
Declared Intention (Not) to Be Vaccinated against COVID-19, and Actual Behavior—The Longitudinal Study in the Polish Sample


Abstract
:1. Introduction
1.1. What Drives Vaccine Skepticism?
1.2. Acceptance or Rejection of Vaccinations as a Consequence of Conscious Intention-Own Research
2. Methods
2.1. Participants and the Study Design
2.2. Procedure
3. Results
3.1. Attitude toward Mandatory Vaccination of Children vs. Attitude toward Mandatory Vaccination against COVID-19
3.2. Declared Intent of Vaccinating against COVID-19 vs. Actual Vaccination
3.3. Reasons to Get Vaccinated or Not, and Their Association with Intended and Actual Vaccination
3.4. Attitudes toward Mandatory Vaccination of Children and COVID-19 Vaccination Support
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wadlowska, A. Poland Announces COVID Vaccine Plan, Aiming for 70–80% of Population to Vaccinate. Available online: https://notesfrompoland.com/2020/12/02/poland-announces-covid-vaccine-plan-aiming-for-70-80-of-population-to-vaccinate/ (accessed on 15 December 2021).
- Gallè, F.; Sabella, E.A.; Roma, P.; De Giglio, O.; Caggiano, G.; Tafuri, S.; Da Molin, G.; Ferracuti, S.; Montagna, M.T.; Liguori, G.; et al. Knowledge and Acceptance of COVID-19 Vaccination among Undergraduate Students from Central and Southern Italy. Vaccines 2021, 9, 638. [Google Scholar] [CrossRef] [PubMed]
- CBOS Stosunek Do Szczepień Przeciw COVID19 (Attitudes towards COVID19 Vaccination). Available online: https://www.cbos.pl/PL/publikacje/news/2020/41/newsletter.php (accessed on 15 December 2021).
