
Effectiveness of Vaccination against SARS-CoV-2 Infection in the Pre-Delta Era: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Methods
2.1. Search and Selection
2.2. Data Extraction
2.3. Outcome
2.4. SARS-CoV-2 Infection Episodes
2.5. Experimental Group
2.6. Control Group
2.7. Risk of Bias
2.8. Statistical Analysis
3. Results
3.1. Meta-Analysis
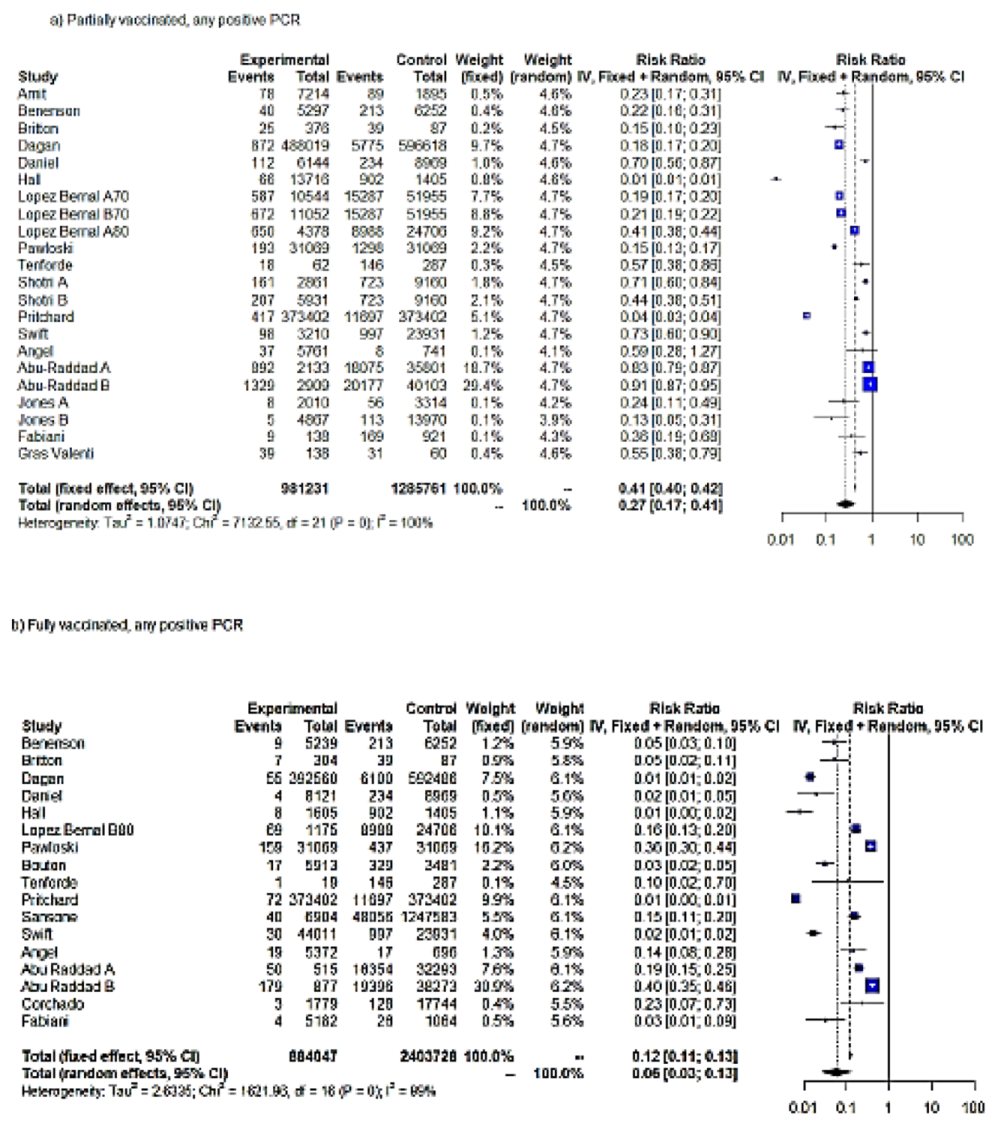
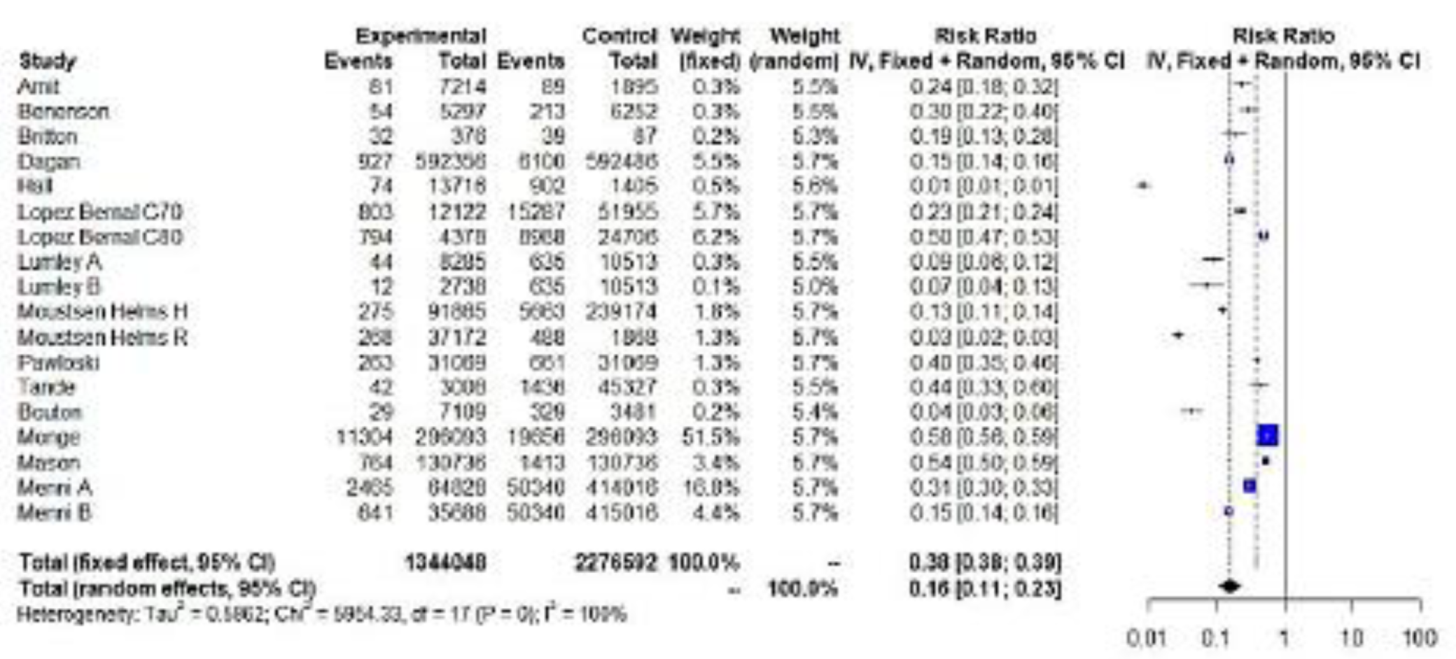
3.1.1. RR of SARS-CoV-2 Infection following Vaccination
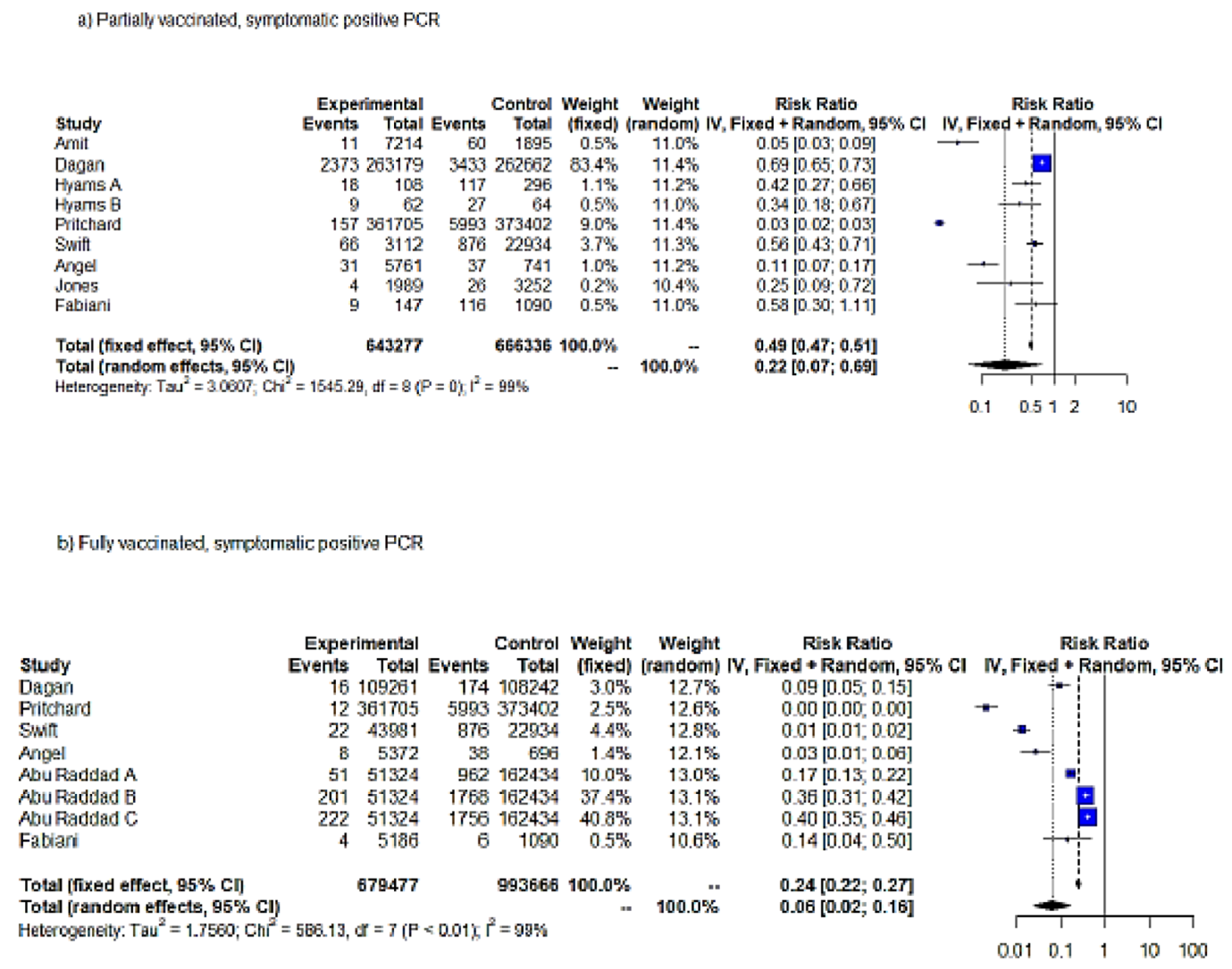
3.1.2. RR of Symptomatic COVID-19 Infection following Vaccination
