
High Influenza Vaccine Effectiveness and Absence of Increased Influenza-like-Illness Epidemic Activity in the 2021–2022 Influenza Season in Catalonia (Spain) Based on Surveillance Data Collected by Sentinel Pharmacies

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Influenza-Like Illness Surveillance Based on Sentinel Pharmacies
2.2. Analysis of the Influenza-Like-Illness Activity
2.3. Influenza Vaccination Effectiveness
2.4. Statistical Analysis
3. Results
3.1. Influenza-Like-Illness Cases Reported by Sentinel Pharmacies
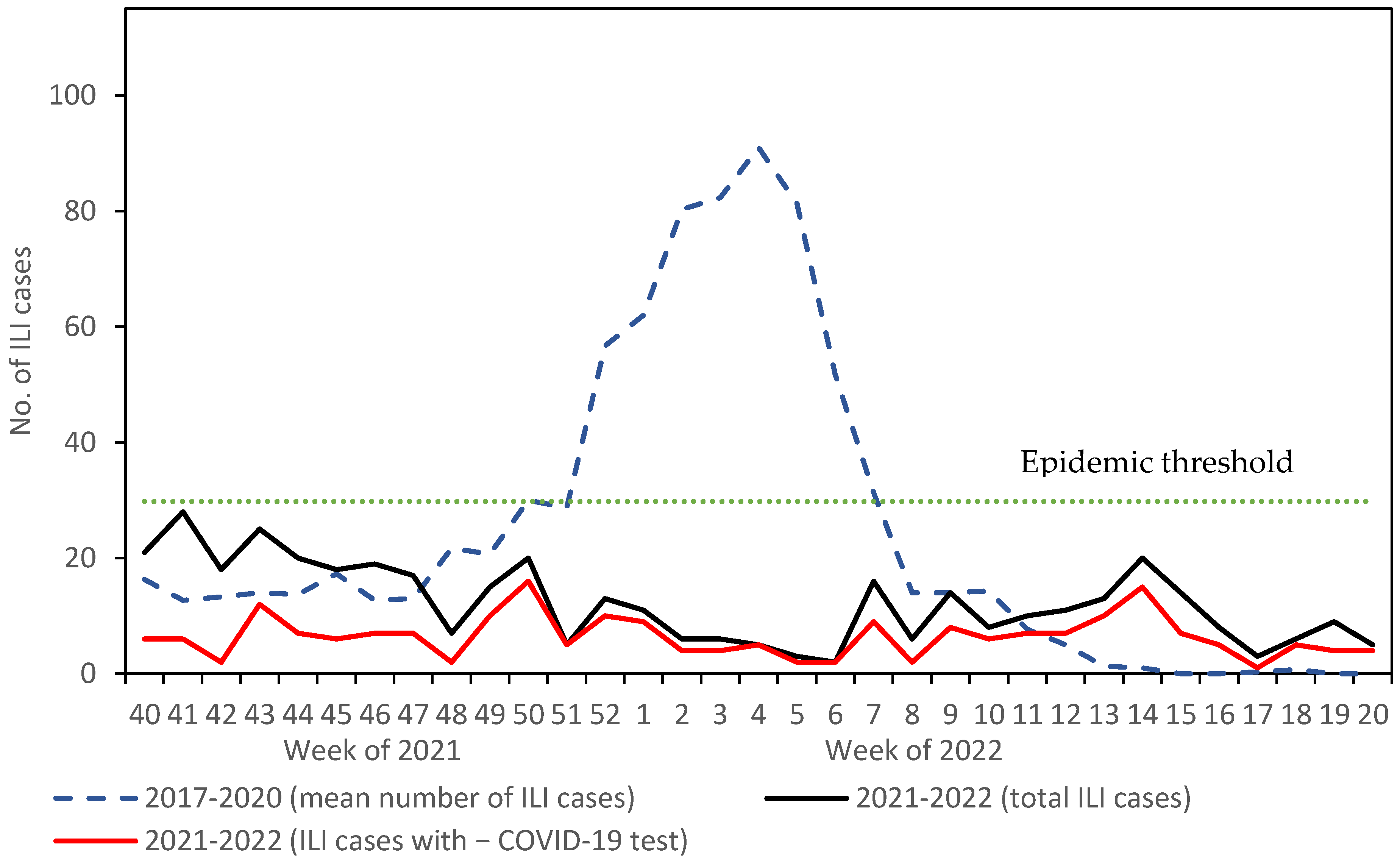
3.2. Influenza-Like-Illness Epidemic Activity
3.3. Influenza Vaccination Effectiveness
3.4. Medications Dispensed and Prescribed to Influenza-Like Illness Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Plans Rubió, P. Role of community pharmacies in the prevention of communicable diseases. Vacunas (Engl. Ed.) 2022, 23, 62–63. [Google Scholar] [CrossRef]
- Pharmaceutical Group of European Union. Pharmacy 2030: A Vision for Community Pharmacy in Europe; PGEU: Brussels, Belgium, 2018; Available online: https://www.pgeu.eu/wp-content/uploads/2019/03/Pharmacy-2030_-A-Vision-for-Community-Pharmacy-in-Europe.pdf (accessed on 25 October 2022).
