
Willingness of the Jordanian Population to Receive a COVID-19 Booster Dose: A Cross-Sectional Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Sampling Type and Sample Size
2.2. Survey Validity and Reliability
2.3. Study Instrument and Data Collection
2.4. Statistical Analysis
3. Results
3.1. Sample Charecteristics
3.2. Sample Charecteristics’ Association with Booster Dose Acceptance
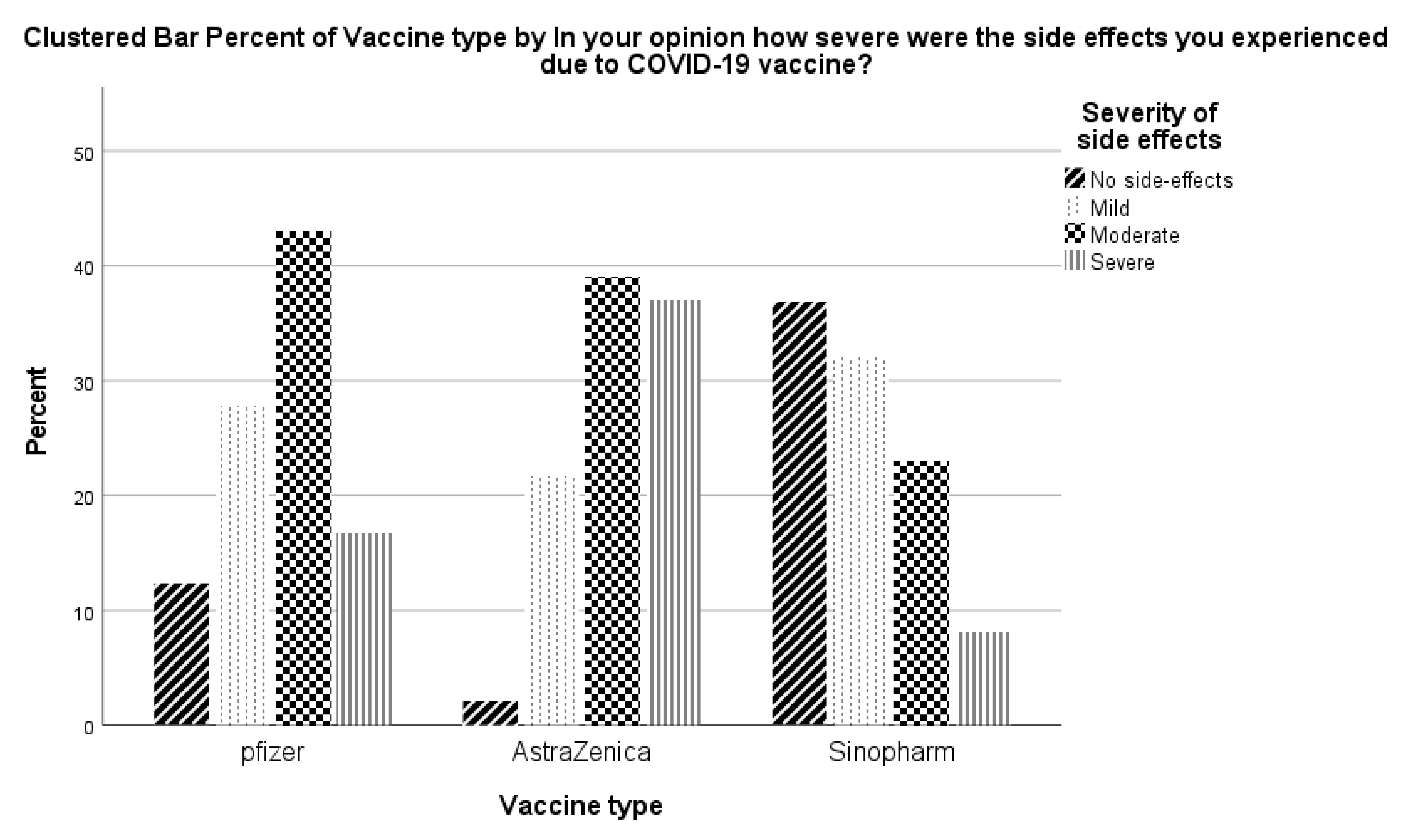
3.3. Resported COVID-19 Side Effects by Vaccine Type
3.4. Reported Reasons for Booster Dose Hesitency/Refusal
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hussein, T.; Hammad, M.H.; Fung, P.L.; Al-Kloub, M.; Odeh, I.; Zaidan, M.A.; Wraith, D. COVID-19 Pandemic Development in Jordan—Short-Term and Long-Term Forecasting. Vaccines 2021, 9, 728. [Google Scholar] [CrossRef]
- WHO Coronavirus (COVID-19) Dashboard with Vaccination Data. Available online: https://covid19.who.int/ (accessed on 1 February 2022).
