
Social Capital, Urbanization Level, and COVID-19 Vaccination Uptake in the United States: A National Level Analysis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Measures
- Vaccination uptake rate: The county-level vaccine uptake rate was percent of adults (aged ≥ 18 years) who are fully vaccinated with any Food and Drug Administration (FDA) - authorized COVID-19 vaccine (i.e., have had the second dose of a two-dose vaccine series or one dose of a single-dose vaccine) based on the jurisdiction and county where the recipient resides [30].
- Demographic characteristics: Population demographic characteristics including gender, race, and ethnicity were aggregated to county-level. Specifically, the variables included percentages of the population who are female, Hispanic, non-Hispanic Asian, non-Hispanic Black, or non-Hispanic Native Hawaiian/Pacific Islander.
- Social determinants of health (SDOH): The SDOH variables include measures of poverty (i.e., percent of population living below federal poverty line) [31], high school education (i.e., percent of population with a high school degree or equivalent) [32], median household income [31], Gini Coefficient (i.e., a measure of income inequality with 0 reflecting complete equality and 1 reflecting complete inequality) [33,34], and percentage of population without health insurance [35].
- Social capital: The Social Capital Index was employed to estimate social capital. This index was developed by the Social Capital Index Project in the United States, which is composed of indicators in multilevel domains including family unity (e.g., births in past year to women who were unmarried and children living with a single parent), community health (e.g., number of nonreligious, nonprofit organizations), institutional health (e.g., voting rates in presidential elections, mail-back census response rates), and collective efficacy (e.g., violent crimes per 100,000 population) [14].
- Urbanization level: The urbanization level across counties was measured using the CDC’s National Center for Health Statistics (NCHS) Rural Classification Scheme for Counties [30], which is a six-level urban–rural classification scheme for US counties and county-equivalent entities. The six categories consist of: (1) large central metropolitan, (2) large fringe metropolitan, (3) medium metropolitan, (4) small metropolitan, (5) non-metropolitan, and (6) noncore. Specifically, large central metro counties are the counties in metropolitan statistical areas (MSA) of 1 million population that contain the entire population of the largest principal city of the MSA, are completely contained within the largest principal