3.1.3. RR of Hospitalization Risk following Vaccination
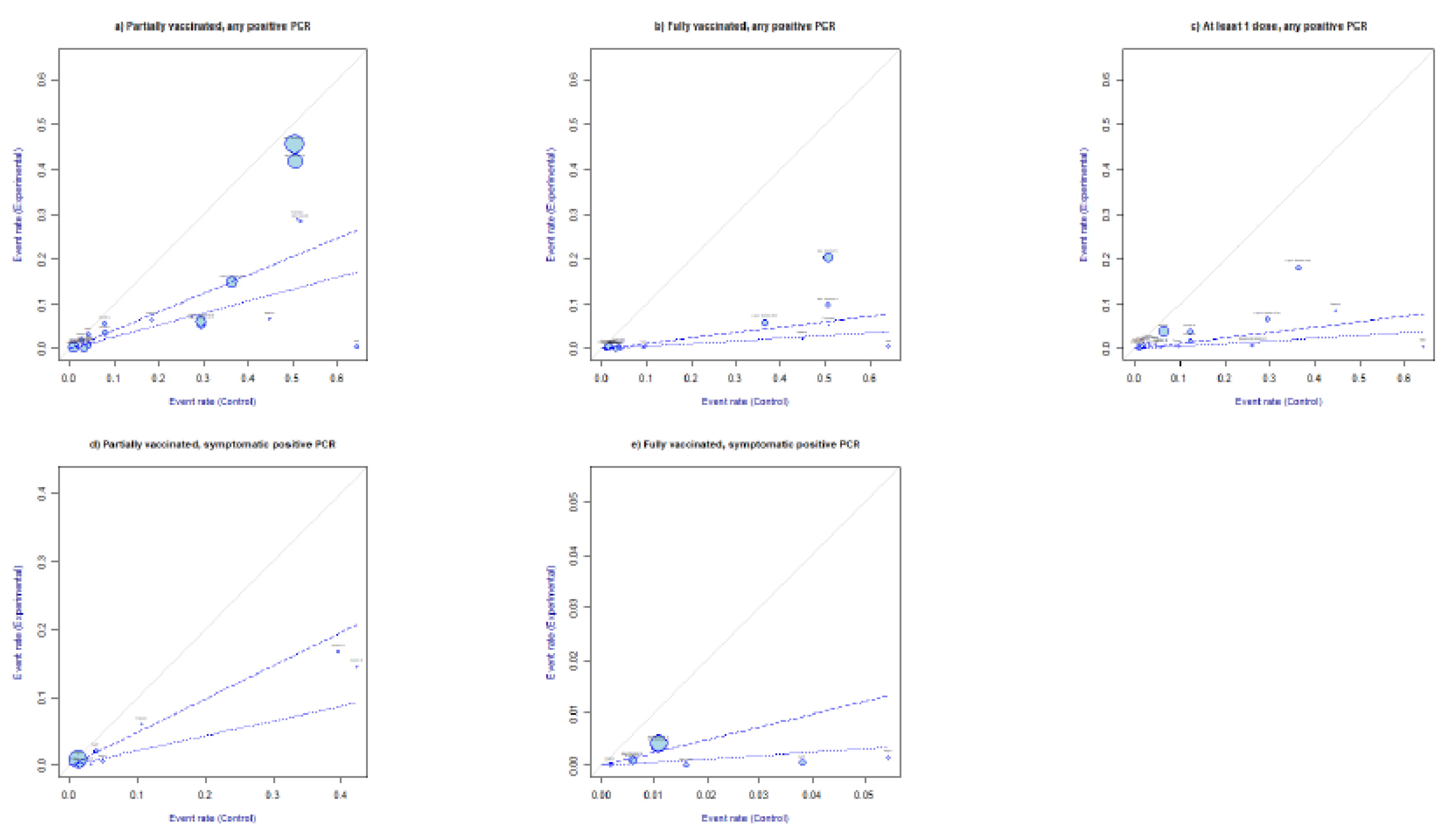
3.1.4. L’ Abbé Plot
3.2. Subgroup Meta-Analysis
3.3. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- COVID19 Database. Available online: https://COVID19.who.int/ (accessed on 13 July 2021).
- Chen, Y.; Liu, Q.; Guo, D. Emerging coronaviruses: Genome structure, replication, and pathogenesis. J. Med. Virol. 2020, 92, 418–423. [Google Scholar] [CrossRef]
- Peng, Y.; Mentzer, A.J.; Liu, G.; Yao, X.; Yin, Z.; Dong, D.; Dejnirattisai, W.; Rostron, T.; Supasa, P.; Liu, C.; et al. Broad and strong memory CD4+ and CD8+ T cells induced by SARS-CoV-2 in UK convalescent individuals following COVID-19. Nat. Immunol. 2020, 21, 1336–1345. [Google Scholar] [CrossRef]
- Ramasamy, M.N.; Minassian, A.M.; Ewer, K.J.; Flaxman, A.L.; Folegatti, P.M.; Owens, D.R.; Voysey, M.; Aley, P.K.; Angus, B.; Babbage, G.; et al. Safety and immunogenicity of ChAdOx1 nCoV-19 vaccine administered in a prime-boost regimen in young and old adults (COV002): A single-blind, randomised, controlled, phase 2/3 trial. Lancet 2021, 396, 1979–1993. [Google Scholar] [CrossRef]
- EMA. Available online: https://www.ema.europa.eu/en/medicines (accessed on 13 July 2021).