- Hansen, R.N.; Nørgaard, L.S.; Hedegaard, U.; Søndergaard, L.; Servilieri, K.; Bendixen, S.; Rossing, C. Integration of and Visions for Community Pharmacy in Primary Health Care in Denmark. Pharm. Pract. (Granada) 2021, 19, 2212. Available online: https://www.pharmacypractice.org/index.php/pp/article/view/2212 (accessed on 25 October 2022). [CrossRef] [PubMed]
- Le, L.M.; Veettil, S.K.; Donaldson, D.; Kategeaw, W.; Hutubessy, R.; Lambach, P.; Chaiyakunapruk, N. The impact of pharmacist involvement on immunization uptake and other outcomes: An updated systematic review and meta-analysis. J. Am. Pharm. Assoc. 2022, 62, 1499–1513. [Google Scholar] [CrossRef] [PubMed]
- Czech, M.; Balcerzak, M.; Antczak, A.; Byliniak, M.; Piotrowska-Rutkowska, E.; Drozd, M.; Juszczyk, G.; Religioni, U.; Vaillancourt, R.; Merks, P. Flu Vaccinations in Pharmacies—A Review of Pharmacists Fighting Pandemics and Infectious Diseases. Int. J. Environ. Res. Public Health 2020, 17, 7945. [Google Scholar] [CrossRef] [PubMed]
- Nusair, M.B.; Arabyat, R.; Mukattash, T.L.; Alhamad, H.; Abu Ghaida, M.T.; Momani, M.Y. Pharmacists’ Perspectives on Providing the Influenza Vaccine in Community Pharmacies: A Qualitative Study. Risk Manag. Healthc. Policy 2020, 13, 2179–2187. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Sanidad. Guía de Procedimientos Para la Vigilancia de la Gripe en España; Ministerio de Sanidad: Madrid, Spain, 2019. Available online: https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/EnfermedadesTransmisibles/Documents/GRIPE/GUIAS/Gu%C3%ADa%20de%20procedimientos%20para%20la%20vigilancia%20de%20gripe%20en%20Espa%C3%B1a_marzo%202019.pdf (accessed on 20 October 2022).
