
Knowledge and Attitudes Concerning Herpes Zoster among People with COPD: An Interventional Survey Study

Abstract
:1. Introduction
2. Methods
2.1. Study Design and Ethics
2.2. Study Population
2.3. Survey
2.4. Intervention
2.5. Statistics
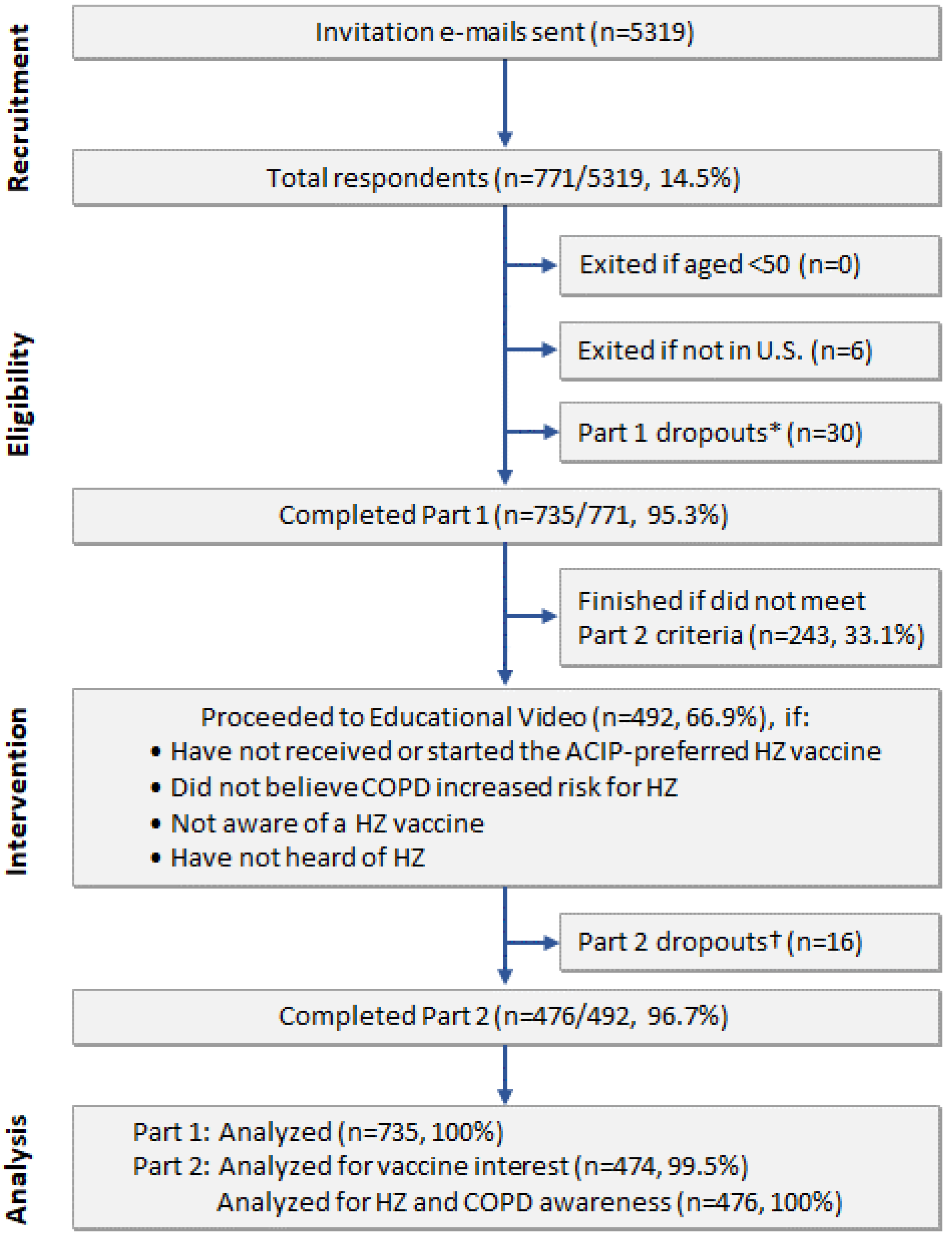