city of the MSA, or contain at least 250,000 residents of any principal city in the MSA. Large fringe metro counties are the counties in MSA of 1 million or more population that do not qualify as large central metro counties. Medium metro counties are the counties in MSA of 250,000–999,999 population. Small metro counties are counties in MSAs of less than 250,000 population. Nonmetropolitan counties are micropolitan counties in micropolitan statistical areas. Noncore counties are the counties that are not in micropolitan statistical areas. For data analysis, we further grouped categories 1 and 2 into “large urban” areas, categories 3 and 4 as “small urban” areas, and categories 5 and 6 as “rural” areas.
2.3. Data Analysis
3. Results
3.1. Bivariate Analysis
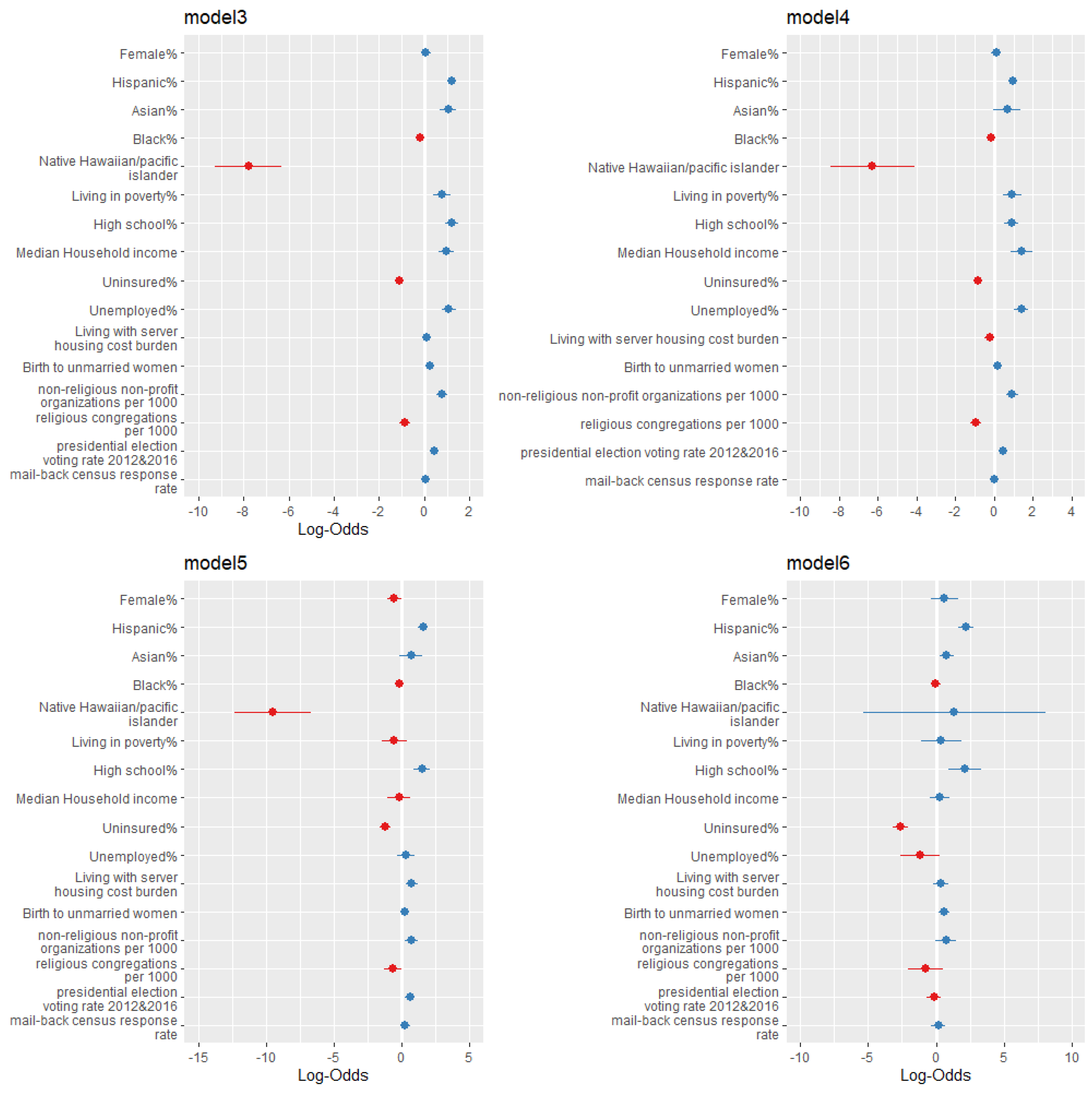
3.2. Regression Analysis
3.3. Stratification Analysis
4. Discussion
4.1. Interpretation of Results
4.2. Public Implications
4.3. Strenths and Limitations
4.4. Future Research and Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Category | Variables | Sources |
|---|---|---|
| Vaccination rate | % Adults fully vaccinated against COVID-19 (as of 7 April 2022) | CDC Vaccine Hesitancy for COVID-19: County and local estimates https://data.cdc.gov/Vaccinations/VaccineHesitancy-for-COVID-19-County-and-local-es/q9mh-h2tw, accessed on 7 April 2022 |
| Demographics | % Female % Hispanic % non-Hispanic Asian % non-Hispanic Black % non-Hispanic Native Hawaiian/Pacific Islander | US Census American Community Survey (ACS) 5-year estimate (2014–2018) https://www.census.gov/newsroom/press-releases/2019/acs-5-year.html, accessed on 15 September 2021 |
| Social Determinants of Health (SDOH) | % Living in Poverty % High School Education % Uninsured % Unemployed % Living with Severe Housing Cost Burden Median Household Income Gini Coefficient | AIDSVu 2018 County Social Determinants of Health. https://aidsvu.org/, accessed on 15 September 2021 |
| Social Capital | % Births to unmarried women % Women currently married % Children with single parent Non-religious non-profit organizations per 1000 Religious congregations per 1000 Presidential election voting rate 2012 and 2016 Mail-back census response rate Violent Crimes per 100000 | Social Capital Project: The Geography of Social Capital in America. https://www.lee.senate.gov/scp-index, accessed on 15 September 2021 |
| Urban/Rural | 2013 urbanization code | CDC National Center for Health Statistics (NCHS) Rural Classification Scheme for Counties (2013) https://www.cdc.gov/nchs/data_access/urban_rural.htm, accessed on 15 September 2021 |
| Potential Predictors | Percentage of Fully Vaccination | |
|---|---|---|