- Rzymski, P.; Poniedziałek, B.; Fal, A. Willingness to Receive the Booster COVID-19 Vaccine Dose in Poland. Vaccines 2021, 9, 1286. [Google Scholar] [CrossRef] [PubMed]
- Ndwandwe, D.; Wiysonge, C.S. COVID-19 vaccines. Curr. Opin. Immunol. 2021, 71, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Moline, H.L.; Whitaker, M.; Deng, L.; Rhodes, J.C.; Milucky, J.; Pham, H.; Patel, K.; Anglin, O.; Reingold, A.; Chai, S.J.; et al. Effectiveness of COVID-19 Vaccines in Preventing Hospitalization Among Adults Aged ≥65 Years—COVID-NET, 13 States, February-April 2021. MMWR. Morb. Mortal. Wkly. Rep. 2021, 70, 1088–1093. [Google Scholar] [CrossRef] [PubMed]
- CDC. COVID-19 Vaccines for People with Underlying Medical Conditions. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations/underlying-conditions.html (accessed on 1 February 2022).
- Vasireddy, D.; Vanaparthy, R.; Mohan, G.; Malayala, S.V.; Atluri, P. Review of COVID-19 Variants and COVID-19 Vaccine Efficacy: What the Clinician Should Know? J. Clin. Med. Res. 2021, 13, 317–325. [Google Scholar] [CrossRef]
- Arbel, R.; Hammerman, A.; Sergienko, R.; Friger, M.; Peretz, A.; Netzer, D.; Yaron, S. BNT162b2 Vaccine Booster and Mortality Due to COVID-19. N. Engl. J. Med. 2021, 385, 2413–2420. [Google Scholar] [CrossRef]
- Mathieu, E.; Ritchie, H.; Ortiz-Ospina, E.; Roser, M.; Hasell, J.; Appel, C.; Giattino, C.; Rodés-Guirao, L. Coronavirus Pandemic (COVID-19). Our World Data 2020, 5, 947–953. [Google Scholar] [CrossRef]
- Pal, S.; Shekhar, R.; Kottewar, S.; Upadhyay, S.; Singh, M.; Pathak, D.; Kapuria, D.; Barrett, E.; Sheikh, A.B. COVID-19 Vaccine Hesitancy and Attitude toward Booster Doses among US Healthcare Workers. Vaccines 2021, 9, 1358. [Google Scholar] [CrossRef]
- Klugar, M.; Riad, A.; Mohanan, L.; Pokorná, A. COVID-19 Vaccine Booster Hesitancy (VBH) of Healthcare Workers in Czechia: National Cross-Sectional Study. Vaccines 2021, 9, 1437. [Google Scholar] [CrossRef]
- Salmon, D.A.; Dudley, M.Z.; Glanz, J.M.; Omer, S.B. Vaccine Hesitancy: Causes, Consequences, and a Call to Action. Am. J. Prev. Med. 2015, 49, S391–S398. [Google Scholar] [CrossRef]
- Sugawara, N.; Yasui-Furukori, N.; Fukushima, A.; Shimoda, K. Attitudes of Medical Students toward COVID-19 Vaccination: Who Is Willing to Receive a Third Dose of the Vaccine? Vaccines 2021, 9, 1295. [Google Scholar] [CrossRef]
- Gabarron, E.; Oyeyemi, S.O.; Wynn, R. COVID-19-related misinformation on social media: A systematic review. Bull. World Health Organ. 2021, 99, 455. [Google Scholar] [CrossRef]
- McAteer, J.; Yildirim, I.; Chahroudi, A. The VACCINES Act: Deciphering Vaccine Hesitancy in the Time of COVID-19. Clin. Infect. Dis. 2020, 71, 703–705. [Google Scholar] [CrossRef]
- Dettori, M.; Arghittu, A.; Deiana, G.; Azara, A.; Masia, M.D.; Palmieri, A.; Spano, A.L.; Serra, A.; Castiglia, P. Influenza Vaccination Strategies in Healthcare Workers: A Cohort Study (2018–2021) in an Italian University Hospital. Vaccines 2021, 9, 971. [Google Scholar] [CrossRef]
- González-Block, M.Á.; Arroyo-Laguna, J.; Rodríguez-Zea, B.; Pelcastre-Villafuerte, B.E.; Gutiérrez-Calderón, E.; Díaz-Portillo, S.P.; Puentes-Rosas, E.; Sarti, E. The importance of confidence, complacency, and convenience for influenza vaccination among key risk groups in large urban areas of Peru. Hum. Vaccines Immunother. 2021, 17, 465–474. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Report of the Sage Working Group on Vaccine Hesitancy. Available online: https://www.who.int/immunization/sage/meetings/2014/october/1_Report_WORKING_GROUP_vaccine_hesitancy_final.pdf (accessed on 25 February 2022).
