

Parental Seasonal Influenza Vaccine Hesitancy and Associated Factors in Shanghai, China, during the COVID-19 Pandemic: A Cross-Sectional Study

 ,
,
Abstract
:1. Introduction
2. Methods
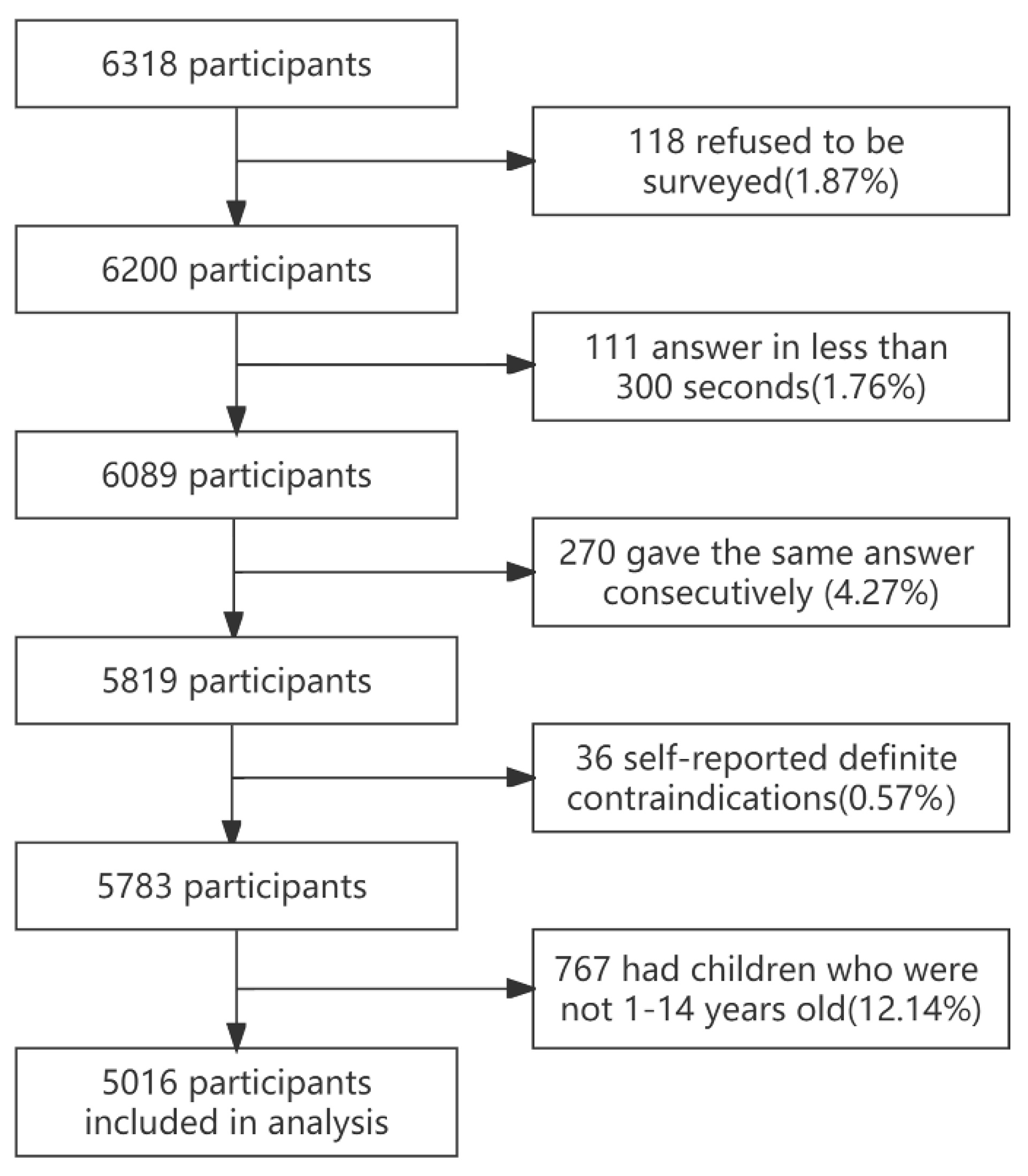
2.1. Study Design and Participants
2.2. Measures
- (1)
- Basic information on the parents, including age, gender, household location, education level, occupation, income, self-assessed health status, number of children, age of the youngest child, gender of the child, influenza illness history, and influenza and COVID-19 vaccination history.
