
COVID-19 Vaccines: Fear of Side Effects among German Health Care Workers

 , , , , , , and
, , , , , , and 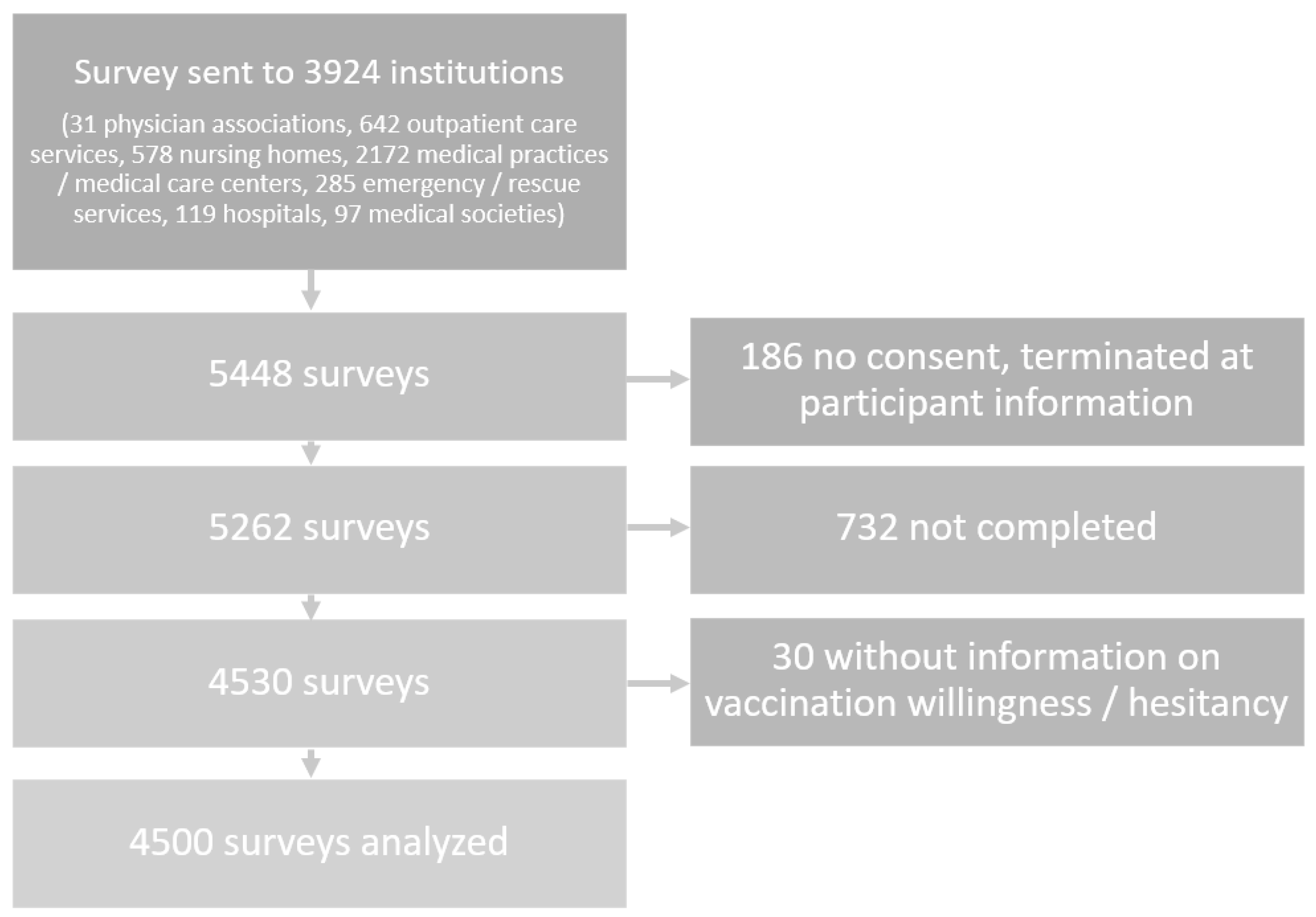{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Category Construction and Qualitative Analysis
2.3. Quantitative Statistical Analysis
2.4. Ethics
3. Results
3.1. Data Basis
3.2. Experienced Side Effects
3.2.1. Frequencies of Experienced Side Effects
3.2.2. Associations between Experienced Side Effects and Fear of Side Effects after a COVID-19-Vaccination
3.3. Fear of Short-Term Side Effects
3.3.1. Frequencies of Feared Short-Term Side Effects
3.3.2. Feared Short-Term Side Effects and Vaccine Hesitancy
3.4. Fear of Long-Term Side Effects
3.4.1. Frequencies of Feared Long-Term Side Effects
3.4.2. Feared Long-Term Side Effects and Vaccine Hesitancy
3.5. Associations between Professional Groups and Feared Side Effects
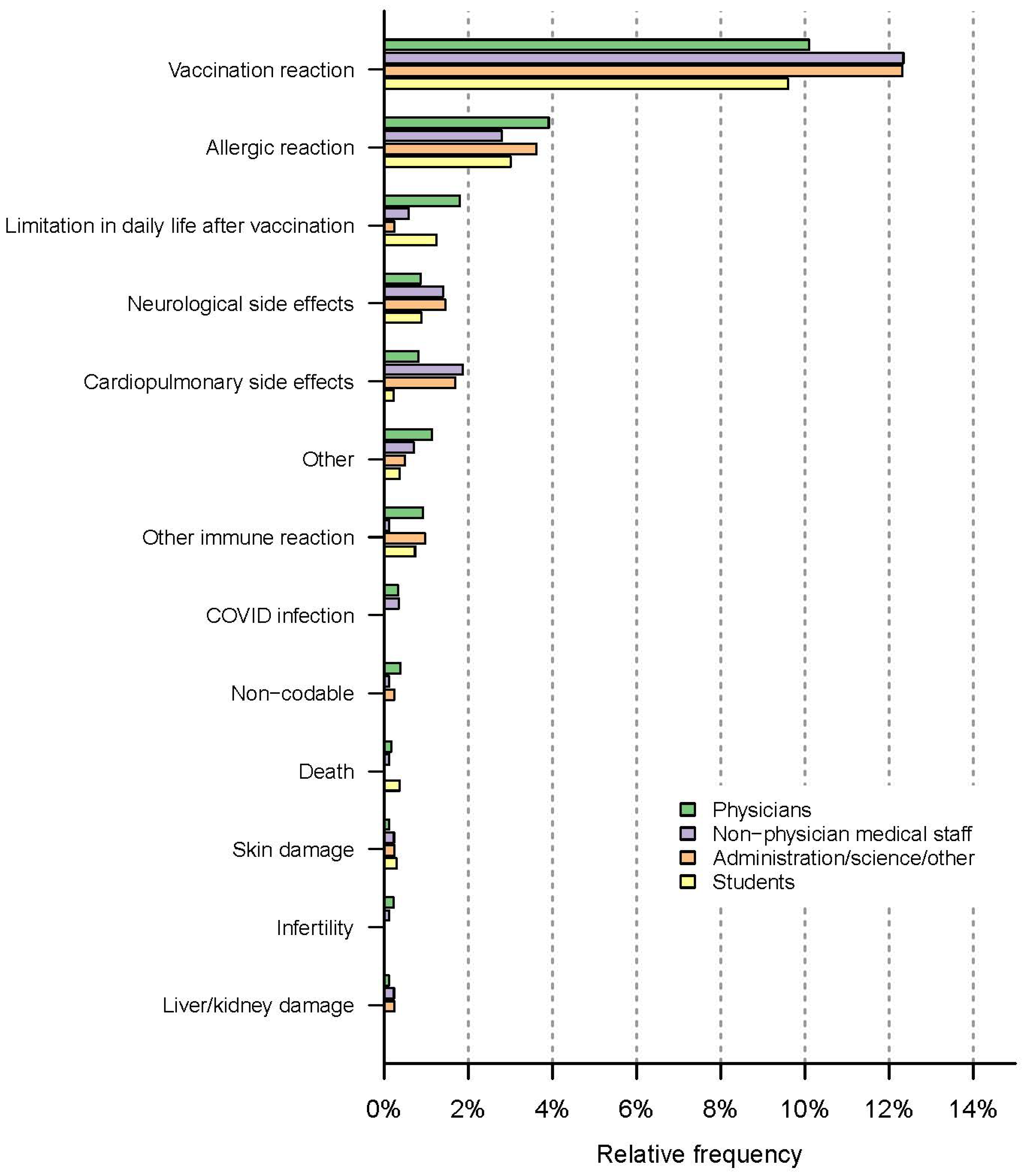
3.5.1. Associations between Professional Groups and Fear of Short-Term Side Effects
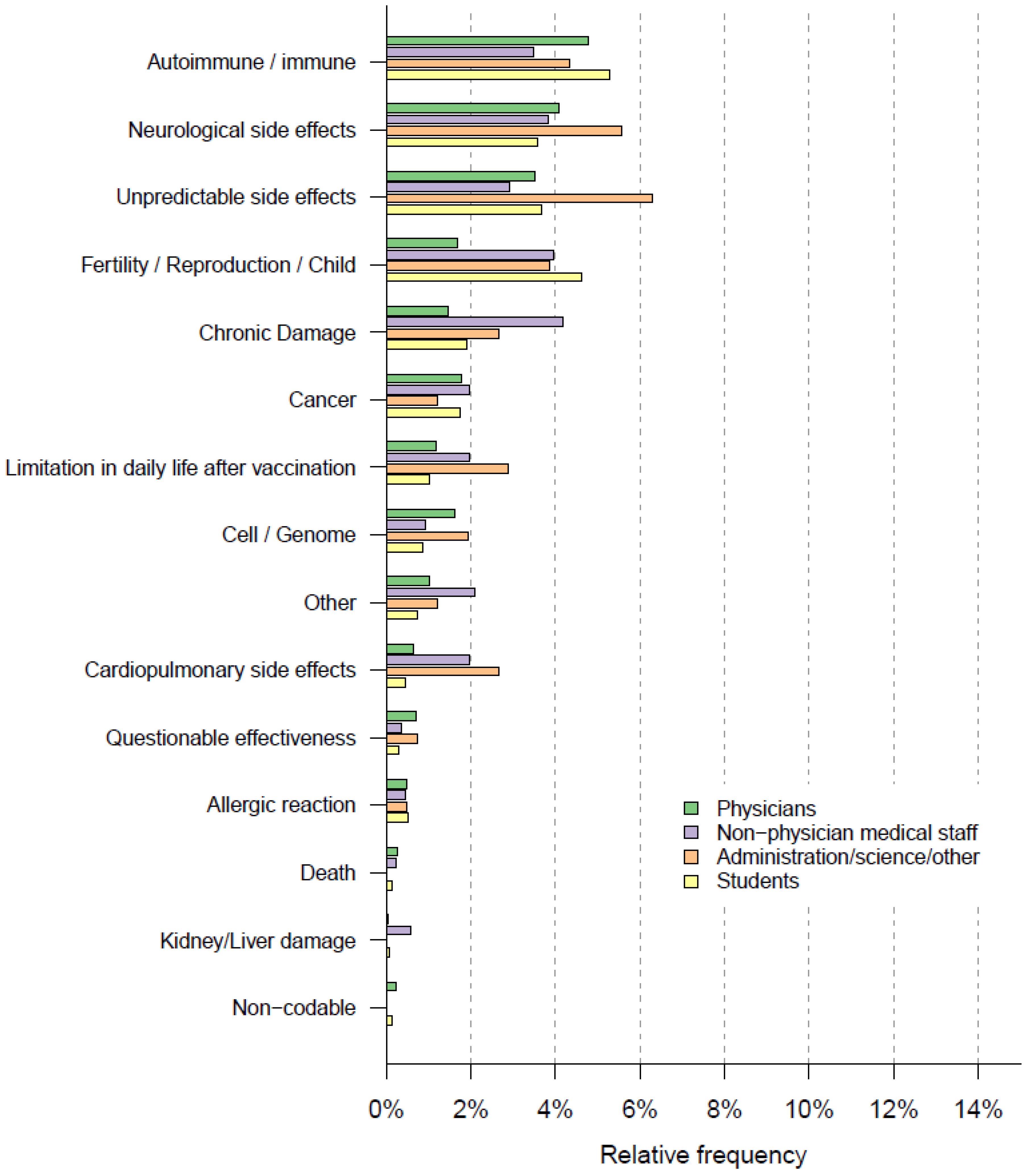
3.5.2. Associations between Professional Groups and Fear of Long-Term Side Effects
3.6. Attitude toward Vaccination within Colleagues and Friends, and Associations with Fear of Short-Term Side Effects
4. Discussion
4.1. Experienced Side Effects
4.2. Fear of Short- and Long-Term Side Effects
4.3. Fear of Side Effects and Association with Vaccine Hesitancy
4.4. Associations between Professional Groups and Fear of Side Effects
4.5. Attitude toward Vaccination within Colleagues and Friends, and Associations with Fear of Side Effects
