
Influenza Vaccination Uptake in the General Italian Population during the 2020–2021 Flu Season: Data from the EPICOVID-19 Online Web-Based Survey

 , ,
, ,  , , , , , , and
on behalf of EPICOVID19
, , , , , , and
on behalf of EPICOVID19
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Data Collection and Variables
2.3. Statistical Analysis
2.4. Ethics and Consent Form
3. Results
3.1. Characteristics of Respondents
3.2. Vaccination Coverage According to the Different Italian Regions
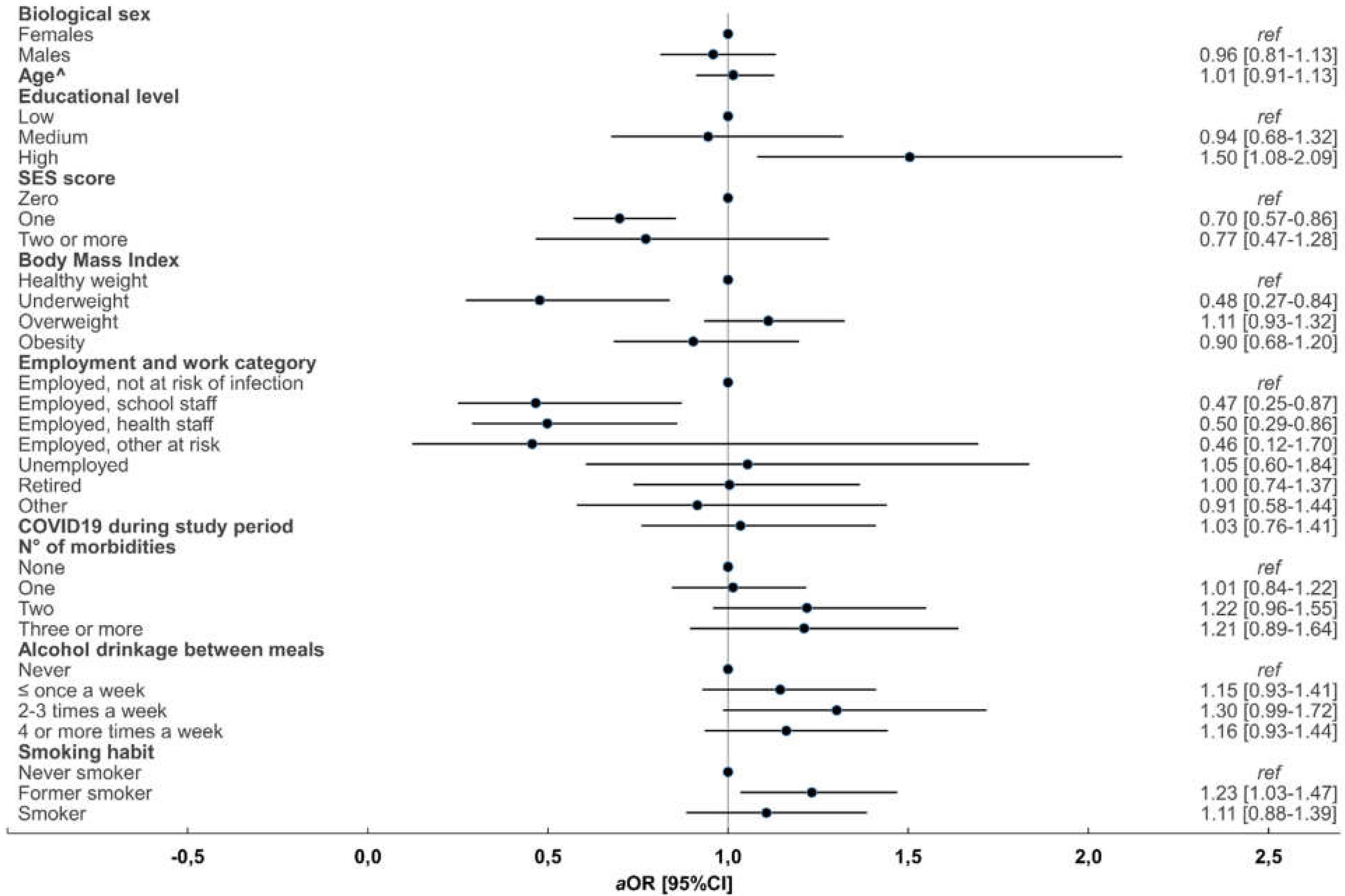
3.3. Factors Associated with Flu Vaccine Uptake during the 2019/2020 and 2020/2021 Flu Seasons
4. Discussion
Study Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Demicheli, V.; Jefferson, T.; Di Pietrantonj, C.; Ferroni, E.; Thorning, S.; Thomas, R.E.; Rivetti, A. Vaccines for preventing influenza in the elderly. Cochrane Database Syst. Rev. 2018, 2, CD004876. [Google Scholar] [PubMed] [Green Version]
- Jefferson, T.; Rivetti, A.; Di Pietrantonj, C.; Demicheli, V. Vaccines for preventing influenza in healthy children. Cochrane Database Syst. Rev. 2018, 2, CD004879. [Google Scholar] [CrossRef] [PubMed]
- Demicheli, V.; Jefferson, T.; Ferroni, E.; Rivetti, A.; Di Pietrantonj, C. Vaccines for preventing influenza in healthy adults. Database Syst. Rev. 2018, 2, CD001269. [Google Scholar] [CrossRef] [PubMed]
- Demurtas, J.; Celotto, S.; Beaudart, C.; Sanchez-Rodriguez, D.; Balci, C.; Soysal, P.; Solmi, M.; Celotto, D.; Righi, E.; Smith, L.; et al. The efficacy and safety of influenza vaccination in older people: An umbrella review of evidence from meta-analyses of both observational and randomized controlled studies. Ageing Res. Rev. 2020, 62, 101118. [Google Scholar] [CrossRef] [PubMed]
