
Validation of the GSP®/DELFIA® Anti-SARS-CoV-2 IgG Kit Using Dried Blood Samples for High-Throughput Serosurveillance and Standardized Quantitative Measurement of Anti-Spike S1 IgG Antibody Responses Post-Vaccination

 ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Anti-S1 Spike IgG Immunoassay
2.2. Assay Performance Characteristics
2.3. Patient Enrolled and Sample Collection
2.4. Statistical Analysis
3. Results
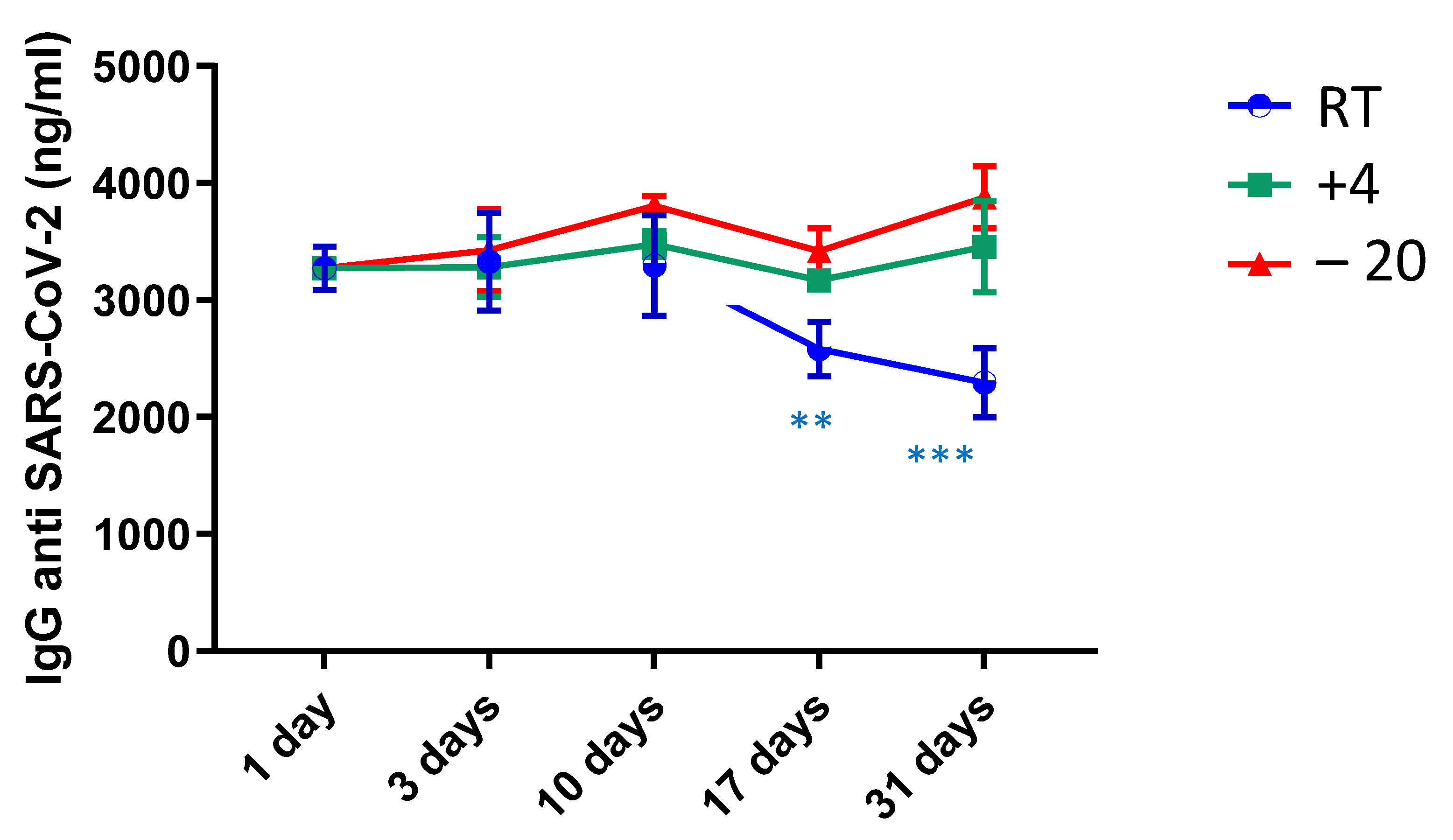
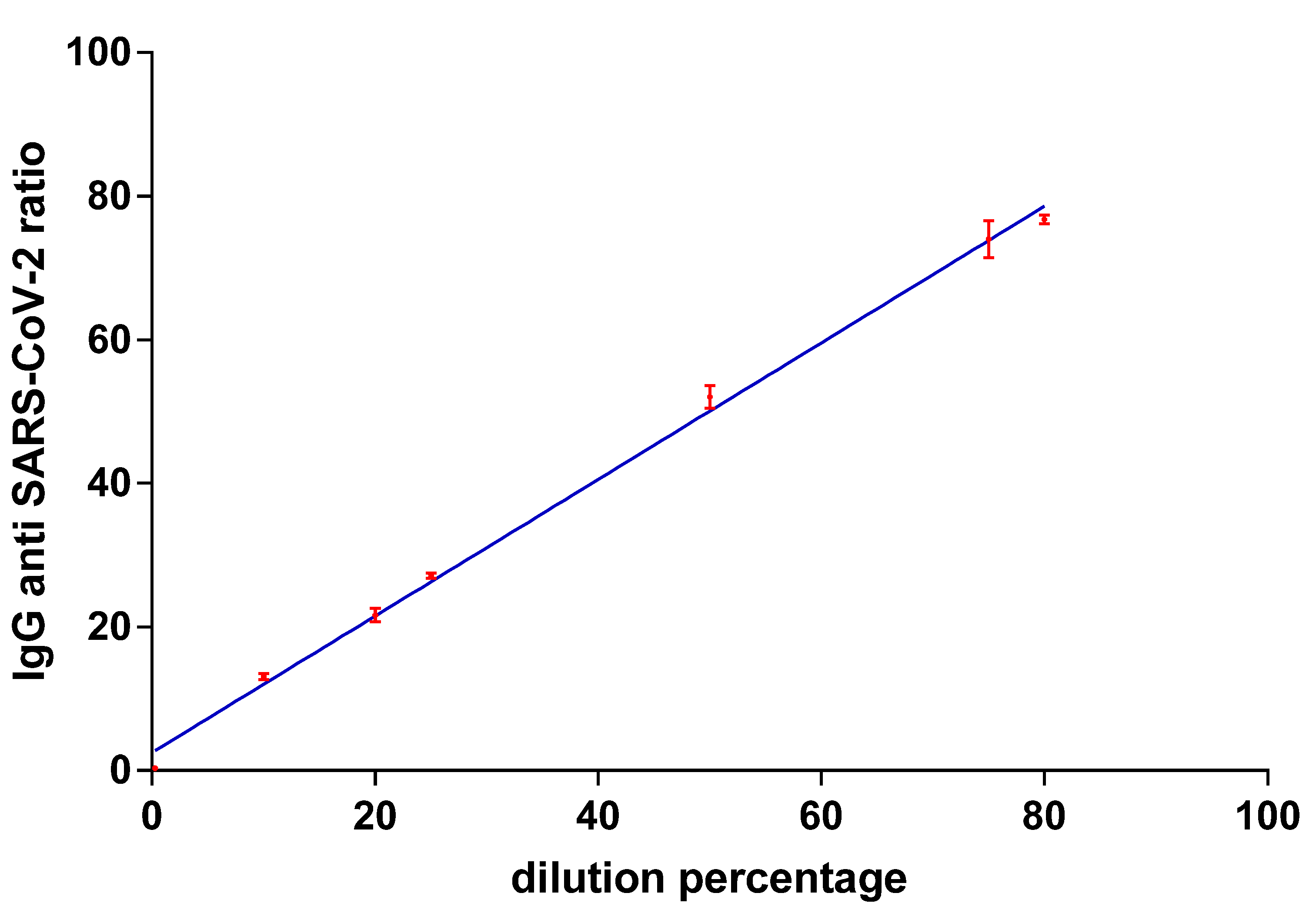
3.1. Linearity Repeatability and Accuracy and Stability over Time
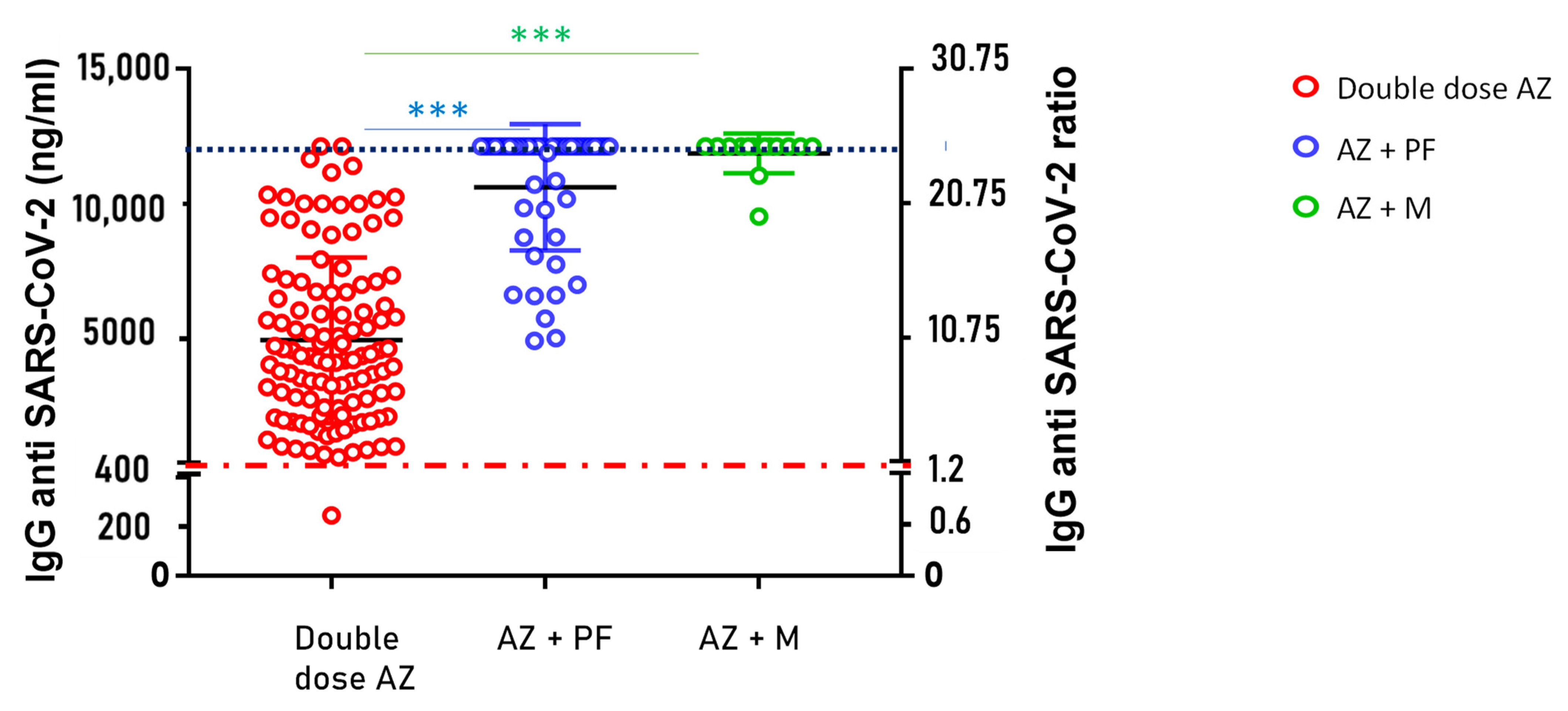
3.2. Evaluation of IgG Anti-SARS-CoV-2 Levels in Subjects Undergoing Heterologous Vaccination
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dong, Y.; Dai, T.; Wang, B.; Zhang, L.; Zeng, L.-H.; Huang, J.; Yan, H.; Zhang, L.; Zhou, F. The Way of SARS-CoV-2 Vaccine Development: Success and Challenges. Signal. Transduct. Target Ther. 2021, 6, 387. [Google Scholar] [CrossRef]
- Lauer, S.A.; Grantz, K.H.; Bi, Q.; Jones, F.K.; Zheng, Q.; Meredith, H.R.; Azman, A.S.; Reich, N.G.; Lessler, J. The Incubation Period of Coronavirus Disease 2019 (COVID-19) From Publicly Reported Confirmed Cases: Estimation and Application. Ann. Intern. Med. 2020, 172, 577–582. [Google Scholar] [CrossRef] [Green Version]