4.6. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Verity, R.; Okell, L.C.; Dorigatti, I.; Winskill, P.; Whittaker, C.; Imai, N.; Cuomo-Dannenburg, G.; Thompson, H.; TWalker, P.G.; Fu, H.; et al. Estimates of the severity of coronavirus disease 2019: A model-based analysis. Lancet Infect. Dis. 2020, 20, 669–677. [Google Scholar] [CrossRef]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 long-term effects of COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16144. [Google Scholar] [CrossRef] [PubMed]
- Mallory, M.L.; Lindesmith, L.C.; Baric, R.S. Vaccination-induced herd immunity: Successes and challenges. J. Allergy Clin. Immunol. 2018, 142, 64–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eichner, M. Berichtüber Die Erstellung Einer Strukturierten Literaturrecherche zur Rolle der Geimpften am SARS-CoV-2-Pandemiegeschehen; Epimos GmbH, Ed.; Ministerium für Soziales, Gesundheit und Integration Baden-Württemberg: Stuttgart, Germany, 2021. [Google Scholar]
- Siciliani, L.; Wild, C.; McKee, M.; Kringos, D.; Barry, M.M.; Barros, P.P.; Maeseneerg, J.; Murauskieneh, L.; Ricciardii, W.; On behalf of the members of the Expert Panel on Effective Ways of Investing in Health. Strengthening vaccination programmes and health systems in the European Union: A framework for action. Health Policy 2020, 124, 511–518. [Google Scholar] [CrossRef]
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Friedrich, M. WHO’s top health threats for 2019. JAMA Netw. 2019, 321, 1041. [Google Scholar] [CrossRef]