- (2)
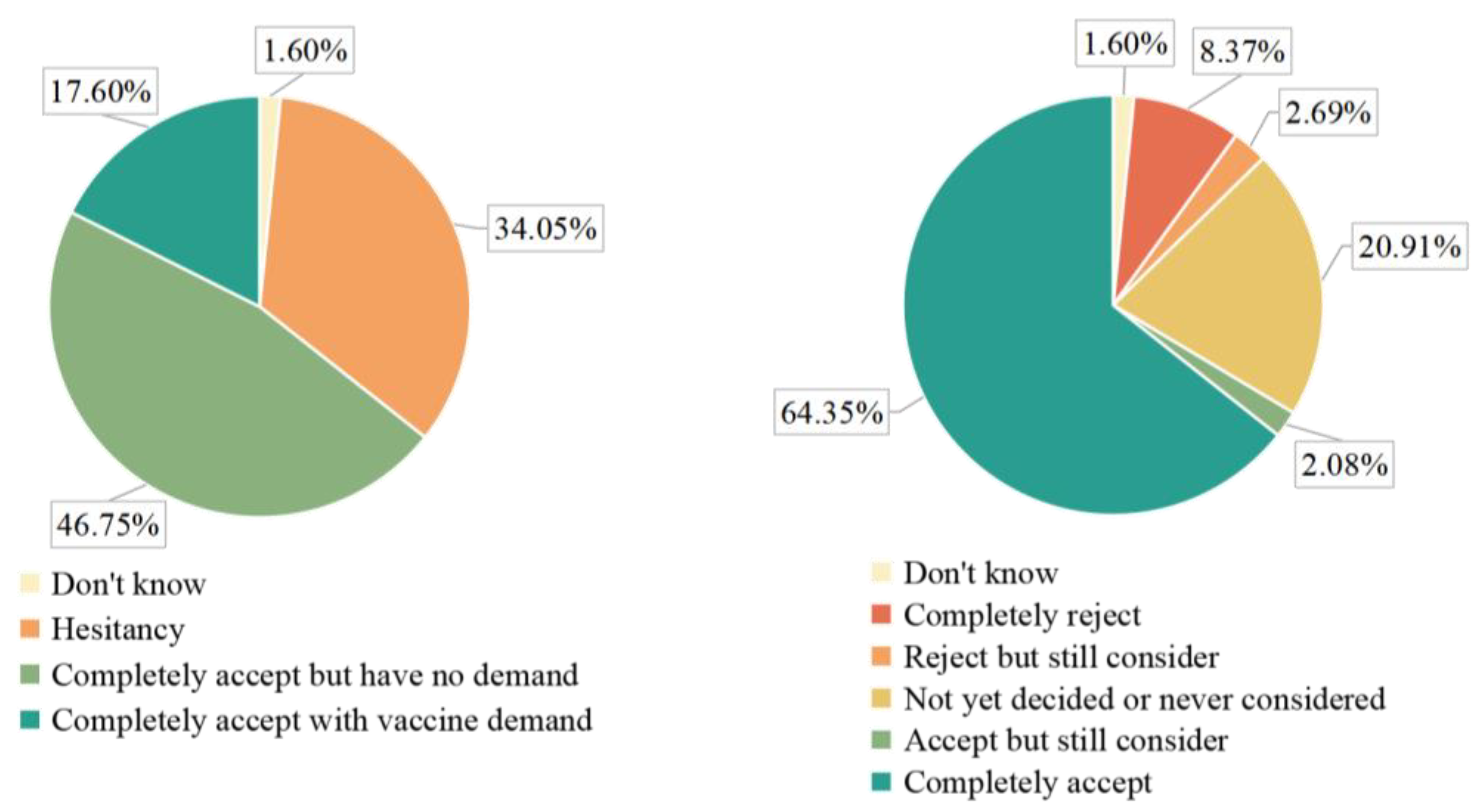
- The extent of IVH was assessed using a five-point Likert question, “Your willingness to get your child vaccinated against influenza in the coming year (2022/2023 influenza season),” which was determined based on responses classified as (i) complete rejecting, (ii) rejecting but still considering (inclined to reject), (iii) undecided or never considered (neutral), (iv) accepted but still considering (inclined to accept), and (v) complete accepted. Respondents judged to have choices 1, 2, 3, and 4 in this study were considered IVH. The question was followed by two additional multiple-choice questions about why the child was not vaccinated last year and about future IVH. In addition, we included the concept of influenza vaccine demand (IVD), meaning complete acceptance of influenza vaccine and actively seeking influenza vaccination services. Those who were utterly receptive and received the influenza vaccine the last year (2021/2022 influenza season) were expected to have “potential” IVD because future vaccination schedules were uncertain and those who had previously received the vaccine showed greater vaccine demand [22].
- (3)
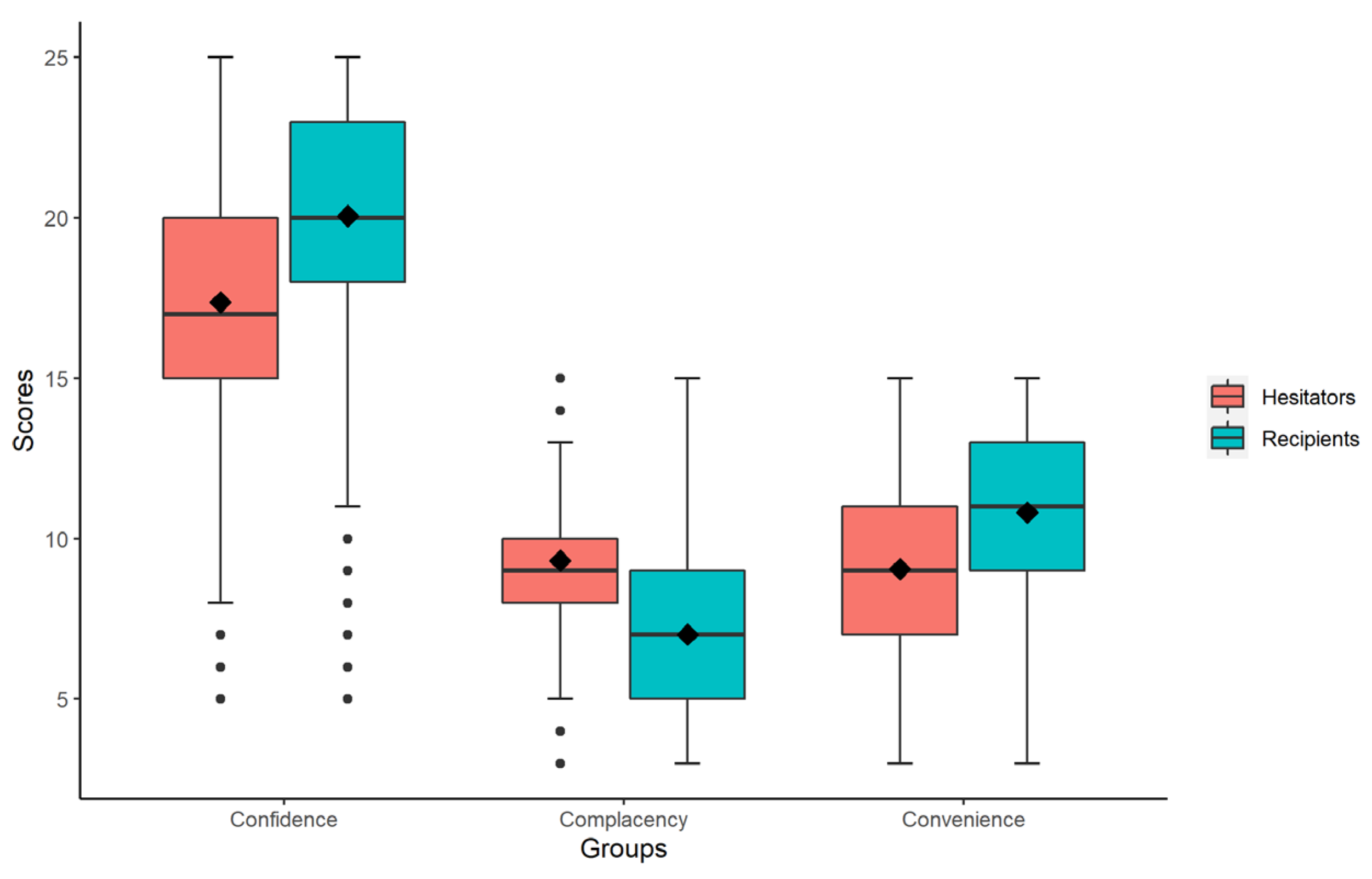
- We used a scale based on the “3C” model (containing the dimensions of confidence, complacency, and convenience) to measure parental IVH characteristics scores [15]. The scale was theoretically guided by the SAGE “3C” model concerning previous studies [22,28] and was revised based on literature reading, resident