- Plans-Rubió, P.; Jambrina, A.M.; Carmona, G.; Rabanal, M.; Jané, M.; Rius, P. Influenza syndromic surveillance based on sentinel pharmacies in Catalonia (Spain) in 2017–2020. Int. J. Mod. Pharm. Res. 2021, 5, 207–221. [Google Scholar]
- Plans-Rubió, P.; Jambrina, A.M.; Rius, P.; Carmona, G.; Rabanal, M.; Girones, M. Absence of the influenza epidemic in the 2020-2021 influenza seaon in Catalonia, Spain, based on surveillance data collected by sentinel pharmacies. Int. J. Mod. Pharm. Res. 2022, 6, 29–36. [Google Scholar]
- Jambrina, A.M.; Rams, N.; Rius, P.; Perelló, M.; Gironès, M.; Pareja, C.; Pérez-Cano, F.J.; Franch, À.; Rabanal, M. Creation and Implementation of a New Sentinel Surveillance Model in Pharmacy Offices in Southern Europe. Int. J. Environ. Res. Public Health 2022, 19, 8600. [Google Scholar] [CrossRef] [PubMed]
- Koppeschaar, C.E.; Colizza, V.; Guerrisi, C.; Turbelin, C.; Duggan, J.; Edmunds, W.J.; Kjelsø, C.; Mexia, R.; Moreno, Y.; Meloni, S.; et al. Influenzanet: Citizens Among 10 Countries Collaborating to Monitor Influenza in Europe. JMIR Public Health Surveill. 2017, 3, e66. [Google Scholar] [CrossRef] [PubMed]
- Vega, T.; Lozano, J.E.; Merhoff, T.; Snacken, R.; Mott, J.; Ortiz de Lejarazu, R.; Nunes, B. Influenza surveillance in Europe: Establishing epidemic thresholds by the moving epidemic method. Influenza Other Respir. Viruses 2013, 7, 546–558. [Google Scholar] [CrossRef]
- Asociación Española de Pediatría. Coberturas de Vacunación en la Temporada 2021–2022; AEP: Madrid, Spain, 2022; Available online: https://vacunasaep.org/sites/vacunasaep.org/files/gripe_cobertura-vacunal_2021-22_mayores64.pdf?1663520973 (accessed on 3 November 2022).
- Farrington, C.P. Estimation of vaccine effectiveness using the screening method. Int. J. Epidemiol. 1993, 22, 742–746. [Google Scholar] [CrossRef]
- Institut d’Estadística de Catalunya (IDESCAT). Anuari Estadístic de Catalunya; IDESCAT: Barcelona, Spain, 2022. [Google Scholar]
- Uchida, M.; Kaneko, M.; Hidaka, Y.; Yamamoto, H.; Honda, T.; Takeuchi, S.; Saito, M.; Kawa, S. Effectiveness of vaccination and wearing masks on seasonal influenza in Matsumoto City, Japan, in the 2014/2015 season: An observational study among all elementary schoolchildren. Prev. Med. Rep. 2016, 6, 86–91. [Google Scholar] [CrossRef]
- Huang, Q.S.; Wood, T.; Jelley, L.; Jennings, T.; Jefferies, S.; Daniells, K.; Nesdale, A.; Dowell, T.; Turner, N.; Campbell-Stokes, P.; et al. Impact of the COVID-19 nonpharmaceutical interventions on influenza and other respiratory viral infections in New Zealand. Nat. Commun. 2021, 12, 1001. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). Interim US Flu Vaccine Effectiveness (VE) Data for 2021–2022. Reviewed 3 August 2022. Available online: https://www.cdc.gov/flu/vaccines-work/2021-2022.html (accessed on 3 November 2022).
- Goad, J.; Influenza Activity and Vaccine Effectiveness during the 2021–2022 Influenza Season. Pharm. Times 2022. Available online: https://www.pharmacytimes.com/view/influenza-activity-and-vaccine-effectiveness-during-the-2021-2022-season (accessed on 3 November 2022).
- World Health Organization (WHO). Evaluation of Influenza Vaccine Effectiveness: A Guide to the Design and Interpretation of Observational Studies; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Gilca, R.; Amini, R.; Douville-Fradet, M.; Charest, H.; Dubuque, J.; Boulianne, N.; Skowronski, D.M.; De Serres, G. Other respiratory viruses are important contributors to adult respiratory hospitalizations and mortality even during peak weeks of the influenza season. Open Forum. Infect. Dis. 2014, 1, ofu086. [Google Scholar] [CrossRef] [PubMed]
- Sub-Direcció General de Vigilància Epidemiològica. Pla D’informació de les Infeccions Respiratòries Agudes A Catalunya. Temporada 2021–2022; Sub-Direcció General de Vigilància Epidemiològica: Barcelona, Spain, 2022; Available online: https://canalsalut.gencat.cat/web/.content/_Professionals/Vigilancia_epidemiologica/documents/arxius/spfi.pdf (accessed on 10 October 2022).
