
Effects of Religious Practice and Teachings about Sexual Behavior on Intent to Vaccinate against Human Papillomavirus


Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey of Christian Parents
2.2. Survey Description
2.3. Confirmatory Factor Analysis and Structural Equation Modeling
2.4. Univariate Analysis
3. Results
3.1. Characteristics of Study Respondents
3.2. Confirmatory Factor Analysis
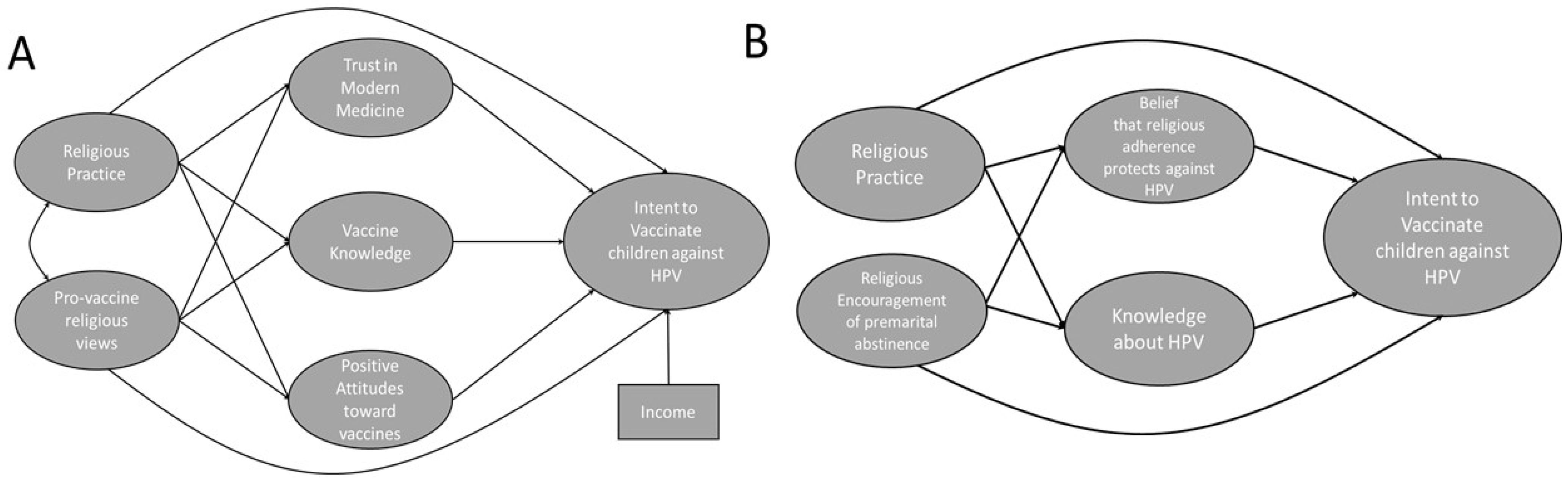
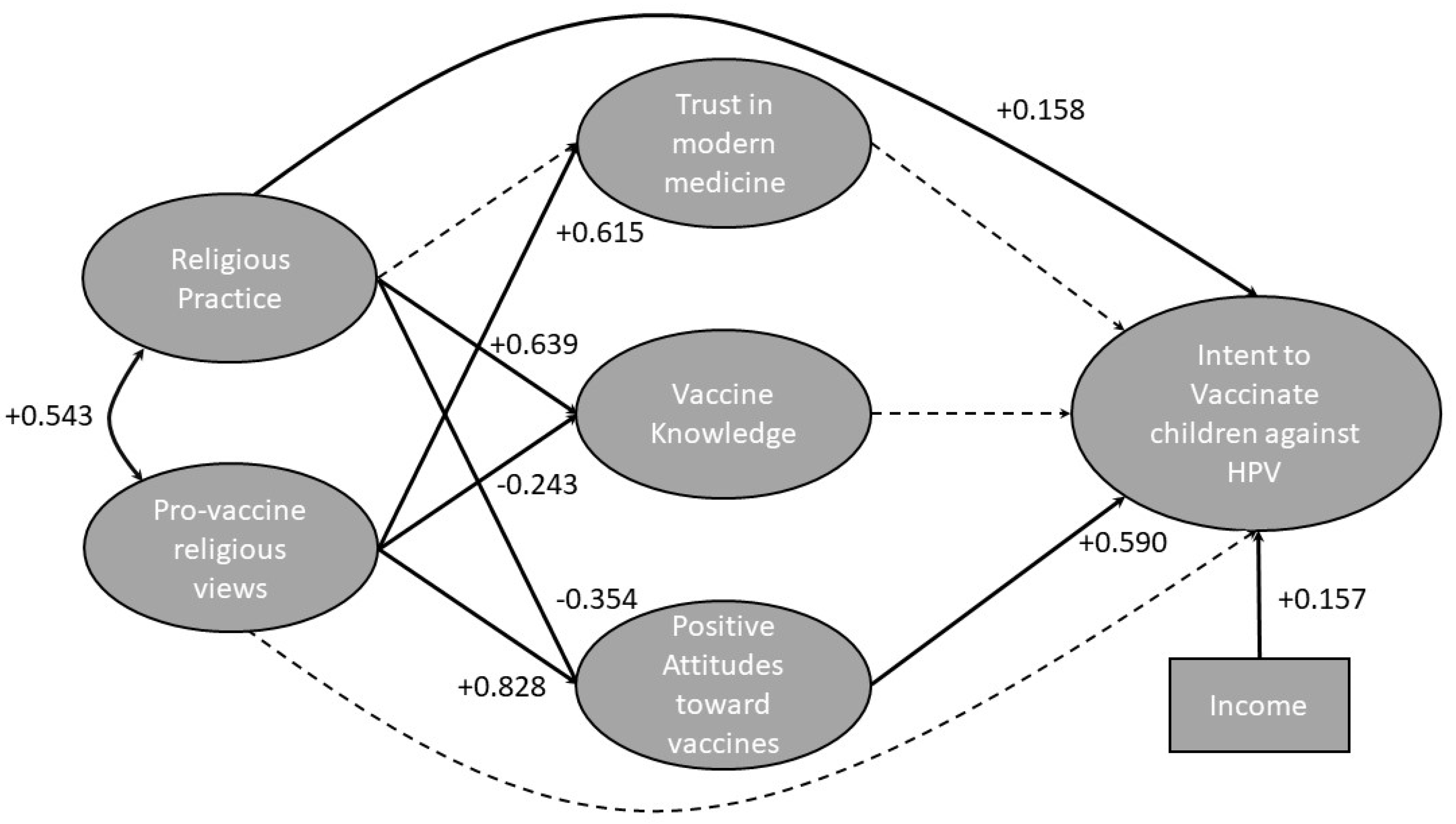
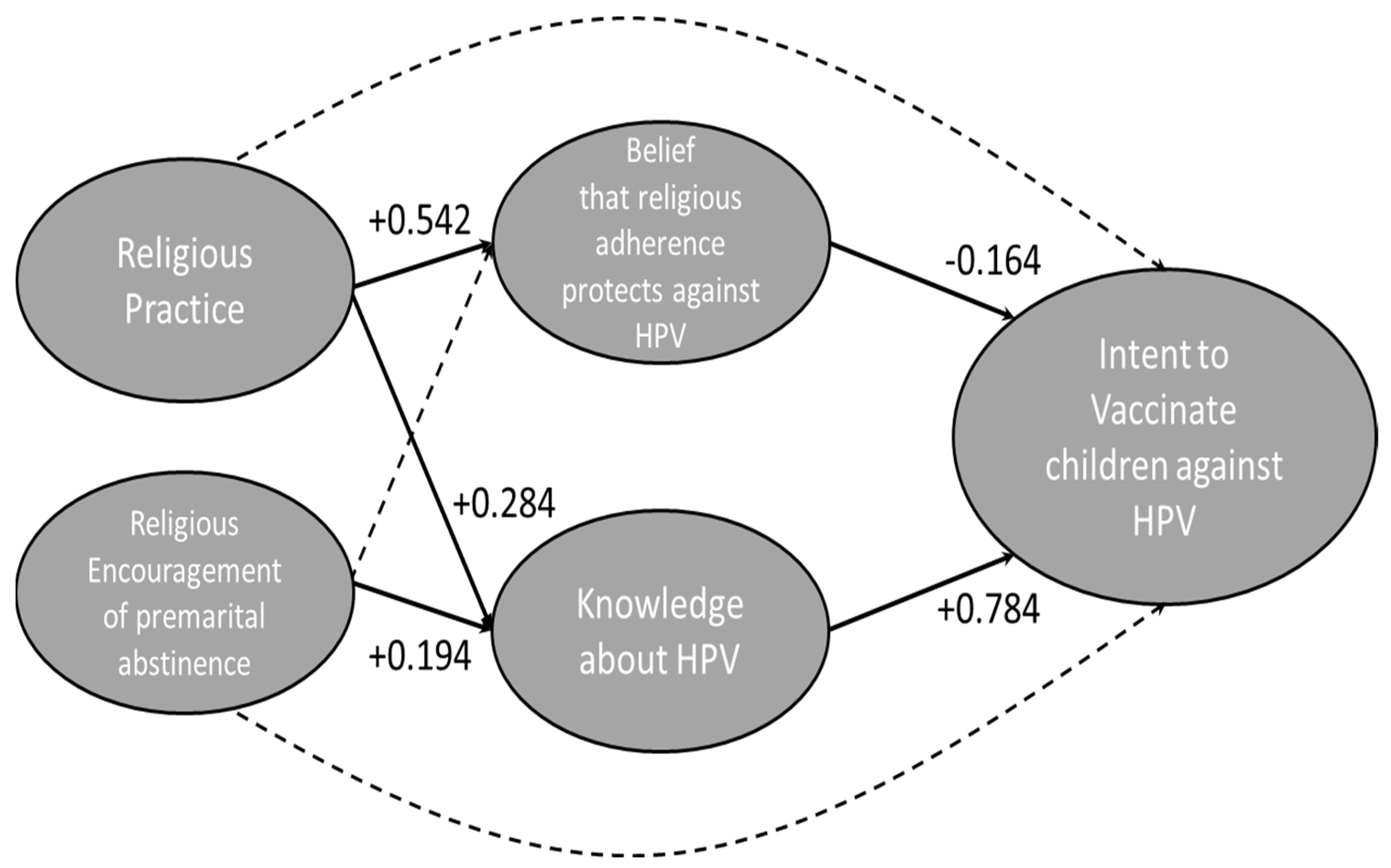
3.3. Structural Equation Modeling
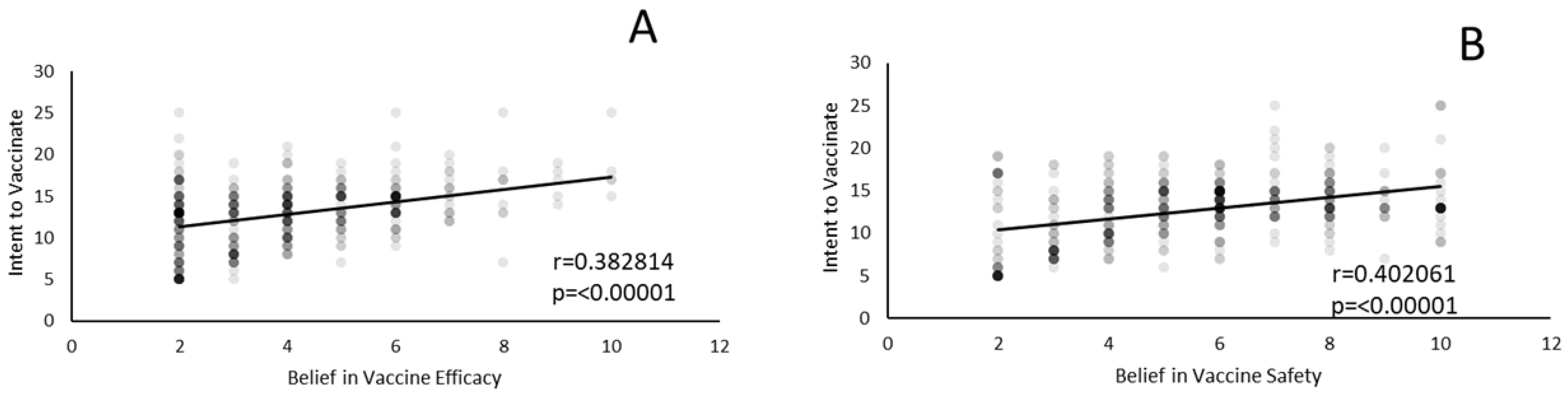
3.4. Univariate Factor Analysis
4. Discussion
4.1. Future Directions
4.2. Strengths/Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brianti, P.; De Flammineis, E.; Mercuri, S.R. Review of HPV-related diseases and cancers. New Microbiol. 2017, 40, 80–85. [Google Scholar]
- Braaten, K.P.; Laufer, M.R. Human Papillomavirus (HPV), HPV-Related Disease, and the HPV Vaccine. Rev. Obs. Gynecol. 2008, 1, 2–10. [Google Scholar]
- McMurray, H.; Nguyen, D.; Westbrook, T.F.; Mcance, D.J. Biology of human papillomaviruses. Int. J. Exp. Pathol. 2001, 82, 15–33. [Google Scholar] [CrossRef] [PubMed]
- Phillips, A.; Patel, C.; Pillsbury, A.; Brotherton, J.; Macartney, K. Safety of Human Papillomavirus Vaccines: An Updated Review. Drug Saf. 2017, 41, 329–346. [Google Scholar] [CrossRef]
- Meites, E.; Szilagyi, P.G.; Chesson, H.W.; Unger, E.R.; Romero, J.R.; Markowitz, L.E. Human Papillomavirus Vaccination for Adults: Updated Recommendations of the Advisory Committee on Immunization Practices. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 698–702. [Google Scholar] [CrossRef] [Green Version]