- Giacchetta, I.; Primieri, C.; Cavalieri, R.; Domnich, A.; de Waure, C. The burden of seasonal influenza in Italy: A systematic review of influenza-related complications, hospitalizations, and mortality. Influenza Other Respir. Viruses 2022, 16, 351–365. [Google Scholar] [CrossRef] [PubMed]
- Pezzotti, P.; Marchetti, S.; Ricciardi, W.; Rizzo, C. Investigating the impact of influenza on excess mortality in all ages in Italy during recent seasons (2013/14-2016/17 seasons). Int. J. Infect. Dis. 2019, 88, 127–134. [Google Scholar] [CrossRef] [Green Version]
- Barriers of Influenza Vaccination Intention and Behavior: A Systematic Review of Influenza Vaccine Hesitancy 2005–2016. Available online: https://apps.who.int/iris/handle/10665/251671 (accessed on 26 October 2021).
- Influenza vaccination coverage and effectiveness. Available online: https://www.euro.who.int/en/health-topics/communicable-diseases/influenza/vaccination/influenza-vaccination-coverage-and-effectiveness (accessed on 26 October 2021).
- Italian Influenza Vaccination Coverage National Data. Available online: http://www.salute.gov.it/portale/influenza/dettaglioContenutiInfluenza.jsp?lingua=italiano&id=679&area=influenza&menu=vuoto (accessed on 25 October 2021).
- Le Vaccinazioni in Italia. Available online: https://www.epicentro.iss.it/vaccini/dati_Ita#flu (accessed on 25 October 2021).