- GAVI. Available online: https://www.gavi.org/vaccineswork/what-difference-between-efficacy-and-effectiveness (accessed on 13 July 2021).
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Baden, L.R.; el Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [Green Version]
- Voysey, M.; Clemens, S.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against COVID-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef] [PubMed]
- Rothman, K.J.; Greenland, S.; Lash, T.L. Modern Epidemiology; Wolters Kluwer Health: Philadelphia, PA, USA; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008. [Google Scholar]
- McAloon, C.; Collins, Á.; Hunt, K.; Barber, A.; Byrne, A.W.; Butler, F.; Casey, M.; Griffin, J.; Lane, E.; McEvoy, D.; et al. Incubation period of COVID-19: A rapid systematic review and meta-analysis of observational research. BMJ Open 2020, 10, e039652. [Google Scholar] [CrossRef]
- Peterson, J.; Welch, V.; Losos, M.; Tugwell, P.J. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2011; pp. 1–12. [Google Scholar]
- Higgins, J.P.; Thompson, S.G. Controlling the risk of spurious findings from meta-regression. Stat. Med. 2004, 23, 1663–1682. [Google Scholar] [CrossRef]
- Schwarzer, G.; Carpenter, J.R.; Rücker, G. Meta-Analysis with R; Springer: Cham, Switzerland, 2015. [Google Scholar]
- Viechtbauer, W.; Cheung, M.W. Outlier and influence diagnostics for meta-analysis. Res. Synth. Methods 2010, 1, 112–125. [Google Scholar] [CrossRef]
- Baujat, B.; Mahé, C.; Pignon, J.P.; Hill, C. A graphical method for exploring heterogeneity in meta-analyses: Application to a meta-analysis of 65 trials. Stat. Med. 2002, 21, 2641–2652. [Google Scholar] [CrossRef]
- Olkin, I.; Dahabreh, I.J.; Trikalinos, T.A. GOSH—A graphical display of study heterogeneity. Res. Synth. Methods 2012, 3, 214–223. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Jones, N.K.; Rivett, L.; Seaman, S.; Samworth, R.J.; Warne, B.; Workman, C.; Ferris, M.; Wright, J.; Quinnell, N.; Shaw, A.; et al. Single-dose BNT162b2 vaccine protects against asymptomatic SARS-CoV-2 infection. eLife 2021, 10, e68808. [Google Scholar] [CrossRef]
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Robertson, C.; Stowe, J.; Tessier, E.; Simmons, R.; Cottrell, S.; Roberts, R.; O’Doherty, M.; et al. Effectiveness of the Pfizer-BioNTech and Oxford-AstraZeneca vaccines on COVID-19 related symptoms, hospital admissions, and mortality in older adults in England: Test negative case-control study. BMJ 2021, 373, n1088. [Google Scholar] [CrossRef]
- Shrotri, M.; Krutikov, M.; Palmer, T.; Giddings, R.; Azmi, B.; Subbarao, S.; Fuller, C.; Irwin-Singer, A.; Davies, D.; Tut, G.; et al. Vaccine effectiveness of the first dose of ChAdOx1 nCoV-19 and BNT162b2 against SARS-CoV-2 infection in residents of long-term care facilities in England (VIVALDI): A prospective cohort study. Lancet Infect. Dis. 2021, 21, 1529–1538. [Google Scholar] [CrossRef]
- Moustsen-Helms, I.R.; Emborg, H.D.; Nielsen, J.; Nielsen, K.F.; Krause, T.G.; Molbak, K.; Moeller, K.L.; Berthelsen, A.S.; Valentiner-Branth, P. Vaccine effectiveness after 1st and 2nd dose of the BNT162b2 mRNA COVID-19 Vaccine in long-term care facility residents and healthcare workers—A Danish cohort study. medRxiv 2021. medRxiv:2021.03.08.21252200. [Google Scholar]
- Abu-Raddad, L.J.; Chemaitelly, H.; Butt, A.A. National Study Group for COVID-19 Vaccination. Effectiveness of the BNT162b2 Covid-19 Vaccine against the B.1.1.7 and B.1.351 Variants. N. Engl. J. Med. 2021, 385, 187–189. [Google Scholar] [CrossRef]
- Pritchard, E.; Matthews, P.C.; Stoesser, N.; Eyre, D.W.; Gethings, O.; Vihta, K.D.; Jones, J.; House, T.; VanSteenHouse, H.; Bellet, I.; et al. Impact of vaccination on new SARS-CoV-2 infections in the United Kingdom. Nat. Med. 2021, 27, 1370–1378. [Google Scholar] [CrossRef]
