
High Prevalence of Non-Vaccinated Oncogenic Human Papillomavirus Genotypes in High-Grade Squamous Intraepithelial Lesions of the Cervix: Thought-Provoking Results of a Detailed HPV Genotype Analysis

Abstract
:1. Background
2. Materials and Methods
2.1. Sampling, Cytological and Histological Diagnoses
2.2. Sample Preparation, HPV Detection, and Genotyping by HPV Direct Flow CHIP
2.3. Statistics
3. Results
3.1. Patients Characteristics
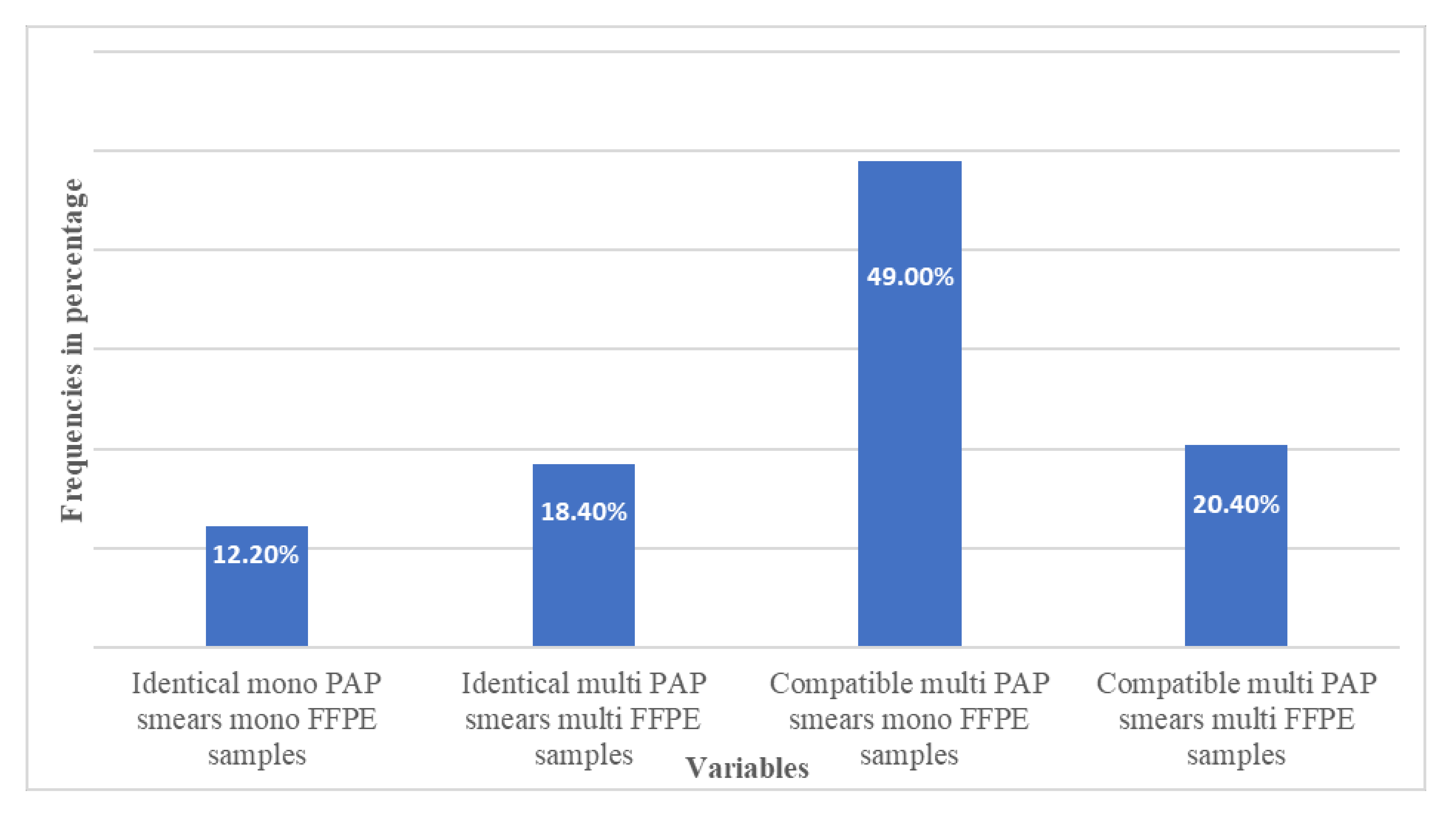
3.2. HPV Prevalence and Agreement between the Relating Sample Types
3.3. Occurrence of the Specific Genotypes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CI | confidence interval |
| FFPE | formalin-fixed paraffin-embedded |
| GYN | gynecological |
| HPV | human papillomavirus |
| HSIL | high-grade squamous intraepithelial lesions |
| HR | high-risk |
| LR | low-risk |
| LSIL | low-grade squamous intraepithelial lesions |
| PAP | Papanicolaou |
| SIL | squamous intraepithelial lesions |
| VT | vaccinated type |
References
- Graham, S.V. The human papillomavirus replication cycle, and its links to cancer progression: A comprehensive review. Clin. Sci. 2017, 131, 2201–2221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papillomavirus Episteme: A Comprehensive Papillomaviridae Database and Analysis Resource. 2012. Available online: https://pave.niaid.nih.gov/#home (accessed on 24 February 2022).
- Van Doorslaer, K.; Li, Z.; Xirasagar, S.; Maes, P.; Kaminsky, D.; Liou, D.; Sun, Q.; Kaur, R.; Huyen, Y.; McBride, A.A. The Papillomavirus Episteme: A major update to the papillomavirus sequence database. Nucleic Acids Res. 2017, 45, D499–D506. [Google Scholar] [CrossRef] [PubMed]
- WHO; International Agency for Research on Cancer. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans; Human Papillomaviruses; IARC: Lyon, France, 2011; Volume 90. [Google Scholar]
- Smith, J.S.; Lindsay, L.; Hoots, B.; Keys, J.; Franceschi, S.; Winer, R.; Clifford, G.M. Human papillomavirus type distribution in invasive cervical cancer and high-grade cervical lesions: A meta-analysis update. Int. J. Cancer 2007, 121, 621–632. [Google Scholar] [CrossRef] [PubMed]
- Clifford, G.M.; Smith, J.S.; Aguado, T.; Franceschi, S. Comparison of HPV type distribution in high-grade cervical lesions and cervical cancer: A meta-analysis. Br. J. Cancer 2003, 89, 101–105. [Google Scholar] [CrossRef] [Green Version]
- Clifford, G.M.; Smith, J.S.; Plummer, M.; Muñoz, N.; Franceschi, S. Human papillomavirus types in invasive cervical cancer worldwide: A meta-analysis. Br. J. Cancer 2003, 88, 63–73. [Google Scholar] [CrossRef]