- Sub-Direcció General de Vigilància Epidemiològica. Pla D’informació de les Infeccions Respiratòries Agudes A Catalunya 2021–2022; Sub-Direcció General de Vigilància Epidemiològica: Barcelona, Spain, 2022; Available online: https://canalsalut.gencat.cat/web/.content/_Professionals/Vigilancia_epidemiologica/documents/arxius/pla-pidirac-2021-22.pdf (accessed on 10 October 2022).
- Centers for Disease Control and Prevention (CDC). Weekly U.S. Influenza Surveillance Report; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2022. Available online: https://www.cdc.gov/flu/weekly/weeklyarchives2021-2022/week20.htm (accessed on 3 November 2022).
- Government of Canada. FluWatch Report: May 15 to May 21, 2022 (week 20). Available online: https://health/services/publications/diseases-conditions/fluwatch/2021-2022/week-20-may-15-may-21-2022.html (accessed on 3 November 2022).
- Statems Serum Institut. Influenza Season 2021/2022. Available online: https://en.ssi.dk/surveillance-and-preparedness/surveillance-in-denmark/annual-reports-on-disease-incidence/influenza-season-2021-2022 (accessed on 3 November 2022).
- Pivette, M.; Mueller, J.E.; Crépey, P.; Bar-Hen, A. Drug sales data analysis for outbreak detection of infectious diseases: A systematic literature review. BMC Infect. Dis. 2014, 14, 604. [Google Scholar] [CrossRef]
- Ziemann, A.; Fouillet, A.; Brand, H.; Krafft, T. Success Factors of European Syndromic Surveillance Systems: A Worked Example of Applying Qualitative Comparative Analysis. PLoS ONE 2016, 11, e0155535. [Google Scholar] [CrossRef]
- Dailey, L.; Watkins, R.E.; Plant, A.J. Timeliness of data sources used for influenza surveillance. JAMIA 2007, 14, 626–631. [Google Scholar] [CrossRef]
- Pharmaceutical Group of the European Union (PGEU). Position Paper on the Role of Community Pharmacists in COVID-19—Lessons Learned from the Pandemic. Available online: https://www.pgeu.eu/wp-content/uploads/2020/03/PGEU-Position-Paper-on-on-the-Lessons-Learned-from-COVID-19-ONLINE.pdf (accessed on 2 November 2022).
- OECD. Beyond Containment: Health Systems Responses to COVID-19 in the OECD. OECD. 2020. Available online: https://read.oecd-ilibrary.org/view/?ref=119_119689-ud5comtf84&title=Beyond_Containment:Health_systems_responses_to_COVID-19_in_the_OECD (accessed on 2 November 2022).
- WHO. Strengthening the Health System Response to COVID-19; WHO: Geneva, Switzerland, 2020; Available online: https://apps.who.int/iris/bitstream/handle/10665/333072/WHO-EURO-2020-806-40541-54465-eng.pdf?sequence=1&isAllowed=y (accessed on 2 October 2022).
- Verjee, Z.; Duggan, C.; Swaminathan, S.; Gellin, B.; Piervincenzi, R.; Etienne, C. Quality, Speed & Equity: Delivering COVID-19 Vaccines to the World. Virtual Webinar; 15 March 2021. Available online: https://zoom.us/webinar/register/WN_S69BcKzhRDy8ll1I1SRuxw (accessed on 15 March 2021).
- Royal Pharmaceutical Society. RPS Statement on the Role of Pharmacists in the COVID-19 Vaccination Programme; Royal Pharmaceutical Society: London, UK, 2020. [Google Scholar]
- CDC. Pharmacies Participating in COVID-19 Vaccination. Available online: https://www.cdc.gov/vaccines/covid-19/retail-pharmacy-program/participating-pharmacies.html (accessed on 2 November 2022).