| Pearson r | p-Value | |
| Percentage of female | 0.047 | <0.01 |
| Percentage of non-Hispanic Black | −0.120 | <0.01 |
| Percentage of non-Hispanic Asian | 0.244 | <0.01 |
| Percentage of non-Hispanic Native Hawaiian/Pacific Islander | −0.100 | <0.01 |
| Percentage of Hispanic | 0.138 | <0.01 |
| Percentage of living in poverty | −0.234 | <0.01 |
| Percentage of high school education | 0.288 | <0.01 |
| Median household income | 0.375 | <0.01 |
| Gini Coefficient | −0.014 | 0.42 |
| Percentage of uninsured | −0.327 | <0.01 |
| Percentage of unemployed | 0.049 | <0.01 |
| Percentage of living with severe housing cost burden | 0.152 | <0.01 |
| Percentage of births to unmarried women | −0.062 | <0.01 |
| Percentage of women currently married | 0.001 | 0.96 |
| Percentage of children with single parent | −0.026 | 0.15 |
| Number of non-religious non-profit organizations per 1000 | 0.118 | <0.01 |
| Religious congregation per 1000 | −0.321 | <0.01 |
| Presidential election voting rate, 2012 and 2016 | 0.212 | <0.01 |
| Mail-back census response rate | 0.158 | <0.01 |
| 2013_urbanization_code | −0.274 | <0.01 |
| Violent crimes per 100,000 | 0.000 | 1.0 |
| Model 1 | Model 2 | Model 3 | |||||
|---|---|---|---|---|---|---|---|
| Independent Variables | OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Demographic background | % Female | 1.409 ** | (1.124, 1.767) | 1.245 * | (1.010, 1.534) | 1.063 | (0.853, 1.326) |
| % Hispanic | 1.392 *** | (1.227, 1.581) | 3.704 *** | (3.189, 4.302) | 3.410 *** | (2.929, 3.972) | |
| % non-Hispanic Asian | 22.611 *** | (16.065, 31.826) | 3.177 *** | (2.225, 4.536) | 2.865 *** | (2.026, 4.062) | |
| % non-Hispanic Black | 0.640 *** | (0.575, 0.713) | 0.924 | (0.818, 1.044) | 0.835 ** | (0.735, 0.950) | |
| % non-Hispanic Native Hawaiian/Pacific Islander | 0.00003 *** | (0.000006, 0.0002) | 0.0004 *** | (0.00008, 0.002) | 0.0004 *** | (0.00009, 0.002) | |
| % Living in poverty | 1.556 * | (1.094, 2.215) | 2.169 *** | (1.489, 3.161) | |||
| % High school education | 4.746 *** | (3.639, 6.189) | 3.391 *** | (2.511, 4.584) | |||
| Social Determinant of Health | Median household income | 2.908 *** | (2.120, 3.988) | 2.679 *** | (1.919, 3.743) | ||
| % Unemployed | 4.415 *** | (3.359, 5.803) | 2.947 *** | (2.175, 3.996) | |||
| % Uninsured | 0.306 *** | (0.259, 0.362) | 0.338 *** | (0.282, 0.405) | |||
| % Living with severe housing cost burden | 1.293 ** | (1.082, 1.544) | 1.123 | (0.927, 1.361) | |||
| Social Capital | % births to unmarried women | 1.251 *** | (1.130, 1.385) | ||||
| Non-religious non-profit organizations per 1000 | 2.176 *** | (1.741, 2.723) | |||||