- Pawlowski, C.; Lenehan, P.; Puranik, A.; Agarwal, V.; Venkatakrishnan, A.J.; Niesen, M.; O’Horo, J.C.; Virk, A.; Swift, M.D.; Badley, A.D.; et al. FDA-authorized mRNA COVID-19 vaccines are effective per real-world evidence synthesized across a multi-state health system. MedRxiv 2021, 8, 979–992.e8. [Google Scholar] [CrossRef] [PubMed]
- Bouton, T.C.; Lodi, S.; Turcinovic, J.; Weber, S.E.; Quinn, E.; Korn, C.; Steiner, J.; Schechter-Perkins, E.M.; Duffy, E.; Ragan, E.J.; et al. COVID-19 vaccine impact on rates of SARS-CoV-2 cases and post vaccination strain sequences among healthcare workers at an urban academic medical center: A prospective cohort study. medRxiv 2021. [Google Scholar]
- Tenforde, M.W.; Olson, S.M.; Self, W.H.; Talbot, H.K.; Lindsell, C.J.; Steingrub, J.S.; Shapiro, N.I.; Ginde, A.A.; Douin, D.J.; Prekker, M.E.; et al. Effectiveness of Pfizer-BioNTech and Moderna Vaccines Against COVID-19 Among Hospitalized Adults Aged ≥65 Years—United States, January–March 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 674–679. [Google Scholar] [CrossRef]
- Swift, M.D.; Breeher, L.E.; Tande, A.J.; Tommaso, C.P.; Hainy, C.M.; Chu, H.; Murad, M.H.; Berbari, E.F.; Virk, A. Effectiveness of Messenger RNA Coronavirus Disease 2019 (COVID-19) Vaccines Against Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection in a Cohort of Healthcare Personnel. Clin. Infect. Dis. 2021, 73, e1376–e1379. [Google Scholar] [CrossRef] [PubMed]
- Mason, T.; Whitston, M.; Hodgson, J.; Watkinson, R.E.; Lau, Y.S.; Abdulrazeg, O.; Sutton, M. Effects of BNT162b2 mRNA vaccine on COVID-19 infection and hospitalisation amongst older people: Matched case control study for England. BMC Med. 2021, 19, 275. [Google Scholar] [CrossRef]
- Gras-Valentí, P.; Chico-Sánchez, P.; Algado-Sellés, N.; Jiménez-Sepúlveda, N.J.; Gómez-Sotero, I.L.; Fuster-Pérez, M.; Cartagena-Llopis, L.; Sánchez-Valero, M.; Cerezo-Milán, P.; Martínez-Tornero, I.; et al. Effectiveness of the first dose of BNT162b2 vaccine to preventing COVID-19 in healthcare personnel. Rev. Esp. Salud Publica 2021, 95, e202104070. [Google Scholar] [PubMed]
- Hall, V.J.; Foulkes, S.; Saei, A.; Andrews, N.; Oguti, B.; Charlett, A.; Wellington, E.; Stowe, J.; Gillson, N.; Atti, A.; et al. COVID-19 vaccine coverage in health-care workers in England and effectiveness of BNT162b2 mRNA vaccine against infection (SIREN): A prospective, multicentre, cohort study. Lancet 2021, 397, 1725–1735. [Google Scholar] [CrossRef]
- Britton, A.; Jacobs Slifka, K.M.; Edens, C.; Nanduri, S.A.; Bart, S.M.; Shang, N.; Harizaj, A.; Armstrong, J.; Xu, K.; Ehrlich, H.Y.; et al. Effectiveness of the Pfizer-BioNTech COVID-19 Vaccine Among Residents of Two Skilled Nursing Facilities Experiencing COVID-19 Outbreaks—Connecticut, December 2020–February 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Monge, S.; Olmedo, C.; Alejos, B.; Lapeña, M.F.; Sierra, M.J.; Limia, A. COVID-19 Registries Study Group2. Direct and Indirect Effectiveness of mRNA Vaccination against Severe Acute Respiratory Syndrome Coronavirus 2 in Long-Term Care Facilities, Spain. Emerg. Infect. Dis. 2021, 27, 2595–2603. [Google Scholar] [CrossRef] [PubMed]
- Hyams, C.; Marlow, R.; Maseko, Z.; King, J.; Ward, L.; Fox, K.; Heath, R.; Tuner, A.; Friedrich, Z.; Morrison, L.; et al. Effectiveness of BNT162b2 and ChAdOx1 nCoV-19 COVID-19 vaccination at preventing hospitalisations in people aged at least 80 years: A test-negative, case-control study. Lancet Infect. Dis. 2021, 21, 1539–1548. [Google Scholar] [CrossRef]
- Angel, Y.; Spitzer, A.; Henig, O.; Saiag, E.; Sprecher, E.; Padova, H.; Ben-Ami, R. Association Between Vaccination With BNT162b2 and Incidence of Symptomatic and Asymptomatic SARS-CoV-2 Infections Among Health Care Workers. JAMA 2021, 325, 2457–2465. [Google Scholar] [CrossRef] [PubMed]