- Squeri, R.; Di Pietro, A.; La Fauci, V.; Genovese, C. Healthcare workers’ vaccination at European and Italian level: A narrative review. Acta Bio Med. Atenei Parm. 2019, 90 (Suppl. 9), 45. [Google Scholar]
- Nomura, S.; Eguchi, A.; Yoneoka, D.; Kawashima, T.; Tanoue, Y.; Murakami, M.; Sakamoto, H.; Maruyama-Sakurai, K.; Gilmour, S.; Shi, S.; et al. Reasons for being unsure or unwilling regarding intention to take COVID-19 vaccine among Japanese people: A large cross-sectional national survey. Lancet Reg. Health West. Pac. 2021, 18, 100223. [Google Scholar] [CrossRef]
- Kelkar, A.H.; Blake, J.A.; Cherabuddi, K.; Cornett, H.; McKee, B.L.; Cogle, C.R. Vaccine Enthusiasm and Hesitancy in Cancer Patients and the Impact of a Webinar. Healthcare 2021, 9, 351. [Google Scholar] [CrossRef]
- Robert Koch Institute. KROCO-Die Krankenhausbasierte Online-Befragung zur COVID-19-Impfung Ergebnisbericht zur ersten Befragungswelle; Robert Koch Institute, Ed.; Ergebnisbericht Erste Welle: Berlin, Germany, 2021. [Google Scholar]
- Holzmann-Littig, C.; Braunisch, M.C.; Kranke, P.; Popp, M.; Seeber, C.; Fichtner, F.; Littig, B.; Carbajo-Lozoya, J.; Allwang, C.; Frank, T.; et al. COVID-19 Vaccination Acceptance and Hesitancy among Healthcare Workers in Germany. Vaccines 2021, 9, 777. [Google Scholar] [CrossRef]
- Robert Koch Institute. KROCO-Die Krankenhausbasierte Online-Befragung zur COVID-19-Impfung – Ergebnisbericht zur dritten Befragungswelle; Robert Koch Institute, Ed.; Ergebnisbericht Erste Welle: Berlin, Germany, 2022. [Google Scholar]