- Wilson, S.L.; Wiysonge, C. Social media and vaccine hesitancy. BMJ Glob. Health 2020, 5, e004206. [Google Scholar] [CrossRef]
- World Health Organization (WHO). The Current COVID-19 Situation in Jordan. Available online: https://www.who.int/countries/jor/ (accessed on 25 February 2022).
- Adam Redfern covidvax.live-Jordan. Available online: https://covidvax.live/location/jor (accessed on 3 January 2022).
- Indexmundi Jordan Demographics Profile. Available online: https://www.indexmundi.com/jordan/demographics_profile.html (accessed on 25 February 2022).
- Peduzzi, P.; Concato, J.; Feinstein, A.R.; Holford, T.R. Importance of events per independent variable in proportional hazards regression analysis. II. Accuracy and precision of regression estimates. J. Clin. Epidemiol. 1995, 48, 1503–1510. [Google Scholar] [CrossRef]
- Streiner, D.L.; Norman, G.R.; Cairney, J. Health Measurement Scales: A Practical Guide to Their Development and Use, 5th ed.; Oxford University Press: New York, NY, USA, 2015; ISBN 978-0-19-968521-9. [Google Scholar]
- Sharma, B. A focus on reliability in developmental research through Cronbach’s Alpha among medical, dental and paramedical professionals. Asian Pac. J. Health Sci. 2016, 3, 271–278. [Google Scholar] [CrossRef]
- Cortina, J.M. What is coefficient alpha? An examination of theory and applications. J. Appl. Psychol. 1993, 78, 98–104. [Google Scholar] [CrossRef]
- Al-Qerem, W.; Jarab, A.S.; Qarqaz, R.; Hayek, M. Al Attitudes of a sample of Jordanian young adults toward different available COVID-19 vaccines. Vacunas 2021, in press. [Google Scholar] [CrossRef]
- Al-Qerem, W.A.; Jarab, A.S. COVID-19 Vaccination Acceptance and Its Associated Factors Among a Middle Eastern Population. Front. Public Health 2021, 9, 2914. [Google Scholar] [CrossRef]
- Certain Medical Conditions and Risk for Severe COVID-19 Illness|CDC. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html (accessed on 3 January 2022).