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2020, 27, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Green, M.S.; Abdullah, R.; Vered, S.; Nitzan, D. A study of ethnic, gender and educational differences in attitudes toward COVID-19 vaccines in Israel—Implications for vaccination implementation policies. Isr. J Health Policy Res. 2021, 10, 26. [Google Scholar] [CrossRef] [PubMed]
- Thaker, J.; Ganchoudhuri, S. The Role of Attitudes, Norms, and Efficacy on Shifting COVID-19 Vaccine Intentions: A Longitudinal Study of COVID-19 Vaccination Intentions in New Zealand. Vaccines 2021, 9, 1132. [Google Scholar] [CrossRef] [PubMed]
- Rutjens, B.T.; Sutton, R.M.; van der Lee, R. Not all skepticism is equal. Exploring the ideological antecedents of science acceptance and rejection. Personal. Soc. Psychol. Bull. 2017, 44, 384–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hornsey, M.J.; Harris, E.A.; Fielding, K.S. The psychological roots of anti-vaccination attitudes: A 24-nation investigation. Health Psychol. 2018, 37, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Petrovic, M.; Roberts, R.; Ramsay, M. Second dose of measles, mumps, and rubella vaccine: Questionnaire survey of health professionals. BMJ 2001, 322, 82–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Speers, T.; Lewis, J. Journalists and jabs: Media coverage of the MMR vaccine. Commun. Med. 2004, 1, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Kata, A. A postmodern Pandora’s box: Antivaccination misinformation on the internet. Vaccine 2010, 29, 1709–1716. [Google Scholar] [CrossRef] [PubMed]