- Markowitz, L.E.; Dunne, E.F.; Saraiya, M.; Lawson, H.W.; Chesson, H.; Unger, E.R.; Centers for Disease Control and Prevention (CDC); Advisory Committee on Immunization Practices (ACIP). Quadrivalent Human Papillomavirus Vaccine: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm. Rep. 2007, 56, 1–24. [Google Scholar]
- Lin, X.; Rodgers, L.; Zhu, L.; Stokley, S.; Meites, E.; Markowitz, L.E. Human papillomavirus vaccination coverage using two-dose or three-dose schedule criteria. Vaccine 2017, 35, 5759–5761. [Google Scholar] [CrossRef]
- Berenson, A.B.; Laz, T.H.; Rahman, M. Reduction in Vaccine-Type Human Papillomavirus Prevalence Among Women in the United States, 2009–2012. J. Infect. Dis. 2016, 214, 1961–1964. [Google Scholar] [CrossRef]
- Canfell, K. Towards the global elimination of cervical cancer. Papillomavirus Res. 2019, 8, 100170. [Google Scholar] [CrossRef]
- Fava, J.P.; Colleran, J.; Bignasci, F.; Cha, R.; Kilgore, P.E. Adolescent human papillomavirus vaccination in the United States: Opportunities for integrating pharmacies into the immunization neighborhood. Hum. Vaccines Immunother. 2017, 13, 1844–1855. [Google Scholar] [CrossRef]
- Reagan-Steiner, S.; Yankey, D.; Jeyarajah, J.; Elam-Evans, L.D.; Singleton, J.A.; Curtis, C.R.; MacNeil, J.; Markowitz, L.E.; Stokley, S. National, Regional, State, and Selected Local Area Vaccination Coverage Among Adolescents Aged 13–17 Years—United States, 2015. MMWR Morb. Mortal. Wkly. Rep. 2016, 65, 850–858. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.M.; Mott, N.; Clark, S.J.; Harper, D.M.; Shuman, A.G.; Prince, M.E.P.; Dossett, L.A. HPV Vaccination Among Young Adults in the US. JAMA 2021, 325, 1673–1674. [Google Scholar] [CrossRef] [PubMed]