3. Results
3.1. Population Characteristics
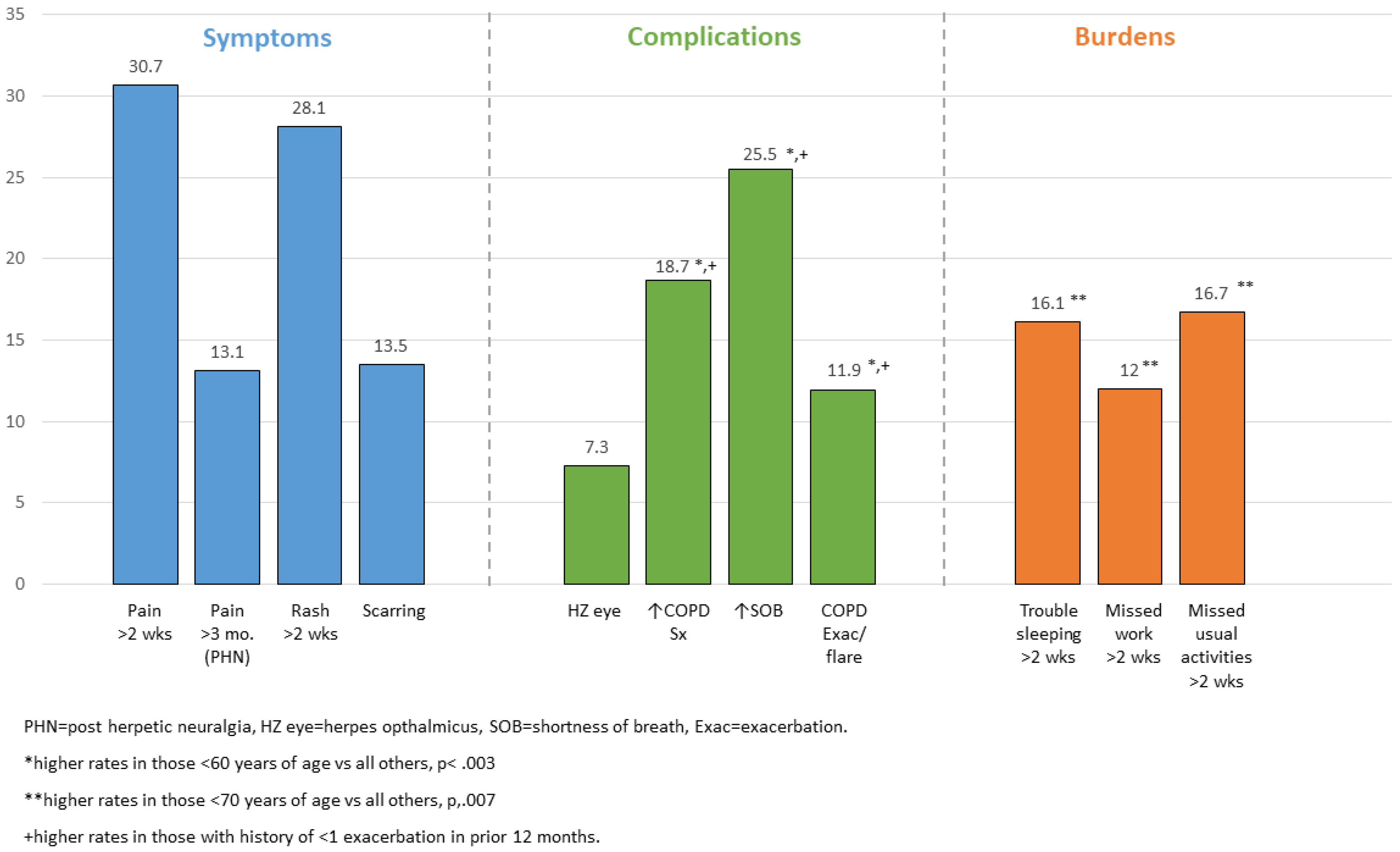
3.2. Experience and Perceived Burden of HZ
3.3. Perceived HZ Risk Associated with COPD and Opportunities for HZ Prevention
3.4. Barriers to HZ Vaccination
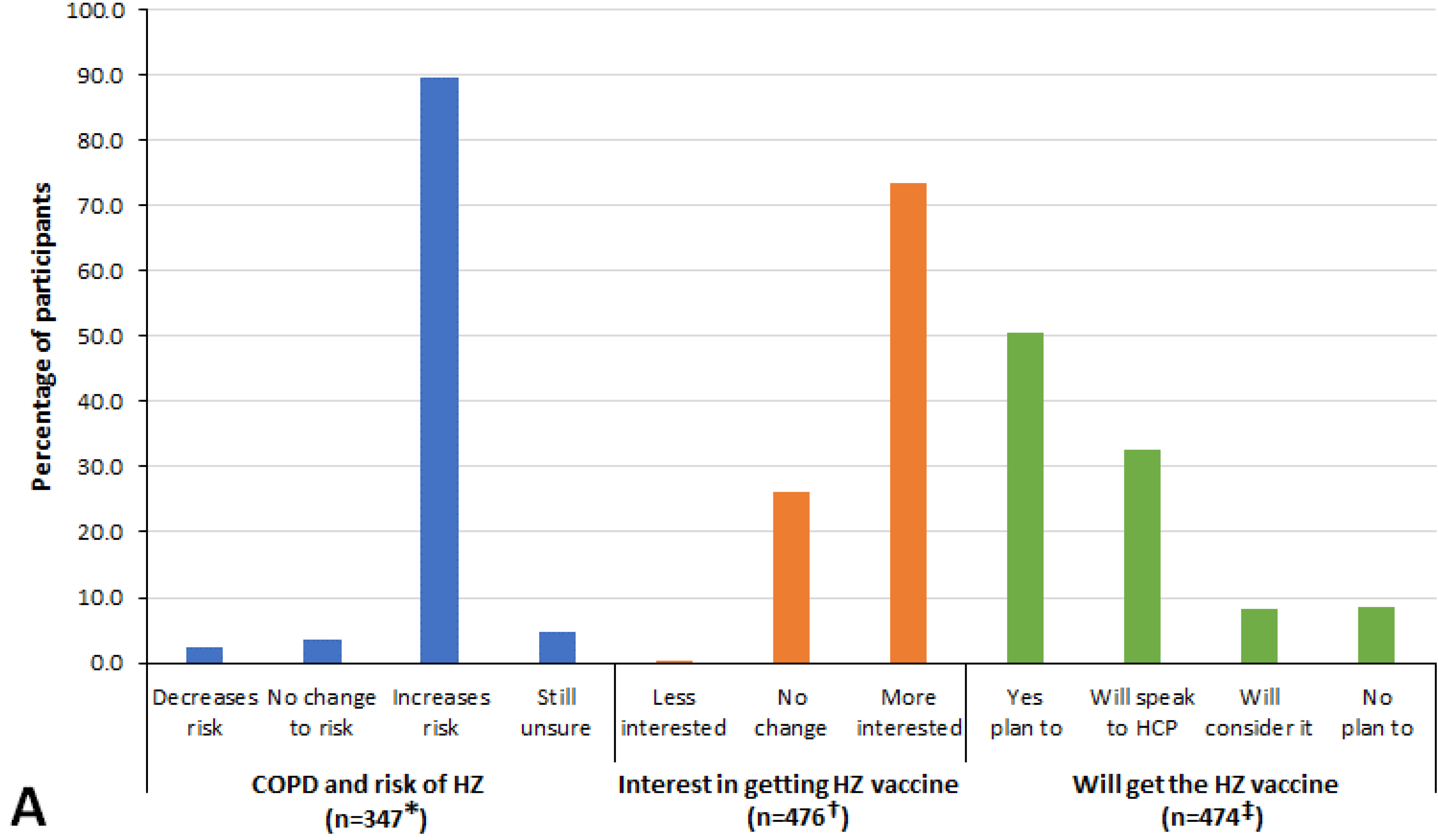
3.5. Responses after the HZ Educational Video
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention (CDC). Shingles (Herpes Zoster): Shingles Burden and Trends. Available online: https://www.cdc.gov/shingles/surveillance.html (accessed on 21 July 2021).