- Moran, M.B.; Lucas, M.; Everhart, L.; Morgan, A.; Prickett, E. What makes anti-vaccine websites persuasive? A content analysis of techniques used by antivaccine websites to engender antivaccine sentiment. J. Commun. Healthc. 2016, 9, 151–163. [Google Scholar] [CrossRef]
- Stasiuk, K.; Polak, M.; Dolinski, D.; Maciuszek, J. The credibility of health information sources as predictors of attitudes toward vaccination—the results from a longitudinal study in Poland. Vaccines 2021, 9, 933. [Google Scholar] [CrossRef] [PubMed]
- Stasiuk, K.; Maciuszek, J.; Polak, M.; Doliński, D. Profiles of vaccine hesitancy: The relation between personal experience with vaccines, attitude towards mandatory vaccination, and support for anti-vaccine arguments among vaccine hesitant individuals. Soc. Psychol. Bull. 2021, 16, 1–20. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Processes 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Fazio, T.H. Multiple processes by which attitudes quide behavior: The MODE model as a integrative framwork. Adv. Exp. Soc. Psychol. 1990, 23, 75–109. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Action at Time 2 | |||||
|---|---|---|---|---|---|
| Total | Anti-Vaccine | Undecided | Vaccinated | ||
| Declaration at Time 1 | Anti-vaccine | 217 | 126 (58%) | 43 (20%) | 48 (22%) |
| Undecided | 265 | 30 (11%) | 86 (32%) | 149 (56%) | |
| Pro-vaccine | 393 | 6 (2%) | 8 (2%) | 379 (96%) | |
| Total | 875 | 162 (18%) | 137 (16%) | 576 (66%) | |
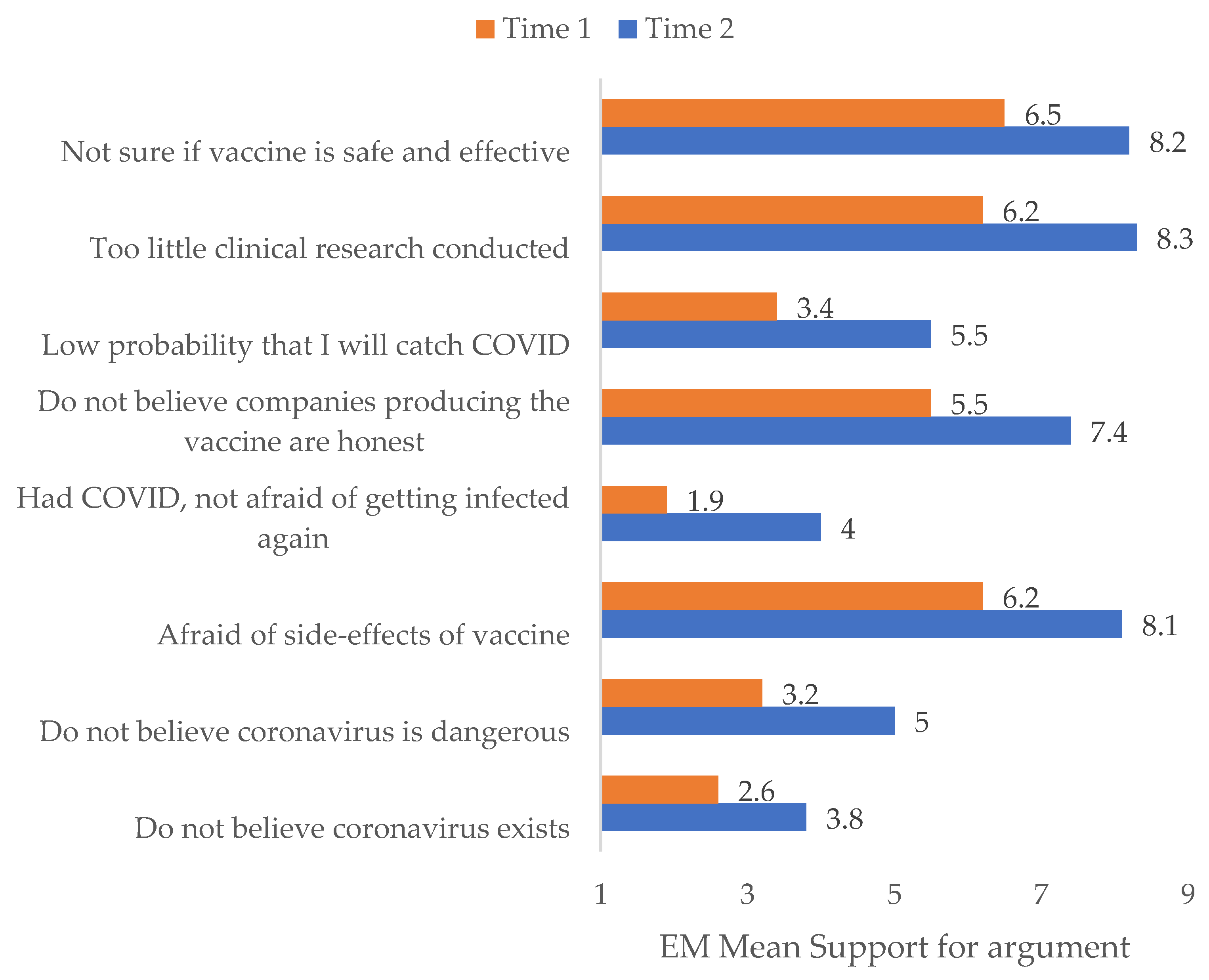
| Time 1 | Time 2 | |||