- Best, A.L.; Thompson, E.L.; Adamu, A.M.; Logan, R.; Delva, J.; Thomas, M.; Cunningham, E.; Vamos, C.; Daley, E. Examining the Influence of Religious and Spiritual Beliefs on HPV Vaccine Uptake Among College Women. J. Relig. Health 2019, 58, 2196–2207. [Google Scholar] [CrossRef] [PubMed]
- Bernat, D.H.; Gerend, M.A.; Chevallier, K.; Zimmerman, M.A.; Bauermeister, J.A. Characteristics associated with initiation of the human papillomavirus vaccine among a national sample of male and female young adults. J. Adolesc. Health 2013, 53, 630–636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bodson, J.; Wilson, A.; Warner, E.L.; Kepka, D. Religion and HPV vaccine-related awareness, knowledge, and receipt among insured women aged 18-26 in Utah. PLoS ONE 2017, 12, e0183725. [Google Scholar] [CrossRef] [Green Version]
- Shelton, R.C.; Snavely, A.C.; De Jesus, M.; Othus, M.D.; Allen, J.D. HPV vaccine decision-making and acceptance: Does religion play a role? J. Relig. Health 2013, 52, 1120–1130. [Google Scholar] [CrossRef] [Green Version]
- Thomas, T.; Blumling, A.; Delaney, A. The Influence of Religiosity and Spirituality on Rural Parents’ Health Decision Making and Human Papillomavirus Vaccine Choices. Adv. Nurs. Sci. 2015, 38, E1–E12. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 4th ed.; The Guilford Press: New York, NY, USA, 2015; 534p. [Google Scholar]
- MacCallum, R.C.; Widaman, K.F.; Zhang, S.; Hong, S. Sample size in factor analysis. Psychol. Methods 1999, 4, 84. [Google Scholar] [CrossRef]
- Ogueji, I.A.; Adejumo, A.O. Perceived HIV stigmatization and association with cervical screening adoption among HIV-positive women in a Nigerian Secondary Health Facility: Implications for psychological interventions. J. HIV/AIDS Soc. Serv. 2022, 21, 17–26. [Google Scholar] [CrossRef]
