
Systemic Cancer Therapy Does Not Significantly Impact Early Vaccine-Elicited SARS-CoV-2 Immunity in Patients with Solid Tumors

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. SARS-CoV-2 Spike ELISA
2.3. IFN-γ ELISPOT
2.4. Statistical Analysis
3. Results
3.1. Study Design and Demographics
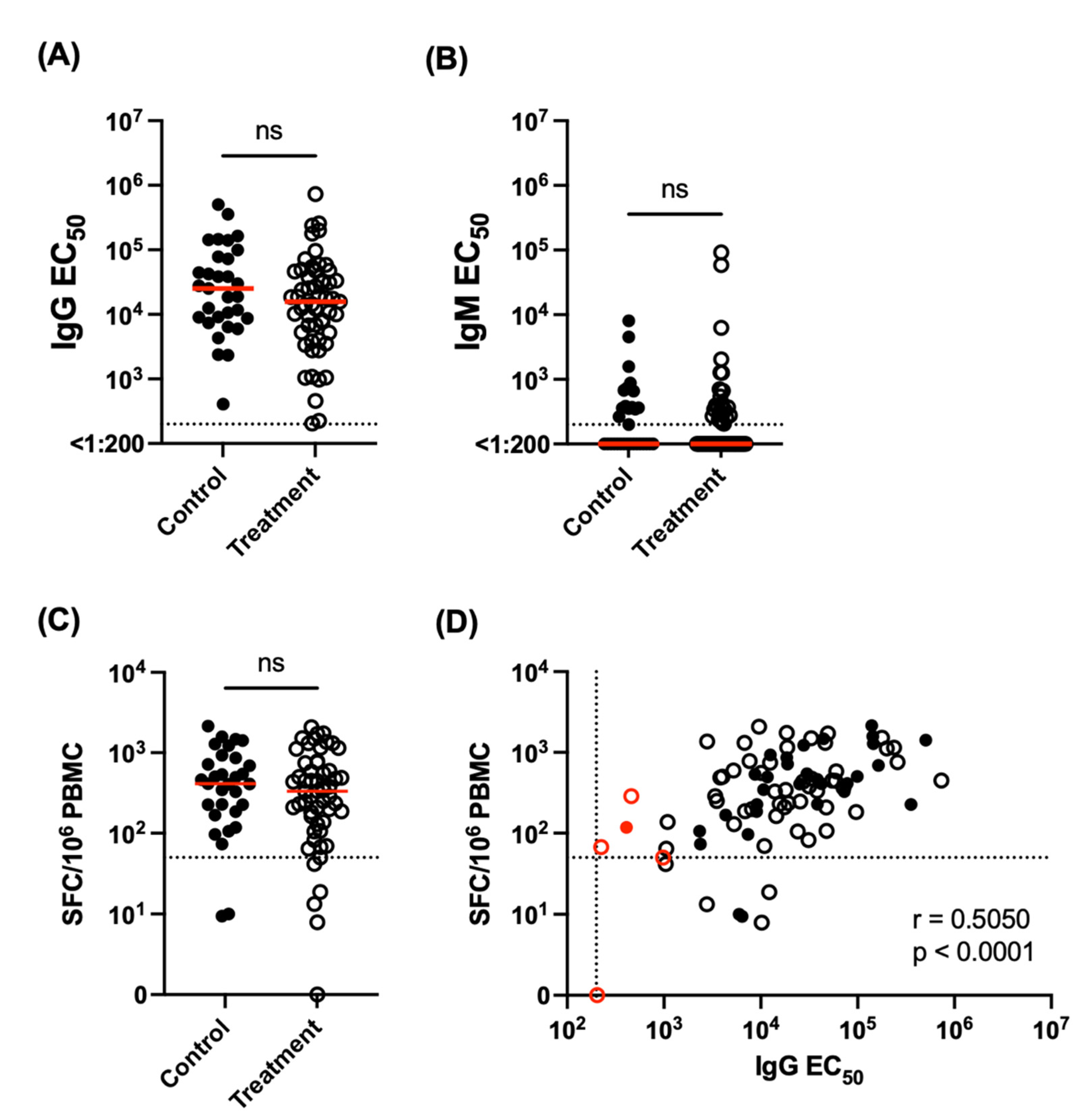
3.2. SARS-CoV-2 Vaccine Immunogenicity
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grivas, P.; Khaki, A.; Wise-Draper, T.; French, B.; Hennessy, C.; Hsu, C.-Y.; Shyr, Y.; Li, X.; Choueiri, T.; Painter, C.; et al. Association of clinical factors and recent anticancer therapy with COVID-19 severity among patients with cancer: A report from the COVID-19 and Cancer Consortium. Ann Oncol. 2021, 32, 787–800. [Google Scholar] [CrossRef] [PubMed]
- Martin-Moro, F.; Marquet, J.; Piris, M.; Michael, B.M.; Sáez, A.J.; Corona, M.; Jiménez, C.; Astibia, B.; García, I.; Rodríguez, E.; et al. Survival study of hospitalised patients with concurrent COVID-19 and haematological malignancies. Br. J. Haematol. 2020, 190, e16–e20. [Google Scholar] [CrossRef]
- Robilotti, E.V.; Babady, N.E.; Mead, P.A.; Rolling, T.; Perez-Johnston, R.; Bernardes, M.; Bogler, Y.; Caldararo, M.; Figueroa, C.J.; Glickman, M.S.; et al. Determinants of COVID-19 disease severity in patients with cancer. Nat. Med. 2020, 26, 1218–1223. [Google Scholar] [CrossRef] [PubMed]
- Ruthrich, M.M.; Giessen-Jung, C.; Borgmann, S.; Classen, A.Y.; Dolff, S.; Grüner, B.; Hanses, F.; Isberner, N.; Köhler, P.; Lanznaster, J.; et al. COVID-19 in cancer patients: Clinical characteristics and outcome-an analysis of the LEOSS registry. Ann. Hematol. 2021, 100, 383–393. [Google Scholar] [CrossRef] [PubMed]
- Sharafeldin, N.; Bates, B.; Song, Q.; Madhira, V.; Yan, Y.; Dong, S.; Lee, E.; Kuhrt, N.; Shao, Y.R.; Liu, F.; et al. Outcomes of COVID-19 in Patients With Cancer: Report From the National COVID Cohort Collaborative (N3C). J. Clin. Oncol. 2021, 39, 2232–2246. [Google Scholar] [CrossRef]
- Venkatesulu, B.P.; Chandrasekar, V.T.; Girdhar, P.; Advani, P.; Sharma, A.; Elumalai, T.; Hsieh, C.E.; I Elghazawy, H.; Verma, V.; Krishnan, S.; et al. A Systematic Review and Meta-Analysis of Cancer Patients Affected by a Novel Coronavirus. JNCI Cancer Spectr. 2021, 5, pkaa102. [Google Scholar] [CrossRef] [PubMed]
- Gosain, R.; Abdou, Y.; Singh, A.; Rana, N.; Puzanov, I.; Ernstoff, M.S. COVID-19 and Cancer: A Comprehensive Review. Curr. Oncol. Rep. 2020, 22, 53. [Google Scholar] [CrossRef]
- Shehata, M.A.; Karim, N.A. Influenza vaccination in cancer patients undergoing systemic therapy. Clin. Med. Insights Oncol. 2014, 8, 57–64. [Google Scholar] [CrossRef]