- Mezencev, R.; Klement, C.; Dluholucký, S. Potential problem of the co-occurrence of pandemic COVID-19 and seasonal influenza. Epidemiol. Mikrobiol. Imunol. 2021, 70, 68–71. [Google Scholar]
- Zipfel, C.M.; Colizza, V.; Bansal, S. The missing season: The impacts of the COVID-19 pandemic on influenza. Vaccine 2021, 39, 3645–3648. [Google Scholar] [CrossRef]
- Iacobucci, G. COVID-19: Risk of death more than doubled in people who also had flu, English data show. BMJ 2020, 370, m3720. [Google Scholar] [CrossRef]
- Noale, M.; Trevisan, C.; Maggi, S.; Antonelli Incalzi, R.; Pedone, C.; Di Bari, M.; Adorni, F.; Jesuthasan, N.; Sojic, A.; Galli, M.; et al. The Association between Influenza and Pneumococcal Vaccinations and SARS-Cov-2 Infection: Data from the EPICOVID19 Web-Based Survey. Vaccines 2020, 8, 471. [Google Scholar] [CrossRef]
- Marín-Hernández, D.; Schwartz, R.E.; Nixon, D.F. Epidemiological evidence for association between higher influenza vaccine uptake in the elderly and lower COVID-19 deaths in Italy. J. Med. Virol. 2021, 93, 64–65. [Google Scholar] [CrossRef] [PubMed]
- Conlon, A.; Ashur, C.; Washer, L.; Eagle, K.A.; Hofmann Bowman, M.A. Impact of the influenza vaccine on COVID-19 infection rates and severity. Am. J. Infect. Control 2021, 49, 694–700. [Google Scholar] [CrossRef] [PubMed]
- Fink, G.; Orlova-Fink, N.; Schindler, T.; Grisi, S.; Ferrer, A.P.S.; Daubenberger, C.; Brentani, A. Inactivated trivalent influenza vaccination is associated with lower mortality among patients with COVID-19 in Brazil. BMJ Evid.-Based Med. 2021, 26, 192–193. [Google Scholar] [CrossRef] [PubMed]
- Flu and Flu vaccination FAQ. Available online: https://www.salute.gov.it/portale/gard/dettaglioFaqGard.jsp?lingua=italiano&id=103 (accessed on 24 November 2021).
- Italian flu vaccination coverage 2020/2021. Available online: https://www.salute.gov.it/portale/news/p3_2_1_1_1.jsp?lingua=italiano&menu=notizie&p=dalministero&id=5548 (accessed on 26 October 2021).
- Boots suspends flu vaccinations for under 65s as pharmacies report huge demand. Available online: https://pharmaceutical-journal.com/article/news/boots-suspends-flu-vaccinations-for-under-65s-as-pharmacies-report-huge-demand (accessed on 26 October 2021).
- Del Riccio, M.; Lina, B.; Caini, S.; Staadegaard, L.; Wiegersma, S.; Kynčl, J.; Combadière, B.; MacIntyre, C.R.; Paget, J. Letter to the editor: Increase of influenza vaccination coverage rates during the COVID-19 pandemic and implications for the upcoming influenza season in northern hemisphere countries and Australia. Eurosurveillance 2021, 26, 2101143. [Google Scholar] [CrossRef] [PubMed]
- Flu vaccine shortage: Time to prioritise. Available online: https://www.vaccinestoday.eu/stories/flu-vaccine-shortages-time-to-prioritise/ (accessed on 4 February 2022).
- Adorni, F.; Jesuthasan, N.; Perdixi, E.; Sojic, A.; Giacomelli, A.; Noale, M.; Trevisan, C.; Franchini, M.; Pieroni, S.; Cori, L.; et al. Epidemiology of SARS-CoV-2 Infection in Italy Using Real-World Data: Methodology and Cohort Description of the Second Phase of Web-Based EPICOVID19 Study. Int. J. Environ. Res. Public Health 2022, 19, 1274. [Google Scholar] [CrossRef]
- Townsend, P.; Phillimore, P.; Beattie, A. Health and Deprivation: Inequality and the North; Croom Helm: London, UK, 1988. [Google Scholar]
- Italian Vaccine Day 27 December 2020. Available online: https://www.salute.gov.it/portale/nuovocoronavirus/dettaglioVideoNuovoCoronavirus.jsp?lingua=english&menu=multimedia&p=video&id=2286 (accessed on 2 November 2021).