interviews, and expert consultations. “Confidence” refers to faith in the safety and efficacy of vaccines and the vaccination system. “Complacency” refers to the lack of awareness of the need for and importance of vaccination. “Convenience” refers to vaccine affordability, geographic accessibility, and quality of immunization services. A Likert 5-point scale was used, with complete disagreement, relative disagreement, fair, relative agreement, and complete agreement, corresponding to a score of 1–5, respectively, and items in the complacency section were scored in reverse.
- (4)
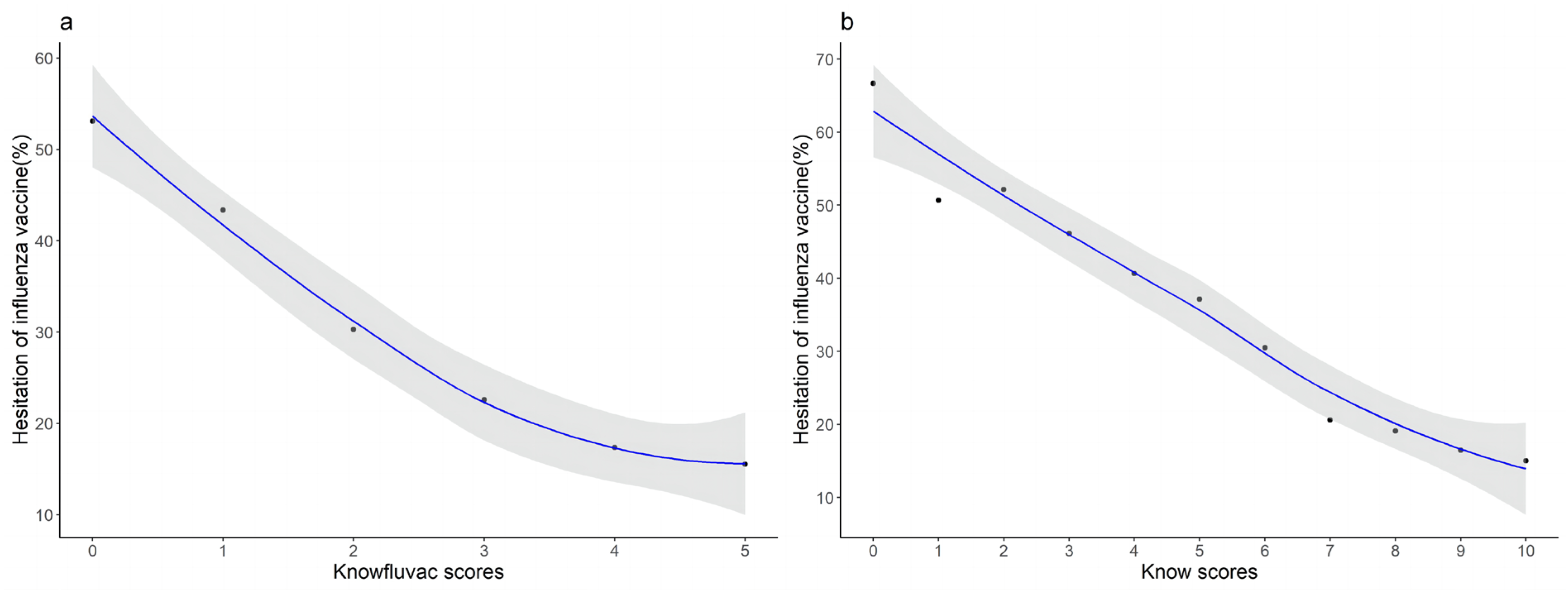
- Possible predictors of IVH (such as knowledge, experience to vaccinate, and influence from others and society). For knowledge about influenza infection and the influenza vaccine, we set five questions each, totaling ten. Knowledge about influenza infection in children included concepts, transmission routes, symptoms, and preventive measures; learning about the influenza vaccine, including age, the best time, the interval, and doses of vaccination. The level of knowledge was divided into three levels according to scores: 0 to 1 was low, 2 to 3 was moderate, and 4 to 5 was high. Regarding overall knowledge, a total score of 0 to 2 was low, 3 to 6 was mild, and 7 to 10 was high. In addition, we used the question “Have you heard of the flu vaccine?” to determine “do not know” and a multiple-choice question “What is the main source of information about flu and flu vaccine?” to determine the information channels.