- Tachez, R.; Smahelova, J.; Saláková, M.; Arbyn, M.; Rob, L.; Skapa, P.; Jirásek, T.; Hamsikova, E. Human Papillomavirus Genotype Distribution in Czech Woman an Men with Diseases Etiologycally Linked to HPV. PLoS ONE 2011, 6, e21913. [Google Scholar] [CrossRef]
- Man, I.; Vänskä, S.; Lehtinen, M.; Bogaards, J. Human Papillomavirus Genotype Replacement: Still Too Early to Tell? J. Infect. Dis. 2021, 224, 481–491. [Google Scholar] [CrossRef] [Green Version]
- Sousa, H.; Tavares, A.; Campos, C.; Marinho-Dias, J.; Brito, M.; Medeiros, R.; Baldaque, I.; Lobo, C.; Leça, L.; Monteiro, P.; et al. High-Risk human papillomavirus genotype distribution in the Northern region of Portugal: Data from regional cervical cancer screening program. Papillomavirus Res. 2019, 8, 100179. [Google Scholar] [CrossRef]
- Stanley, M. Pathology and epidemiology of HPV infection in females. Gynecol. Oncol. 2010, 117, S5–S10. [Google Scholar] [CrossRef]
- De Brot, L.; Pellegrini, B.; Moretti, S.T.; Carraro, D.M.; Soares, F.A.; Rocha, R.M.; Baiocchi, G.; Werneck da Cunha, I.; Piana de Andrade, V. Infections with Multiple High-Risk HPV Types Are Associated With High-Grade and Persistent Low-Grade Intraepithelial Lesions of the Cervix. Cancer Cytopathol. 2017, 125, 138–143. [Google Scholar] [CrossRef]
- Gheit, T. Mucosal and Cutaneous Human Papillomavirus Infections and Cancer Biology. Front. Oncol. 2019, 9, 355. [Google Scholar] [CrossRef] [Green Version]
- Schiffman, M.; Castel, P.E.; Jeronimo, J.; Rodriguez, A.C.; Wacholder, S. Human papillomavirus and cervical cancer. Lancet 2007, 370, 890–907. [Google Scholar] [CrossRef]
- Maucort-Boulch, D.; Plummer, M.; Castle, P.E.; Demuth, F.; Safaeian, M.; Wheeler, C.M.; Schiffman, M. Predictors of human papillomavirus persistence among women with equivocal or mildly abnormal cytology. Int. J. Cancer 2010, 126, 684–691. [Google Scholar] [CrossRef]
- Cubie, H.A. Diseases associated with human papillomavirus infection. Virology 2013, 445, 21–34. [Google Scholar] [CrossRef] [Green Version]
- Veldhuijzen, N.J.; Snijders, P.J.F.; Reiss, P.; Meijer, C.J.L.M.; van de Wijgert, J.H.H.M. Factors affecting transmission of mucosal human papillomavirus. Lancet Infect. Dis. 2010, 10, 862–874. [Google Scholar] [CrossRef]
- Zur Hausen, H. Papillomaviruses in the causation of human cancers—A brief historical account. Virology 2009, 384, 260–265. [Google Scholar] [CrossRef] [Green Version]