- Ogueji, I.A.; Okoloba, M.M. Underlying factors in the willingness to receive and barriers to receiving the COVID-19 vaccine among residents in the UK and Nigeria: A qualitative study. Curr. Psychol. 2022, 1–12. [Google Scholar] [CrossRef]
- Gallè, F.; Sabella, E.A.; Roma, P.; Da Molin, G.; Diella, G.; Montagna, M.T.; Ferracuti, S.; Liguori, G.; Orsi, G.B.; Napoli, C. Acceptance of COVID-19 Vaccination in the Elderly: A Cross-Sectional Study in Southern Italy. Vaccines 2021, 9, 1222. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Range | Number | Percent of Total Responses |
|---|---|---|
| Age (n = 442) | ||
| 18–25 | 38 | 8.60% |
| 26–35 | 170 | 38.45% |
| 36–45 | 173 | 39.14% |
| 46–55 | 37 | 8.37% |
| Over 55 | 24 | 5.43% |
| Gender (n = 422) | ||
| Male | 175 | 39.60% |
| Female | 267 | 60.4% |
| Non-binary/third gender | 0 | 0% |
| Prefer not to answer | 0 | 0% |
| Race/Ethnicity (n= 442) | ||
| American Indian/Alaska Native | 3 | 0.67% |
| Asian | 12 | 2.67% |
| Black/African American | 40 | 8.91% |
| Hispanic/Latino | 25 | 5.57% |
| Native Hawaiian/Pacific Islander | 0 | 0 |
| White | 368 | 81.96% |
| Prefer not to answer | 1 | 0.22% |
| Marital status (n = 442) | ||
| Single | 54 | 12.22% |
| Partnered | 332 | 75.11% |
| Married | 19 | 4.30% |
| Divorced | 7 | 1.58% |
| Widow/widower | 30 | 6.79% |
| Number of Children (n = 442) | ||
| One | 130 | 29.41% |
| Two | 220 | 49.77% |
| More than Two | 92 | 20.81% |
| Education (n = 442) | ||
| Have not finished high school | 12 | 2.71% |
| Finished high school | 115 | 26.02% |
| Some college | 79 | 17.87% |