- Laubli, H.; Balmelli, C.; Kaufmann, L.; Stanczak, M.; Syedbasha, M.; Vogt, D.; Hertig, A.; Müller, B.; Gautschi, O.; Stenner, F.; et al. Influenza vaccination of cancer patients during PD-1 blockade induces serological protection but may raise the risk for immune-related adverse events. J. Immunother. Cancer 2018, 6, 40. [Google Scholar] [CrossRef] [Green Version]
- Thomas, S.J.; Perez, J.L.; Lockhart, S.P.; Hariharan, S.; Kitchin, N.; Bailey, R.; Liau, K.; Lagkadinou, E.; Türeci, Ö.; Şahin, U.; et al. Efficacy and safety of the BNT162b2 mRNA COVID-19 vaccine in participants with a history of cancer: Subgroup analysis of a global phase 3 randomized clinical trial. Vaccine 2022, 40, 1483–1492. [Google Scholar] [CrossRef]
- Oosting, S.F.; Van der Veldt, A.A.M.; Kessel, G.C.H.; Fehrmann, R.S.N.; van Binnendijk, R.S.; Dingemans, A.-M.C.; Smit, E.F.; Hiltermann, T.J.N.; Hartog, G.D.; Jalving, M.; et al. mRNA-1273 COVID-19 vaccination in patients receiving chemotherapy, immunotherapy, or chemoimmunotherapy for solid tumours: A prospective, multicentre, non-inferiority trial. Lancet Oncol. 2021, 22, 1681–1691. [Google Scholar] [CrossRef]
- Greenberger, L.M.; Saltzman, L.A.; Senefeld, J.W.; Johnson, P.W.; DeGennaro, L.J.; Nichols, G.L. Antibody response to SARS-CoV-2 vaccines in patients with hematologic malignancies. Cancer Cell 2021, 39, 1031–1033. [Google Scholar] [CrossRef] [PubMed]
- Addeo, A.; Shah, P.K.; Bordry, N.; Hudson, R.D.; Albracht, B.; Di Marco, M.; Kaklamani, V.; Dietrich, P.-Y.; Taylor, B.S.; Shah, D.P.; et al. Immunogenicity of SARS-CoV-2 messenger RNA vaccines in patients with cancer. Cancer Cell 2021, 39, 1091–1098.e2. [Google Scholar] [CrossRef] [PubMed]
- Benjamini, O.; Rokach, L.; Itchaki, G.; Braester, A.; Shvidel, L.; Goldschmidt, N.; Shapira, S.; Dally, N.; Avigdor, A.; Rahav, G.; et al. Safety and efficacy of BNT162b mRNA Covid19 Vaccine in patients with chronic lymphocytic leukemia. Haematologica 2021, 8, E542–E544. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.H.; Campbell, N.; Johnson, M.; Joseph-Pietras, D.; Collins, G.P.; O’Callaghan, A.; Fox, C.P.; Ahearne, M.; Johnson, P.W.; Goldblatt, D.; et al. Antibody responses after SARS-CoV-2 vaccination in patients with lymphoma. Lancet Haematol. 2021, 8, e542–e544. [Google Scholar] [CrossRef]
- Herishanu, Y.; Avivi, I.; Aharon, A.; Shefer, G.; Levi, S.; Bronstein, Y.; Morales, M.; Ziv-Baran, T.; Arbel, Y.S.; Scarfò, L.; et al. Efficacy of the BNT162b2 mRNA COVID-19 vaccine in patients with chronic lymphocytic leukemia. Blood 2021, 137, 3165–3173. [Google Scholar] [CrossRef]