- Vygen-Bonnet, S.; Koch, J.; Bogdan, C.; Harder, T.; Heininger, U.; Kling, K.; Littmann, M.; Meerpohl, J.; Meyer, H.; Mertens, T.; et al. Beschluss und Wissenschaftliche Begründung der Ständigen Impfkommission (STIKO) für die COVID-19-Impfempfehlung. Robert Koch Inst. 2020, 3, 63. [Google Scholar]
- Kwok, K.O.; Li, K.-K.; Wei, W.I.; Tang, A.; Wong, S.Y.S.; Lee, S.S. Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int. J. Nurs. Stud. 2021, 114, 103854. [Google Scholar] [CrossRef]
- Li, M.; Luo, Y.; Watson, R.; Zheng, Y.; Ren, J.; Tang, J.; Chen, Y. Healthcare workers’(HCWs) attitudes and related factors towards COVID-19 vaccination: A rapid systematic review. Postgrad. Med. J. 2021, 140195. [Google Scholar] [CrossRef]
- Wang, K.; Wong, E.L.Y.; Ho, K.F.; Cheung, A.W.L.; Chan, E.Y.Y.; Yeoh, E.K.; Wong, S.Y.S. Intention of nurses to accept coronavirus disease 2019 vaccination and change of intention to accept seasonal influenza vaccination during the coronavirus disease 2019 pandemic: A cross-sectional survey. Vaccine 2020, 38, 7049–7056. [Google Scholar] [CrossRef]
- Shaw, J.; Stewart, T.; Anderson, K.B.; Hanley, S.; Thomas, S.J.; Salmon, D.A.; Morley, C. Assessment of US Healthcare Personnel Attitudes Towards Coronavirus Disease 2019 (COVID-19) Vaccination in a Large University Healthcare System. Clin. Infect. Dis. 2021, 73, 1776–1783. [Google Scholar] [CrossRef]
- Shekhar, R.; Sheikh, A.; Upadhyay, S.; Singh, M.; Kottewar, S.; Mir, H.; Barrett, E.; Pal, S. COVID-19 Vaccine Acceptance among Health Care Workers in the United States. Vaccines 2021, 9, 119. [Google Scholar] [CrossRef]