| Associate degree | 53 | 12.00% |
| Bachelor’s degree | 84 | 19.00% |
| Post-baccalaureate | 99 | 22.40% |
| Income (n = 442) | ||
| Less than $5000 | 14 | 3.17% |
| $5000–$9999 | 7 | 1.58% |
| $10,000–$14,999 | 14 | 3.17% |
| $15,000–$19,999 | 11 | 2.49% |
| $20,000–$29,000 | 43 | 9.72% |
| $30,000–$39,999 | 36 | 8.14% |
| $40,000–$49,999 | 32 | 7.24% |
| $50,000–$59,999 | 38 | 8.60% |
| $60,000–$74,999 | 39 | 8.82% |
| $75,000–$99,999 | 55 | 12.42% |
| $100,000–$124,999 | 49 | 11.09% |
| $125,000–$149,999 | 48 | 10.86% |
| $150,000 or more | 56 | 12.67% |
| Specific Christian religious affiliation (n = 442) | ||
| Anglican/Episcopalian | 4 | 0.90% |
| Baptist | 58 | 13.12% |
| Catholic | 136 | 30.77% |
| Christian (non-denominational) | 172 | 38.91% |
| Church of Christ/Disciples of Christ | 7 | 1.83% |
| Congregational | 3 | 0.68% |
| Jehovah’s Witness | 4 | 0.90% |
| LDS (Mormon) | 3 | 0.68% |
| Lutheran | 4 | 0.90% |
| Methodist/Wesleyan | 7 | 1.58% |
| Orthodox (Eastern) | 4 | 0.90% |
| Pentecostal/Charismatic | 15 | 3.39% |
| Protestant (other) | 20 | 4.52% |
| Reformed/Presbyterian | 2 | 0.45% |
| Seventh-day Adventist | 1 | 0.23% |
| Other | 2 | 0.45% |
| Model (Latent Variables) | TLI | CFI | RMSEA | SRMR | Chi-Square Test | ||
|---|---|---|---|---|---|---|---|
| χ2 | df | p-Value | |||||
| Model A (religious practice, pro-vaccine religious views, trust in modern medicine, vaccine knowledge, positive attitudes toward vaccines, and intent to vaccinate) | 0.948 | 0.955 | 0.041 | 0.055 | 5321.84 | 351 | <0.001 |
| Model B (religious practice, religious encouragement of premarital abstinence, beliefs that religious adherence protects against HPV, HPV knowledge, and intent to vaccinate) | 0.927 | 0.938 | 0.058 | 0.065 | 4455.42 | 210 | <0.001 |