- Quint, W.; Jenkins, D.; Molijn, A.; Struijk, L.; van de Sandt, M.; Doorbar, J.; Mols, J.; Van Hoof, C.; Hardt, K.; Struyf, F.; et al. One virus, one lesion--individual components of CIN lesions contain a specific HPV type. J. Pathol. 2012, 227, 62–71. [Google Scholar] [CrossRef]
- Plummer, M.; Vaccarella, S.; Franceschi, S. Multiple Human Papillomavirus Infections: The Exception or the Rule? J. Infect. Dis. 2011, 203, 891–893. [Google Scholar] [CrossRef] [Green Version]
- Li, N.; Franceschi, S.; Howell-Jones, R.; Snijders, P.J.; Clifford, G.M. Human papillomavirus type distribution in 30,848 invasive cervical cancers worldwide: Variation by geographical region, histological type and year of publication. Int. J. Cancer 2010, 128, 327–335. [Google Scholar] [CrossRef]
- Torii, Y.; Fujii, T.; Kukimoto, I.; Saito, M.; Iwata, T.; Takahashi, H.; Ichikawa, R.; Kawai, S.; Otani, S.; Aoki, D. Comparison of methods using paraffin-embedded tissues and exfoliated cervical cells to evaluate human papillomavirus genotype attribution. Cancer Sci. 2016, 107, 1520–1526. [Google Scholar] [CrossRef] [Green Version]
- Serrano, B.; de Sanjosé, S.; Tous, S.; Quiros, B.; Muñoz, N.; Bosch, X.; Alemany, L. Human papillomavirus genotype attribution for HPVs 6, 11, 16, 18, 31, 33, 45, 52 and 58 in female anogenital lesions. Eur. J. Cancer 2015, 51, 1732–1741. [Google Scholar] [CrossRef]
- Insinga, R.P.; Liaw, K.L.; Johnson, L.G.; Madeleine, M.M. A systematic review of the prevalence and attribution of human papillomavirus types among cervical, vaginal, and vulvar precancers and cancers in the United States. Cancer Epidemiol. Biomarkers Prev. 2008, 17, 1611–1622. [Google Scholar] [CrossRef] [Green Version]
- Kim, G.; Cho, H.; Lee, D.; Park, S.; Lee, J.; Wang, H.Y.; Kim, S.; Park, K.H.; Lee, H. Comparison of FFPE histological versus LBP cytological samples for HPV detection and typing in cervical cancer. Exp. Mol. Pathol. 2017, 102, 321–326. [Google Scholar] [CrossRef]
- Bottari, F.; Passerini, R.; Renne, G.; Guerrier, M.E.; Sandri, M.T.; Li, A.; Orlandini, A.; Iacobone, A.D. Onclarity Performance in Human Papillomavirus DNA Detection in Formalin-Fixed Paraffin-Embedded Cervical Samples. J. Low. Genit. Tract Dis. 2021, 25, 216–220. [Google Scholar] [CrossRef]
- Bonde, J.; Bottari, F.; Iacobone, A.D.; Cocuzza, C.E.; Sandri, M.T.; Bogliatto, F.; Khan, K.S.; Ejegod, D.M.; Gary, D.S.; Andrews, J.C. Human Papillomavirus Same Genotype Persistence and Risk: A Systematic Review. J. Low. Genit. Tract Dis. 2021, 25, 27–37. [Google Scholar] [CrossRef]