- Unroe, K.T.; Evans, R.; Weaver, L.; Rusyniak, D.; Blackburn, J. Willingness of long-term care staff to receive a COVID-19 vaccine: A single state survey. J. Am. Geriatr. Soc. 2021, 69, 593–599. [Google Scholar] [CrossRef]
- Gagneux-Brunon, A.; Detoc, M.; Bruel, S.; Tardy, B.; Rozaire, O.; Frappe, P.; Botelho-Nevers, E. Intention to get vaccinations against COVID-19 in French healthcare workers during the first pandemic wave: A cross-sectional survey. J. Hosp. Infect. 2021, 108, 168–173. [Google Scholar] [CrossRef]
- Gadoth, M.A.; Halbrook, M.M.; Martin-Blais, R.; Gray, A.; Tobin, N.H.; Ferbas, K.G.; Aldrovandi, M.G.M.; Rimoin, M.A.W. Cross-sectional Assessment of COVID-19 Vaccine Acceptance Among Health Care Workers in Los Angeles. Ann. Intern. Med. 2021, 174, 882–885. [Google Scholar] [CrossRef]
- Di Gennaro, F.; Murri, R.; Segala, F.V.; Cerruti, L.; Abdulle, A.; Saracino, A.; Bavaro, D.F.; Fantoni, M. Attitudes towards Anti-SARS-CoV2 Vaccination among Healthcare Workers: Results from a National Survey in Italy. Viruses 2021, 13, 371. [Google Scholar] [CrossRef]
- Biswas, N.; Mustapha, T.; Khubchandani, J.; Price, J.H. The Nature and Extent of COVID-19 Vaccination Hesitancy in Healthcare Workers. J. Community Health 2021, 46, 1244–1251. [Google Scholar] [CrossRef] [PubMed]
- Stebbins, R.A. Exploratory Research in the Social Sciences; Sage: Thousand Oaks, CA, USA, 2001. [Google Scholar]
- Döring, N.; Bortz, J. Forschungsmethoden und Evaluation; Springer: Wiesbaden, Germany, 2016. [Google Scholar]
- Leiner, D.J. SoSci Survey. 3.1.06 019. Available online: https://www.soscisurvey.de/en/about (accessed on 19 April 2022).