3. Quality Control and Statistical Analysis
4. Results
4.1. Sociodemographic Characteristics of the Participants
4.2. Parental Influenza Vaccine Hesitancy
4.3. Predictors of Influenza Vaccine Hesitancy
4.4. Information Channels, Reasons for Not Being Vaccinated Last Year, and Future IVH
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Iuliano, A.D.; Roguski, K.M.; Chang, H.H.; Muscatello, D.J.; Palekar, R.; Tempia, S.; Cohen, C.; Gran, J.M.; Schanzer, D.; Cowling, B.J.; et al. Estimates of global seasonal influenza-associated respiratory mortality: A modelling study. Lancet 2018, 391, 1285–1300. [Google Scholar] [CrossRef] [PubMed]
- Somes, M.P.; Turner, R.M.; Dwyer, L.J.; Newall, A.T. Estimating the annual attack rate of seasonal influenza among unvaccinated individuals: A systematic review and meta-analysis. Vaccine 2018, 36, 3199–3207. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Li, Y.; O’Brien, K.L.; Madhi, S.A.; Widdowson, M.A.; Byass, P.; Omer, S.B.; Abbas, Q.; Ali, A.; Amu, A.; et al. Global burden of respiratory infections associated with seasonal influenza in children under 5 years in 2018: A systematic review and modelling study. Lancet Glob. Health 2020, 8, e497–e510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roman, P.C.; Kirtland, K.; Zell, E.R.; Jones-Jack, N.; Shaw, L.; Shrader, L.; Sprague, C.; Schultz, J.; Le, Q.; Nalla, A.; et al. Influenza Vaccinations During the COVID-19 Pandemic-11 U.S. Jurisdictions, September–December 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1575–1578. [Google Scholar] [CrossRef] [PubMed]
- National Immunization Advisory Committee (NIAC) Technical Working Group (TWG), Influenza Vaccination TWG. Technical Guidelines for Seasonal Influenza Vaccination in China (2022–2023). Available online: https://www.chinacdc.cn/jkzt/crb/bl/lxxgm/jszl_2251/202208/t20220825_260956.html (accessed on 25 August 2022).
- World Health Organization. Vaccines against influenza: WHO position paper-May 2022. Wkly. Epidemiol. Rec. 2022, 19, 185–208. [Google Scholar]
- Grohskopf, L.A.; Blanton, L.H.; Ferdinands, J.M.; Chung, J.R.; Broder, K.R.; Talbot, H.K.; Morgan, R.L.; Fry, A.M. Prevention and Control of Seasonal Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices-United States, 2022–2023 Influenza Season. MMWR Recomm. Rep. 2022, 71, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Yue, N.; Zheng, M.; Wang, D.; Duan, C.; Yu, X.; Zhang, X.; Bao, C.; Jin, H. Influenza vaccination coverage of population and the factors influencing influenza vaccination in mainland China: A meta-analysis. Vaccine 2018, 36, 7262–7269. [Google Scholar] [CrossRef]
- Imburgia, T.M.; Hendrix, K.S.; Donahue, K.L.; Sturm, L.A.; Zimet, G.D. Predictors of influenza vaccination in the U.S. among children 9-13years of age. Vaccine 2017, 35, 2338–2342. [Google Scholar] [CrossRef]
- Gates, D.M.; Cohen, S.A.; Orr, K.; Caffrey, A.R. Pediatric influenza vaccination rates lower than previous estimates in the United States. Vaccine 2022, 40, 6337–6343. [Google Scholar] [CrossRef]
- Shibata, N.; Kimura, S.; Hoshino, T.; Takeuchi, M.; Urushihara, H. Effectiveness of influenza vaccination for children in Japan: Four-year observational study using a large-scale claims database. Vaccine 2018, 36, 2809–2815. [Google Scholar] [CrossRef]
- Santibanez, T.A.; Srivastav, A.; Zhai, Y.; Singleton, J.A. Trends in Childhood Influenza Vaccination Coverage, United States, 2012–2019. Public Health Rep. 2020, 135, 640–649. [Google Scholar] [CrossRef] [PubMed]
- Yan, S.; Wang, Y.; Zhu, W.; Zhang, L.; Gu, H.; Liu, D.; Zhu, A.; Xu, H.; Hao, L.; Ye, C. Barriers to influenza vaccination among different populations in Shanghai. Hum. Vaccines Immunother. 2021, 17, 1403–1411. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 10 January 2019).
