
Evaluation of Two-Month Antibody Levels after Heterologous ChAdOx1-S/BNT162b2 Vaccination Compared to Homologous ChAdOx1-S or BNT162b2 Vaccination

 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Recruitment and Study Cohort Characteristics
2.2. Determination of Antibody Levels
2.3. Additional Testing for Asymptomatic SARS-CoV-2 Infection
2.4. Statistical Analysis
3. Results
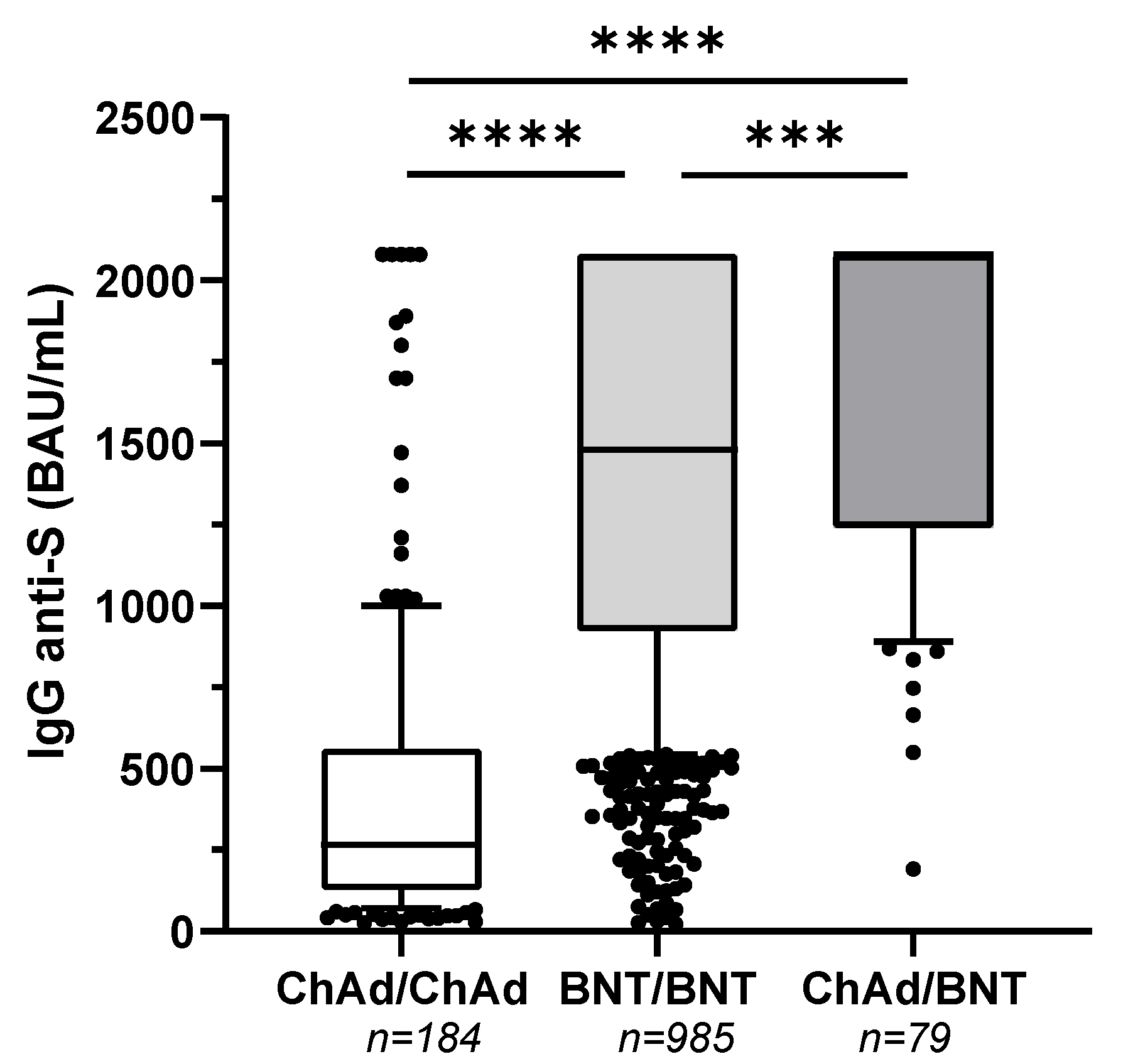
3.1. SARS-CoV-2 TrimericS IgG Antibody Levels Two Months after Vaccination
3.2. SARS-CoV-2 Antigen and Anti-N Antibodies Testing Results
3.3. Factors Affecting IgG Response
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- COVID-19 Vaccines. Available online: www.aifa.gov.it/en/vaccini-covid-19 (accessed on 11 February 2022).