| Religious congregations per 1000 | 0.417 *** | (0.325, 0.529) | |||||
| Presidential election voting rate 2012 and 2016 | 1.581 *** | (1.319, 1.894) | |||||
| Mail-back census response rate | 1.072 | (0.941, 1.221) | |||||
| Adjusted R Square | 0.145 | 0.333 | 0.396 | ||||
| Number of observations | 3142 | 3142 | 2897 | ||||
| Model 4 (Rural) | Model 5 (Small Urban) | Model 6 (Large Urban) | |||||
|---|---|---|---|---|---|---|---|
| Independent Variables | OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Demographic background | % Female | 1.121 | (0.867, 1.451) | 0.583 * | (0.349, 0.977) | 1.896 | (0.698, 5.222) |
| % Hispanic | 2.633 *** | (2.191, 3.165) | 4.798 *** | (3.391, 6.798) | 9.004 *** | (5.112, 15.908) | |
| % non-Hispanic Asian | 1.969 | (0.971, 3.991) | 1.963 | (0.864, 4.468) | 2.212 ** | (1.318, 3.734) | |
| % non-Hispanic Black | 0.878 | (0.743, 1.037) | 0.857 | (0.654, 1.123) | 0.965 | (0.669, 1.392) | |
| % non-Hispanic Native Hawaiian/Pacific Islander | 0.002 *** | (0.0002, 0.015) | 0.00007 *** | (0.000004, 0.001) | 3.878 | (0.005, 3212.368) | |
| Social Determinant of Health | % living in poverty | 2.505 *** | (1.549, 4.050) | 0.569 | (0.225, 1.437) | 1.463 | (0.336, 6.383) |
| % high school education | 2.439 *** | (1.683, 3.539) | 4.442 *** | (2.421, 8.159) | 8.249 *** | (2.524, 27.041) | |
| Median household income | 4.182 *** | (2.373, 7.386) | 0.821 | (0.357,1.887) | 1.910 | (0.622,2.765) | |
| % Unemployed | 4.110 *** | (2.856, 5.914) | 1.335 | (0.716, 2.503) | 0.309 | (0.073, 1.301) | |
| % Uninsured | 0.434 *** | (0.349, 0.539) | 0.298 *** | (0.199, 0.44) | 0.072 *** | (0.040, 0.129) | |
| % Living with severe housing cost burden | 0.797 | (0.624, 1.018) | 2.104 *** | (1.372, 3.228) | 1.463 | (0.846, 2.530) | |
| Social Capital | % births to unmarried women | 1.230 *** | (1.095, 1.382) | 1.246 | (0.971, 1.597) | 1.871 ** | (1.262, 2.776) |
| Non-religious non-profit organizations per 1000 | 2.551 *** | (1.909, 3.407) | 2.021 ** | (1.290, 3.179) | 2.121 | (0.991, 4.587) | |
| Religious congregations per 1000 | 0.396 *** | (0.296, 0.528) | 0.521 * | (0.275,0.985) | 0.470 | (0.133,1.656) | |
| Presidential election voting rate 2012 and 2016 | 1.591 *** | (1.261, 2.009) | 1.810 *** | (1.283, 2.554) | 0.859 | (0.499, 1.478) | |
| Mail-back census response rate | 1.031 | (0.889, 1.195) | 1.271 | (0.892, 1.812) | 1.190 | (0.706, 2.003) | |
| Adjusted R Square | 0.285 | 0.442 | 0.569 | ||||
| Number of observations | 1762 | 707 | 428 | ||||

References
- Centers for Disease Control and Prevention. COVID Data Tracker. 2022. Available online: https://covid.cdc.gov/covid-data-tracker/#datatracker-home (accessed on 7 April 2022).