- Cori, L.; Curzio, O.; Adorni, F.; Prinelli, F.; Noale, M.; Trevisan, C.; Fortunato, L.; Giacomelli, A.; Bianchi, F. Fear of COVID-19 for Individuals and Family Members: Indications from the National Cross-Sectional Study of the EPICOVID19 Web-Based Survey. Int. J. Environ. Res. Public Health 2021, 18, 3248. [Google Scholar] [CrossRef]
- Castro-Sánchez, E.; Mena-Tudela, D.; Soriano-Vidal, F.J.; Vila-Candel, R. Health literacy: A crucial determinant of vaccination decision-making. Int. J. Infect. Dis. 2020, 97, 202–203. [Google Scholar] [CrossRef]
- Zhang, F.; Or, P.P.; Chung, J.W. The effects of health literacy in influenza vaccination competencies among community-dwelling older adults in Hong Kong. BMC Geriatr. 2020, 20, 103. [Google Scholar] [CrossRef]
- Italian health care workers ISTAT. Available online: http://dati.istat.it/Index.aspx?DataSetCode=DCIS_PERS_SANIT (accessed on 4 February 2022).
- Montalti, M.; Di Valerio, Z.; Rallo, F.; Squillace, L.; Costantino, C.; Tomasello, F.; Mauro, G.L.; Stillo, M.; Perrone, P.; Resi, D.; et al. Attitudes toward the SARS-CoV-2 and Influenza Vaccination in the Metropolitan Cities of Bologna and Palermo, Italy. Vaccines 2021, 9, 1200. [Google Scholar] [CrossRef]
- Domnich, A.; Grassi, R.; Fallani, E.; Spurio, A.; Bruzzone, B.; Panatto, D.; Marozzi, B.; Cambiaggi, M.; Vasco, A.; Orsi, A.; et al. Changes in Attitudes and Beliefs Concerning Vaccination and Influenza Vaccines between the First and Second COVD-19 Pandemic Waves: A Longitudinal Study. Vaccines 2021, 9, 1016. [Google Scholar] [CrossRef]
- Schmid, P.; Rauber, D.; Betsch, C.; Lidolt, G.; Denker, L. Barriers of Influenza Vaccination Intention and Behavior—A Systematic Review of Influenza Vaccine Hesitancy, 2005–2016. PLoS ONE 2017, 12, 2005–2016. [Google Scholar] [CrossRef] [PubMed]
- Yuen, C.Y.S.; Tarrant, M. Determinants of uptake of influenza vaccination among pregnant women—A systematic review. Vaccine 2014, 32, 4602–4613. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.; van Hoek, A.J.; Boccia, D.; Thomas, S.L. Lower vaccine uptake amongst older individuals living alone: A systematic review and meta-analysis of social determinants of vaccine uptake. Vaccine 2017, 35, 2315–2328. [Google Scholar] [CrossRef]
- Bachtiger, P.; Adamson, A.; Chow, J.J.; Sisodia, R.; Quint, J.K.; Peters, N.S. The Impact of the COVID-19 Pandemic on the Uptake of Influenza Vaccine: UK-Wide Observational Study. JMIR Public Health Surveill. 2021, 7, e26734. [Google Scholar] [CrossRef] [PubMed]
- Giacomelli, A.; Galli, M.; Maggi, S.; Pagani, G.; Antonelli Incalzi, R.; Pedone, C.; Di Bari, M.; Noale, M.; Trevisan, C.; Bianchi, F.; et al. Missed Opportunities of Flu Vaccination in Italian Target Categories: Insights from the Online EPICOVID 19 Survey. Vaccines 2020, 8, 669. [Google Scholar] [CrossRef] [PubMed]