- Heterologous Primary and Booster COVID-19 Vaccination. Evidence Based Regulatory Considerations. Available online: www.ema.europa.eu/en/documents/report/heterologous-primary-booster-covid-19-vaccination-evidence-based-regulatory-considerations_en.pdf (accessed on 11 February 2022).
- Stuart, A.S.V.; Shaw, R.H.; Liu, X.; Greenland, M.; Aley, P.K.; Andrews, N.J.; Cameron, J.C.; Charlton, S.; Clutterbuck, E.A.; Collins, A.M.; et al. Immunogenicity, safety, and reactogenicity of heterologous COVID-19 primary vaccination incorporating mRNA, viral-vector, and protein-adjuvant vaccines in the UK (Com-COV2): A single-blind, randomised, phase 2, non-inferiority trial. Lancet 2022, 399, 36–49. [Google Scholar] [CrossRef]
- Liu, X.; Shaw, R.H.; Stuart, A.S.; Greenland, M.; Aley, P.K.; Andrews, N.J.; Cameron, J.C.; Charlton, S.; Clutterbuck, E.A.; Collins, A.M.; et al. Safety and immunogenicity of heterologous versus homologous prime-boost schedules with an adenoviral vectored and mRNA COVID-19 vaccine (Com-COV): A single-blind, randomised, non-inferiority trial. Lancet 2021, 398, 856–869. [Google Scholar] [CrossRef]
- Normark, J.; Vikström, L.; Gwon, Y.-D.; Persson, I.-L.; Edin, A.; Björsell, T.; Dernstedt, A.; Christ, W.; Tevell, S.; Evander, M.; et al. Heterologous ChAdOx1 nCoV-19 and mRNA-1273 Vaccination. N. Engl. J. Med. 2021, 385, 1049–1051. [Google Scholar] [CrossRef] [PubMed]
- LIAISON® SARS-CoV-2 TrimericS IgG Assay A Quantitative Assay for Immune Status Monitoring with an Accurate Correlation of Neutralizing IgG Antibodies. Available online: https://www.diasorin.com/sites/default/files/allegati_prodotti/liaisonr_sars-cov-2_trimerics_igg_assay_m0870004408_a_lr_0.pdf (accessed on 11 February 2022).