- Harpaz, R.; Ortega-Sanchez, I.R.; Seward, J.F. Prevention of herpes zoster: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm. Rep. 2008, 57, 1–30. [Google Scholar] [PubMed]
- Kawai, K.; Yawn, B.P.; Wollan, P.; Harpaz, R. Increasing Incidence of Herpes Zoster Over a 60-year Period from a Population-based Study. Clin. Infect. Dis. 2016, 63, 221–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Oorschot, D.; Vroling, H.; Bunge, E.; Diaz-Decaro, J.; Curran, D.; Yawn, B. A systematic literature review of herpes zoster incidence worldwide. Hum. Vaccines Immunother. 2021, 17, 1714–1732. [Google Scholar] [CrossRef] [PubMed]
- Yawn, B.P.; Saddier, P.; Wollan, P.C.; Sauver, J.S.; Kurland, M.J.; Sy, L.S. A Population-Based Study of the Incidence and Complication Rates of Herpes Zoster Before Zoster Vaccine Introduction. Mayo Clin. Proc. 2007, 82, 1341–1349. [Google Scholar] [CrossRef] [PubMed]
- Yawn, B.P.; Wollan, P.C.; Kurland, M.J.; Sauver, J.L.S.; Saddier, P. Herpes Zoster Recurrences More Frequent Than Previously Reported. Mayo Clin. Proc. 2011, 86, 88–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghaswalla, P.; Thompson-Leduc, P.; Cheng, W.Y.; Kunzweiler, C.; Wang, M.-J.; Bogart, M.; Patterson, B.J.; Duh, M.S.; Wojciehowski, J.; Park, S.; et al. Increased Health Care Resource Utilization and Costs Associated with Herpes Zoster Among Patients Aged ≥50 Years with Chronic Obstructive Pulmonary Disease in the United States. Chronic Obstr. Pulm. Dis. J. COPD Found. 2021, 8, 502–516. [Google Scholar] [CrossRef] [PubMed]
- Harvey, M.; Prosser, L.A.; Rose, A.M.; Ortega-Sanchez, I.R.; Harpaz, R. Aggregate health and economic burden of herpes zoster in the United States: Illustrative example of a pain condition. Pain 2020, 161, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Meyers, J.L.; Candrilli, S.D.; Rausch, D.A.; Yan, S.; Patterson, B.J.; Levin, M.J. Costs of herpes zoster complications in older adults: A cohort study of US claims database. Vaccine 2019, 37, 1235–1244. [Google Scholar] [CrossRef] [PubMed]
- Yawn, B.P.; Itzler, R.F.; Wollan, P.C.; Pellissier, J.M.; Sy, L.S.; Saddier, P. Health Care Utilization and Cost Burden of Herpes Zoster in a Community Population. Mayo Clin. Proc. 2009, 84, 787–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ernst, P.; Dell’Aniello, S.; Mikaeloff, Y.; Suissa, S. Risk of herpes zoster in patients prescribed inhaled corticosteroids: A cohort study. BMC Pulm. Med. 2011, 11, 59. [Google Scholar] [CrossRef] [Green Version]
- Esteban-Vasallo, M.D.; Domínguez-Berjón, M.F.; Gil-Prieto, R.; Astray-Mochales, J.; de Miguel, Á.G. Sociodemographic characteristics and chronic medical conditions as risk factors for herpes zoster—A population-based study from primary care in Madrid (Spain). Hum. Vaccines Immunother. 2014, 10, 1650–1660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joesoef, R.M.; Harpaz, R.; Leung, J.; Bialek, S.R. Chronic Medical Conditions as Risk Factors for Herpes Zoster. Mayo Clin. Proc. 2012, 87, 961–967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawai, K.; Yawn, B.P. Risk Factors for Herpes Zoster: A Systematic Review and Meta-analysis. Mayo Clin. Proc. 2017, 92, 1806–1821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muñoz-Quiles, C.; López-Lacort, M.; Díez-Domingo, J. Risk and impact of herpes zoster among COPD patients: A population-based study, 2009–2014. BMC Infect. Dis. 2018, 18, 203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.-W.; Chen, Y.-H.; Wang, K.-H.; Wang, C.-Y.; Lin, H.-W. Risk of herpes zoster among patients with chronic obstructive pulmonary disease: A population-based study. Can. Med. Assoc. J. 2011, 183, E275–E280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mareque, M.; Oyagüez, I.; Morano, R.; Casado, M. Systematic review of the evidence on the epidemiology of herpes zoster: Incidence in the general population and specific subpopulations in Spain. Public Health 2019, 167, 136–146. [Google Scholar] [CrossRef] [PubMed]
- Marra, F.; Parhar, K.; Huang, B.; Vadlamudi, N. Risk Factors for Herpes Zoster Infection: A Meta-Analysis. Open Forum Infect. Dis. 2020, 7, ofaa005. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.R.; Karmali, S.; Donaldson, G.C.; Goldring, J.J.; Wedzicha, J.A.; Hurst, J.R. Prevalence of Herpes Zoster in COPD And Relationships with Inhaled Corticosteroids, Exacerbation Frequency and FEV1. Am. J. Respir. Crit. Care Med. 2010, 181, A5926. [Google Scholar]
- Centers for Disease Control and Prevention (CDC). Vaccines and Preventable Diseases. What Everyone Should Know About Zostavax. Available online: https://www.cdc.gov/vaccines/vpd/shingles/public/zostavax/index.html (accessed on 21 July 2021).