- Huang, H.J.; Tung, H.J.; Yang, L.Y.; Chao, A.; Tang, Y.H.; Chou, H.H.; Chang, W.Y.; Wu, R.C.; Huang, C.C.; Lin, C.Y.; et al. Role of human papillomavirus status after conization for high-grade cervical intraepithelial neoplasia. Int. J. Cancer 2021, 148, 665–672. [Google Scholar] [CrossRef]
- Chao, A.; Lin, C.T.; Hsueh, S.; Chou, H.H.; Chang, T.C.; Chen, M.Y.; Lai, C.H. Usefulness of human papillomavirus testing in the follow-up of patients with high-grade cervical intraepithelial neoplasia after conization. Am. J. Obstet. Gynecol. 2004, 190, 1046–1051. [Google Scholar] [CrossRef]
- Kyrgiou, M.; Tsoumpou, I.; Vrekoussis, T.; Martin-Hirsch, P.; Arbyn, M.; Prendiville, W.; Mitrou, S.; Koliopoulos, G.; Dalkalitsis, N.; Stamatopoulos, P.; et al. The up-to-date evidence on colposcopy practice and treatment of cervical intraepithelial neoplasia: The Cochrane colposcopy & cervical cytopathology collaborative group (C5 group) approach. Cancer Treat Rev. 2006, 32, 516–523. [Google Scholar] [CrossRef] [PubMed]
- Kalliala, I.; Athanasiou, A.; Veroniki, A.A.; Salanti, G.; Efthimiou, O.; Raftis, N.; Bowden, S.; Paraskevaidi, M.; Aro, K.; Arbyn, M.; et al. Incidence and mortality from cervical cancer and other malignancies after treatment of cervical intraepithelial neoplasia: A systematic review and meta-analysis of the literature. Ann Oncol. 2020, 31, 213–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrarez-Hernandez, E.; Preda, O.; Alonso, S.; Pardo, R.S.; Olmo, A. Detection and Genotyping of Human Papillomavirus DNA in Formalin-Fixed Pareffin-Embadded Specimens with the HPV Direct Flow CHIP System. Open Virol. J. 2013, 7, 91–95. [Google Scholar] [CrossRef] [Green Version]
- Kocjan, B.J.; Hošnjak, L.; Poljak, M. Detection of alpha human papillomaviruses in archival formalin-fixed, paraffin-embedded (FFPE) tissue specimens. J. Clin. Virol. 2016, 76 (Suppl. 1), S88–S97. [Google Scholar] [CrossRef] [PubMed]
- Herrarez-Hernandez, E.; Alvarez-Perez, M.; Navarro-Bustos, G.; Esquivias, J.; Alonso, S.; Aneiros-Fernandez, J.; Lacruz-Pelea, C.; Sanchez-Aguera, M.; Santamaria, J.S.; Chanon de Antonio, J.; et al. HPV Direct Flow CHIP: A new human papillomavirus genotyping method based on direct PCR from crude-cell extras. J. Virol. Methods 2013, 193, 9–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rideg, O.; Oszter, A.; Makk, E.; Kálmán, E.; Farkas, K.; Tornóczky, T.; Kovács, K. Wide Spectrum Analysis of Human Papillomavirus Genotypes in External Anogenital Warts. Vaccines 2021, 9, 604. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, A.K.; Myers, L.; Hammons, A.F.; Clark, R.A.; Dunlap, K.; Kissinger, P.J.; Hagensee, M.E. Prevalence and clustering patterns of human papillomavirus genotypes in multiple infections. Cancer Epidemiol. Biomarkers Prev. 2005, 14, 2439–2445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaturvedi, A.K.; Katki, H.A.; Hildesheim, A.; Rodríguez, A.C.; Quint, W.; Schiffman, M.; Van Doorn, L.J.; Porras, C.; Wacholder, S.; Gonzalez, P.; et al. Human papillomavirus infection with multiple types: Pattern of coinfection and risk of cervical disease. J. Infect. Dis. 2011, 203, 910–920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trottier, H.; Mahmud, S.; Costa, M.C.; Sobrinho, J.P.; Duarte-Franco, E.; Rohan, T.E.; Ferenczy, A.; Villa, L.L.; Franco, E.L. Human papillomavirus infections with multiple types and risk of cervical neoplasia. Cancer Epidemiol. Biomarkers Prev. 2006, 15, 1274–1280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chagas, B.S.; Comar, M.; Gurgel, A.P.; Paiva, S.; Seraceni, S.; de Freitas, A.C.; Crovella, S. Association Study between Cervical Lesions and Single or Multiple Vaccine-Target and Non-Vaccine Target Human Papillomavirus (HPV) Types in Women from Northeastern Brazil. PLoS ONE 2015, 10, e0132570. [Google Scholar] [CrossRef] [Green Version]
- Dickson, E.L.; Vogel, R.I.; Geller, M.A.; Downs, L.S., Jr. Cervical cytology and multiple type HPV infection: A study of 8182 women ages 31-65. Gynecol. Oncol. 2014, 133, 405–408. [Google Scholar] [CrossRef] [Green Version]
- Mejlhede, N.; Pedersen, B.V.; Frisch, M.; Fomsgaard, A. Multiple human papilloma virus types in cervical infections: Competition or synergy? APMIS 2010, 118, 346–352. [Google Scholar] [CrossRef]
- Salazar, K.L.; Zhou, H.S.; Xu, J.; Peterson, L.E.; Schwartz, M.R.; Mody, D.R.; Ge, Y. Multiple Human Papilloma Virus Infections and Their Impact on the Development of High-Risk Cervical Lesions. Acta Cytol. 2015, 59, 391–398. [Google Scholar] [CrossRef]
- Moody, C.A.; Laimins, L.A. Human papillomavirus oncoproteins: Pathways to transformation. Nat. Rev. Cancer 2010, 10, 550–560. [Google Scholar] [CrossRef]
- Groves, I.J.; Coleman, N. Pathogenesis of human papillomavirus-associated mucosal disease. J. Pathol. 2015, 235, 527–538. [Google Scholar] [CrossRef] [Green Version]
- Kyo, S.; Klumpp, D.J.; Inoue, M.; Kanaya, T.; Laimins, L.A. Expression of AP1 during cellular differentiation determines human papillomavirus E6/E7 expression in stratified epithelial cells. J. Gen. Virol. 1997, 78, 401–411. [Google Scholar] [CrossRef]
