
Optimization of Vaccination Clinics to Improve Staffing Decisions for COVID-19: A Time-Motion Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Sites
2.2. Data Source
2.3. Ethical Approval
2.4. Statistical Analysis
2.5. Model
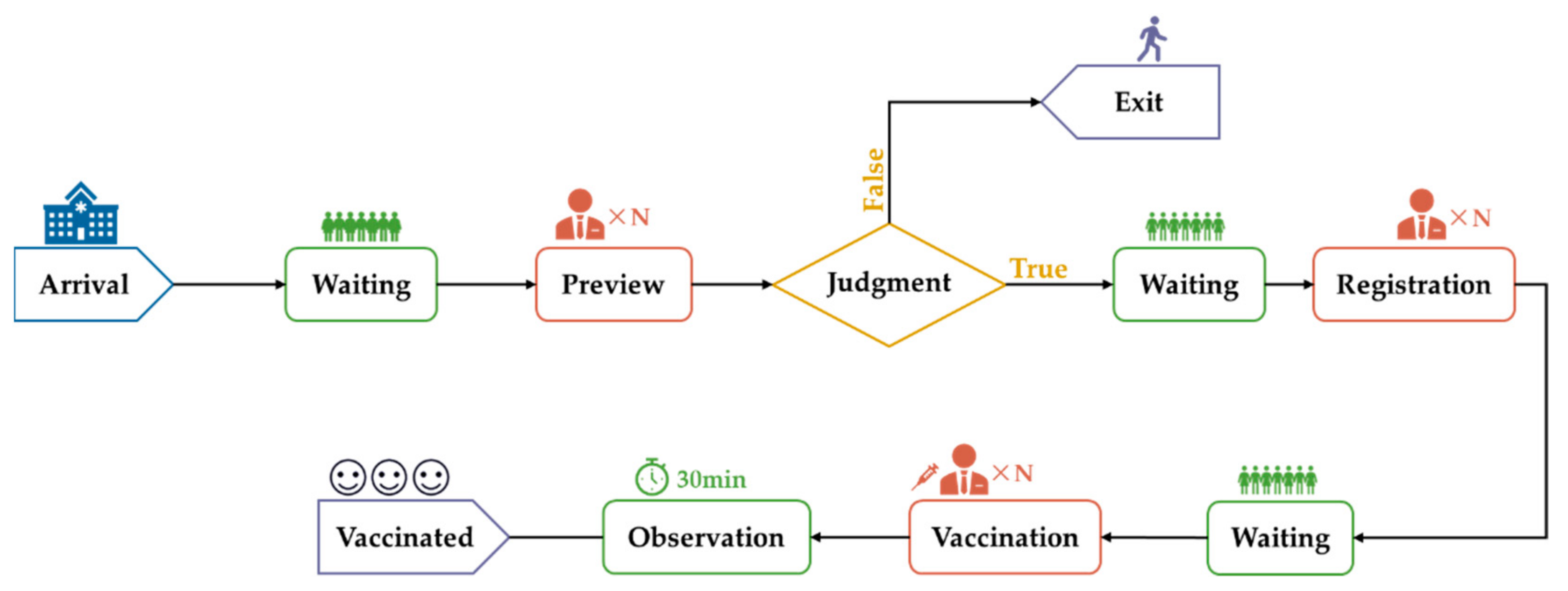
2.5.1. The Framework of a Discrete-Event Simulation Model
2.5.2. Parameter Setting
2.5.3. OptQuest Optimization