- Corchado-Garcia, J.; Zemmour, D.; Hughes, T.; Bandi, H.; Cristea-Platon, T.; Lenehan, P.; Pawlowski, C.; Bade, S.; O’Horo, J.C.; Gores, G.J.; et al. Analysis of the Effectiveness of the Ad26.COV2.S Adenoviral Vector Vaccine for Preventing COVID-19. JAMA Netw. Open 2021, 4, e2132540. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.L.; Wang, Y.Y.; Yang, Z.H.; Huang, D.; Weng, H.; Zeng, X.T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med. Res. 2020, 7, 7. [Google Scholar] [CrossRef] [Green Version]
- Haas, E.J.; Angulo, F.J.; McLaughlin, J.M.; Anis, E.; Singer, S.R.; Khan, F.; Brooks, N.; Smaja, M.; Mircus, G.; Pan, K.; et al. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: An observational study using national surveillance data. Lancet 2021, 397, 1819–1829. [Google Scholar] [CrossRef]
- Lumley, S.F.; Rodger, G.; Constantinides, B.; Sanderson, N.; Chau, K.K.; Street, T.L.; O’Donnell, D.; Howarth, A.; Hatch, S.B.; Marsden, B.D.; et al. An observational cohort study on the incidence of SARS-CoV-2 infection and B.1.1.7 variant infection in healthcare workers by antibody and vaccination status. Clin. Infect. Dis. 2021. advance online publication. [Google Scholar] [CrossRef]
- Menni, C.; Klaser, K.; May, A.; Polidori, L.; Capdevila, J.; Louca, P.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Merino, J.; et al. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID Symptom Study app in the UK: A prospective observational study. Lancet Infect. Dis. 2021, 21, 939–949. [Google Scholar] [CrossRef]
- Drury, R.E.; O’Connor, D. Symptom study app provides real-world data on COVID-19 vaccines. Lancet Infect. Dis. 2021, 21, 890–891. [Google Scholar] [CrossRef]
- Thompson, M.G.; Burgess, J.L.; Naleway, A.L.; Tyner, H.L.; Yoon, S.K.; Meece, J.; Olsho, L.; Caban-Martinez, A.J.; Fowlkes, A.; Lutrick, K.; et al. Interim Estimates of Vaccine Effectiveness of BNT162b2 and mRNA-1273 COVID-19 Vaccines in Preventing SARS-CoV-2 Infection Among Health Care Personnel, First Responders, and Other Essential and Frontline Workers—Eight, U.S.; Locations, December 2020–March 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 495–500. [Google Scholar]
- Vasileiou, E.; Simpson, C.R.; Shi, T.; Kerr, S.; Agrawal, U.; Akbari, A.; Bedston, S.; Beggs, J.; Bradley, D.; Chuter, A.; et al. Interim findings from first-dose mass COVID-19 vaccination roll-out and COVID-19 hospital admissions in Scotland: A national prospective cohort study. Lancet 2021, 397, 1646–1657. [Google Scholar] [CrossRef]
- Amit, S.; Regev-Yochay, G.; Afek, A.; Kreiss, Y.; Leshem, E. Early rate reductions of SARS-CoV-2 infection and COVID-19 in BNT162b2 vaccine recipients. Lancet 2021, 397, 875–877. [Google Scholar] [CrossRef]
- Benenson, S.; Oster, Y.; Cohen, M.J.; Nir-Paz, R. BNT162b2 mRNA Covid-19 Vaccine Effectiveness among Health Care Workers. N. Engl. J. Med. 2021, 384, 1775–1777. [Google Scholar] [CrossRef] [PubMed]
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef]
- Daniel, W.; Nivet, M.; Warner, J.; Podolsky, D.K. Early Evidence of the Effect of SARS-CoV-2 Vaccine at One Medical Center. N. Engl. J. Med. 2021, 384, 1962–1963. [Google Scholar] [CrossRef] [PubMed]
- Fabiani, M.; Ramigni, M.; Gobbetto, V.; Mateo-Urdiales, A.; Pezzotti, P.; Piovesan, C. Effectiveness of the Comirnaty (BNT162b2, BioNTech/Pfizer) vaccine in preventing SARS-CoV-2 infection among healthcare workers, Treviso province, Veneto region, Italy, 27 December 2020 to 24 March 2021. Euro Surveill. 2021, 26, 2100420. [Google Scholar] [CrossRef] [PubMed]
- Tande, A.J.; Pollock, B.D.; Shah, N.D.; Farrugia, G.; Virk, A.; Swift, M.; Breeher, L.; Binnicker, M.; Berbari, E.F. Impact of the COVID-19 Vaccine on Asymptomatic Infection Among Patients Undergoing Pre-Procedural COVID-19 Molecular Screening. Clin. Infect. Dis. 2021, ciab229, advance online publication. [Google Scholar] [CrossRef] [PubMed]