|---|---|---|---|---|
| Reason | M | SE | M | SE |
| Do not believe coronavirus exists | 2.621 | 0.160 | 3.895 | 0.186 |
| Do not believe coronavirus is dangerous | 3.211 | 0.161 | 5.018 | 0.176 |
| Afraid of side-effects of vaccine | 6.249 | 0.139 | 8.147 | 0.146 |
| Had COVID, not afraid of getting infected again | 1.989 | 0.147 | 4.007 | 0.202 |
| Do not believe companies producing the vaccine are honest | 5.540 | 0.152 | 7.484 | 0.158 |
| Low probability that I will catch COVID | 3.460 | 0.155 | 5.533 | 0.165 |
| Too little clinical research conducted | 6.295 | 0.137 | 8.316 | 0.136 |
| Not sure if vaccine is safe and effective | 6.509 | 0.130 | 8.281 | 0.142 |
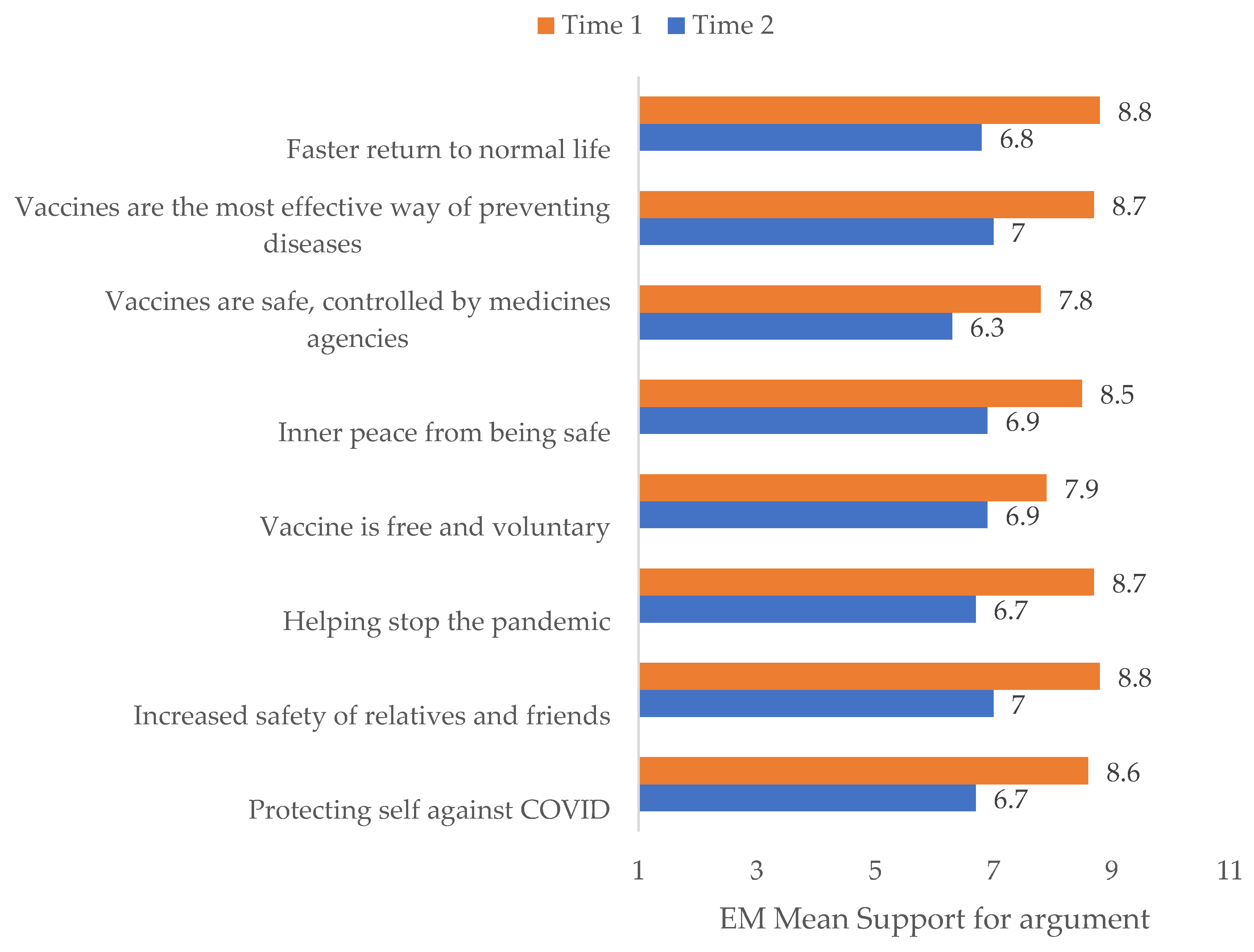
| Time 1 | Time 2 | |||
|---|---|---|---|---|
| Reason | M | SE | M | SE |
| Protecting self against COVID | 8.625 | 0.094 | 6.720 | 0.088 |
| Increased safety of relatives and friends | 8.887 | 0.086 | 7.039 | 0.080 |
| Helping stop the pandemic | 8.781 | 0.085 | 6.794 | 0.086 |
| Vaccine is free and voluntary | 7.915 | 0.130 | 6.949 | 0.088 |
| Inner peace from being safe | 8.548 | 0.099 | 6.995 | 0.077 |
| Vaccines are safe, controlled by medicines agencies | 7.859 | 0.108 | 6.350 | 0.095 |
| Vaccines are the most effective way of preventing diseases | 8.730 | 0.089 | 7.064 | 0.067 |
| Faster return to normal life | 8.851 | 0.081 | 6.841 | 0.086 |
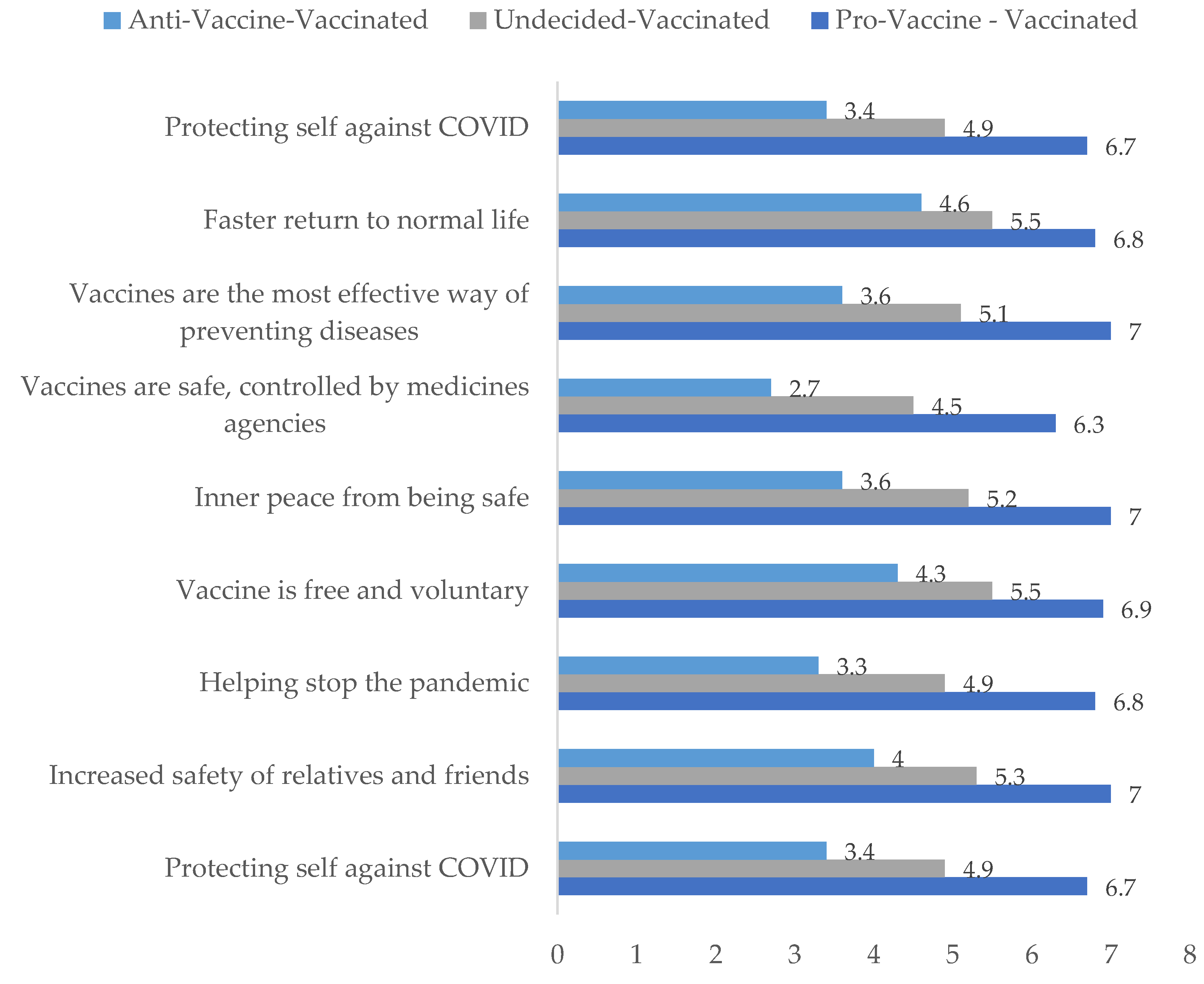
| Intention to Behavior | Pro-Vaccine → Vaccinated | Undecided → Vaccinated | Anti-Vaccine → Vaccinated | |||
|---|---|---|---|---|---|---|
| Reason | M | SE | M | SE | M | SE |