- Moss, P. The T cell immune response against SARS-CoV-2. Nat. Immunol. 2022, 23, 186–193. [Google Scholar] [CrossRef]
- Kundu, R.; Narean, J.S.; Wang, L.; Fenn, J.; Pillay, T.; Fernandez, N.D.; Conibear, E.; Koycheva, A.; Davies, M.; Lalvani, A.; et al. Cross-reactive memory T cells associate with protection against SARS-CoV-2 infection in COVID-19 contacts. Nat. Commun. 2022, 13, 80. [Google Scholar] [CrossRef]
- Swadling, L.; Diniz, M.O.; Schmidt, N.M.; Amin, O.E.; Chandran, A.; Shaw, E.; Pade, C.; Gibbons, J.M.; Le Bert, N.; Maini, M.K.; et al. Pre-existing polymerase-specific T cells expand in abortive seronegative SARS-CoV-2. Nature 2022, 601, 110–117. [Google Scholar] [CrossRef]
- Liu, J.; Chandrashekar, A.; Sellers, D.; Barrett, J.; Jacob-Dolan, C.; Lifton, M.; McMahan, K.; Sciacca, M.; VanWyk, H.; Barouch, D.H.; et al. Vaccines Elicit Highly Conserved Cellular Immunity to SARS-CoV-2 Omicron. Nature 2022, 603, 493–496. [Google Scholar] [CrossRef]
- Gao, Y.; Cai, C.; Grifoni, A.; Müller, T.R.; Niessl, J.; Olofsson, A.; Humbert, M.; Hansson, L.; Österborg, A.; Buggert, M.; et al. Ancestral SARS-CoV-2-specific T cells cross-recognize the Omicron variant. Nat. Med. 2022, 28, 472–476. [Google Scholar] [CrossRef] [PubMed]
- Kessel, G.C.H.; Geers, D.; Schmitz, K.S.; Mykytyn, A.Z.; Lamers, M.M.; Bogers, S.; Gommers, L.; Sablerolles, R.S.G.; Nieuwkoop, N.N.; de Vries, R.D.; et al. Divergent SARS CoV-2 Omicron-reactive T- and B cell responses in COVID-19 vaccine recipients. Sci. Immunol. 2022, 7, eabo2202. [Google Scholar]
- Garcia-Beltran, W.F.; Denis, K.J.S.; Hoelzemer, A.; Lam, E.C.; Nitido, A.D.; Sheehan, M.L.; Berrios, C.; Ofoman, O.; Chang, C.C.; Balazs, A.B.; et al. mRNA-based COVID-19 vaccine boosters induce neutralizing immunity against SARS-CoV-2 Omicron variant. Cell 2022, 185, 457–466.e4. [Google Scholar] [CrossRef] [PubMed]
- Thakkar, A.; Gonzalez-Lugo, J.D.; Goradia, N.; Gali, R.; Shapiro, L.C.; Pradhan, K.; Rahman, S.; Kim, S.Y.; Ko, B.; Sica, R.A.; et al. Seroconversion rates following COVID-19 vaccination among patients with cancer. Cancer Cell 2021, 39, 1081–1090.e2. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Control (n = 31) | Treatment (n = 55) | |
|---|---|---|
| Median Age (range) | 64 (50–83) | 66 (41–85) |
| Sex | ||
| Male | 54.8% (17/31) | 49.1% (27/55) |
| Female | 45.2% (14/31) | 50.9% (28/55) |
| Vaccine type | ||
| Pfizer | 54.8% (17/31) | 60.0% (33/55) |
| Moderna | 45.2% (14/31) | 40.0% (22/55) |
| Primary cancer location | ||