- Eysenbach, G. Improving the quality of Web surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e132. [Google Scholar] [CrossRef] [PubMed]
- Weber, R.P. Basic Content Analysis; Sage: Newbury Park, CA, USA, 1990. [Google Scholar]
- Robert Koch Institute. Tabelle mit den Gemeldeten Impfungen nach Bundesländern und Impfquoten nach Altersgruppen; 13 April 2022; Robert Koch Institute: Berlin, Germany, 2022; Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Daten/Impfquotenmonitoring.html;jsessionid=2A0A76449DC16ABF1B00FE780CFF1716.internet101?nn=13490888 (accessed on 19 April 2022).
- Gastanaduy, P.; Haber, P.; Rota, P.A.; Patel, M. Measles: Centers for Disease Control and Prevention. 2021. Available online: https://www.cdc.gov/vaccines/pubs/pinkbook/meas.html (accessed on 19 April 2022).
- Spencer, J.P.; Pawlowski, R.H.T.; Thomas, S. Vaccine Adverse Events: Separating Myth from Reality. Am. Fam. Physician 2017, 95, 786–794. [Google Scholar] [PubMed]
- Centers for Disease Control and Prevention. Measles, Mumps, Rubella (MMR) Vaccine. 2022. Available online: https://www.cdc.gov/vaccinesafety/vaccines/mmr-vaccine.html (accessed on 19 April 2022).
- Rzymski, P.; Poniedziałek, B.; Fal, A. Willingness to Receive the Booster COVID-19 Vaccine Dose in Poland. Vaccines 2021, 9, 1286. [Google Scholar] [CrossRef]
- Gee, J.; Marquez, P.; Su, J.; Calvert, G.M.; Liu, R.; Myers, T.; Nair, N.; Martin, S.; Clark, T.; Markowitz, L.; et al. First Month of COVID-19 Vaccine Safety Monitoring-United States, December 14, 2020–January 13, 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 283–288. [Google Scholar] [CrossRef]
- Patone, M.; Handunnetthi, L.; Saatci, D.; Pan, J.; Katikireddi, S.V.; Razvi, S.; Hunt, D.; Mei, X.W.; Dixon, S.; Zaccardi, F.; et al. Neurological complications after first dose of COVID-19 vaccines and SARS-CoV-2 infection. Nat. Med. 2021, 27, 2144–2153. [Google Scholar] [CrossRef]
- Barda, N.; Dagan, N.; Ben-Shlomo, Y.; Kepten, E.; Waxman, J.; Ohana, R.; Hernán, M.A.; Lipsitch, M.; Kohane, I.; Netzer, D.; et al. Safety of the BNT162b2 mRNA COVID-19 Vaccine in a Nationwide Setting. N. Engl. J. Med. 2021, 385, 1078–1090. [Google Scholar] [CrossRef]
- Tenforde, M.W.; Olson, S.M.; Self, W.H.; Talbot, H.K.; Lindsell, C.J.; Steingrub, J.S. Effectiveness of Pfizer-BioNTech and Moderna Vaccines Against COVID-19 Among Hospitalized Adults Aged ≥65 Years-United States, January–March 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 674–679. [Google Scholar] [CrossRef]
- Scobie, H.M.; Johnson, A.G.; Suthar, A.B.; Severson, R.; Alden, N.B.; Balter, S.; Bertolino, D.; Blythe, D.; Brady, S.; Cadwell, B.; et al. Monitoring incidence of COVID-19 cases, hospitalizations, and deaths, by vaccination status—13 US jurisdictions, 4 April–17 July 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 1284. [Google Scholar] [CrossRef]
- Sharif, N.; Alzahrani, K.J.; Ahmed, S.N.; Dey, S.K. Efficacy, Immunogenicity and Safety of COVID-19 Vaccines: A Systematic Review and Meta-Analysis. Front. Immunol. 2021, 12, 714170. [Google Scholar] [CrossRef]