| Protecting self against COVID | 6.760 | 0.102 | 4.946 | 0.163 | 3.458 | 0.287 |
| Increased safety of relatives and friends | 7.069 | 0.096 | 5.356 | 0.153 | 4.021 | 0.269 |
| Helping stop the pandemic | 6.823 | 0.100 | 4.953 | 0.160 | 3.375 | 0.281 |
| Vaccine is free and voluntary | 6.963 | 0.104 | 5.557 | 0.166 | 4.375 | 0.293 |
| Inner peace from being safe | 7.011 | 0.095 | 5.289 | 0.152 | 3.667 | 0.268 |
| Vaccines are safe, controlled by medicines agencies | 6.391 | 0.106 | 4.557 | 0.168 | 2.750 | 0.297 |
| Vaccines are the most effective way of preventing diseases | 7.079 | 0.091 | 5.141 | 0.145 | 3.667 | 0.256 |
| Faster return to normal life | 6.858 | 0.098 | 5.550 | 0.156 | 4.688 | 0.276 |
| Protecting self against COVID | 6.760 | 0.102 | 4.946 | 0.163 | 3.458 | 0.287 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maciuszek, J.; Polak, M.; Stasiuk, K. Declared Intention (Not) to Be Vaccinated against COVID-19, and Actual Behavior—The Longitudinal Study in the Polish Sample. Vaccines 2022, 10, 147. https://doi.org/10.3390/vaccines10020147
Maciuszek J, Polak M, Stasiuk K. Declared Intention (Not) to Be Vaccinated against COVID-19, and Actual Behavior—The Longitudinal Study in the Polish Sample. Vaccines. 2022; 10(2):147. https://doi.org/10.3390/vaccines10020147
Chicago/Turabian StyleMaciuszek, Jozef, Mateusz Polak, and Katarzyna Stasiuk. 2022. "Declared Intention (Not) to Be Vaccinated against COVID-19, and Actual Behavior—The Longitudinal Study in the Polish Sample" Vaccines 10, no. 2: 147. https://doi.org/10.3390/vaccines10020147