- Fedele, F.; Aria, M.; Esposito, V.; Micillo, M.; Cecere, G.; Spano, M.; De Marco, G. COVID-19 vaccine hesitancy: A survey in a population highly compliant to common vaccinations. Hum. Vaccines Immunother. 2021, 17, 3348–3354. [Google Scholar] [CrossRef]
- Alcendor, D.J. Targeting COVID Vaccine Hesitancy in Rural Communities in Tennessee: Implications for Extending the COVID-19 Pandemic in the South. Vaccines 2021, 9, 1279. [Google Scholar] [CrossRef]
- Elgendy, M.O.; Abdelrahim, M.E.A. Public awareness about coronavirus vaccine, vaccine acceptance, and hesitancy. J. Med. Virol. 2021, 93, 6535–6543. [Google Scholar] [CrossRef]
- Tsang, S.; Royse, C.F.; Terkawi, A.S. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi J. Anaesth. 2017, 11, S80–S89. [Google Scholar] [CrossRef]
- Canova, S.; Cortinovis, D.L.; Ambrogi, F. How to describe univariate data. J. Thorac. Dis. 2017, 9, 1741. [Google Scholar] [CrossRef] [Green Version]
- Apostolopoulos, V.; Tafuri, S.; Qin, C.; Wang, R.; Tao, L.; Liu, M.; Liu, J. Acceptance of a Third Dose of COVID-19 Vaccine and Associated Factors in China Based on Health Belief Model: A National Cross-Sectional Study. Vaccines 2022, 10, 89. [Google Scholar] [CrossRef]
- Saeed, B.Q.; Al-Shahrabi, R.; Alhaj, S.S.; Alkokhardi, Z.M.; Adrees, A.O. Side effects and perceptions following Sinopharm COVID-19 vaccination. Int. J. Infect. Dis. 2021, 111, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Anand, P.; Stahel, V.P. Review the safety of COVID-19 mRNA vaccines: A review. Patient Saf. Surg. 2021, 15, 20. [Google Scholar] [CrossRef] [PubMed]
- Al Bawab, A.Q.; Al-Qerem, W.; Abusara, O.; Alkhatib, N.; Mansour, M.; Horne, R. What Are the Factors Associated with Nonadherence to Medications in Patients with Chronic Diseases? Healthcare 2021, 9, 1237. [Google Scholar] [CrossRef] [PubMed]
- Jimmy, B.; Jose, J. Patient Medication Adherence: Measures in Daily Practice. Oman Med. J. 2011, 26, 155. [Google Scholar] [CrossRef]
- Atal, S.; Sadasivam, B.; Ahmed, S.N.; Ray, A. Medication concordance in modern medicine—A critical appraisal from an Indian perspective. J. Fam. Med. Prim. Care 2019, 8, 1313. [Google Scholar] [CrossRef]
- Dowell, J.; Jones, A.; Snadden, D. Exploring medication use to seek concordance with “non-adherent” patients: A qualitative study. Br. J. Gen. Pract. 2002, 52, 24–32. [Google Scholar]
- Phatak, H.M.; Thomas, J. Relationship between beliefs about medications and nonadherence to prescribed chronic medications. Ann. Pharmacother. 2006, 40, 1737–1742. [Google Scholar] [CrossRef]
- Vogel, E.A.; Henriksen, L.; Schleicher, N.C.; Prochaska, J.J. Perceived Susceptibility to and Seriousness of COVID-19: Associations of Risk Perceptions with Changes in Smoking Behavior. Int. J. Environ. Res. Public Health 2021, 18, 7621. [Google Scholar] [CrossRef]
- Zewude, B.; Habtegiorgis, T.; Hizkeal, A.; Dela, T.; Siraw, G. Perceptions and Experiences of COVID-19 Vaccine Side-Effects Among Healthcare Workers in Southern Ethiopia: A Cross-Sectional Study. Pragmatic Obs. Res. 2021, 12, 131–145. [Google Scholar] [CrossRef]
- Menni, C.; Klaser, K.; May, A.; Polidori, L.; Capdevila, J.; Louca, P.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Merino, J.; et al. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID Symptom Study app in the UK: A prospective observational study. Lancet Infect. Dis. 2021, 21, 939–949. [Google Scholar] [CrossRef]
- Zarocostas, J. How to fight an infodemic. Lancet 2020, 395, 676. [Google Scholar] [CrossRef]
- Xue, J.; Chen, J.; Hu, R.; Chen, C.; Zheng, C.; Su, Y.; Zhu, T. Twitter Discussions and Emotions About the COVID-19 Pandemic: Machine Learning Approach. J. Med. Internet Res. 2020, 22, e20550. [Google Scholar] [CrossRef]
- Fenner, Y.; Garland, S.M.; Moore, E.E.; Jayasinghe, Y.; Fletcher, A.; Tabrizi, S.N.; Gunasekaran, B.; Wark, J.D. Web-based recruiting for health research using a social networking site: An exploratory study. J. Med. Internet Res. 2012, 14, e20. [Google Scholar] [CrossRef]
- Cantrell, M.A.; Lupinacci, P. Methodological issues in online data collection. J. Adv. Nurs. 2007, 60, 544–549. [Google Scholar] [CrossRef]
- The Jordanian Department of Statistics Population Estimares-Databook. Available online: http://dosweb.dos.gov.jo/Data (accessed on 25 February 2022).