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Phadke, V.K.; Bednarczyk, R.A.; Salmon, D.A.; Omer, S.B. Association Between Vaccine Refusal and Vaccine-Preventable Diseases in the United States: A Review of Measles and Pertussis. JAMA 2016, 315, 1149–1158. [Google Scholar] [CrossRef] [Green Version]
- Hopkins Tanne, J. Measles: Two US outbreaks are blamed on low vaccination rates. BMJ 2019, 364, l312. [Google Scholar] [CrossRef] [PubMed]
- Yu, W.; Cao, L.; Liu, Y.; Li, K.; Rodewald, L.; Zhang, G.; Wang, F.; Cao, L.; Li, Y.; Cui, J.; et al. Two media-reported vaccine events in China from 2013 to 2016: Impact on confidence and vaccine utilization. Vaccine 2020, 38, 5541–5547. [Google Scholar] [CrossRef]
- The, L. Vaccine scandal and confidence crisis in China. Lancet 2018, 392, 360. [Google Scholar] [CrossRef]
- Du, F.; Chantler, T.; Francis, M.R.; Sun, F.Y.; Zhang, X.; Han, K.; Rodewald, L.; Yu, H.; Tu, S.; Larson, H.; et al. The determinants of vaccine hesitancy in China: A cross-sectional study following the Changchun Changsheng vaccine incident. Vaccine 2020, 38, 7464–7471. [Google Scholar] [CrossRef]
- Kempe, A.; Saville, A.W.; Albertin, C.; Zimet, G.; Breck, A.; Helmkamp, L.; Vangala, S.; Dickinson, L.M.; Rand, C.; Humiston, S.; et al. Parental Hesitancy About Routine Childhood and Influenza Vaccinations: A National Survey. Pediatrics 2020, 146, e20193852. [Google Scholar] [CrossRef]
- Wei, Z.; Sun, X.; Yang, Y.; Zhan, S.; Fu, C. Seasonal influenza vaccine hesitancy profiles and determinants among Chinese children’s guardians and the elderly. Expert Rev. Vaccines 2021, 20, 601–610. [Google Scholar] [CrossRef]
- Wang, Q.; Xiu, S.; Zhao, S.; Wang, J.; Han, Y.; Dong, S.; Huang, J.; Cui, T.; Yang, L.; Shi, N.; et al. Vaccine Hesitancy: COVID-19 and Influenza Vaccine Willingness among Parents in Wuxi, China-A Cross-Sectional Study. Vaccines 2021, 9, 342. [Google Scholar] [CrossRef]
- Goldman, R.D.; McGregor, S.; Marneni, S.R.; Katsuta, T.; Griffiths, M.A.; Hall, J.E.; Seiler, M.; Klein, E.J.; Cotanda, C.P.; Gelernter, R.; et al. Willingness to Vaccinate Children against Influenza after the Coronavirus Disease 2019 Pandemic. J. Pediatr. 2021, 228, 87–93.e82. [Google Scholar] [CrossRef]
- Salawati, E.; Alwafi, H.; Samannodi, M.; Minshawi, F.; Gari, A.; Abualnaja, S.; Almatrafi, M.A. Parents’ Willingness to Vaccinate Their Children Against Seasonal Influenza After the COVID-19 Pandemic in Saudi Arabia: A Retrospective Cross-Sectional Survey. Patient Prefer. Adherence 2021, 15, 2821–2835. [Google Scholar] [CrossRef]
- Seiler, M.; Goldman, R.D.; Staubli, G.; Hoeffe, J.; Gualco, G.; Manzano, S. Parents’ intent to vaccinate against influenza during the COVID-19 pandemic in two regions in Switzerland. Swiss Med. Wkly. 2021, 151, w20508. [Google Scholar] [CrossRef]
- Sokol, R.L.; Grummon, A.H. COVID-19 and Parent Intention to Vaccinate Their Children Against Influenza. Pediatrics 2020, 146, e2020022871. [Google Scholar] [CrossRef]
- Quinn, S.C.; Jamison, A.M.; An, J.; Hancock, G.R.; Freimuth, V.S. Measuring vaccine hesitancy, confidence, trust and flu vaccine uptake: Results of a national survey of White and African American adults. Vaccine 2019, 37, 1168–1173. [Google Scholar] [CrossRef]
- Schmid, P.; Rauber, D.; Betsch, C.; Lidolt, G.; Denker, M.L. Barriers of Influenza Vaccination Intention and Behavior—A Systematic Review of Influenza Vaccine Hesitancy, 2005–2016. PLoS ONE 2017, 12, e0170550. [Google Scholar] [CrossRef] [Green Version]
- Guay, M.; Gosselin, V.; Petit, G.; Baron, G.; Gagneur, A. Determinants of vaccine hesitancy in Quebec: A large population-based survey. Hum. Vaccines Immunother. 2019, 15, 2527–2533. [Google Scholar] [CrossRef]
- Rey, D.; Fressard, L.; Cortaredona, S.; Bocquier, A.; Gautier, A.; Peretti-Watel, P.; Verger, P. Vaccine hesitancy in the French population in 2016, and its association with vaccine uptake and perceived vaccine risk-benefit balance. Eurosurveillance 2018, 23, 17–00816. [Google Scholar] [CrossRef] [Green Version]
- Han, Y.; Wang, Q.; Zhao, S.; Wang, J.; Dong, S.; Cui, T.; Liu, M.; Shi, N.; Yang, L.; Han, Y.; et al. Parental category B vaccine hesitancy and associated factors in China: An online cross-sectional survey. Expert Rev. Vaccines 2022, 21, 145–153. [Google Scholar] [CrossRef]