- Swadźba, J.; Anyszek, T.; Panek, A.; Martin, E. Anti-Spike SARS-CoV-2 IgG Assessment with a Commercial Assay during a 4-Month Course after COVID-19 Vaccination. Vaccines 2021, 9, 1367. Available online: https://www.mdpi.com/2076-393X/9/11/1367 (accessed on 11 February 2022). [CrossRef] [PubMed]
- De Santi, M.; Diotallevi, A.; Brandi, G. Seroprevalence of Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) infection in an Italian cohort in Marche Region, Italy. Acta Biomed. 2021, 92, e2021070. [Google Scholar] [PubMed]
- Borobia, A.M.; Carcas, A.J.; Pérez-Olmeda, M.; Castaño, L.; Bertran, M.J.; García-Pérez, J.; Campins, M.; Portolés, A.; González-Pérez, M.; Morales, M.T.G.; et al. Immunogenicity and reactogenicity of BNT162b2 booster in ChAdOx1-S-primed participants (CombiVacS): A multicentre, open-label, randomised, controlled, phase 2 trial. Lancet 2021, 398, 121–130. Available online: https://www.sciencedirect.com/science/article/pii/S0140673621014203 (accessed on 11 February 2022). [CrossRef]
- He, Q.; Mao, Q.; An, C.; Zhang, J.; Gao, F.; Bian, L.; Li, C.; Liang, Z.; Xu, M.; Wang, J. Heterologous prime-boost: Breaking the protective immune response bottleneck of COVID-19 vaccine candidates. Emerg. Microbes Infect. 2021, 10, 629–637. [Google Scholar] [CrossRef] [PubMed]
- Spencer, A.J.; McKay, P.F.; Belij-Rammerstorfer, S.; Ulaszewska, M.; Bissett, C.D.; Hu, K.; Samnuan, K.; Blakney, A.K.; Wright, D.; Sharpe, H.R.; et al. Heterologous vaccination regimens with self-amplifying RNA and adenoviral COVID vaccines induce robust immune responses in mice. Nat. Commun. 2021, 12, 2893. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, T.; Klemis, V.; Schub, D.; Mihm, J.; Hielscher, F.; Marx, S.; Abu-Omar, A.; Ziegler, L.; Guckelmus, C.; Urschel, R.; et al. Immunogenicity and reactogenicity of heterologous ChAdOx1 nCoV-19/mRNA vaccination. Nat. Med. 2021, 27, 1530–1535. [Google Scholar] [CrossRef] [PubMed]
- Barros-Martins, J.; Hammerschmidt, S.I.; Cossmann, A.; Odak, I.; Stankov, M.V.; Morillas Ramos, G.; Dopfer-Jablonka, A.; Heidemann, A.; Ritter, C.; Friedrichsen, M.; et al. Immune responses against SARS-CoV-2 variants after heterologous and homologous ChAdOx1 nCoV-19/BNT162b2 vaccination. Nat. Med. 2021, 27, 1525–1529. [Google Scholar] [CrossRef] [PubMed]
- Terpos, E.; Trougakos, I.P.; Apostolakou, F.; Charitaki, I.; Sklirou, A.D.; Mavrianou, N.; Papanagnou, E.-D.; Liacos, C.-I.; Gumeni, S.; Rentziou, G.; et al. Age-dependent and gender-dependent antibody responses against SARS-CoV-2 in health workers and octogenarians after vaccination with the BNT162b2 mRNA vaccine. Am. J. Hematol. 2021, 96, E257–E259. Available online: https://onlinelibrary.wiley.com/doi/abs/10.1002/ajh.26185 (accessed on 11 February 2022). [CrossRef] [PubMed]
- Müller, L.; Andrée, M.; Moskorz, W.; Drexler, I.; Walotka, L.; Grothmann, R.; Ptok, J.; Hillebrandt, J.; Ritchie, A.; Rabl, D.; et al. Age-dependent Immune Response to the Biontech/Pfizer BNT162b2 Coronavirus Disease 2019 Vaccination. Clin. Infect. Dis. 2021, 73, 2065–2072. [Google Scholar] [CrossRef] [PubMed]
- Bertoletti, A.; Le Bert, N.; Qui, M.; Tan, A.T. SARS-CoV-2-specific T cells in infection and vaccination. Cell. Mol. Immunol. 2021, 18, 2307–2312. [Google Scholar] [CrossRef] [PubMed]
- Deming, M.E.; Lyke, K.E. A ‘mix and match’ approach to SARS-CoV-2 vaccination. Nat. Med. 2021, 27, 1510–1511. [Google Scholar] [CrossRef] [PubMed]
- Thakkar, A.; Gonzalez-Lugo, J.D.; Goradia, N.; Gali, R.; Shapiro, L.C.; Pradhan, K.; Rahman, S.; Kim, S.Y.; Ko, B.; Sica, R.A.; et al. Seroconversion rates following COVID-19 vaccination among patients with cancer. Cancer Cell 2021, 39, 1081–1090.e2. Available online: https://www.sciencedirect.com/science/article/pii/S1535610821002853 (accessed on 11 February 2022).