- World Bank Group. Hashemite Kingdom of Jordan Promoting Poverty Reduction and Shared Prosperity: Systematic Country Diagnostic. World Bank, Washington, DC. © World Bank. 2016. Available online: https://openknowledge.worldbank.org/handle/10986/23956 (accessed on 24 February 2022).
- The Jordanian Department of Statistics Distribution of Jordanian Households and Household Individuals by Groups of Annual Current Income (%). Available online: http://www.dos.gov.jo/dos_home_e/main/linked-html/household/2017/G3/Table1G3_Jor.pdf (accessed on 24 February 2022).
- Al-Qerem. 3rd Dose Acceptance. 2022. Available online: https://zenodo.org/record/6026138#.Yif-aZYRWUk (accessed on 9 February 2022).


{kind=link}
| Frequency (%) (n = 915) | ||
|---|---|---|
| Age | 18–29 years | 418 (45.7) |
| 30–39 years | 228 (24.9) | |
| 40–49 years | 143 (15.6) | |
| 50–59 years | 90 (9.8) | |
| 60 years or more | 36 (3.9) | |
| Marital status | Married | 457 (49.9) |
| Do you have children? | Yes | 433 (47.3) |
| Do you have a chronic disease? | Yes | 203 (22.2) |
| Do you Smoke? | No | 660 (72.1) |
| Ex-smoker | 32 (3.5) | |
| Yes | 223 (24.4) | |
| Educational level | High school or less | 66 (7.2) |
| Diploma | 41 (4.5) | |
| University student | 168 (18.4) | |
| Bachelor | 586 (64.0) | |
| Postgraduate | 54 (5.9) | |
| Household average monthly income | Less than 500 JD | 340 (37.2) |
| 500–1000 JD | 393 (43.0) | |
| More than 1000 JD | 182 (19.9) | |
| Residence | North region | 87 (9.5) |
| South region | 23 (2.5) | |
| Zarqa | 90 (9.8) | |
| Middle region | 50 (5.5) | |
| Amman | 631 (69.0) | |
| Other | 34 (3.7) | |
| Side effects experienced from a COVID-19 vaccine | No symptom | 193 (21.1) |
| Mild | 266 (29.1) | |
| Moderate | 323 (35.3) | |
| Severe | 133 (14.5) | |
| Know someone who died due to COVID-19? | Yes | 677 (74.0) |
| Reported side effects due to COVID-19 vaccine | Headache | 501 (54.8) |
| Hyperthermia | 517 (56.5) | |
| Pain at site of injection | 615 (67.2) | |
| Muscle pain | 275 (30.1) | |
| Weakness | 365 (39.9) | |
| Spasm | 356 (38.9) | |
| Nausea | 158 (17.3) | |
| Rash | 21 (2.3) | |
| Chills | 192 (21.0) | |
| Water retention | 22 (2.4) | |
| No symptoms | 155 (16.9) | |
| Variables | Are You Willing to Receive the Booster Dose for COVID-19 Vaccine | p-Value | ||
|---|---|---|---|---|
| No (n = 281, 30.7%) | Not Sure (n = 226, 24.7%) | Yes (n = 408, 44.6%) | ||
| Participant Age | 0.167 | |||
| 18–29 years | 138 (33.0) | 111 (26.6) | 169 (40.4) | |
| 30–39 years | 74 (32.5) | 53 (23.2) | 101 (44.3) | |
| 40–49 years | 39 (27.3) | 36 (25.2) | 68 (47.6) | |
| 50–59 years | 20 (22.2) | 21 (23.3) | 49 (54.4) | |
| 60 years or more | 10 (27.8) | 5 (13.9) | 21 (58.3 | |
| Do you have children? | 0.20 | |||
| No | 158 (32.8%) | 122 (25.3%) | 202 (41.9%) | |
| Yes | 123 (28.4%) | 104 (24.0%) | 206 (47.6%) | |
| Marital status | 0.20 | |||
| Married | 132(28.9%) | 108 (23.6%) | 217 (47.5%) | |
| Other | 149 (32.5%) | 118 (25.8%) | 191 (41.7%) | |
| Education level | 0.18 | |||