- Damnjanović, K.; Graeber, J.; Ilić, S.; Lam, W.Y.; Lep, Ž.; Morales, S.; Pulkkinen, T.; Vingerhoets, L. Parental Decision-Making on Childhood Vaccination. Front. Psychol. 2018, 9, 735. [Google Scholar] [CrossRef]
- Ma, L.; Han, X.; Ma, Y.; Yang, Y.; Xu, Y.; Liu, D.; Yang, W.; Feng, L. Decreased influenza vaccination coverage among Chinese healthcare workers during the COVID-19 pandemic. Infect. Dis. Poverty 2022, 11, 105. [Google Scholar] [CrossRef]
- Janssen, C.; Mosnier, A.; Gavazzi, G.; Combadière, B.; Crépey, P.; Gaillat, J.; Launay, O.; Botelho-Nevers, E. Coadministration of seasonal influenza and COVID-19 vaccines: A systematic review of clinical studies. Hum. Vaccines Immunother. 2022, 2131166. [Google Scholar] [CrossRef]
- Salem, M.L.; El-Hennawy, D. The possible beneficial adjuvant effect of influenza vaccine to minimize the severity of COVID-19. Med. Hypotheses 2020, 140, 109752. [Google Scholar] [CrossRef]
- Smith, L.E.; Webster, R.K.; Weinman, J.; Amlôt, R.; Yiend, J.; Rubin, G.J. Psychological factors associated with uptake of the childhood influenza vaccine and perception of post-vaccination side-effects: A cross-sectional survey in England. Vaccine 2017, 35, 1936–1945. [Google Scholar] [CrossRef] [Green Version]
- Ren, J.; Wagner, A.L.; Zheng, A.; Sun, X.; Boulton, M.L.; Huang, Z.; Zikmund-Fisher, B.J. The demographics of vaccine hesitancy in Shanghai, China. PLoS ONE 2018, 13, e0209117. [Google Scholar] [CrossRef]
- Yufika, A.; Wagner, A.L.; Nawawi, Y.; Wahyuniati, N.; Anwar, S.; Yusri, F.; Haryanti, N.; Wijayanti, N.P.; Rizal, R.; Fitriani, D.; et al. Parents’ hesitancy towards vaccination in Indonesia: A cross-sectional study in Indonesia. Vaccine 2020, 38, 2592–2599. [Google Scholar] [CrossRef]
- Jing, L.; Na, Y.; Qing, H. Influenza vaccine hesitancy among parents of children in primary/secondary schools and kindergartens in Guiyang city: A “3C” model-based analysis. Chin. J. Public Health 2022, 38, 705. [Google Scholar] [CrossRef]
- Helmkamp, L.J.; Szilagyi, P.G.; Zimet, G.; Saville, A.W.; Gurfinkel, D.; Albertin, C.; Breck, A.; Vangala, S.; Kempe, A. A validated modification of the vaccine hesitancy scale for childhood, influenza and HPV vaccines. Vaccine 2021, 39, 1831–1839. [Google Scholar] [CrossRef]
- Fogel, B.; Schaefer, E.W.; Hicks, S.D. Early influenza vaccination rates decline in children during the COVID-19 pandemic. Vaccine 2021, 39, 4291–4295. [Google Scholar] [CrossRef]
- De Albuquerque Veloso Machado, M.; Roberts, B.; Wong, B.L.H.; van Kessel, R.; Mossialos, E. The Relationship Between the COVID-19 Pandemic and Vaccine Hesitancy: A Scoping Review of Literature Until August 2021. Front. Public Health 2021, 9, 747787. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sociodemographic Characteristics | N | % |
|---|---|---|
| Age (years) | ||
| <30 | 174 | 3.69 |
| 30–40 | 2797 | 59.30 |
| 40–50 | 1658 | 35.15 |
| ≥50 | 88 | 1.87 |
| Gender | ||
| Father | 1178 | 23.48 |
| Mother | 3838 | 76.52 |
| Household Registration | ||
| Shanghai | 3353 | 66.85 |
| Other areas (≥6 months of residence) | 1663 | 33.15 |
| Education level | ||
| Junior high school and below | 517 | 10.31 |
| High school or equivalent | 985 | 19.64 |
| Bachelor’s degree or equivalent | 2939 | 58.59 |
| Master’s degree or above | 575 | 11.46 |
| Health care worker | ||
| No | 4715 | 94.00 |
| Yes | 301 | 6.00 |
| Teacher | ||
| No | 4815 | 95.99 |
| Yes | 201 | 4.01 |
| Monthly per capita household income 2 (RMB 1) | ||
| <2000 | 124 | 2.47 |
| 2000–5000 | 572 | 11.40 |
| 5000–10,000 | 1566 | 31.22 |
| ≥10,000 | 2754 | 54.90 |
| Self-assessment of health status | ||
| Healthy or good | 4845 | 96.59 |
| General or weak | 171 | 3.41 |
| Number of children | ||
| 1 | 3160 | 63.00 |
| 2 | 1719 | 34.27 |
| ≥3 | 137 | 2.73 |
| Child’s age (years) | ||
| <3 | 700 | 13.96 |
| 3–5 | 828 | 16.51 |
| 5–7 | 1015 | 20.24 |
| 7–12 | 1363 | 27.17 |
| 12–14 | 1110 | 22.13 |
| Child’s gender | ||
| Male | 2680 | 53.43 |
| Female | 2336 | 46.57 |
| Self-assessment of child health status | ||
| Healthy or good | 4772 | 95.14 |
| General or weak | 244 | 4.86 |
| Dimensions | Total Score Average | IVH Status | t | p | OR (95%CI) | |
|---|---|---|---|---|---|---|
| Vaccine Hesitant (IVH = 1) | Vaccine Acceptant (IVH = 0) | |||||
| Confidence | 19.13 ± 4.05 | 17.37 ± 3.76 | 20.06 ± 3.90 | 23.329 | <0.001 | 0.839 (0.826–0.853) |