- Merck & Co., Inc. Product Discontinuation Notice: Zostavax® (Zoster Vaccine Live). Available online: https://web.archive.org/web/20200818193428/https://www.merckvaccines.com/wp-content/uploads/sites/8/2020/06/US-CIN-00033.pdf (accessed on 21 July 2021).
- Cunningham, A.L.; Lal, H.; Kovac, M.; Chlibek, R.; Hwang, S.-J.; Diez-Domingo, J.; Godeaux, O.; Levin, M.J.; McElhaney, J.E.; Puig-Barberà, J.; et al. Efficacy of the Herpes Zoster Subunit Vaccine in Adults 70 Years of Age or Older. N. Engl. J. Med. 2016, 375, 1019–1032. [Google Scholar] [CrossRef] [PubMed]
- Dooling, K.L.; Guo, A.; Patel, M.; Lee, G.M.; Moore, K.; Belongia, E.; Harpaz, R. Recommendations of the Advisory Committee on Immunization Practices for Use of Herpes Zoster Vaccines. Morb. Mortal. Wkly. Rep. 2018, 67, 103–108. [Google Scholar] [CrossRef] [Green Version]
- Lal, H.; Cunningham, A.L.; Godeaux, O.; Chlibek, R.; Diez-Domingo, J.; Hwang, S.-J.; Levin, M.J.; McElhaney, J.E.; Poder, A.; Puig-Barberà, J.; et al. Efficacy of an Adjuvanted Herpes Zoster Subunit Vaccine in Older Adults. N. Engl. J. Med. 2015, 372, 2087–2096. [Google Scholar] [CrossRef]
- Hung, M.C.; Williams, W.W.; Lu, P.J.; Woods, L.O.; Koppaka, R.; Lindley, M.C. Vaccination Coverage among Adults in the United States, National Health Interview Survey, 2017. Available online: https://www.cdc.gov/vaccines/imz-managers/coverage/adultvaxview/pubs-resources/NHIS-2017.html (accessed on 1 February 2021).
- Terlizzi, E.P.; Black, M.P.H. Centers for Disease Control and Prevention (CDC). National Center for Health Statistics. Shingles Vaccination among Adults aged 60 and Over: United States, NCHS Data Brief No. 370, July. Available online: https://www.cdc.gov/nchs/products/databriefs/db370.htm (accessed on 21 July 2021).