2.5.4. Scenario Setting
2.5.5. Optimal Staffing for Booster Dose Vaccination at Different Stages
3. Results
3.1. Actual Arrival Situation of Representative Clinics
3.2. Time Spent in Each Step in Clinics
3.2.1. Basic Information of Vaccination Clinics
3.2.2. Time Spent in Each Step at Different Vaccination Clinics
3.2.3. Time Spent on the Track Investigation
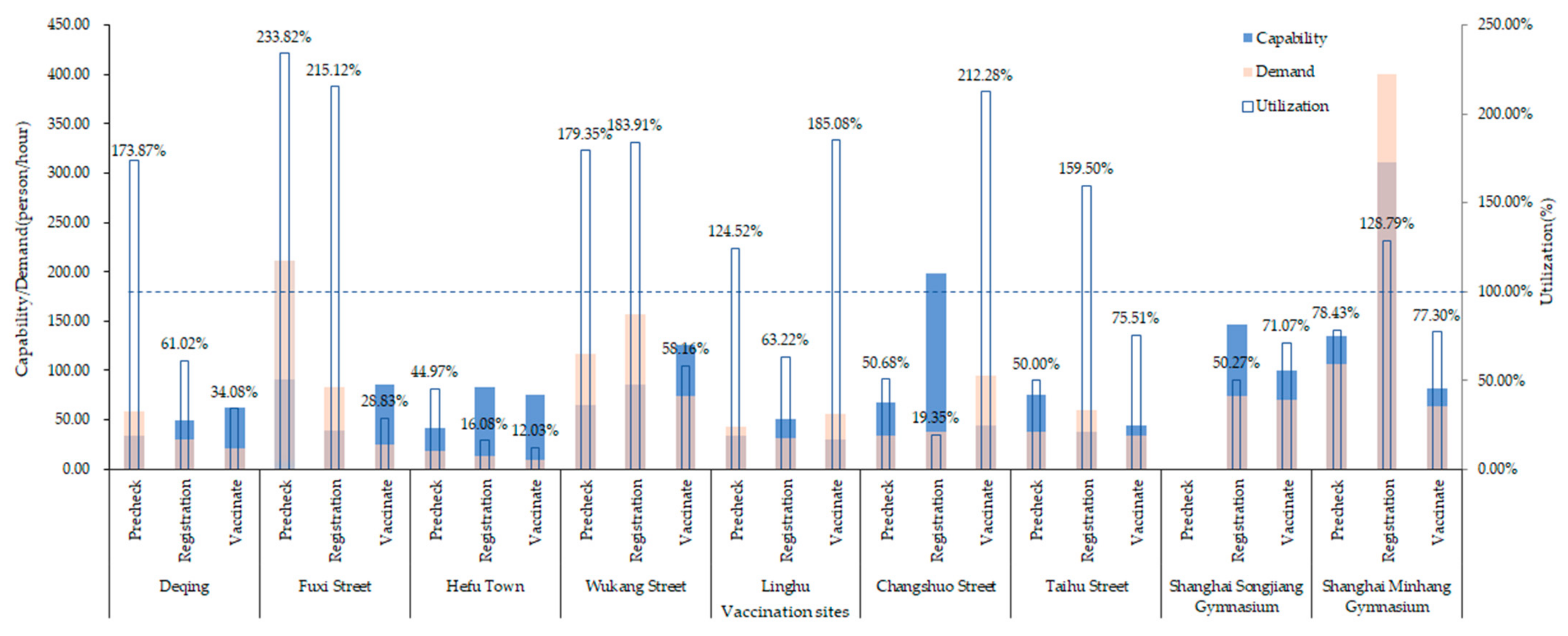
3.3. Capability, Demand and Utilization of Each Vaccination Clinic
3.4. Queuing Time at Each Clinic
3.5. Optimal Staffing under Different Scenarios
3.5.1. Scenarios 1 and 2
3.5.2. Scenarios 3–6
3.5.3. Scenarios 7–10
3.6. Capacity Assessment of Optimal Staffing
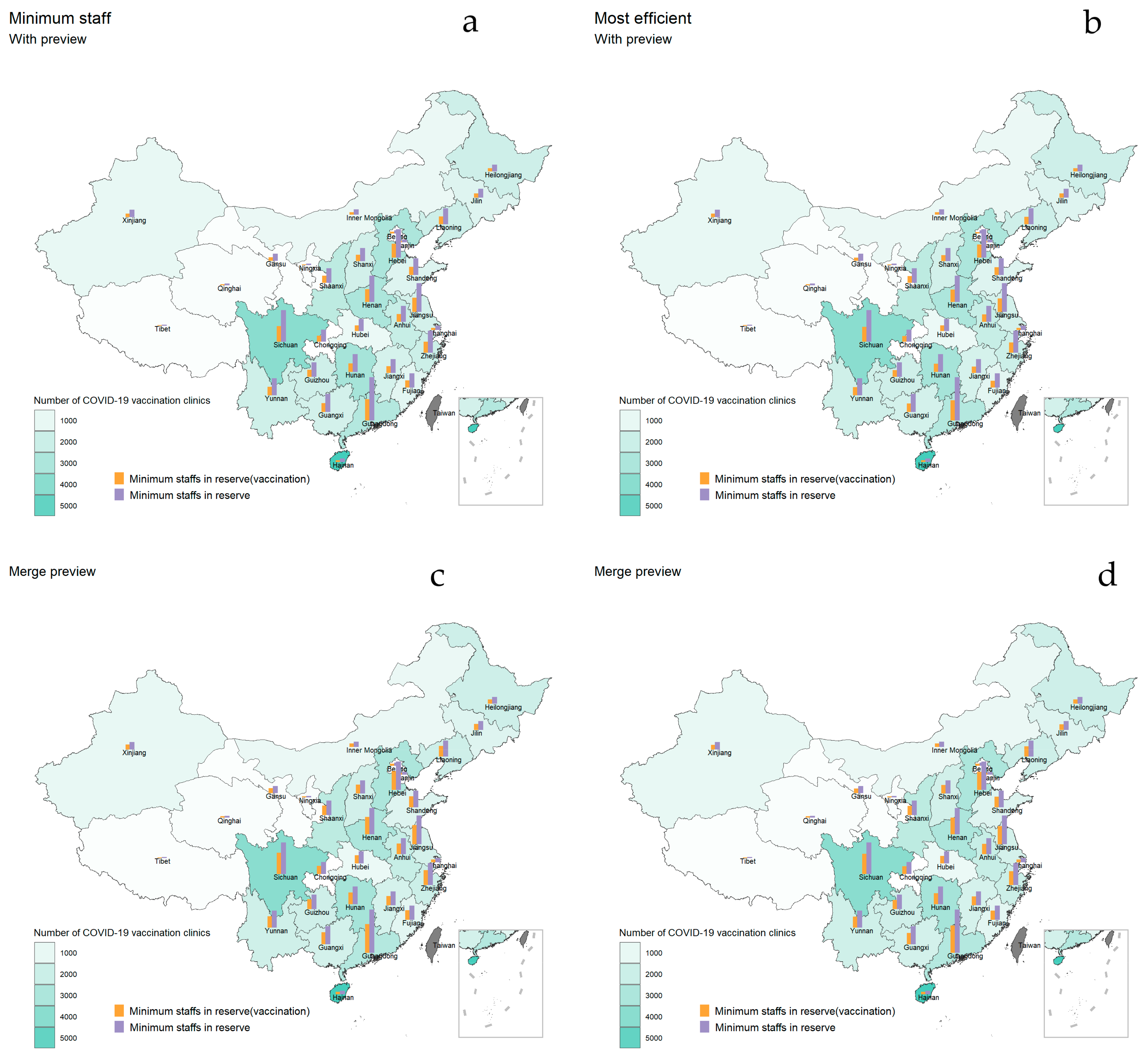
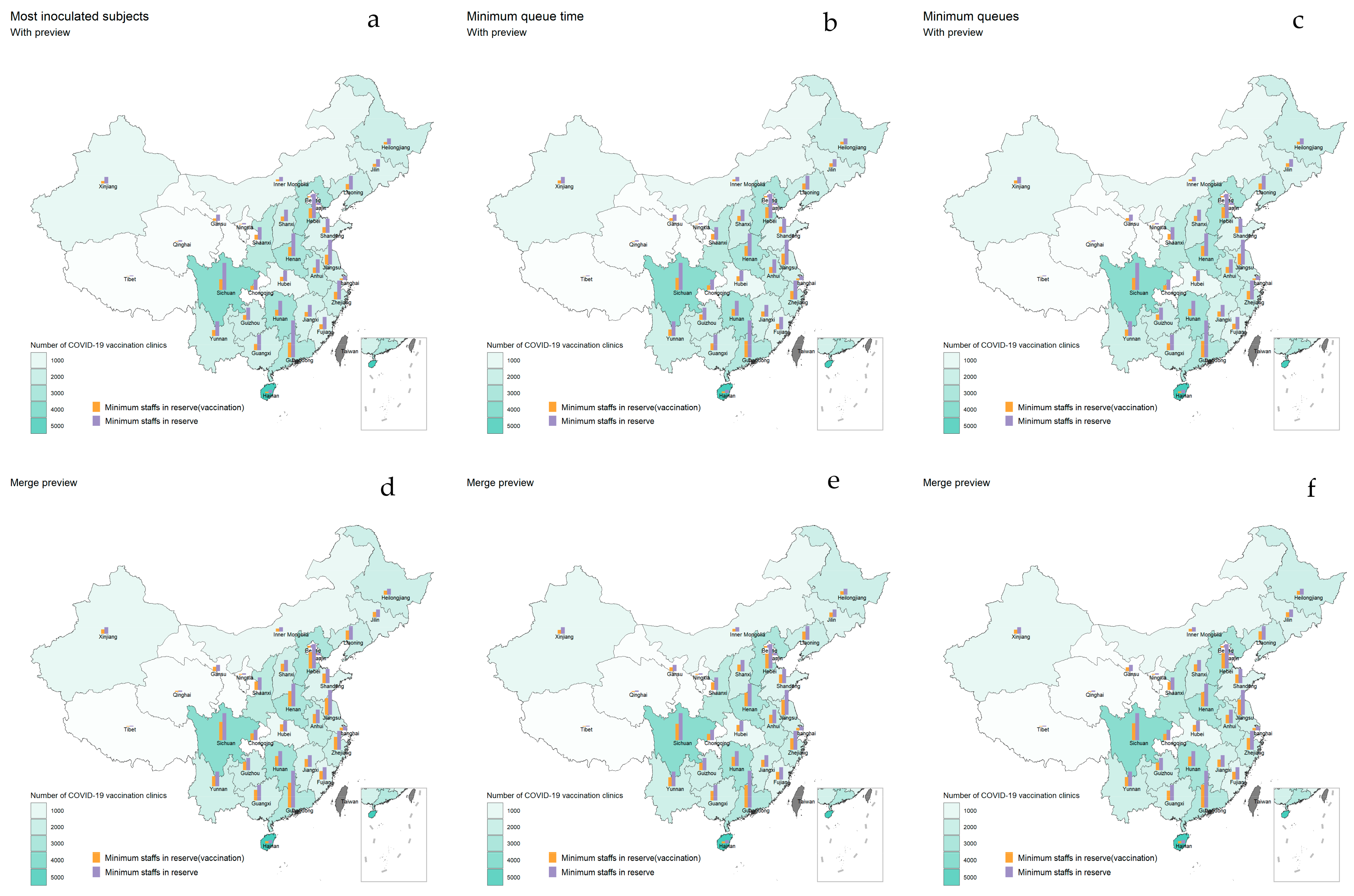
3.7. Optimization of Staffing for Booster Vaccination in China
3.7.1. Booster Vaccination Human Resource Situation and Progress Nationwide
3.7.2. Optimization of Staffing for Vaccination When Small-Scale Outbreaks Continued to Occur
3.7.3. Optimal Allocation of Vaccination Personnel for Booster When the Epidemic Was Stable
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 22 September 2022).