| Safety | 3.64 ± 0.98 | 3.20 ± 0.92 | 3.87 ± 0.92 | 24.179 | <0.001 | 0.470 (0.438–0.503) |
| Effectiveness | 7.58 ± 1.72 | 6.86 ± 1.62 | 7.97 ± 1.65 | 22.657 | <0.001 | 0.672 (0.647–0.698) |
| Trust in the vaccine delivery system | 7.91 ± 1.79 | 7.31 ± 1.78 | 8.22 ± 1.72 | 17.239 | <0.001 | 0.750 (0.725–0.777) |
| Complacency | 7.81 ± 2.56 | 9.32 ± 2.26 | 7.01 ± 2.34 | −33.649 | <0.001 | 1.549 (1.500–1.599) |
| No necessity | 5.26 ± 1.84 | 6.36 ± 1.58 | 4.67 ± 1.69 | −34.966 | <0.001 | 1.873 (1.790–1.960) |
| No severity | 2.55 ± 0.97 | 2.95 ± 0.95 | 2.34 ± 0.91 | −21.807 | <0.001 | 2.017 (1.883–2.161) |
| Convenience | 10.21 ± 2.58 | 9.06 ± 2.74 | 10.82 ± 2.26 | 22.775 | <0.001 | 0.746 (0.726–0.766) |
| Convenient transportation and time | 3.59 ± 1.09 | 2.92 ± 1.01 | 3.95 ± 0.96 | 34.818 | <0.001 | 0.362 (0.338–0.389) |
| Suitable price | 3.02 ± 1.11 | 2.99 ± 1.18 | 3.03 ± 1.08 | 1.092 | 0.275 | 0.970 (0.920–1.023) |
| Good service quality | 3.60 ± 1.09 | 3.15 ± 1.09 | 3.84 ± 1.02 | 21.746 | <0.001 | 0.541 (0.510–0.575) |
| Characteristics | IVH = 1 n (%) | N | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|---|---|
| Unadjusted OR | 95%CI | p | Adjusted OR | 95%CI | p | |||
| Sociodemographic characteristics of parents | ||||||||
| Age (<30 years old) | 39 (23.4) | 167 | Ref | Ref | ||||
| 30–40 | 838 (30.5) | 2751 | 1.4 | (1.0–2.1) | 0.053 | 0.86 | (0.54–1.4) | 0.507 |
| 40–50 | 701 (42.9) | 1636 | 2.5 | (1.7–3.6) | <0.001 | 1.1 | (0.65–1.7) | 0.798 |
| ≥50 | 37 (43.0) | 86 | 2.5 | (1.4–4.3) | 0.001 | 1.3 | (0.64–2.7) | 0.455 |
| Gender (Male) | 386 (33.6) | 1150 | Ref | Ref | ||||
| Female | 1322 (34.9) | 3786 | 1.1 | (0.92–1.2) | 0.401 | 1.5 | (1.3–1.8) | <0.001 |
| Household Registration (Shanghai) | 1235 (37.4) | 3302 | Ref | Ref | ||||
| Other areas (Residence ≥ 6 months) | 473 (29.0) | 1634 | 0.68 | (0.60–0.78) | <0.001 | 0.74 | (0.62–0.88) | 0.001 |
| Education level (Junior high school and below) | 140 (27.8) | 504 | Ref | Ref | ||||
| High school or equivalent | 310 (32.0) | 969 | 1.2 | (0.97–1.6) | 0.096 | 1.3 | (0.97–1.8) | 0.073 |
| Bachelor’s degree or equivalent | 1035 (35.7) | 2896 | 1.4 | (1.2–1.8) | 0.001 | 2.1 | (1.5–2.9) | <0.001 |
| Master’s degree or above | 223 (39.3) | 567 | 1.7 | (1.3–2.2) | <0.001 | 2.1 | (1.4–3.1) | <0.001 |
| Health care worker (No) | 1611 (34.7) | 4639 | Ref | Ref | ||||
| Yes | 97 (32.7) | 297 | 0.91 | (0.71–1.2) | 0.468 | – | – | - |
| Teacher (No) | 1634 (34.4) | 4740 | Ref | Ref | ||||
| Yes | 74 (37.8) | 196 | 1.2 | (0.86–1.5) | 0.344 | – | – | - |
| Monthly per capita household income (<2000 RNB) | 52 (44.1) | 118 | Ref | Ref | ||||
| 2000–5000 | 168 (30.3) | 554 | 0.55 | (0.37–0.83) | 0.004 | 0.70 | (0.41–1.2) | 0.196 |
| 5000–10,000 | 519 (33.6) | 1543 | 0.64 | (0.44–0.94) | 0.022 | 0.74 | (0.45–1.2) | 0.240 |
| ≥10,000 | 969 (35.6) | 2721 | 0.70 | (0.48–1.0) | 0.062 | 0.85 | (0.51–1.41) | 0.526 |
| Number of children (1) | 1128 (36.3) | 3107 | Ref | Ref | ||||
| 2 | 538 (31.8) | 1694 | 0.82 | (0.72–0.93) | 0.002 | 0.98 | (0.82–1.2) | 0.785 |
| ≥3 | 42 (31.1) | 135 | 0.79 | (0.55–1.1) | 0.220 | 0.93 | (0.57–1.5) | 0.782 |
| Self-assessed health status (Healthy) | 1273 (33.1) | 3851 | Ref | Ref | ||||
| Good | 355 (38.7) | 917 | 1.3 | (1.1–1.5) | 0.001 | 1.1 | (0.87–1.3) | 0.581 |
| General or weak | 80 (47.6) | 168 | 1.8 | (1.4–2.5) | <0.001 | 1.1 | (0.74–1.7) | 0.586 |
| Child’s age (<3 years old) | 161 (23.5) | 686 | Ref | Ref | ||||
| 3–5 | 208 (25.5) | 817 | 1.1 | (0.88–1.4) | 0.372 | 1.3 | (0.96–1.8) | 0.085 |
| 5–7 | 294 (29.4) | 1001 | 1.4 | (1.1–1.7) | 0.007 | 1.3 | (0.96–1.7) | 0.090 |
| 7–12 | 524 (39.1) | 1342 | 2.1 | (1.7–2.6) | <0.001 | 1.9 | (1.4–2.6) | <0.001 |
| 12–14 | 521 (47.8) | 1090 | 3.0 | (2.4–3.7) | <0.001 | 2.4 | (1.7–3.4) | <0.001 |
| Child’s gender (Male) | 907 (34.3) | 2641 | Ref | Ref | ||||
| Female | 801 (34.9) | 2295 | 1.0 | (0.91–1.2) | 0.681 | 1.00 | (0.86–1.2) | 0.990 |
| Self-assessment of the child’s health status (Healthy) | 1588 (33.8) | 4697 | Ref | Ref | ||||
| General or weak | 120 (50.2) | 239 | 2.0 | (1.5–2.6) | <0.001 | 2.3 | (1.6–3.3) | <0.001 |
| Experience and willingness to get vaccinated | ||||||||
| Has the child had the flu in the last three years (No) | 1389 (34.3) | 4055 | ref | Ref | ||||