| Anus | 0% (0/31) | 5.5% (3/55) |
| Bile Duct | 0% (0/31) | 1.8% (1/55) |
| Breast | 25.8% (8/31) | 1.8% (1/55) |
| Colon | 0% (0/31) | 7.3% (4/55) |
| Endometrium | 3.2% (1/31) | 1.8% (1/55) |
| Esophagus | 0% (0/31) | 1.8% (1/55) |
| H&N | 9.7% (3/31) | 1.8% (1/55) |
| Liver | 0% (0/31) | 3.6% (2/55) |
| Lung | 16.1% (5/31) | 58.2% (32/55) |
| Pancreas | 0% (0/31) | 10.9% (6/55) |
| Parotid | 3.2% (1/31) | 0% (0/55) |
| Peritoneum | 0% (0/31) | 1.8% (1/55) |
| Prostate | 38.7% 12/31 | 0% (0/55) |
| Rectum | 3.2% (1/31) | 0% (0/55) |
| Tongue | 0% (0/31) | 1.8% (1/55) |
| Vulva | 0% (0/31) | 1.8% (1/55) |
| Stage | ||
| 0 | 3.2% (1/31) | 0% (0/55) |
| I | 25.8% (8/31) | 1.8% (1/55) |
| II | 41.9% (13/31) | 7.3% (4/55) |
| III | 19.4% (6/31) | 32.7% (18/55) |
| IV | 9.7% (3/31) | 58.2% (32/55) |
| Systemic Anticancer Treatment | |
|---|---|
| Chemotherapy | 25.5% (14/55) |
| Immunotherapy | 38.2% (21/55) |
| Chemotherapy and Immunotherapy | 14.5% (8/55) |
| Chemotherapy, immunotherapy, and radiation | 21.8% (12/55) |
| Age | Sex | Primary Tumor Site | Stage | Current Treatment | Vaccine | IgG EC50 | ELISPOT SFC/106 PBMC |
|---|---|---|---|---|---|---|---|
| 74 | F | Lung | IIIA | Durvalumab | Pfizer | 1:204 | 0.00 |
| 77 | M | Lung | IIIA | Alimta, Keytruda | Pfizer | 1:224 | 67.50 |
| 69 | M | Prostate | IIIB | N/A | Pfizer | 1:409 | 118.33 |
| 57 | F | Lung | IV | Pembrolizumab, Pemetrexed | Pfizer | 1:459 | 287.78 |
| 67 | M | Lung | IVB | Pembrolizumab, Carboplatin, Alimta | Pfizer | 1:980 | 50.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Waickman, A.T.; Lu, J.; Chase, C.; Fang, H.; McDowell, E.; Bingham, E.; Bogart, J.; Graziano, S.; Thomas, S.J.; Gentile, T. Systemic Cancer Therapy Does Not Significantly Impact Early Vaccine-Elicited SARS-CoV-2 Immunity in Patients with Solid Tumors. Vaccines 2022, 10, 738. https://doi.org/10.3390/vaccines10050738
Waickman AT, Lu J, Chase C, Fang H, McDowell E, Bingham E, Bogart J, Graziano S, Thomas SJ, Gentile T. Systemic Cancer Therapy Does Not Significantly Impact Early Vaccine-Elicited SARS-CoV-2 Immunity in Patients with Solid Tumors. Vaccines. 2022; 10(5):738. https://doi.org/10.3390/vaccines10050738
Chicago/Turabian StyleWaickman, Adam T., Joseph Lu, Corey Chase, Hengsheng Fang, Erinn McDowell, Erin Bingham, Jeffrey Bogart, Stephen Graziano, Stephen J. Thomas, and Teresa Gentile. 2022. "Systemic Cancer Therapy Does Not Significantly Impact Early Vaccine-Elicited SARS-CoV-2 Immunity in Patients with Solid Tumors" Vaccines 10, no. 5: 738. https://doi.org/10.3390/vaccines10050738