- Meyers, E.; Heytens, S.; Formukong, A.; Vercruysse, H.; De Sutter, A.; Geens, T.; Hofkens, K.; Janssens, H.; Nys, E.; Padalko, E.; et al. Comparison of Dried Blood Spots and Venous Blood for the Detection of SARS-CoV-2 Antibodies in a Population of Nursing Home Residents. Microbiol. Spectr. 2021, 9, e0017821. [Google Scholar] [CrossRef]
- Rossi, C.; Lanuti, P.; Cicalini, I.; De Bellis, D.; Pierdomenico, L.; Del Boccio, P.; Zucchelli, M.; Natale, L.; Sinjari, B.; Catitti, G.; et al. BNT162b2 MRNA Vaccination Leads to Long-Term Protection from COVID-19 Disease. Vaccines 2021, 9, 1164. [Google Scholar] [CrossRef]
- Lanuti, P.; Rossi, C.; Cicalini, I.; Pierdomenico, L.; Damiani, V.; Semeraro, D.; Verrocchio, S.; Del Boccio, P.; Evangelista, A.; Sarra, A.; et al. Picture of the Favourable Immune Profile Induced by Anti-SARS-CoV-2 Vaccination. Biomedicines 2021, 9, 1035. [Google Scholar] [CrossRef] [PubMed]
- Cicalini, I.; Rossi, C.; Natale, L.; Cufaro, M.C.; Catitti, G.; Vespa, S.; De Bellis, D.; Iannetti, G.; Lanuti, P.; Bucci, I.; et al. Passive Immunity to SARS-CoV-2 at Birth Induced by Vaccination in the First Trimester of Pregnancy. Int. J. Environ. Res. Public Health 2021, 18, 12789. [Google Scholar] [CrossRef] [PubMed]
- Younes, N.; Al-Sadeq, D.W.; Al-Jighefee, H.; Younes, S.; Al-Jamal, O.; Daas, H.I.; Yassine, H.M.; Nasrallah, G.K. Challenges in Laboratory Diagnosis of the Novel Coronavirus SARS-CoV-2. Viruses 2020, 12, 582. [Google Scholar] [CrossRef] [PubMed]