- Damiani, G.; Federico, B.; Visca, M.; Agostini, F.; Ricciardi, W. The impact of socioeconomic level on influenza vaccination among Italian adults and elderly: A cross-sectional study. Prev. Med. 2007, 45, 373–379. [Google Scholar] [CrossRef]
- Endrich, M.M.; Blank, P.R.; Szucs, T.D. Influenza vaccination uptake and socioeconomic determinants in 11 European countries. Vaccine 2009, 27, 4018–4024. [Google Scholar] [CrossRef]
- MacDonald, N.E.; SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Turhan, Z.; Dilcen, H.Y.; Dolu, İ. The mediating role of health literacy on the relationship between health care system distrust and vaccine hesitancy during COVID-19 pandemic. Curr. Psychol. 2021, 1–10. [Google Scholar] [CrossRef]
- Dadaczynski, K.; Okan, O.; Messer, M.; Leung, A.Y.M.; Rosário, R.; Darlington, E.; Rathmann, K. Digital Health Literacy and Web-Based Information-Seeking Behaviors of University Students in Germany During the COVID-19 Pandemic: Cross-sectional Survey Study. J. Med. Internet Res. 2021, 23, e24097. [Google Scholar] [CrossRef]
- Coupland, C.; Harcourt, S.; Vinogradova, Y.; Smith, G.; Joseph, C.; Pringle, M.; Hippisley-Cox, J. Inequalities in uptake of influenza vaccine by deprivation and risk group: Time trends analysis. Vaccine 2007, 25, 7363–7371. [Google Scholar] [CrossRef] [PubMed]
- Kohlhammer, Y.; Schnoor, M.; Schwartz, M.; Raspe, H.; Schäfer, T. Determinants of influenza and pneumococcal vaccination in elderly people: A systematic review. Public Health 2007, 121, 742–751. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.A.; Moniz, M.H.; Iott, B.; Power, R.; Griggs, J.J. Obesity and the receipt of influenza and pneumococcal vaccination: A systematic review and meta-analysis. BMC Obes. 2016, 3, 24. [Google Scholar] [CrossRef] [Green Version]
- Jiménez-García, R.; Ariñez-Fernandez, M.C.; Garcia-Carballo, M.; Hernández-Barrera, V.; de Miguel, A.G.; Carrasco-Garrido, P. Influenza vaccination coverage and related factors among Spanish patients with chronic obstructive pulmonary disease. Vaccine 2005, 23, 3679–3686. [Google Scholar] [CrossRef] [PubMed]
- Greco, D.; Rizzo, C.; Puzelli, S.; Caraglia, A.; Maraglino, F.; Bella, A. L’impatto dei virus influenzali in Italia nella stagione 2020–2021 durante la pandemia di COVID-19. Boll. Epidemiol. Naz. 2021, 2, 1–6. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Flu Shot in 2019/2020 | NO | YES | NO | YES | Total |
|---|---|---|---|---|---|---|
| Flu Shot in 2020/2021 | NO | NO | YES | YES | ||
| n (%) | n (%) | n (%) | n (%) | |||