- COVID EA. Vaccine: EMA Finds Possible Link to very Rare Cases of Unusual Blood Clots with Low Blood Platelets. European Medicines Agency News, 20 April 2021, p. 4. European Medicines Agency. Available online: https://www.ema.europa.eu/en/news/covid-19-vaccine-janssen-ema-finds-possible-link-very-rare-cases-unusual-blood-clots-low-blood (accessed on 9 October 2021).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Method | PCR Test | SARS-CoV-2 Vaccination Protocol | N | Fixed Effect Model | Random Effect Model | τ2 | I2 | ||
|---|---|---|---|---|---|---|---|---|---|
| RR [95%-CI] | p-Value | RR [95%-CI] | p-Value | ||||||
| Inverse Variance (IV) | Any positive PCR | Partially vaccinated | 22 | 0.4115 [0.4025; 0.4207] | 0 | 0.2657 [0.1710; 0.4127] | <0.0001 * | 1.0747 [0.6223; 3.0350] | 99.70% |
| Fully vaccinated | 17 | 0.1204 [0.1120; 0.1295] | 0 | 0.0586 [0.0266; 0.1292] | <0.0001 * | 1.6228 [1.0654; 2.4896] | 99.00% | ||
| At least one dose | 18 | 0.3813 [0.3752; 0.3875] | 0 | 0.1617 [0.1130; 0.2313] | <0.0001 * | 0.5862 [0.4444; 2.6714] | 99.70% | ||
| Symptomatic positive PCR test | Partially vaccinated | 9 | 0.4885 [0.4658; 0.5122] | <0.0001 | 0.2181 [0.0685; 0.6944] | 0.01 * | 3.0607 [0.7297; 10.0860] | 99.50% | |
| Fully vaccinated | 8 | 0.2439 [0.2231; 0.2666] | <0.0001 | 0.0629 [0.0245; 0.1613] | <0.0001 * | 1.7560 [1.1035; 14.6961] | 98.80% | ||
| Mantel–Haenszel (MH) | Any positive PCR | Partially vaccinated | 22 | 0.2490 [0.2436; 0.2546] | 0.2656 [0.1617; 0.4363] | 1.374 | |||
| Fully vaccinated | 17 | 0.0447 [0.0419; 0.0477] | 0.0586 [0.0228; 0.1505] | 3.7986 | |||||
| At least one dose | 18 | 0.3369 [0.3315; 0.3424] | 0.1616 [0.1122; 0.2328] | 0.6083 | |||||
| Symptomatic positive PCR test | Partially vaccinated | 9 | 0.2758 [0.2644; 0.2878] | 0 | 0.2182 [0.0567; 0.8388] | 0.0267 * | 4.1669 | 99.60% | |
| Fully vaccinated | 8 | 0.0811 [0.0752; 0.0874] | 0 | 0.0626 [0.0167; 0.2344] | <0.0001 * | 3.5394 | 99.40% | ||
| Subgroups | N | Results for Subgroups | Between-Group Heterogeneity | |||||
|---|---|---|---|---|---|---|---|---|
| RR (95%-CI) | I2 | tau2 | Q | df(Q) | I-Value | |||
| (a) Partially Vaccinated, Any Positive PCR—Fixed Effect | ||||||||
| Vaccine | BNT162b2 | 16 | 0.5250 (0.5123;0.5381) | 99.60% | 0.7549 | 3108.43 | 3 | 0 |
| ChAdOx1/AZD1222 | 2 | 0.2277 (0.2122;0.2443) | 98.90% | 0.3565 | ||||
| BNT162b2/mRNA-1273 | 3 | 0.2778 (0.2474;0.3120) | 98.80% | 1.0692 | ||||
| BNT162b2/ChAdOx1/AZD1222 | 1 | 0.0357 (0.0323;0.0393) | - | |||||
| Quality | NOS ≤ 6 | 15 | 0.4816 (0.4704;0.4931) | 99.60% | 0.6113 | 1502.28 | 1 | 0 |
| NOS > 6 | 7 | 0.1219 (0.1142;0.1302) | 99.70% | 3.3748 | ||||
| Age | <69 years | 15 | 0.4828 (0.4702;0.4958) | 99.80% | 1.5669 | 463.24 | <0.0001 | |
| ≥69 years | 7 | 0.2845 (0.2733;0.2962) | 98.60% | 0.2424 | ||||
| Lineage | B.1.1.7 | 8 | 0.3903 (0.3777;0.4033) | 99.70% | 0.9447 | 3031.61 | 3 | 0 |
| B.1.1.7/non-B.1.1.7 | 5 | 0.1492 (0.1418;0.1569) | 99.70% | 1.4303 | ||||
| Not specified | 8 | 0.3254 (0.2971;0.3565) | 97.10% | 0.6506 | ||||
| B.1.351 | 1 | 0.9080 (0.8717;0.9458) | - | |||||
| (b) Fully Vaccinated, Any Positive PCR—Fixed Effect | ||||||||
| Vaccine | BNT162b2 | 11 | 0.1680 (0.1537; 0.1836) | 98.40% | 1.7775 | 702.84 | 3 | <0.0001 |
| BNT162b2/mRNA-1273 | 4 | 0.1624 (0.1394; 0.1893) | 98.90% | 3.7392 | ||||
| BNT162b2/ChAdOx1/AZD1222 | 1 | 0.0062 (0.0049; 0.0078) | - | - | ||||
| Ad26.COV2.S | 1 | 0.2338 (0.0745; 0.7337) | - | - | ||||
| Quality | NOS ≤ 6 | 11 | 0.1947 (0.1797; 0.2108) | 98.50% | 1.3935 | 827.35 | 1 | <0.0001 |
| NOS >6 | 6 | 0.0112 (0.0094; 0.0134) | 95.90% | 1.6474 | ||||
| Age | <69 years | 13 | 0.1171 (0.1084; 0.1266) | 99.30% | 3.0726 | 4.21 | 1 | 0.0403 |