| Model for the remaining variables (religious influence, religious hope, parent/peer influence on sexual behavior, fear of HPV vaccine side-effects) | 0.966 | 0.973 | 0.041 | 0.045 | 2699.05 | 120 | <0.001 |
| Combined model | 0.902 | 0.911 | 0.042 | 0.065 | 13,280.52 | 1485 | <0.001 |
| Model (Latent Variables) | TLI | CFI | RMSEA | SRMR | Chi-Square Test | ||
|---|---|---|---|---|---|---|---|
| χ2 | df | p-Value | |||||
| Model A | 0.939 | 0.946 | 0.043 | 0.061 | 5531.44 | 378 | <0.001 |
| Model B | 0.927 | 0.939 | 0.058 | 0.065 | 4455.42 | 210 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Redd, D.S.; Jensen, J.L.; Hughes, S.J.; Pogue, K.; Sloan-Aagard, C.D.; Miner, D.S.; Altman, J.D.; Crook, T.B.; Zentz, L.; Bodily, R.J.; et al. Effects of Religious Practice and Teachings about Sexual Behavior on Intent to Vaccinate against Human Papillomavirus. Vaccines 2022, 10, 397. https://doi.org/10.3390/vaccines10030397
Redd DS, Jensen JL, Hughes SJ, Pogue K, Sloan-Aagard CD, Miner DS, Altman JD, Crook TB, Zentz L, Bodily RJ, et al. Effects of Religious Practice and Teachings about Sexual Behavior on Intent to Vaccinate against Human Papillomavirus. Vaccines. 2022; 10(3):397. https://doi.org/10.3390/vaccines10030397
Chicago/Turabian StyleRedd, David S., Jamie L. Jensen, Savannah J. Hughes, Kendall Pogue, Chantel D. Sloan-Aagard, Dashiell S. Miner, Jessica D. Altman, Triston B. Crook, Lydia Zentz, Ruth J. Bodily, and et al. 2022. "Effects of Religious Practice and Teachings about Sexual Behavior on Intent to Vaccinate against Human Papillomavirus" Vaccines 10, no. 3: 397. https://doi.org/10.3390/vaccines10030397