{kind=link}
| Age | Influenza-Like Illness Cases Reported by Sentinel Pharmacies in the 2021–2022 Influenza Season | |||
|---|---|---|---|---|
| Total ILI Cases | ILI Cases with a Negative COVID-19 Test | |||
| No. | % (95% CI) | No. | % (95% CI) | |
| Both sexes | ||||
| 0–4 years | 19 | 4.7 (2.5–6.9) | 9 | 4.2 (1.3–7.2) |
| 5–14 years | 32 | 8.0 (5.2–10.7) | 16 | 7.5 (3.8–11.3) |
| 15–64 years | 315 | 78.4 (74.2–82.5) | 167 | 78.8 (73.0–84.5) |
| ≥65 years | 36 | 8.9 (4.0–11.9) | 20 | 9.4 (5.3–13.6) |
| Total | 402 | 100 | 212 | 100 |
| Men | ||||
| 0–4 years | 13 | 9.8 (2.8–10.2) | 7 | 6.8 (1.4–12.1) |
| 5–14 years | 18 | 6.5 (4.8–13.2) | 9 | 8.7 (2.8–14.7) |
| 15–64 years | 157 | 73.9 (72.6–84.4) | 81 | 78.6 (70.2–87.0) |
| ≥65 years | 12 | 9.8 (2.5–9.5) | 6 | 5.8 (0.8–10.8) |
| Total | 200 | 100 | 103 | 100 |
| Women | ||||
| 0–4 years | 6 | 4.7 (0.4–5.6) | 2 | 1.8 (0.2–6.5) |
| 5–14 years | 14 | 9.4 (3.2–10.7) | 7 | 6.4 (1.4–11.5) |
| 15–64 years | 158 | 69.4 (72.3–84.2) | 86 | 78.9 (70.8–87.0) |
| ≥65 years | 24 | 16.5 (7.2–16.6) | 14 | 12.8 (6.1–19.6) |
| Total | 202 | 100 | 109 | 100 |
| Age | Influenza Vaccination Coverage in ILI Cases Reported by Sentinel Pharmacies and Influenza Vaccination Effectiveness | |||||
|---|---|---|---|---|---|---|
| ILI Cases with a Negative COVID-19 test | Total ILI Cases | |||||
| No. | % (95% CI) | n | No. | % (95% CI) | n | |
| 0–4 years | 0 | 0.0 (0.0–33.6) | 9 | 0 | 0.0 (0.0–17.6) | 19 |
| 5–14 years | 1 | 6.3 (0.2–30.2) | 16 | 1 | 3.1 (0.1–16.2) | 32 |
| 15–64 years | 10 | 6.0 (2.1–9.9) | 167 | 12 | 3.8 (1.5–6.1) | 315 |
| ≥65 years | 6 | 30.0 (11.9–54.3) | 20 | 11 | 30.5 (14.1–47.0) | 36 |
| Total | 17 | 8.0 (4.1–11.9) | 212 | 24 | 6.0 (3.5–8.4) | 402 |
| Vaccine Effectiveness (≥65 years) | 76.0 (37.5–90.8) | 75.4 (49.9–87.9) | ||||
| Age | Dispensation of Medications to ILI Cases with a Negative COVID-19 Test | Prescription of Medications to ILI Cases with a Negative COVID-19 Test | ||||
|---|---|---|---|---|---|---|
| No. | % (95% CI) | n | No. | % (95% CI) | n | |
| Both sexes | ||||||
| 0–4 years | 8 | 88.9 (51.8–99.7) | 9 | 12 | 66.7 (29.9–92.5) | 9 |
| 5–14 years | 14 | 87.5 (61.6–98.4) | 16 | 6 | 18.8 (4.0–45.6) | 16 |
| 15–64 years | 156 | 93.4 (89.3–97.5) | 167 | 92 | 37.7 (30.1–43.4) | 167 |
| ≥65 years | 19 | 95.0 (75.1–99.9) | 20 | 12 | 45.0 (23.1–66.5) | 20 |
| Total | 197 | 92.9 (89.2–96.6) | 212 | 122 | 8.2 (31.4–45.0) | 212 |
| Men | ||||||
| 0–4 years | 6 | 85.7 (42.1–99.6) | 7 | 8 | 57.1 (18.4–90.1) | 7 |
| 5–14 years | 7 | 77.8 (40.0–97.2) | 9 | 3 | 22.2 (2.9–60.0) | 9 |
| 15–64 years | 73 | 90.1 (83.0–97.2) | 81 | 42 | 35.8 (24.7–46.9) | 81 |