- Piret, J.; Boivin, G. Pandemics throughout history. Front. Microbiol. 2021, 11, 3594. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. COVID-19. 2021. Available online: https://www.cdc.gov/coronavirus/2019-nCoV/index.html (accessed on 9 September 2021).
- Gee, J.; Marquez, P.; Su, J.; Calvert, G.M.; Liu, R.; Myers, T.; Nair, N.; Martin, S.; Clark, T.; Markowitz, L.; et al. First month of COVID-19 vaccine safety monitoring—United States, December 14, 2020–January 13, 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 283–288. [Google Scholar] [CrossRef] [PubMed]
- CDC. COVID Data Tracker. Secondary COVID Data Tracker: COVID-19 Vaccinations in the United States. 2022. Available online: https://covid.cdc.gov/covid-data-tracker/#vaccinations_vacc-people-onedose-pop-5yr (accessed on 7 April 2022).
- Malik, A.; McFadden, S.; Elharake, J.; Omer, S. Determinants of COVID-19 vaccine acceptance in the US. EClinicalMedicine 2020, 26, 100495. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.H.; Joshi, A.D.; Drew, D.A.; Merino, J.; Ma, W.; Lo, C.; Kwon, S.; Wang, K.; Graham, M.S.; Polidori, L.; et al. Racial and ethnic differences in COVID-19 vaccine hesitancy and uptake. MedRxiv 2021. [Google Scholar]
- CDC. Disparities in COVID-19 Vaccination Coverage Between Urban and Rural Counties–United States, December 14, 2020–April 10, 2021. Secondary Disparities in COVID-19 Vaccination Coverage Between Urban and Rural Counties–United States, December 14, 2020–April 10, 2021. 2021. Available online: https://www.cdc.gov/mmwr/volumes/70/wr/mm7020e3.htm (accessed on 11 April 2022).
- Barry, V.; Dasgupta, S.; Weller, D.L.; Kriss, J.L.; Cadwell, B.L.; Rose, C.; Pingali, C.; Musial, T.; Sharpe, J.D.; Flores, S.A.; et al. Patterns in COVID-19 Vaccination Coverage, by Social Vulnerability and Urbanicity—United States, December 14, 2020–May 1, 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 818. [Google Scholar] [CrossRef]
- Whiteman, A.; Wang, A.; McCain, K.; Gunnels, B.; Toblin, R.; Lee, J.T.; Bridges, C.; Reynolds, L.; Murthy, B.P.; Qualters, J.; et al. Demographic and social factors associated with COVID-19 vaccination initiation among adults aged ≥ 65 years—United States, December 14, 2020–April 10, 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 725. [Google Scholar] [CrossRef]
- Adler, P.S.; Kwon, S.-W. Social capital: Prospects for a new concept. Acad. Manag. Rev. 2002, 27, 17–40. [Google Scholar] [CrossRef] [Green Version]
- Woolcock, M.; Narayan, D. Social capital: Implications for development theory, research, and policy. World Bank Res. Obs. 2000, 15, 225–249. [Google Scholar] [CrossRef] [Green Version]
- Moore, S.; Carpiano, R.M. Introduction to the special issue on “Social capital and health: What have we learned in the last 20 years and where do we go from here?”. Soc. Sci. Med. 2020, 257, 113014. [Google Scholar] [CrossRef]
- U.S. Congress, Joint Economic Committee. Social Capital Project: The Geography of Social Capital in America. Secondary Social Capital Project: The Geography of Social Capital in America. 2018. Available online: https://www.lee.senate.gov/services/files/DA64FDB7-3B2E-40D4-B9E3-07001B81EC31 (accessed on 7 April 2022).