| High school or less | 17 (25.8) | 12 (18.2) | 37 (65.1) | |
| University student | 59 (35.1) | 47 (28.0) | 62 (36.9) | |
| Diploma | 17 (41.5) | 7 (17.1) | 17 (41.5) | |
| Bachelor’s degree | 174 (29.7) | 147 (25.1) | 255 (45.2) | |
| Postgraduate | 14 (25.9) | 13 (24.1) | 27 (50.0) | |
| Household average monthly income | 0.10 | |||
| Less than 500 JD | 112 (32.9) | 82 (24.1) | 146 (42.9) | |
| 500–1000 JD | 119 (30.3) | 108 (27.5) | 166 (42.2) | |
| More than 1000 JD | 50 (27.5) | 36 (19.8) | 96 (52.7) | |
| In your opinion how severe were the symptoms you experienced due to COVID-19 vaccine? | 0.003 | |||
| Mild | 74 (27.8) | 65 (24.4) | 127 (47.7) | |
| Moderate | 105 (32.5) | 85 (26.3) | 133 (41.2) | |
| Sever | 58 (43.6) | 28 (21.1) | 47 (35.3) | |
| No symptom | 44 (22.8) | 48 (24.9) | 101 (52.3) | |
| Did you take the COVID-19 vaccine out of conviction, or you were forced by laws imposed by the state? | <0.001 | |||
| I took it out of conviction | 52 (13.9) | 58 (15.5) | 264 (70.6) | |
| I took it out of conviction and because of the laws | 45 (19.8) | 92 (40.5) | 90 (36.6) | |
| I took it because of the imposed laws, not because I believe in it | 182 (59.1) | 75 (24.4) | 51 (16.6) | |
| Do you know someone who has died from COVID-19? | 0.28 | |||
| No | 82 (34.7) | 55 (23.3) | 99 (41.9) | |
| Yes | 198 (29.2) | 171 (25.3) | 308 (45.5) | |
| In your opinion, how serious is COVID-19? | 3.5 (3–4) | 3 (3–4) | 4 (3–4) | 0.03 |
| Risk level | 0.009 | |||
| Low | 139 (32.6) | 123 (28.9) | 164 (38.5) | |
| Medium | 74 (28.1) | 58 (22.1) | 131 (49.8) | |
| High | 68 (30.1) | 45 (19.9) | 113 (50.0) | |
| Knowledge level | 0.09 | |||
| Low | 135 (33.7) | 103 (25.7) | 163 (40.6) | |
| High | 146 (28.4) | 123 (23.9) | 245 (47.7) | |
| Practice level | 0.23 | |||
| Low | 141 (32.9) | 109 (25.4) | 179 (41.7) | |
| High | 140 (28.8) | 117 (24.1) | 229 (47.1) | |
| Vaccine type | <0.001 | |||
| Pfizer | 175 (33.3) | 142 (27) | 208 (39.6) | |
| AstraZeneca | 21(45.7) | 8 (17.4) | 17 (37) | |
| Sinopharm | 85(24.7) | 76 (22.1) | 183 (53.2) | |
| Characteristics | Intent to Vaccinate No vs. Yes OR (95%CI) | Intent to Vaccinate Not Sure vs. Yes OR (95%CI) |
|---|---|---|
| In your opinion, how serious is COVID-19? | 0.91 (0.76–1.10) | 0.90 (0.75–1.07) |
| Participant Age | ||
| 18–29 years | 0.92 (0.31–2.79) | 2.20 (0.65–7.49) |
| 30–39 years | 0.97 (0.34–2.81) | 1.67 (0.51–5.50) |
| 40–49 years | 0.77 (0.26–2.32) | 1.66 (0.49–5.59) |
| 50–59 years | 0.56 (0.18–1.79) | 1.62 (0.47–5.60) |
| 60 years or more | Reference | |
| Marital status | ||
| Other | 0.86 (0.39–1.92) | 1.17 (0.51–2.68) |
| Married | Reference | |
| Do you have children | ||
| No | 1.25 (0.60–2.60) | 0.73 (0.33–1.61) |
| Yes | Reference | |
| Education level | ||
| High school or less | 0.39 (0.13–1.17) | 0.38 (0.21–1.10) |
| University student | 0.95 (0.36–2.48) | 0.70 (0.28–1.74) |
| Diploma | 0.73 (0.23–2.32) | 0.36 (0.10–1.23) |
| Bachelor’s degree | 0.79 (0.34–1.84) | 0.60 (0.27–1.35) |
| Postgraduate | Reference | |
| Household average monthly income | ||