| ≥65 years | 6 | 100.0 (83.0–97.2) | 6 | 6 | 66.7 (22.3–95.7) | 6 |
| Total | 92 | 89.3 (82.9–95.8) | 103 | 59 | 37.9 (28.0–47.7) | 103 |
| Women | ||||||
| 0–4 years | 2 | 100.0 (15.8–100) | 2 | 4 | 100.0 (15.8–100) | 2 |
| 5–14 years | 7 | 100.0 (59.0–100) | 7 | 3 | 14.3 (0.4–57.9) | 7 |
| 15–64 years | 83 | 96.5 (90.1–99.3) | 86 | 50 | 39.5 (28.6–50.4) | 86 |
| ≥65 years | 13 | 92.9 (66.1–99.5) | 14 | 6 | 35.7 (12.8–64.9) | 14 |
| Total | 105 | 96.3 (90.9–99.0) | 109 | 63 | 38.5 (28.9–48.1) | 109 |
| Drug | Drugs Dispensed (n = 212) | Drugs Prescribed (n = 212) | ||
|---|---|---|---|---|
| No. | % (95% CI) | No. | % (95% CI) | |
| Paracetamol | 162 | 76.4 (70.5–82.4) | 64 | 30.2 (23.8–36.6) |
| Ibuprofen | 46 | 21.7 (15.9–27.5) | 22 | 10.4 (6.0–14.7) |
| Acetylsalicylic acid | 1 | 0.5 (0.0–2.6) | 0 | 0.0 (0.0–1.7) |
| Cough medication | 67 | 31.6 (25.1–38.1) | 19 | 9.0 (3.8–13.0) |
| Antihistamines | 45 | 21.2 (14.5–27.0) | 16 | 7.5 (2.7–7.2) |
| Epinephrine | 13 | 6.1 (2.7–9.6) | 2 | 0.9 (0.1–3.4) |
| Antibiotic | 14 | 6.6 (3.0–10.2) | 14 | 6.6 (3.0–10.2) |
| Antiseptic | 5 | 2.4 (0.8–5.4) | 1 | 0.5 (0.0–2.6) |
| Mucolytic | 10 | 4.7 (1.6–7.8) | 8 | 3.8 (1.0–6.6) |
| Medicinal plants | 5 | 2.4 (0.8–5.4) | 1 | 0.6 (0.0–2.6) |
| Bronchodilator | 5 | 2.4 (0.8–5.4) | 3 | 1.4 (0.3–4.1) |
| Anti-inflammatory | 5 | 2.4 (0.8–5.4) | 2 | 0.9 (0.1–3.4) |
| Oseltamivir | 1 | 0.5 (0.0–2.6) | 1 | 0.5 (0.0–2.6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Plans Rubió, P.; Jambrina, A.M.; Rius, P.; Carmona, G.; Rabanal, M.; Gironès, M. High Influenza Vaccine Effectiveness and Absence of Increased Influenza-like-Illness Epidemic Activity in the 2021–2022 Influenza Season in Catalonia (Spain) Based on Surveillance Data Collected by Sentinel Pharmacies. Vaccines 2022, 10, 2140. https://doi.org/10.3390/vaccines10122140
Plans Rubió P, Jambrina AM, Rius P, Carmona G, Rabanal M, Gironès M. High Influenza Vaccine Effectiveness and Absence of Increased Influenza-like-Illness Epidemic Activity in the 2021–2022 Influenza Season in Catalonia (Spain) Based on Surveillance Data Collected by Sentinel Pharmacies. Vaccines. 2022; 10(12):2140. https://doi.org/10.3390/vaccines10122140
Chicago/Turabian StylePlans Rubió, Pedro, Anna M. Jambrina, Pilar Rius, Gloria Carmona, Manel Rabanal, and Montse Gironès. 2022. "High Influenza Vaccine Effectiveness and Absence of Increased Influenza-like-Illness Epidemic Activity in the 2021–2022 Influenza Season in Catalonia (Spain) Based on Surveillance Data Collected by Sentinel Pharmacies" Vaccines 10, no. 12: 2140. https://doi.org/10.3390/vaccines10122140