| Sex at birth | Male | 8513 (37.5) | 630 (39.5) | 3242 (38.9) | 3942 (44.7) | 16,327 (39.4) |
| Female | 14,197 (62.5) | 966 (60.5) | 5097 (61.1) | 4886 (55.3) | 25,146 (60.6) | |
| Age class at first interview | 18–59 | 19,776 (87.1) | 1375 (86.2) | 5240 (62.8) | 4090 (46.3) | 30,481 (73.5) |
| 60–64 | 1857 (8.2) | 125 (7.8) | 1473 (17.7) | 1282 (14.5) | 4737 (11.4) | |
| 65+ | 1077 (4.7) | 96 (6.0) | 1626 (19.5) | 3456 (39.1) | 6255 (15.1) | |
| Educational level ± | Low | 747 (3.3) | 44 (2.8) | 245 (2.9) | 345 (3.9) | 1381 (3.3) |
| Medium | 7479 (32.9) | 461 (28.9) | 2504 (30.0) | 2490 (28.2) | 12,934 (31.2) | |
| High | 14,484 (63.8) | 1091 (68.4) | 5590 (67.0) | 5993 (67.9) | 27,158 (65.5) | |
| Employment and work category at risk of infection | Employed, not at risk | 11,980 (52.8) | 806 (50.5) | 3409 (40.9) | 2378 (26.9) | 18,573 (44.8) |
| Employed, school staff | 2150 (9.5) | 163 (10.2) | 714 (8.6) | 626 (7.1) | 3653 (8.8) | |
| Employed, health staff | 1292 (5.7) | 121 (7.6) | 972 (11.7) | 1138 (12.9) | 3523 (8.5) | |
| Employed, other at risk | 1228 (5.4) | 70 (4.4) | 334 (4.0) | 206 (2.3) | 1838 (4.4) | |
| Unemployed | 1724 (7.6) | 101 (6.3) | 419 (5.0) | 402 (4.6) | 2646 (6.4) | |
| Students | 1045 (4.6) | 96 (6.0) | 147 (1.8) | 145 (1.6) | 1433 (3.5) | |
| Retired | 1474 (6.5) | 125 (7.8) | 1835 (22.0) | 3457 (39.2) | 6891 (16.6) | |
| Other | 1817 (8.0) | 114 (7.1) | 509 (6.1) | 476 (5.4) | 2916 (7.0) | |
| COVID-19 ¶ during study period | 2504 (11.0) | 237 (14.8) | 811 (9.7) | 859 (9.7) | 4411 (10.6) | |
| N° of morbidities | None | 15,708 (69.2) | 1046 (65.5) | 4861 (58.3) | 4414 (50.0) | 26,029 (62.8) |
| One | 4737 (20.9) | 360 (22.6) | 2141 (25.7) | 2357 (26.7) | 9595 (23.1) | |
| Two | 1551 (6.8) | 133 (8.3) | 860 (10.3) | 1261 (14.3) | 3805 (9.2) | |
| Three or more | 714 (3.1) | 57 (3.6) | 477 (5.7) | 796 (9.0) | 2044 (4.9) | |
| Smoker | No | 13,257 (58.4) | 1000 (62.7) | 4671 (56.0) | 4990 (56.5) | 23,918 (57.7) |
| Former smoker | 4818 (21.2) | 358 (22.4) | 2214 (26.5) | 2693 (30.5) | 10,083 (24.3) | |
| Smoker | 4635 (20.4) | 238 (14.9) | 1454 (17.4) | 1145 (13.0) | 7472 (18.0) | |
| Alcohol drinking between meals | Never | 3918 (17.3) | 286 (17.9) | 1608 (19.3) | 1970 (22.3) | 7782 (18.8) |
| ≤once a week | 10,329 (45.5) | 743 (46.6) | 3615 (43.4) | 3485 (39.5) | 18,172 (43.8) | |
| 2–3 times a week | 4526 (19.9) | 284 (17.8) | 1420 (17.0) | 1347 (15.3) | 7577 (18.3) | |
| 4 or more times a week | 3937 (17.3) | 283 (17.7) | 1696 (20.3) | 2026 (22.9) | 7942 (19.1) | |
| SES score * | 0 | 12,591 (55.4) | 960 (60.2) | 5550 (66.6) | 6272 (71.0) | 25,373 (61.2) |