{kind=link}
| Characteristic | All | ChAd/ChAd | BNT/BNT | ChAd/BNT | |
|---|---|---|---|---|---|
| n = 1248 | n = 184 (15%) | n = 985 (79%) | n = 79 (6%) | ||
| Gender | Male | 412 (33%) | 83 (45%) | 292 (30%) | 37 (47%) |
| Female | 836 (67%) | 101 (55%) | 693 (70%) | 42 (53%) | |
| Age | Years (median, IQR) | 52 (44–59) | 55 (48–61) | 51 (43–58) | 52 (46–57) |
| Interval between prime and boost dose | Days (median, IQR) | 74 (74–74) | 25 (21–35) | 83 (83–83) | |
| Interval between boost dose and antibody titer test | Days (median, IQR) | 61 (57–65) | 60 (60–60) | 61 (55–67) | |
| Factor | n = 175 (62%) | n = 32 (11%) | n = 77 (27%) | 3p Value |
|---|---|---|---|---|
| Vaccine schedule | ChAd/ChAd; | BNT/BNT | ChAd/BNT | <0.0001 |
| Sex (Male) | 81 (46%) | 11 (34%) | 37 (48%) | 0.965 |
| 1 Age | 55 (48–61) | 52 (43–60) | 52 (46–57) | 0.167 |
| 1 BMI | 23.84 (21.8–27.08) | 24.15 (21.65–27.15) | 23.84 (21.99–26.12) | 0.631 |
| Smoking | 18 (10%) | 1 (3%) | 15 (19%) | 0.148 |
| Diabetes | 3 (2%) | 5 (16%) | 1 (1%) | 0.411 |
| Cardiovascular diseases | 7 (4%) | 3 (9%) | 2 (3%) | 0.127 |
| Respiratory tract diseases | 2 (1%) | 3 (9%) | 0 (0%) | 0.747 |
| COVID-19 diagnosis | 4 (2%) | 0 (0%) | 4 (5%) | 0.264 |
| 2 Vaccine side effects | 66 (38%) | 12 (38%) | 36 (47%) | 0.697 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barocci, S.; Orlandi, C.; Diotallevi, A.; Buffi, G.; Ceccarelli, M.; Vandini, D.; Carlotti, E.; Galluzzi, L.; Rocchi, M.B.L.; Magnani, M.; et al. Evaluation of Two-Month Antibody Levels after Heterologous ChAdOx1-S/BNT162b2 Vaccination Compared to Homologous ChAdOx1-S or BNT162b2 Vaccination. Vaccines 2022, 10, 491. https://doi.org/10.3390/vaccines10040491
Barocci S, Orlandi C, Diotallevi A, Buffi G, Ceccarelli M, Vandini D, Carlotti E, Galluzzi L, Rocchi MBL, Magnani M, et al. Evaluation of Two-Month Antibody Levels after Heterologous ChAdOx1-S/BNT162b2 Vaccination Compared to Homologous ChAdOx1-S or BNT162b2 Vaccination. Vaccines. 2022; 10(4):491. https://doi.org/10.3390/vaccines10040491
Chicago/Turabian StyleBarocci, Simone, Chiara Orlandi, Aurora Diotallevi, Gloria Buffi, Marcello Ceccarelli, Daniela Vandini, Eugenio Carlotti, Luca Galluzzi, Marco Bruno Luigi Rocchi, Mauro Magnani, and et al. 2022. "Evaluation of Two-Month Antibody Levels after Heterologous ChAdOx1-S/BNT162b2 Vaccination Compared to Homologous ChAdOx1-S or BNT162b2 Vaccination" Vaccines 10, no. 4: 491. https://doi.org/10.3390/vaccines10040491