- Theel, E.S. Performance Characteristics of High-Throughput Serologic Assays for Severe Acute Respiratory Syndrome Coronavirus 2 with Food and Drug Administration Emergency Use Authorization: A Review. Clin. Lab. Med. 2022, 42, 15–29. [Google Scholar] [CrossRef] [PubMed]
- Amanna, I.J.; Slifka, M.K.; Crotty, S. Immunity and Immunological Memory Following Smallpox Vaccination. Immunol. Rev. 2006, 211, 320–337. [Google Scholar] [CrossRef] [PubMed]
- Earle, K.A.; Ambrosino, D.M.; Fiore-Gartland, A.; Goldblatt, D.; Gilbert, P.B.; Siber, G.R.; Dull, P.; Plotkin, S.A. Evidence for Antibody as a Protective Correlate for COVID-19 Vaccines. Vaccine 2021, 39, 4423–4428. [Google Scholar] [CrossRef] [PubMed]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing Antibody Levels Are Highly Predictive of Immune Protection from Symptomatic SARS-CoV-2 Infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.; Rosadas, C.; Katsanovskaja, K.; Weber, I.D.; Shute, J.; Ijaz, S.; Marchesin, F.; McClure, E.; Elias, S.; Flower, B.; et al. Simple, Sensitive, Specific Self-Sampling Assay Secures SARS-CoV-2 Antibody Signals in Sero-Prevalence and Post-Vaccine Studies. Sci. Rep. 2022, 12, 1885. [Google Scholar] [CrossRef] [PubMed]
- Zava, T.T.; Zava, D.T. Validation of Dried Blood Spot Sample Modifications to Two Commercially Available COVID-19 IgG Antibody Immunoassays. Bioanalysis 2021, 13, 13–28. [Google Scholar] [CrossRef]