| 1 | 8133 (35.8) | 516 (32.3) | 2378 (28.5) | 2216 (25.1) | 13,243 (31.9) | |
| 2 | 1781 (7.8) | 111 (7.0) | 385 (4.6) | 320 (3.6) | 2597 (6.3) | |
| 3–4 | 205 (0.9) | 9 (0.6) | 26 (0.3) | 20 (0.2) | 260 (0.6) | |
| BMI | Healthy weight (18–24) | 13,702 (60.3) | 917 (57.5) | 4621 (55.4) | 4700 (53.2) | 23,940 (57.7) |
| Underweight (<18.5) | 827 (3.6) | 77 (4.8) | 219 (2.6) | 203 (2.3) | 1326 (3.2) | |
| Overweight (25–29) | 6069 (26.7) | 451 (28.3) | 2613 (31.3) | 2886 (32.7) | 12,019 (29.0) | |
| Obesity (≥30) | 1841 (8.1) | 131 (8.2) | 765 (9.2) | 913 (10.3) | 3650 (8.8) | |
| Unknown | 271 (1.2) | 20 (1.3) | 121 (1.5) | 126 (1.4) | 538 (1.3) | |
| Total | 22,710 (54.8) | 1596 (3.8) | 8339 (20.1) | 8828 (21.3) | 41,473 (100) |
| Flu Shot in 2019/2020 | YES | NO | YES | ||||
|---|---|---|---|---|---|---|---|
| Flu Shot in 2020/2021 | NO | YES | YES | ||||
| Variables | aOR (95% CI) | p | aOR (95% CI) | p | aOR (95% CI) | p | |
| Sex at birth | Females | 1 | - | 1 | - | 1 | - |
| Males | 1.13 [1.01–1.27] | 0.028 | 1.01 [0.95–1.07] | 0.694 | 1.25 [1.18–1.33] | 0.000 | |
| Age class at first survey | 18–59 | 1 | - | 1 | - | 1 | - |
| 60–64 | 0.92 [0.74–1.14] | 0.447 | 2.72 [2.50–2.96] | 0.000 | 2.67 [2.44–2.93] | 0.000 | |
| 65+ | 1.09 [0.79–1.51] | 0.582 | 4.61 [4.07–5.23] | 0.000 | 9.23 [8.18–10.42] | 0.000 | |
| Educational level ± | Low | 1 | - | 1 | - | 1 | - |
| Medium | 1.07 [0.78–1.48] | 0.659 | 1.33 [1.13–1.56] | 0.001 | 1.15 [0.98–1.34] | 0.089 | |
| High | 1.34 [0.98–1.84] | 0.070 | 1.69 [1.44–1.97] | 0.000 | 1.71 [1.46–2.00] | 0.000 | |
| Employment and work category at risk of infection | Employed, not at risk | 1 | - | 1 | - | 1 | - |
| Employed, school staff | 1.10 [0.92–1.31] | 0.309 | 1.04 [0.94–1.14] | 0.437 | 1.30 [1.17–1.44] | 0.000 | |
| Employed, health staff | 1.33 [1.09–1.63] | 0.006 | 2.66 [2.42–2.92] | 0.000 | 4.49 [4.08–4.94] | 0.000 | |
| Employed, other at risk | 0.89 [0.69–1.15] | 0.371 | 1.07 [0.94–1.22] | 0.298 | 0.99 [0.85–1.16] | 0.923 | |
| Unemployed | 1.08 [0.85–1.38] | 0.510 | 0.94 [0.83–1.08] | 0.387 | 1.34 [1.16–1.54] | 0.000 | |
| Students | 1.55 [1.24–1.95] | 0.000 | 0.66 [0.55–0.79] | 0.000 | 1.04 [0.87–1.25] | 0.670 | |
| Retired | 1.19 [0.88–1.60] | 0.264 | 1.24 [1.10–1.39] | 0.000 | 1.88 [1.67–2.11] | 0.000 | |
| Other | 0.97 [0.79–1.19] | 0.761 | 0.85 [0.77–0.95] | 0.004 | 1.06 [0.94–1.19] | 0.360 | |
| COVID19 ¶ during study period | 1.35 [1.17–1.57] | 0.000 | 0.82 [0.75–0.90] | 0.000 | 0.84 [0.77–0.92] | 0.000 | |
| N° of morbidities | None | 1 | - | 1 | - | 1 | - |
| One | 1.14 [1.01–1.30] | 0.035 | 1.32 [1.24–1.41] | 0.000 | 1.48 [1.39–1.58] | 0.000 | |
| Two | 1.32 [1.09–1.59] | 0.005 | 1.51 [1.37–1.66] | 0.000 | 2.12 [1.93–2.33] | 0.000 | |