| Less than 500 JD | 1.23 (0.72–2.10) | 1.63 (0.95–2.78) |
| 500–1000 JD | 1.29 (0.77–2.17) | 1.79 (1.07–3.0) * |
| More than 1000 JD | Reference | |
| In your opinion how severe were the symptoms you experienced due to COVID-19 vaccine? | ||
| No symptom | 0.34 (0.18–0.65) ** | 0.81 (0.43–1.54) |
| Mild | 0.54 (0.31–0.97) * | 0.87 (0.48–1.60) |
| Moderate | 0.64 (0.37–1.13) | 1.08 (0.60–1.96) |
| Severe | Reference | |
| Did you take the COVID-19 vaccine out of conviction, or you were forced by laws imposed by the state? | ||
| I took it because of the imposed laws, not because I believe in it | 20.88 (13.13–33.21) ** | 7.42 (4.58–12.01) ** |
| I took it out of conviction and because of the laws | 2.68 (1.66–4.34) ** | 4.99 (3.27–7.63) ** |
| I took it out of conviction | Reference | |
| Do you know someone who has died from COVID-19? | ||
| No | 1.42 (0.93–2.17) | 0.94 (0.61–1.44) |
| Yes | Reference | |
| Knowledge level | ||
| Low | 1.17 (0.81–1.70) | 1.18 (0.82–1.71) |
| High | Reference | |
| Risk level | ||
| Low | 1.52 (0.94–2.46) | 1.70 (1.06–2.74) * |
| Medium | 0.89 (0.53–1.49) | 0.93 (0.55–1.56) |
| High | Reference | |
| Total practice score | ||
| Low | 1.01 (0.69–1.47) | 1.06 (0.73–1.52) |
| High | Reference |
| Reasons | Frequency (%) |
|---|---|
| The booster dose will not provide me with any further protection against COVID-19. | 277 (30.3) |
| The booster dose will have severe side effects. | 312 (34.1) |
| I can’t tolerate another dose because the side-effects of the previous ones were severe. | 225 (24.6) |
| I was infected with COVID-19, therefore I do not need the booster dose. | 120 (13.1) |
| The symptoms I experienced due to COVID-19 infection were mild; therefore, I will not receive the booster dose. | 238 (26.0) |
| Taking the booster dose now has no benefit, however I may receive it in the future. | 351 (38.4) |
| I took the last dose a short time ago, so there will be no need to take the booster dose for at least a year. | 338 (36.9) |
| The benefits of a booster dose have not been scientifically proven. | 364 (39.8) |
| The booster dose is a conspiracy to boost corporate profits. | 318 (34.8) |
| A booster dose will be imposed only based on agreements reached between pharmaceutical companies and governments. | 279 (30.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Qerem, W.; Al Bawab, A.Q.; Hammad, A.; Ling, J.; Alasmari, F. Willingness of the Jordanian Population to Receive a COVID-19 Booster Dose: A Cross-Sectional Study. Vaccines 2022, 10, 410. https://doi.org/10.3390/vaccines10030410
Al-Qerem W, Al Bawab AQ, Hammad A, Ling J, Alasmari F. Willingness of the Jordanian Population to Receive a COVID-19 Booster Dose: A Cross-Sectional Study. Vaccines. 2022; 10(3):410. https://doi.org/10.3390/vaccines10030410
Chicago/Turabian StyleAl-Qerem, Walid, Abdel Qader Al Bawab, Alaa Hammad, Jonathan Ling, and Fawaz Alasmari. 2022. "Willingness of the Jordanian Population to Receive a COVID-19 Booster Dose: A Cross-Sectional Study" Vaccines 10, no. 3: 410. https://doi.org/10.3390/vaccines10030410