| Yes | 319 (36.2) | 881 | 1.1 | (0.94–1.3) | 0.269 | – | – | - |
| Did the child receive a flu vaccine for the 2021/2022 flu season (No) | 1656 (41.4) | 4001 | ref | Ref | ||||
| Yes | 52 (5.6) | 935 | 0.08 | (0.06–0.11) | <0.001 | 0.13 | (0.09–0.18) | <0.001 |
| The number of doses of the child’s COVID-19 vaccine (0 dose) | 698 (32.8) | 2129 | ref | Ref | ||||
| 1 dose | 90 (29.3) | 307 | 0.85 | (0.65–1.1) | 0.225 | 0.59 | (0.42–0.82) | 0.002 |
| 2 doses | 920 (36.8) | 2500 | 1.2 | (1.1–1.3) | 0.004 | 0.67 | (0.54–0.82) | <0.001 |
| Have you ever Refused or postponed free vaccinations for your child, except for illnesses or allergies (No) | 1109 (31.9) | 3479 | Ref | Ref | ||||
| Yes | 316 (37.3) | 847 | 1.3 | (1.1–1.5) | 0.003 | 1.2 | (0.95–1.4) | 0.132 |
| Uncertain | 283 (46.4) | 610 | 1.9 | (1.6–2.2) | <0.001 | 1.1 | (0.85–1.4) | 0.490 |
| Whether they think free vaccines are more important than self-pay vaccines (No) | 349 (28.7) | 1215 | Ref | Ref | ||||
| Yes | 606 (36.5) | 1660 | 1.4 | (1.2–1.7) | <0.001 | 1.1 | (0.90–1.4) | 0.315 |
| Uncertain | 753 (36.5) | 2061 | 1.4 | (1.2–1.7) | <0.001 | 1.0 | (0.78–1.2) | 0.679 |
| Knowledge | ||||||||
| Score on the flu infection knowledge test (Low) | 465 (44.4) | 1048 | Ref | Ref | ||||
| Moderate | 791 (36.8) | 2147 | 0.73 | (0.63–0.85) | <0.001 | 0.95 | (0.78–1.2) | 0.605 |
| High | 452 (26.0) | 1741 | 0.44 | (0.37–0.52) | <0.001 | 0.88 | (0.70–1.1) | 0.252 |
| Score on the flu vaccination knowledge test (Low) | 1162 (43.8) | 2652 | Ref | Ref | ||||
| Moderate | 462 (26.2) | 1763 | 0.46 | (0.40–0.52) | <0.001 | 0.59 | (0.50–0.71) | <0.001 |
| High | 84 (16.1) | 521 | 0.25 | (0.19–0.32) | <0.001 | 0.57 | (0.41–0.78) | <0.001 |
| Influences from others and society | ||||||||
| Have you ever been affected by negative news about the flu vaccine (No) | 659 (26.6) | 2481 | Ref | Ref | ||||
| Yes | 498 (40.7) | 1224 | 1.9 | (1.6–2.2) | <0.001 | 1.7 | (1.4–2.0) | <0.001 |
| Uncertain | 551 (44.8) | 1231 | 2.2 | (1.9–2.6) | <0.001 | 1.6 | (1.3–1.9) | <0.001 |
| Have you ever received a doctor-recommended influenza vaccine (No) | 938 (38.4) | 2445 | Ref | Ref | ||||
| Yes | 388 (23.6) | 1645 | 0.50 | (0.43–0.57) | <0.001 | 0.81 | (0.68–0.98) | 0.027 |
| Uncertain | 382 (45.2) | 846 | 1.3 | (1.1–1.5) | 0.001 | 1.0 | (0.81–1.3) | 0.870 |
| Have you ever been influenced by people around you to give your child a flu vaccination (No) | 897 (37.9) | 2368 | Ref | Ref | ||||
| Yes | 446 (25.0) | 1782 | 0.55 | (0.48–0.63) | <0.001 | 0.63 | (0.52–0.76) | <0.001 |
| Uncertain | 365 (46.4) | 786 | 1.4 | (1.2–1.7) | <0.001 | 0.90 | (0.70–1.2) | 0.431 |
| “3C” Factors | ||||||||
| Confidence (Low) | 857 (50.2) | 1581 | Ref | Ref | ||||
| Moderate | 559 (32.7) | 1664 | 0.43 | (0.37–0.49) | <0.001 | 0.79 | (0.66–0.96) | 0.017 |
| High | 292 (17.1) | 1691 | 0.18 | (0.15–0.21) | <0.001 | 0.66 | (0.52–0.83) | 0.001 |
| Complacency (Low) | 134 (7.9) | 1449 | Ref | Ref | ||||
| Moderate | 422 (24.7) | 1405 | 4.2 | (3.4–5.2) | <0.001 | 3.3 | (2.6–4.3) | <0.001 |
| High | 1152 (67.5) | 2082 | 12.2 | (10.0–14.8) | <0.001 | 7.3 | (5.7–9.4) | <0.001 |
| Convenience (Low) | 624 (36.5) | 1041 | Ref | Ref | ||||
| Moderate | 654 (38.3) | 1775 | 0.39 | (0.33–0.46) | <0.001 | 0.29 | (0.24–0.36) | <0.001 |
| High | 430 (25.2) | 2120 | 0.17 | (0.14–0.20) | <0.001 | 0.31 | (0.25–0.38) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fan, J.; Ye, C.; Wang, Y.; Qi, H.; Li, D.; Mao, J.; Xu, H.; Shi, X.; Zhu, W.; Zhou, Y. Parental Seasonal Influenza Vaccine Hesitancy and Associated Factors in Shanghai, China, during the COVID-19 Pandemic: A Cross-Sectional Study. Vaccines 2022, 10, 2109. https://doi.org/10.3390/vaccines10122109
Fan J, Ye C, Wang Y, Qi H, Li D, Mao J, Xu H, Shi X, Zhu W, Zhou Y. Parental Seasonal Influenza Vaccine Hesitancy and Associated Factors in Shanghai, China, during the COVID-19 Pandemic: A Cross-Sectional Study. Vaccines. 2022; 10(12):2109. https://doi.org/10.3390/vaccines10122109
Chicago/Turabian StyleFan, Jingyi, Chuchu Ye, Yuanping Wang, Hui Qi, Dong Li, Jun Mao, Hongmei Xu, Xiaojin Shi, Weiping Zhu, and Yixin Zhou. 2022. "Parental Seasonal Influenza Vaccine Hesitancy and Associated Factors in Shanghai, China, during the COVID-19 Pandemic: A Cross-Sectional Study" Vaccines 10, no. 12: 2109. https://doi.org/10.3390/vaccines10122109