- Hotchkiss, J.L. Decennial census return rates: The role of social capital. Cent. Econ. Studies. 2017. Available online: https://www2.census.gov/ces/wp/2017/CES-WP-17–39.pdf (accessed on 7 April 2022). [CrossRef]
- Ehsan, A.; Klaas, H.S.; Bastianen, A.; Spini, D. Social capital and health: A systematic review of systematic reviews. SSM-Popul. Health 2019, 8, 100425. [Google Scholar] [CrossRef] [PubMed]
- Pridmore, P.; Thomas, L.; Havemann, K.; Sapag, J.; Wood, L. Social capital and healthy urbanization in a globalized world. J. Urban Health 2007, 84, 130–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flora, C.B.; Flora, J.L. The past and future: Social contract, social policy and social capital. Increasing Underst. Public Probl. Policies 1995, 53–64. [Google Scholar]
- Debertin, D.L. A Comparrison of Social Capital in Rural and Urban Settings. Secondary A Comparrison of Social Capital in Rural and Urban Settings. Available online: https://www.uky.edu/~deberti/socsaea.htm (accessed on 10 October 2021).
- Porter, J.R.; Howell, F.M. Geographical Sociology: Theoretical Foundations and Methodological Applications in the Sociology of Location; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Paranagamage, P.; Austin, S.; Price, A.; Khandokar, F. Social capital in action in urban environments: An intersection of theory, research and practice literature. J. Urban. 2010, 3, 231–252. [Google Scholar] [CrossRef]
- Rönnerstrand, B. Social capital and immunization against the 2009 A (H1N1) pandemic in the American States. Public Health 2014, 128, 709–715. [Google Scholar] [CrossRef] [PubMed]
- Rönnerstrand, B. Contextual generalized trust and immunization against the 2009 A (H1N1) pandemic in the American states: A multilevel approach. SSM-Popul. Health 2016, 2, 632–639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- LaVeist, T.A.; Isaac, L.A.; Williams, K.P. Mistrust of health care organizations is associated with underutilization of health services. Health Serv. Res. 2009, 44, 2093–2105. [Google Scholar] [CrossRef]
- United States Census Bureau. US Census American Community Survey (ACS) 5-Year Estimate (2014–2018). Secondary US Census American Community Survey (ACS) 5-Year Estimate (2014–2018). 2019. Available online: https://www.census.gov/newsroom/press-releases/2019/acs-5-year.html (accessed on 15 September 2021).
- French, J.; Deshpande, S.; Evans, W.; Obregon, R. Key guidelines in developing a pre-emptive COVID-19 vaccination uptake promotion strategy. Int. J. Environ. Res. Public Health 2020, 17, 5893. [Google Scholar] [CrossRef]
- CDC. CDC Vaccine Hesitancy for COVID-19: County and Local Estimates. Secondary CDC Vaccine Hesitancy for COVID-19: County and Local Estimates. 2021. Available online: https://data.cdc.gov/Vaccinations/Vaccine-Hesitancy-for-COVID-19-County-and-local-es/q9mh-h2tw (accessed on 15 September 2021).
- AIDSVu. AIDSVu 2018 County Social Determinants of Health. Secondary AIDSVu 2018 County Social Determinants of Health. 2018. Available online: https://aidsvu.org/ (accessed on 15 September 2021).
- CDC. CDC National Center for Health Statistics (NCHS) Rural Classification Scheme for Counties. Secondary CDC National Center for Health Statistics (NCHS) Rural Classification Scheme for Counties (2013). 2013. Available online: https://www.cdc.gov/nchs/data_access/urban_rural.htm (accessed on 8 August 2021).
- Scobie, H.M.; Johnson, A.G.; Suthar, A.B.; Severson, R.; Alden, N.B.; Balter, S.; Bertolino, D.; Blythe, D.; Brady, S.; Cadwell, B.; et al. Monitoring incidence of COVID-19 cases, hospitalizations, and deaths, by vaccination status—13 US jurisdictions, April 4–July 17, 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 1284. [Google Scholar] [CrossRef]
- United States Census Bureau. Small Area Income and Poverty Estimates. Table 1: 2916 Poverty and Median Income Estimates: Counties. 2016. Available online: https://www.census.gov/programs-surveys/saipe.html (accessed on 5 June 2021).