- Pormohammad, A.; Zarei, M.; Ghorbani, S.; Mohammadi, M.; Razizadeh, M.H.; Turner, D.L.; Turner, D.L.; Turner, R.J. Efficacy and Safety of COVID-19 Vaccines: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Vaccines 2021, 9, 467. [Google Scholar] [CrossRef]
- Rosenblum, H.G.; Hadler, S.C.; Moulia, D.; Shimabukuro, T.T.; Su, J.R.; Tepper, N.K.; Ess, K.C.; Woo, E.J.; Mba-Jonas, A.; Alimchandani, M.; et al. Use of COVID-19 Vaccines After Reports of Adverse Events Among Adult Recipients of Janssen (Johnson & Johnson) and mRNA COVID-19 Vaccines (Pfizer-BioNTech and Moderna): Update from the Advisory Committee on Immunization Practices-United States, July 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 1094–1099. [Google Scholar]
- Iacobucci, G. COVID-19: No evidence that vaccines can affect fertility, says new guidance. BMJ 2021, 372, 509. [Google Scholar] [CrossRef]
- De Sousa, R.; Morton, A. Emotional Truth. Proc. Aristot. Soc. Suppl. Vol. 2002, 76, 47–75. [Google Scholar]
- Taylor, D.M.; Doria, J.R. Self-serving and group-serving bias in attribution. J. Soc. Psychol. 1981, 113, 201–211. [Google Scholar] [CrossRef]
- Hart, W.; Albarracín, D.; Eagly, A.H.; Brechan, I.; Lindberg, M.J.; Merrill, L. Feeling Validated Versus Being Correct: A Meta-Analysis of Selective Exposure to Information. Psychol. Bull. 2009, 135, 555–588. [Google Scholar] [CrossRef] [Green Version]
- European Commission. Europäische Kommission Erteilt Dritte Zulassung für Sicheren und Wirksamen Impfstoff Gegen COVID-19. 2021. Available online: https://ec.europa.eu/commission/presscorner/detail/de/ip_21_306 (accessed on 19 April 2022).
- European Commission. Union register of Medicinal Products for Human Use 2021. Available online: https://ec.europa.eu/health/documents/community-register/html/h1528.htm (accessed on 19 April 2022).
- Koch, J.; Vygen-Bonnet, S.; Bogdan, C.; Burchard, G.; Garbe, E.; Heininger, U.; Hummers, E.; Keller- Stanislawski, B.; von Kries, R.; Ledig, T.; et al. Wissenschaftliche Begründung der STIKO zur Empfehlung, im Alter unter 30 Jahren Ausschließlich Comirnaty zur COVID-19-Grundimmunisierung und-Auffrischimpfung zu verwenden; STIKO: Berlin, Germany, 2021. [Google Scholar]










Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Holzmann-Littig, C.; Frank, T.; Schmaderer, C.; Braunisch, M.C.; Renders, L.; Kranke, P.; Popp, M.; Seeber, C.; Fichtner, F.; Littig, B.; et al. COVID-19 Vaccines: Fear of Side Effects among German Health Care Workers. Vaccines 2022, 10, 689. https://doi.org/10.3390/vaccines10050689
Holzmann-Littig C, Frank T, Schmaderer C, Braunisch MC, Renders L, Kranke P, Popp M, Seeber C, Fichtner F, Littig B, et al. COVID-19 Vaccines: Fear of Side Effects among German Health Care Workers. Vaccines. 2022; 10(5):689. https://doi.org/10.3390/vaccines10050689
Chicago/Turabian StyleHolzmann-Littig, Christopher, Tamara Frank, Christoph Schmaderer, Matthias C. Braunisch, Lutz Renders, Peter Kranke, Maria Popp, Christian Seeber, Falk Fichtner, Bianca Littig, and et al. 2022. "COVID-19 Vaccines: Fear of Side Effects among German Health Care Workers" Vaccines 10, no. 5: 689. https://doi.org/10.3390/vaccines10050689