- Galamb, A.; Pajor, A.; Langmár, Z.; Sobel, G. Az első magyarországi humán papillomavírus központ tapasztalatai (2007–2011) [Results of the first human papilloma virus center in Hungary (2007–2011)]. Orv. Hetil. 2011, 152, 1804–1807. [Google Scholar] [CrossRef]
- Nakagawa, M.; Greenfield, W.; Moerman-Herzog, A.; Coleman, H.N. Cross-Reactivity, Epitope Spreading, and De Novo Immune Stimulation Are Possible Mechanisms of Cross-Protection of Nonvaccine Human Papillomavirus (HPV) Types in Recipients of HPV Therapeutic Vaccines. Clin. Vaccine Immunol. 2015, 22, 679–687. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Song, S.; He, M.; Wang, D.; Shi, J.; Liu, X.; Li, Y.; Chi, X.; Wei, S.; Yang, Y.; et al. Rational design of a triple-type human papillomavirus vaccine by compromising viral-type specificity. Nat. Commun. 2018, 9, 5360. [Google Scholar] [CrossRef] [Green Version]
- Valasoulis, G.; Pouliakis, A.; Michail, G.; Kotarridi, C.; Spathis, A.; Kyrgiou, M.; Paraskevaidis, E.; Daponte, A. Alterations of HPV-Related Biomarkers after Prophylactic HPV Vaccination. A Prospective Pilot Observational Study in Greek Women. Cancers 2020, 12, 1164. [Google Scholar] [CrossRef]
- Di Donato, V.; Caruso, G.; Petrillo, M.; Kontopantelis, E.; Palaia, I.; Perniola, G.; Plotti, F.; Angioli, R.; Muzii, L.; Benedetti Panici, P.; et al. Adjuvant HPV Vaccination to Prevent Recurrent Cervical Dysplasia after Surgical Treatment: A Meta-Analysis. Vaccines 2021, 9, 410. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Number of Infections (%) | ||||||
|---|---|---|---|---|---|---|
| HPV Genotypes | Number of Mono-Infection | Number of Multi-Infection | Number of Total Infections | |||
| High-Risk (HR) HPV Genotypes | FFPE Cone Samples (n = 30) | PAP Smears (n = 6) | FFPE Cone Samples (n = 47) | PAP Smears (n = 138) | FFPE Cone Samples (n = 77) | PAP Smears (n = 144) |
| 16 (VT) | 14 (46.66%) | 4 (66.66%) | 9 (19.14%) | 23 (16.66%) | 23 (29.87%) | 27 (18.75%) |
| 31 (VT) | 6 (20.00%) | - | 3 (6.38%) | 15 (10.86%) | 9 (11.68%) | 15 (10.41%) |
| 51 (VT) | - | - | 6 (12.76%) | 13 (9.42%) | 6 (7.79%) | 13 (9.02%) |
| 33 (VT) | 4 (13.33%) | - | 2 (4.25%) | 9 (6.52%) | 6 (7.79%) | 9 (6.25%) |
| 35 (NVT) | 1 (3.33%) | - | 4 (8.51%) | 7 (5.07%) | 5 (6.49%) | 7 (4.86%) |
| 18 (VT) | - | - | 3 (6.38%) | 8 (5.79%) | 3 (3.89%) | 8 (5.55%) |
| 52 (VT) | 1 (3.33%) | 1 (16.66%) | 2 (4.25%) | 4 (2.89%) | 3 (3.89%) | 5 (3.47%) |