- Morley, G.L.; Taylor, S.; Jossi, S.; Perez-Toledo, M.; Faustini, S.E.; Marcial-Juarez, E.; Shields, A.M.; Goodall, M.; Allen, J.D.; Watanabe, Y.; et al. Sensitive Detection of SARS-CoV-2-Specific Antibodies in Dried Blood Spot Samples. Emerg. Infect. Dis. 2020, 26, 2970–2973. [Google Scholar] [CrossRef] [PubMed]
- Mulchandani, R.; Brown, B.; Brooks, T.; Semper, A.; Machin, N.; Linley, E.; Borrow, R.; Wyllie, D.; EDSAB-HOME Study Investigators. Use of Dried Blood Spot Samples for SARS-CoV-2 Antibody Detection Using the Roche Elecsys ® High Throughput Immunoassay. J. Clin. Virol. 2021, 136, 104739. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Concentration Range (ng/mL) | Calibration Function Y = b1(±SD) x + b0(±SD) n = 5 | R2 (±SD) n = 5 |
|---|---|---|
| 0–000 | y = 0.0028(±0.00027) x + 0.048(±0.04) | 0.99 (± 0.004) |
| 500–10,000 | y = 0.002(±0.00016) x + 0.75(±0.17) | 0.99 (± 0.004) |
| Intra-Assay | Inter-Assay | Accuracy | ||||||
|---|---|---|---|---|---|---|---|---|
| QC Levels (ng/mL) | Measured Concentration (ng/mL) n = 3 | SD n = 3 | CV% | Measured Concentration (ng/mL) n = 15 | SD n = 15 | CV% | Bias% n = 5 | SD (ng/mL) n = 5 |
| 100 | 118.5 | 3.57 | 3.01 | 141.4 | 21.0 | 14.8 | 41.28 | ±12.08 |
| 200 | 218.6 | 7.14 | 3.26 | 190.3 | 22.8 | 12.0 | −3.94 | ±2.48 |
| 300 | 298.3 | 8.98 | 3.01 | 288.6 | 38.0 | 13.2 | −3.83 | ±4.37 |
| 500 | 568.6 | 34.1 | 5.99 | 453.6 | 60.1 | 13.2 | −7.44 | ±6.44 |
| 1000 | 1097.1 | 75.0 | 6.83 | 1015.7 | 96.7 | 9.5 | 1.55 | ±1.51 |
| 3000 | 3193.3 | 42.5 | 1.3 | 3472.0 | 417.2 | 12.0 | 20.72 | ±4.48 |