- Bricout, H.; Torcel-Pagnon, L.; Lecomte, C.; Almas, M.F.; Matthews, I.; Lu, X.; Wheelock, A.; Sevdalis, N. Determinants of shingles vaccine acceptance in the United Kingdom. PLoS ONE 2019, 14, e0220230. [Google Scholar] [CrossRef] [Green Version]
- MacDonald, N.E.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; Goldstein, S.; Larson, H.; Manzo, M.L.; Reingold, A.; et al. Vaccine Hesitancy: Definition, Scope and Determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Aguado, M.T.; Barratt, J.; Beard, J.R.; Blomberg, B.B.; Chen, W.H.; Hickling, J.; Hyde, T.B.; Jit, M.; Jones, R.; Poland, G.A.; et al. Report on WHO meeting on immunization in older adults: Geneva, Switzerland, 22–23 March 2017. Vaccine 2018, 36, 921–931. [Google Scholar] [CrossRef] [PubMed]
- Baalbaki, N.A.; Fava, J.P.; Ng, M.; Okorafor, E.; Nawaz, A.; Chiu, W.; Salim, A.; Cha, R.; Kilgore, P. A Community-Based Survey to Assess Knowledge, Attitudes, Beliefs and Practices Regarding Herpes Zoster in an Urban Setting. Infect. Dis. Ther. 2019, 8, 687–694. [Google Scholar] [CrossRef] [Green Version]
- Lam, A.C.; Chan, M.; Chou, H.; Ho, S.; Li, H.; Lo, C.; Shek, K.; To, S.; Yam, K.; Yeung, I. A cross-sectional study of the knowledge, attitude, and practice of patients aged 50 years or above towards herpes zoster in an out-patient setting. Hong Kong Med. J. 2017, 23, 365–373. [Google Scholar] [CrossRef]
- Roh, N.K.; Park, Y.M.; Kang, H.; Choi, G.S.; Kim, B.J.; Lee, Y.W.; Lew, B.L.; Sim, W.Y. Awareness, Knowledge, and Vaccine Acceptability of, Herpes Zoster in Korea: A Multicenter Survey of 607 Patients. Ann. Dermatol. 2015, 27, 531–538. [Google Scholar] [CrossRef] [Green Version]
- Teeter, B.S.; Garza, K.B.; Stevenson, T.L.; Williamson, M.A.; Zeek, M.L.; Westrick, S.C. Factors associated with herpes zoster vaccination status and acceptance of vaccine recommendation in community pharmacies. Vaccine 2014, 32, 5749–5754. [Google Scholar] [CrossRef] [PubMed]
- Valente, N.; Lupi, S.; Stefanati, A.; Cova, M.; Sulcaj, N.; Piccinni, L.; Gabutti, G.; GPs Study Group. Evaluation of the acceptability of a vaccine against herpes zoster in the over 50 years old: An Italian observational study. BMJ Open 2016, 6, e011539. [Google Scholar] [CrossRef] [Green Version]
- Singleton, J.A.; Santibanez, T.A.; Wortley, P.M. Influenza and Pneumococcal Vaccination of Adults Aged ≥65: Racial/Ethnic Differences. Am. J. Prev. Med. 2005, 29, 412–420. [Google Scholar] [CrossRef]
- Hong, K.; Zhou, F.; Tsai, Y.; Jatlaoui, T.C.; Acosta, A.M.; Dooling, K.L.; Kobayashi, M.; Lindley, M.C. Decline in Receipt of Vaccines by Medicare Beneficiaries During the COVID-19 Pandemic—United States. Morb. Mortal. Wkly. Rep. 2021, 70, 245–249. [Google Scholar] [CrossRef] [PubMed]
- Insinga, R.P.; Itzler, R.F.; Pellissier, J.M.; Saddier, P.; Nikas, A.A. The incidence of herpes zoster in a United States administrative database. J. Gen. Intern. Med. 2005, 20, 748–753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cunningham, A.L.; Levin, M.J. Herpes Zoster Vaccines. J. Infect. Dis. 2018, 218, S127–S133. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, A.; Kroehl, M.E.; Johnson, M.J.; Hammes, A.; Reinhold, D.; Lang, N.; Levin, M.J. Comparative Immune Responses to Licensed Herpes Zoster Vaccines. J. Infect. Dis. 2018, 218, S81–S87. [Google Scholar] [CrossRef] [PubMed]