| Three or more | 1.25 [0.94–1.67] | 0.117 | 1.83 [1.61–2.08] | 0.000 | 2.96 [2.62–3.36] | 0.000 | |
| Smoker | No | 1 | - | 1 | - | 1 | - |
| Former smoker | 0.99 [0.87–1.13] | 0.915 | 1.04 [0.97–1.11] | 0.250 | 0.98 [0.91–1.04] | 0.494 | |
| Smoker | 0.71 [0.62–0.83] | 0.000 | 0.88 [0.81–0.94] | 0.000 | 0.63 [0.58–0.68] | 0.000 | |
| Alcohol drinking between meals | Never | 1 | - | 1 | - | 1 | - |
| ≤ once a week | 0.99 [0.85–1.14] | 0.837 | 1.00 [0.93–1.07] | 0.934 | 0.87 [0.81–0.94] | 0.000 | |
| 2–3 times a week | 0.87 [0.73–1.03] | 0.113 | 0.89 [0.82–0.98] | 0.013 | 0.78 [0.71–0.85] | 0.000 | |
| 4 or more times a week | 1.00 [0.84–1.19] | 0.987 | 0.96 [0.88–1.05] | 0.419 | 0.88 [0.80–0.96] | 0.005 | |
| SES score * | 0 | 1 | - | 1 | - | 1 | - |
| 1 | 0.82 [0.73–0.93] | 0.001 | 0.83 [0.78–0.89] | 0.000 | 0.79 [0.74–0.85] | 0.000 | |
| 2 | 0.81 [0.65–1.02] | 0.068 | 0.68 [0.60–0.77] | 0.000 | 0.59 [0.51–0.67] | 0.000 | |
| 3–4 | 0.59 [0.29–1.18] | 0.136 | 0.42 [0.28–0.65] | 0.000 | 0.33 [0.21–0.54] | 0.000 | |
| BMI | Healthy weight (18.5–24) | 1 | - | 1 | - | 1 | - |
| Underweight (<18.5) | 1.40 [1.10–1.79] | 0.007 | 0.84 [0.72–0.99] | 0.036 | 0.83 [0.70–0.99] | 0.038 | |
| Overweight (25–29) | 1.09 [0.97–1.23] | 0.152 | 1.11 [1.05–1.18] | 0.001 | 1.05 [0.98–1.12] | 0.151 | |
| Obesity (≥30) | 1.03 [0.85–1.25] | 0.740 | 1.08 [0.98–1.19] | 0.114 | 1.09 [0.99–1.21] | 0.083 | |
| Unknown | 1.10 [0.69–1.75] | 0.691 | 1.17 [0.93–1.47] | 0.178 | 1.06 [0.83–1.35] | 0.631 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giacomelli, A.; Galli, M.; Maggi, S.; Noale, M.; Trevisan, C.; Pagani, G.; Antonelli-Incalzi, R.; Molinaro, S.; Bastiani, L.; Cori, L.; et al. Influenza Vaccination Uptake in the General Italian Population during the 2020–2021 Flu Season: Data from the EPICOVID-19 Online Web-Based Survey. Vaccines 2022, 10, 293. https://doi.org/10.3390/vaccines10020293
Giacomelli A, Galli M, Maggi S, Noale M, Trevisan C, Pagani G, Antonelli-Incalzi R, Molinaro S, Bastiani L, Cori L, et al. Influenza Vaccination Uptake in the General Italian Population during the 2020–2021 Flu Season: Data from the EPICOVID-19 Online Web-Based Survey. Vaccines. 2022; 10(2):293. https://doi.org/10.3390/vaccines10020293
Chicago/Turabian StyleGiacomelli, Andrea, Massimo Galli, Stefania Maggi, Marianna Noale, Caterina Trevisan, Gabriele Pagani, Raffaele Antonelli-Incalzi, Sabrina Molinaro, Luca Bastiani, Liliana Cori, and et al. 2022. "Influenza Vaccination Uptake in the General Italian Population during the 2020–2021 Flu Season: Data from the EPICOVID-19 Online Web-Based Survey" Vaccines 10, no. 2: 293. https://doi.org/10.3390/vaccines10020293