| 10,000 | 10028.3 | 360.9 | 3.6 | 9271.7 | 732.3 | 7.9 | −1.64 | ±1.54 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cicalini, I.; Del Boccio, P.; Zucchelli, M.; Rossi, C.; Natale, L.; Demattia, G.; De Bellis, D.; Damiani, V.; Tommolini, M.L.; Pizzinato, E.; et al. Validation of the GSP®/DELFIA® Anti-SARS-CoV-2 IgG Kit Using Dried Blood Samples for High-Throughput Serosurveillance and Standardized Quantitative Measurement of Anti-Spike S1 IgG Antibody Responses Post-Vaccination. Vaccines 2022, 10, 514. https://doi.org/10.3390/vaccines10040514
Cicalini I, Del Boccio P, Zucchelli M, Rossi C, Natale L, Demattia G, De Bellis D, Damiani V, Tommolini ML, Pizzinato E, et al. Validation of the GSP®/DELFIA® Anti-SARS-CoV-2 IgG Kit Using Dried Blood Samples for High-Throughput Serosurveillance and Standardized Quantitative Measurement of Anti-Spike S1 IgG Antibody Responses Post-Vaccination. Vaccines. 2022; 10(4):514. https://doi.org/10.3390/vaccines10040514
Chicago/Turabian StyleCicalini, Ilaria, Piero Del Boccio, Mirco Zucchelli, Claudia Rossi, Luca Natale, Gianmaria Demattia, Domenico De Bellis, Verena Damiani, Maria Lucia Tommolini, Erika Pizzinato, and et al. 2022. "Validation of the GSP®/DELFIA® Anti-SARS-CoV-2 IgG Kit Using Dried Blood Samples for High-Throughput Serosurveillance and Standardized Quantitative Measurement of Anti-Spike S1 IgG Antibody Responses Post-Vaccination" Vaccines 10, no. 4: 514. https://doi.org/10.3390/vaccines10040514