- Cantuaria, M.L.; Blanes-Vidal, V. Self-reported data in environmental health studies: Mail vs. web-based surveys. BMC Med. Res. Methodol. 2019, 19, 238. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.G.; Witte, M.; Rocha, S.; Basner, M. Effectiveness of incentives and follow-up on increasing survey response rates and participation in field studies. BMC Med. Res. Methodol. 2019, 19, 230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yawn, B.P.; Pasquale, C.B.; Przybysz, R.; McCreary, G. How COPD Patient-Powered Research Network registry and Optum electronic health records can supplement each other to provide a comprehensive picture of COPD in real-world settings [Abstract]. Am. J. Respir. Crit. Care Med. 2021, 203, A1134. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Participants with COPD (n = 735) |
|---|---|
| Age, mean (SD), years | 68.5 (7.9) |
| Male/Female, n (%) * | 296/438 (40.3/59.6) |
| Ethnicity, n (%) | |
| Caucasian | 688 (93.6) |
| Black or African American | 18 (2.4) |
| Multi-ethnicity | 15 (2.0) |
| Other/Unknown | 14 (1.9) |
| Overall health, n (%) | |
| Very good or excellent | 63 (8.6) |
| Good | 283 (38.5) |
| Poor or fair | 389 (52.9) |
| Number of days in the past 30 days where physical health was not good, mean (SD) | 10.7 (11.0) |
| Number of days in the past 30 days where mental health was not good, mean (SD) | 6.8 (8.8) |
| Number of days in the past 30 days where poor physical or mental health prevented usual activity, mean (SD) | 8.9 (10.3) |
| One or more exacerbations in the prior year, n (%) † | 395 (53.7) |
| CAT score, mean (SD) | 19.6 (8.0) |
| Previously had HZ, n (%) ‡ | 192 (26.1) |
| Know others who have had HZ, n (%) ‡ | 492 (66.9) |
| Previously vaccinated against HZ, n (%) § | 419 (57.0) |
| One-shot vaccine only (Zostavax® (Merck, Kenilworth, NJ, USA)) | 116 (15.8) |
| Two-shot vaccine (Shingrix® (GlaxoSmithKline, Phildelphia, PA, USA); alone or plus Zostavax®) | 243 (33.1) |
| Not known which kind | 60 (8.2) |
| Symptom/Problem | How Bothersome Are the Symptoms and Problems for People with COPD, n (%) (n = 735) * | How Important Is Prevention of the Symptoms and Problems for People with COPD, n (%) (n = 735) * | ||||
|---|---|---|---|---|---|---|
| Not at All | Somewhat | Very | Not at All | Somewhat | Very | |
| HZ rash | 19 (2.6) | 169 (23.0) | 547 (74.4) | 11 (1.5) | 91 (12.4) | 633 (86.1) |
| HZ pain: 1–4 weeks | 9 (1.2) | 100 (13.6) | 626 (85.2) | 4 (0.5) | 64 (8.7) | 667 (90.7) |
| 1–3 months | 18 (2.4) | 66 (9.0) | 651 (88.6) | 3 (0.4) | 46 (6.3) | 686 (93.3) |
| >3 months | 27 (3.7) | 58 (7.9) | 650 (88.4) | 6 (0.8) | 39 (5.3) | 690 (93.9) |
| Fear of infecting others | 110 (15.0) | 216 (29.4) | 409 (55.6) | 62 (8.4) | 130 (17.7) | 543 (73.9) |
| Persistent sadness or anxiety | 69 (9.4) | 251 (34.1) | 415 (56.5) | 33 (4.5) | 142 (19.3) | 560 (76.2) |
| Missing work or usual activities | 51 (6.9) | 206 (28.0) | 478 (65.0) | 29 (3.9) | 131 (17.9) | 575 (78.2) |
| Missed social activities | 54 (7.3) | 222 (30.2) | 459 (62.4) | 35 (4.8) | 171 (23.3) | 529 (72.0) |
| Increased COPD symptoms | 64 (8.7) | 148 (20.1) | 523 (71.2) | 25 (3.4) | 89 (12.1) | 621 (84.5) |
| COPD exacerbation | 66 (9.0) | 134 (18.2) | 535 (72.8) | 28 (3.8) | 72 (9.8) | 635 (86.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yawn, B.P.; Merrill, D.D.; Martinez, S.; Callen, E.; Cotton, J.; Williams, D.; Loskutova, N.Y. Knowledge and Attitudes Concerning Herpes Zoster among People with COPD: An Interventional Survey Study. Vaccines 2022, 10, 420. https://doi.org/10.3390/vaccines10030420
Yawn BP, Merrill DD, Martinez S, Callen E, Cotton J, Williams D, Loskutova NY. Knowledge and Attitudes Concerning Herpes Zoster among People with COPD: An Interventional Survey Study. Vaccines. 2022; 10(3):420. https://doi.org/10.3390/vaccines10030420
Chicago/Turabian StyleYawn, Barbara P., Debora D. Merrill, Sergio Martinez, Elisabeth Callen, Janice Cotton, Dennis Williams, and Natalia Y. Loskutova. 2022. "Knowledge and Attitudes Concerning Herpes Zoster among People with COPD: An Interventional Survey Study" Vaccines 10, no. 3: 420. https://doi.org/10.3390/vaccines10030420