- United States Census Bureau. American Community Survey 5-Year Estimates, 2016. Table B15003: Educational Attainment for the Population 25 Years and Over: Counties. 2016. Available online: https://data.census.gov/cedsci/table?q=B15003%3A%20EDUCATIONAL%20ATTAINMENT%20FOR%20THE%20POPULATION%2025%20YEARS%20AND%20OVER&d=ACS%205-Year%20Estimates%20Detailed%20Tables&tid=ACSDT5Y2020.B15003 (accessed on 5 June 2021).
- Gini, C. On the measure of concentration with special reference to income and statistics. Colo. Coll. Publ. Gen. Ser. 1936, 208, 73–79. [Google Scholar]
- United States Census Bureau. American Community Survey 5-Year Estimates, 2016. Table B19083: Gini Index of Income Inequality. 2016. Available online: https://data.census.gov/cedsci/table?q=B19083%3A%20GINI%20INDEX%20OF%20INCOME%20INEQUALITY&tid=ACSDT5Y2020.B19083 (accessed on 5 June 2021).
- United States Census Bureau. Small Area Health Insurance Estimates, 2016: Health Insurance Coverage Status by Age, Race, Hispanic Origin, Sex and Income for Counties and States. 2016. Available online: https://www.census.gov/programs-surveys/sahie.html (accessed on 5 June 2021).
- A Tale of Two Crises: Addressing COVID-19 Vaccine Hesitancy as Promoting Racial Justice. In Hec Forum; Springer: Dordrecht, The Netherlands, 2021.
- Ebrahimi, O.V.; Johnson, M.S.; Ebling, S.; Amundsen, O.M.; Halsøy, Ø.; Hoffart, A.; Skjerdingstad, N.; Johnson, S.U. Risk, trust, and flawed assumptions: Vaccine hesitancy during the COVID-19 pandemic. Front. Public Health 2021, 9, 849. [Google Scholar] [CrossRef] [PubMed]
- Gaffney, A.W.; Woolhandler, S.; Himmelstein, D.U. Association of Uninsurance and VA Coverage with the Uptake and Equity of COVID-19 Vaccination: January–March 2021. J. Gen. Intern. Med. 2022, 37, 1008–1011. [Google Scholar] [CrossRef] [PubMed]
- Tsai, Y.; Lindley, M.C.; Zhou, F.; Stokley, S. Urban-Rural disparities in vaccination service use among low-income adolescents. J. Adolesc. Health 2021, 69, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Dubé, E.; Laberge, C.; Guay, M.; Bramadat, P.; Roy, R.; Bettinger, J.A. Vaccine hesitancy: An overview. Hum. Vaccines Immunother. 2013, 9, 1763–1773. [Google Scholar] [CrossRef]
- Roy, B.; LeBlanc, M. COVID-19 Vaccine Incentives Memorandum. National Governor’s Association. 2021. Available online: https://www.nga.org/wp-content/uploads/2021/10/Vaccine-Incentives-Memo-10.19.21.pdf (accessed on 7 April 2022).
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qiao, S.; Li, Z.; Zhang, J.; Sun, X.; Garrett, C.; Li, X. Social Capital, Urbanization Level, and COVID-19 Vaccination Uptake in the United States: A National Level Analysis. Vaccines 2022, 10, 625. https://doi.org/10.3390/vaccines10040625
Qiao S, Li Z, Zhang J, Sun X, Garrett C, Li X. Social Capital, Urbanization Level, and COVID-19 Vaccination Uptake in the United States: A National Level Analysis. Vaccines. 2022; 10(4):625. https://doi.org/10.3390/vaccines10040625
Chicago/Turabian StyleQiao, Shan, Zhenlong Li, Jiajia Zhang, Xiaowen Sun, Camryn Garrett, and Xiaoming Li. 2022. "Social Capital, Urbanization Level, and COVID-19 Vaccination Uptake in the United States: A National Level Analysis" Vaccines 10, no. 4: 625. https://doi.org/10.3390/vaccines10040625