| ≥69 years | 4 | 0.1487 (0.1200; 0.1843) | 65.00% | 0.2931 | ||||
| Lineage | B.1.1.7 | 4 | 0.1448 (0.1231; 0.1703]) | 95.90% | 0.817 | 1000.54 | 3 | <0.0001 |
| B.1.1.7/non-B.1.1.7 | 5 | 0.0190 (0.0165; 0.0219) | 98.60% | 1.9969 | ||||
| Not specified | 7 | 0.1692 (0.1452; 0.1971) | 97.70% | 3.4732 | ||||
| B.1.351 | 1 | 0.4027 (0.3533; 0.4592) | - | - | ||||
| (c) At Least One Dose, Any Positive PCR—Fixed Effect | ||||||||
| Vaccine | BNT162b2 | 12 | 0.2575 (0.2511; 0.2640) | 99.60% | 0.6218 | 2752.22 | 2 | 0 |
| BNT162b2/mRNA-1273 | 4 | 0.5641 (0.5517; 0.5767) | 98.50% | 0.4039 | ||||
| ChAdOx1/AZD1222 | 2 | 0.1462 (0.1354; 0.1578) | 83.10% | 0.2114 | ||||
| Quality | NOS ≤6 | 16 | 0.2550 (0.2491; 0.2610) | 99.40% | 0.432 | 2182.95 | 1 | 0 |
| NOS >6 | 2 | 0.5525 (0.5402; 0.5650) | 99.90% | 8.9219 | ||||
| Age | <69 years | 12 | 0.2196 (0.2133; 0.2260) | 99.30% | 0.5076 | 2070.75 | 1 | 0 |
| ≥ 69 years | 6 | 0.4927 (0.4832; 0.5025) | 99.80% | 0.5585 | ||||
| Lineage | B.1.1.7 | 4 | 0.3357 (0.3223; 0.3497) | 99.80% | 0.8863 | 1015.58 | 2 | <0.0001 |
| B.1.1.7/non-B.1.1.7 | 5 | 0.1463 (0.1372; 0.1560) | 95.00% | 0.3366 | ||||
| Not specified | 9 | 0.4231 (0.4154; 0.4310) | 99.80% | 0.5975 | ||||
| (d) Partially Vaccinated, Symptomatic Positive PCR—Fixed Effect | ||||||||
| Vaccine | BNT162b2 | 6 | 0.6572 (0.6245; 0.6915]) | 99.60% | 1.1044 | 1414.28 | 3 | <0.0001 |
| ChAdOx1/AZD1222 | 1 | 0.3441 (0.1763; 0.6715) | - | |||||
| BNT162b2/mRNA-1273 | 1 | 0.5552 (0.4336; 0.7111) | - | |||||
| BNT162b2/ChAdOx1/AZD1222 | 1 | 0.0270 (0.0231; 0.0317) | - | |||||
| Quality | NOS ≤6 | 6 | 0.6688 (0.6354; 0.7039) | 99.60% | 0.7447 | 1057.05 | 1 | <0.0001 |
| NOS >6 | 3 | 0.0676 (0.0595; 0.0769) | 99.50% | 3.5694 | ||||
| Age | <69 years | 7 | 0.4902 (0.4673; 0.5143) | 99.60% | 3.384 | 1.25 | 1 | 0.2636 |
| ≥69 years | 2 | 0.3962 (0.2736; 0.5737) | 0.00% | - | ||||
| Lineage | B.1.1.7 | 3 | 0.2410 (0.1801; 0.3224) | 89.10% | 0.5695 | 26.49 | 3 | <0.0001 |
| B.1.1.7/non-B.1.1.7 | 2 | 0.5032 (0.4789; 0.5287) | 99.90% | 5.242 | ||||
| Not specified | 4 | 0.4116 (0.3326; 0.5094) | 94.10% | 1.3278 | ||||
| (e) Fully Vaccinated, Symptomatic Positive PCR—Fixed Model | ||||||||
| Vaccine | BNT162b2 | 6 | 0.3181 (0.2901; 0.3489) | 94.90% | 0.3245 | 488.27 | 2 | <0.0001 |
| BNT162b2/ChAdOx1/AZD1222 | 1 | 0.0021 (0.0012; 0.0036) | - | - | ||||
| BNT162b2/mRNA-1273 | 1 | 0.0131 (0.0086; 0.0200) | - | - | ||||
| Quality | NOS ≤ 6 | 5 | 0.3301 (0.3008; 0.3622) | 93.00% | 0.1911 | 492.15 | 1 | <0.0001 |
| NOS > 6 | 3 | 0.0085 (0.0063; 0.0116) | 94.60% | 1.4624 | ||||
| Lineage | B.1.1.7 | 2 | 0.1347 (0.1034; 0.1753) | 94.80% | 1.565 | 222.39 | 3 | <0.0001 |
| B.1.1.7/non-B.1.1.7 | 3 | 0.2744 (0.2408; 0.3127) | 99.40% | 6.8062 | ||||
| Not specified | 2 | 0.0166 (0.0111; 0.0248) | 91.80% | 2.5779 | ||||
| B.1.351 | 1 | 0.3598 (0.3111; 0.4162) | - | - | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meggiolaro, A.; Sane Schepisi, M.; Nikolaidis, G.F.; Mipatrini, D.; Siddu, A.; Rezza, G. Effectiveness of Vaccination against SARS-CoV-2 Infection in the Pre-Delta Era: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 157. https://doi.org/10.3390/vaccines10020157
Meggiolaro A, Sane Schepisi M, Nikolaidis GF, Mipatrini D, Siddu A, Rezza G. Effectiveness of Vaccination against SARS-CoV-2 Infection in the Pre-Delta Era: A Systematic Review and Meta-Analysis. Vaccines. 2022; 10(2):157. https://doi.org/10.3390/vaccines10020157
Chicago/Turabian StyleMeggiolaro, Angela, Monica Sane Schepisi, Georgios F. Nikolaidis, Daniele Mipatrini, Andrea Siddu, and Giovanni Rezza. 2022. "Effectiveness of Vaccination against SARS-CoV-2 Infection in the Pre-Delta Era: A Systematic Review and Meta-Analysis" Vaccines 10, no. 2: 157. https://doi.org/10.3390/vaccines10020157