| 53 (NVT) | - | - | 3 (6.38%) | 4 (2.89%) | 3 (3.89%) | 4 (2.77%) |
| 56 (NVT) | - | - | 3 (6.38%) | 7 (5.07%) | 3 (3.89%) | 7 (4.86%) |
| 58 (VT) | 1 (3.33%) | - | 2 (4.25%) | 10 (7.24%) | 3 (3.89%) | 10 (6.94%) |
| 45 (VT) | 1 (3.33%) | 1 (16.66%) | 1 (2.12%) | 3 (2.17%) | 2 (2.59%) | 4 (2.77%) |
| 82 (NVT) | 1 (3.33%) | - | 1 (2.12%) | 2 (1.44%) | 2 (2.59%) | 2 (1.38%) |
| 68 (NVT) | 1 (3.33%) | - | - | 1 (0.72%) | 1 (1.29%) | 1 (0.69%) |
| 73 (NVT) | - | - | 1 (2.12%) | 2 (1.44%) | 1 (1.29%) | 2 (1.38%) |
| 39 (NVT) | - | - | 1 (2.12%) | 2 (1.44%) | 1 (1.29%) | 2 (1.38%) |
| 66 (NVT) | - | - | 1 (2.12%) | 4 (2.89%) | 1 (1.29%) | 4 (2.77%) |
| Low-risk (LR) HPV genotypes | ||||||
| 42 (NVT) | - | - | 1 (2.12%) | 4 (2.89%) | 1 (1.29%) | 4 (2.77%) |
| 11 (VT) | - | - | 1 (2.12%) | - | 1 (1.29%) | - |
| 70 (NVT) | - | - | 1 (2.12%) | 3 (2.17%) | 1 (1.29%) | 3 (2.08%) |
| 54 (NVT) | - | - | 1 (2.12%) | 2 (1.44%) | 1 (1.29%) | 2 (1.38%) |
| 62/81 (NVT) | - | - | 1 (2.12%) | 5 (3.62%) | 1 (1.29%) | 5 (3.47%) |
| 6 (VT) | - | - | - | 3 (2.17%) | - | 3 (2.08%) |
| 67 (NVT) | - | - | - | 3 (2.17%) | - | 3 (2.08%) |
| 44/55 (NVT) | - | - | - | 1 (0.72%) | - | 1 (0.69%) |
| 84 (NVT) | - | - | - | 1 (0.72%) | - | 1 (0.69%) |
| 61 (NVT) | - | - | - | 1 (0.72%) | - | 1 (0.69%) |
| 43 (NVT) | - | - | - | 1 (0.72%) | - | 1 (0.69%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rideg, O.; Dergez, T.; Farkas, K.; Kovács, K.; Kálmán, E.; Tornóczky, T.; Oszter, A. High Prevalence of Non-Vaccinated Oncogenic Human Papillomavirus Genotypes in High-Grade Squamous Intraepithelial Lesions of the Cervix: Thought-Provoking Results of a Detailed HPV Genotype Analysis. Vaccines 2022, 10, 748. https://doi.org/10.3390/vaccines10050748
Rideg O, Dergez T, Farkas K, Kovács K, Kálmán E, Tornóczky T, Oszter A. High Prevalence of Non-Vaccinated Oncogenic Human Papillomavirus Genotypes in High-Grade Squamous Intraepithelial Lesions of the Cervix: Thought-Provoking Results of a Detailed HPV Genotype Analysis. Vaccines. 2022; 10(5):748. https://doi.org/10.3390/vaccines10050748
Chicago/Turabian StyleRideg, Orsolya, Tímea Dergez, Kornélia Farkas, Krisztina Kovács, Endre Kálmán, Tamás Tornóczky, and Angéla Oszter. 2022. "High Prevalence of Non-Vaccinated Oncogenic Human Papillomavirus Genotypes in High-Grade Squamous Intraepithelial Lesions of the Cervix: Thought-Provoking Results of a Detailed HPV Genotype Analysis" Vaccines 10, no. 5: 748. https://doi.org/10.3390/vaccines10050748