:8 | 0.96 | 1 | 0.44 | 0.46 | ||||
| gE 1 | 0.44 | 0.44 | 1 | 0.89 | ||||
| gE 0.5 | 0.46 | 0.46 | 0.89 | 1 | ||||
| Pre vacc. (n = 32–64) | Variable 2 | |||||||
| Variable 1 | VZV 1:2 | VZV 1:8 | gE 1 | gE 0.5 | ||||
| r | p | r | p | r | p | r | p | |
| VZV 1:2 | 1 | 0.97 | <0.0001 | 0.27 | 0.13 | 0.39 | 0.003 | |
| VZV 1:8 | 0.96 | <0.0001 | 1 | 0.34 | 0.06 | 0.48 | 0.006 | |
| gE 1 | 0.27 | 0.13 | 0.34 | 0.06 | 1 | 0.77 | <0.0001 | |
| gE 0.5 | 0.39 | 0.003 | 0.48 | 0.006 | 0.77 | <0.0001 | 1 | |
| Post 1st vacc. (n = 24–38) | Variable 2 | |||||||
| Variable 1 | VZV 1:2 | VZV 1:8 | gE 1 | gE 0.5 | ||||
| r | p | r | p | r | p | r | p | |
| VZV 1:2 | 1 | 0.97 | <0.0001 | 0.81 | <0.0001 | 0.59 | 0.002 | |
| VZV 1:8 | 0.97 | <0.0001 | 1 | 0.79 | <0.0001 | 0.56 | 0.005 | |
| gE 1 | 0.81 | <0.0001 | 0.79 | <0.0001 | 1 | 0.78 | <0.0001 | |
| gE 0.5 | 0.59 | 0.002 | 0.56 | 0.005 | 0.78 | <0.0001 | 1 | |
| Post 2nd vacc. (n = 37–42) | Variable 2 | |||||||
| Variable 1 | VZV 1:2 | VZV 1:8 | gE 1 | gE 0.5 | ||||
| r | p | r | p | r | p | r | p | |
| VZV 1:2 | 1 | 0.93 | <0.0001 | 0.45 | 0.005 | 0.53 | 0.001 | |
| VZV 1:8 | 0.93 | <0.0001 | 1 | 0.55 | <0.0001 | 0.61 | <0.0001 | |
| gE 1 | 0.45 | 0.005 | 0.55 | <0.0001 | 1 | 0.95 | <0.0001 | |
| gE 0.5 | 0.53 | 0.001 | 0.61 | <0.0001 | 0.95 | <0.0001 | 1 | |
| Time Points | Antigen for ELISpot | n | r | p |
|---|---|---|---|---|
| Pre–post 1st vacc. | VZV 1:2 | 30 | 0.91 | <0.0001 |
| VZV 1:8 | 27 | 0.89 | <0.0001 | |
| gE 1 | 7 | 0.85 | 0.02 | |
| gE 0.5 | 7 | 0.90 | 0.006 | |
| Pre–post 2nd vacc. | VZV 1:2 | 31 | 0.81 | <0.0001 |
| VZV 1:8 | 28 | 0.71 | <0.0001 | |
| gE 1 | 10 | 0.68 | 0.03 | |
| gE 0.5 | 10 | 0.76 | 0.01 | |
| Post 1st vacc.–post 2nd vacc. | VZV 1:2 | 26 | 0.87 | <0.0001 |
| VZV 1:8 | 26 | 0.83 | <0.0001 | |
| gE 1 | 14 | 0.73 | 0.003 | |
| gE 0.5 | 14 | 0.76 | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koldehoff, M.; Horn, P.A.; Lindemann, M. Cellular Immune Response after Vaccination with an Adjuvanted, Recombinant Zoster Vaccine in Allogeneic Hematopoietic Stem Cell Transplant Recipients. Vaccines 2022, 10, 809. https://doi.org/10.3390/vaccines10050809
Koldehoff M, Horn PA, Lindemann M. Cellular Immune Response after Vaccination with an Adjuvanted, Recombinant Zoster Vaccine in Allogeneic Hematopoietic Stem Cell Transplant Recipients. Vaccines. 2022; 10(5):809. https://doi.org/10.3390/vaccines10050809
Chicago/Turabian StyleKoldehoff, Michael, Peter A. Horn, and Monika Lindemann. 2022. "Cellular Immune Response after Vaccination with an Adjuvanted, Recombinant Zoster Vaccine in Allogeneic Hematopoietic Stem Cell Transplant Recipients" Vaccines 10, no. 5: 809. https://doi.org/10.3390/vaccines10050809