- Choi, J.Y.; Smith, D.M. SARS-CoV-2 variants of concern. Yonsei Med. J. 2021, 62, 961. [Google Scholar] [CrossRef] [PubMed]
- Davies, N.G.; Abbott, S.; Barnard, R.C.; Jarvis, C.I.; Kucharski, A.J.; Munday, J.D.; Pearson, C.A.B.; Russell, T.W.; Tully, D.C.; Washburne, A.D.; et al. Estimated transmissibility and impact of SARS-CoV-2 lineage B.1.1.7 in England. Science 2021, 372, eabg3055. [Google Scholar] [CrossRef] [PubMed]
- Dougherty, K.; Mannell, M.; Naqvi, O.; Matson, D.; Stone, J. SARS-CoV-2 B.1.617.2 (Delta) Variant COVID-19 Outbreak Associated with a Gymnastics Facility—Oklahoma, April-May 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1004–1007. [Google Scholar] [CrossRef] [PubMed]
- Meo, S.A.; Meo, A.S.; Al-Jassir, F.; Klonoff, D.C. Omicron SARS-CoV-2 new variant: Global prevalence and biological and clinical characteristics. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 8012–8018. [Google Scholar] [PubMed]
- Harvey, W.T.; Carabelli, A.M.; Jackson, B.; Gupta, R.; Thomson, E.C.; Harrison, E.M.; Ludden, C.; Reeve, R.; Rambaut, A.; Peacock, S.; et al. SARS-CoV-2 variants, spike mutations and immune escape. Nat. Rev. Microbiol. 2021, 19, 409–424. [Google Scholar] [CrossRef]
- Salazar, P.M.D.; Link, N.B.; Lamarca, K.; Santillana, M. High coverage COVID-19 mRNA vaccination rapidly controls SARS-CoV-2 transmission in long-term care facilities. Commun. Med. 2021, 1, 16. [Google Scholar] [CrossRef]
- Tenforde, M.W.; Patel, M.M.; Ginde, A.A.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; Mohr, N.M.; Zepeski, A.; Gaglani, M.; McNeal, T.; et al. Effectiveness of Severe Acute Respiratory Syndrome Coronavirus 2 Messenger RNA Vaccines for Preventing Coronavirus Disease 2019 Hospitalizations in the United States. Clin. Infect. Dis. 2022, 74, 1515–1524. [Google Scholar] [CrossRef]
- Sheikh, A.; McMenamin, J.; Taylor, B.; Robertson, C. SARS-CoV-2 Delta VOC in Scotland: Demographics, risk of hospital admission, and vaccine effectiveness. Lancet 2021, 397, 2461–2462. [Google Scholar] [CrossRef]
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Stowe, J.; Tessier, E.; Groves, N.; Dabrera, G.; et al. Effectiveness of COVID-19 Vaccines against the B.1.617.2 (Delta) Variant. N. Engl. J. Med. 2021, 385, 585–594. [Google Scholar] [CrossRef]
- Ella, R.; Reddy, S.; Blackwelder, W.; Potdar, V.; Yadav, P.; Sarangi, V.; Aileni, V.K.; Kanungo, S.; Rai, S.; Reddy, P.; et al. Efficacy, safety, and lot to lot immunogenicity of an inactivated SARS-CoV-2 vaccine (BBV152): A double-blind, randomised, controlled phase 3 trial. Lancet 2021, 398, 2173–2184. [Google Scholar] [CrossRef]
- Jara, A.; Undurraga, E.A.; González, C.; Paredes, F.; Fontecilla, T.; Jara, G.; Pizarro, A.; Acevedo, J.; Leo, K.; Leon, F.; et al. Effectiveness of an Inactivated SARS-CoV-2 Vaccine in Chile. N. Engl. J. Med. 2021, 385, 875–884. [Google Scholar] [CrossRef]
- Lusvarghi, S.; Pollett, S.D.; Neerukonda, S.N.; Wang, W.; Wang, R.; Vassell, R.; Epsi, N.J.; Fries, A.C.; Agan, B.K.; Lindholm, D.A.; et al. SARS-CoV-2 BA.1 variant is neutralized by vaccine booster-elicited serum, but evades most convalescent serum and therapeutic antibodies. Sci. Transl. Med. 2022, 14, eabn8543. [Google Scholar] [CrossRef]
- Zhang, H.J.; Ding, L.L.; Pan, X.J.; Shen, L.Z.; Zhu, Y.; Chen, F.X.; Fu, J.; Gao, F.; Lyu, H.K. Willingness to receive novel coronavirus vaccine and factors influencing willingness among healthcare workers in Zhejiang province. Chin. J. Vaccines Immun. 2021, 2, 1–7. [Google Scholar]
- Qian, Q.; Wang, Q.; Yang, L.Q.; Jin, H.; Xiu, S.X. Planned behavior theory based survey on the willingness of health care providers to receive COVID-19 vaccine and its influencing factors in Jiangsu province. Chin. Prev. Med. 2021, 22, 833–840. [Google Scholar]
- WHO Strategic Advisory Group of Experts on Immunization Updates Recommendations on Boosters, COVID-19 Vaccines for Children. Available online: https://www.paho.org/en/news/21-1-2022-who-strategic-advisory-group-experts-immunization-updates-recommendations-boosters (accessed on 22 September 2022).
- Washington, M.L.; Mason, J.; Meltzer, M.I. Maxi-Vac: Planning Mass Smallpox Vaccination Clinics. J. Public Health Manag. Pract. JPHMP 2004, 11, 542–549. [Google Scholar] [CrossRef]
- Asllani, A.; Dileepan, P.; Ettkin, L. A methodology for using simulation to optimize emergency mass vaccination parameters. Med. Syst. 2007, 31, 453–459. [Google Scholar] [CrossRef]
- Andress, K. A postevent smallpox mass vaccination clinic exercise. Disaster Manag. Response 2003, 1, 54–58. [Google Scholar] [CrossRef]
- Phillips, F.B.; Williamson, J.P. Local health department applies incident management system for successful mass influenza clinics. Public Health Manag. Pract. 2005, 11, 269–273. [Google Scholar] [CrossRef]
- Gelman, A.; Carlin, J.B.; Stern, H.S.; Dunson, D.B.; Vehtari, A.; Rubin, D.B. Bayesian Data Analysis; Academic Press: London, UK, 1995; Volume 1, Chapter 3; p. 75. [Google Scholar]
- Coelli, F.C.; Ferreira, R.B.; Almeida, R.M.; Pereira, W.C.A. Computer simulation and discrete-event models in the analysis of a mammography clinic patient flow. Comput. Methods Programs Biomed. 2007, 87, 201–207. [Google Scholar] [CrossRef]
- SilverCraft. OptQuest for Arena User Manua; Rockwell Automation Technologies, Inc.: Milwaukee, WI, USA, 2021. [Google Scholar]
- Ke, H.; Wang, L.P.; Sun, L.M. Survey on the current status of human resource in vaccination clinics in a district of Tianjin. Henan J. Prev. Med. 2021, 32, 136–138+143. [Google Scholar]
- You, J.F.; Cheng, T.; Tian, X.; Fu, S.M. Investigation and operation analysis of vaccination units in Jilin Province. Chin. J. Public Health Manag. 2021, 37, 77–80. [Google Scholar]
- Wang, C.S.; Lu, M.X.; Zhang, M.H.; Ma, Y.T.; Xiao, Z.P.; Wang, Y.; Zhang, Y.Y. Capacity of vaccination clinics for children in Henan Province. J. Prev. Med. 2020, 32, 1174–1177. [Google Scholar]
- Lu, J.; Zhao, J.; Chen, M.H. Investigation on the Service Capacity of Community Vaccination Clinic in Chongming District, Shanghai. China Mod. Med. 2021, 28, 216–219. [Google Scholar]
- Novel Coronavirus Vaccine Training Programme—Implementation of Novel Coronavirus Vaccine Organization with Setting up of Vaccination Units. Available online: http://www.nhc.gov.cn/jkj/s5899tg/202104/1619f941de034452a4b9bcaf307afd79.shtml (accessed on 22 September 2022).
- Hupert, N.; Mushlin, A.I.; Callahan, M.A. Modeling the public health response to bioterrorism: Using discrete event simulation to design antibiotic distribution centers. Med. Decis. Mak. 2002, 22 (Suppl. 5), S17–S25. [Google Scholar] [CrossRef]
- Beeler, M.F.; Aleman, D.M.; Carter, M.W. A Simulation Case Study to Improve Staffing Decisions at Mass Immunization Clinics for Pandemic Influenza; Palgrave Macmillan: London, UK, 2016. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Arrival Rate | With Preview Step 1 | Without Preview Step 2 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Vaccination Recipients | Preview | Registration | Vaccination | Total Staff | Vaccination Recipients | Registration | Vaccination | Total Staff | |
| 105 | 104 | 1 | 1 | 2 | 4 | 94 | 1 | 2 | 3 |
| 1009 | 945 | 5 | 4 | 6 | 15 | 947 | 4 | 7 | 11 |
| 3007 | 3077 | 9 | 8 | 13 | 30 | 3044 | 8 | 16 | 24 |
| Arrival Rate | Minimum Staff Number | Highest Efficiency | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| With Preview Step 1 | Without Preview Step 2 | With Preview Step 1 | Without Preview Step 2 | |||||||||||||||
| Vaccinated | Preview | Registration | Vaccination | Total Staff | Vaccinated | Registration | Vaccination | Total Staff | Vaccinated | Preview | Registration | Vaccination | Total Staff | Vaccinated | Registration | Vaccination | Total Staff | |
| 105 | 104 | 1 | 1 | 1 | 3 | 94 | 1 | 1 | 2 | 104 | 1 | 1 | 1 | 3 | 94 | 1 | 1 | 2 |
| 1009 | 920 | 4 | 4 | 6 | 14 | 936 | 4 | 6 | 10 | 935 | 4 | 4 | 6 | 14 | 936 | 4 | 6 | 10 |
| 3007 | 2901 | 8 | 8 | 16 | 32 | 2929 | 8 | 15 | 23 | 2901 | 9 | 8 | 14 | 31 | 2911 | 8 | 13 | 21 |
| Arrival Rate | Minimum Queuing Time | Minimum Queuing Number | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| With Preview Step 1 | Without Preview Step 2 | With Preview Step 1 | Without Preview Step 2 | |||||||||||||||
| Queuing Time | Preview | Registration | Vaccination | Total Staff | Queuing time | Registration | Vaccination | Total Staff | Queuing Number | Preview | Registration | Vaccination | Total Staff | Queuing number | Registration | Vaccination | Total Staff | |
| 105 | 0 | 1 | 1 | 2 | 4 | 0 | 1 | 2 | 3 | 0 | 1 | 1 | 2 | 4 | 0 | 1 | 2 | 3 |
| 1009 | 0.24 | 4 | 4 | 10 | 18 | 0.06 | 4 | 10 | 14 | 0 | 4 | 4 | 10 | 18 | 0 | 4 | 10 | 14 |
| 3007 | 0.24 | 8 | 10 | 18 | 36 | 0.42 | 10 | 18 | 28 | 1 | 9 | 10 | 18 | 37 | 3 | 9 | 18 | 27 |
| Arrival Rate | With Preview Step 1 | Without Preview Step 2 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Maximum Vaccination Recipients | Minimum Staff Number | Highest Efficiency | Maximum Vaccination Recipients | Minimum Staff Number | Highest Efficiency | |||||||
| Vaccination Recipients | Service Capacity | Vaccination Recipients | Service Capacity | Vaccination Recipients | Service Capacity | Vaccination Recipients | Service Capacity | Vaccination Recipients | Service Capacity | Vaccination Recipients | Service Capacity | |
| 105 | 104 | 1 | 104 | 1 | 104 | 1 | 94 | 0.9 | 94 | 0.9 | 94 | 0.9 |
| 1009 | 945 | 0.94 | 920 | 0.92 | 935 | 0.93 | 947 | 0.94 | 936 | 0.93 | 936 | 0.93 |
| 3007 | 3077 | 1.03 | 2901 | 0.97 | 2901 | 0.97 | 3044 | 1.02 | 2929 | 0.98 | 2911 | 0.97 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, X.; Pan, J.; Liu, Z.; Wang, W. Optimization of Vaccination Clinics to Improve Staffing Decisions for COVID-19: A Time-Motion Study. Vaccines 2022, 10, 2045. https://doi.org/10.3390/vaccines10122045
Wang X, Pan J, Liu Z, Wang W. Optimization of Vaccination Clinics to Improve Staffing Decisions for COVID-19: A Time-Motion Study. Vaccines. 2022; 10(12):2045. https://doi.org/10.3390/vaccines10122045
Chicago/Turabian StyleWang, Xinyu, Jinhua Pan, Zhixi Liu, and Weibing Wang. 2022. "Optimization of Vaccination Clinics to Improve Staffing Decisions for COVID-19: A Time-Motion Study" Vaccines 10, no. 12: 2045. https://doi.org/10.3390/vaccines10122045