
Clinical Presentation of COVID-19 and Antibody Responses in Bangladeshi Patients Infected with the Delta or Omicron Variants of SARS-CoV-2
 , , ,
, , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample Collections
2.2. Quantification of Viral RNA
2.3. The Spike Protein Variants
2.4. Assessment of Anti-SARS CoV-2 Antibodies
2.5. Statistical Analysis
3. Results
3.1. Bangladeshi COVID-19 Patient Characteristics
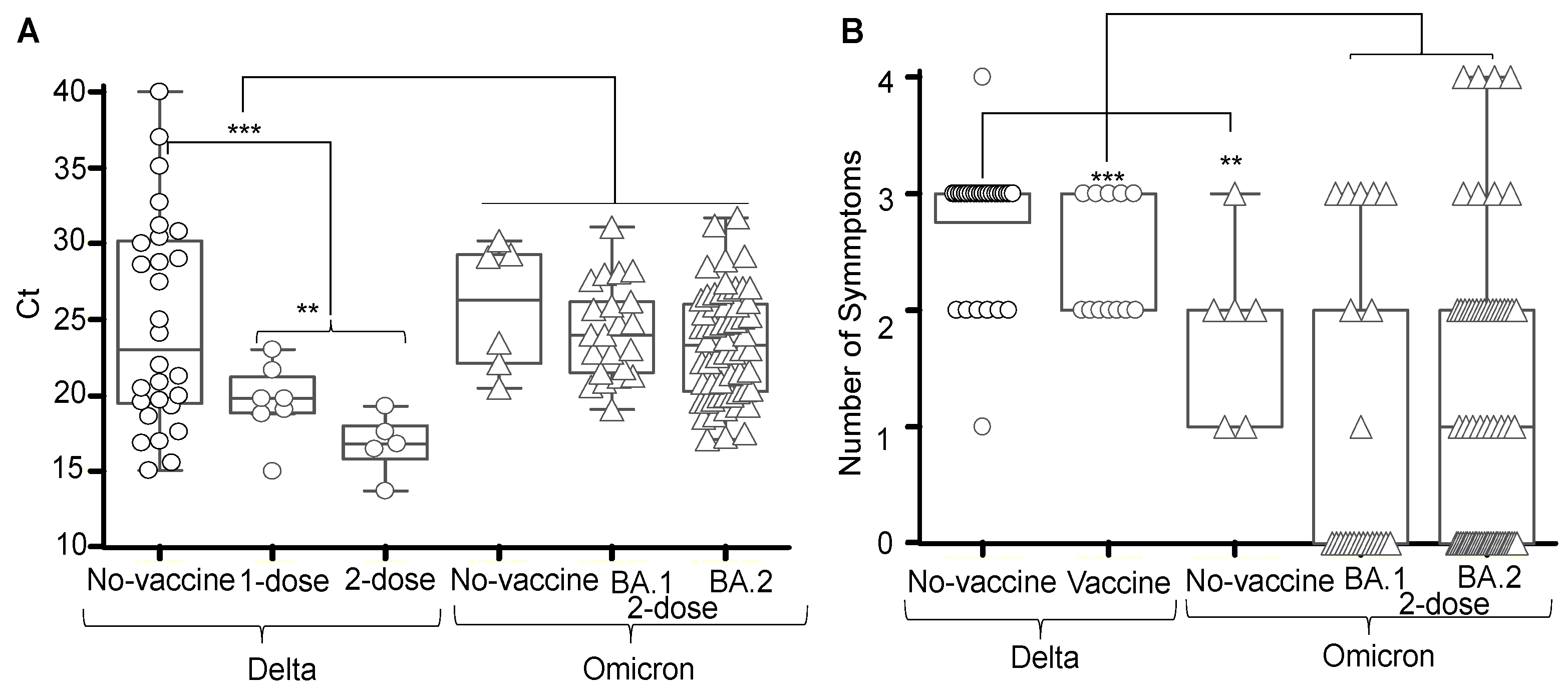
3.2. SARS CoV-2 Variants
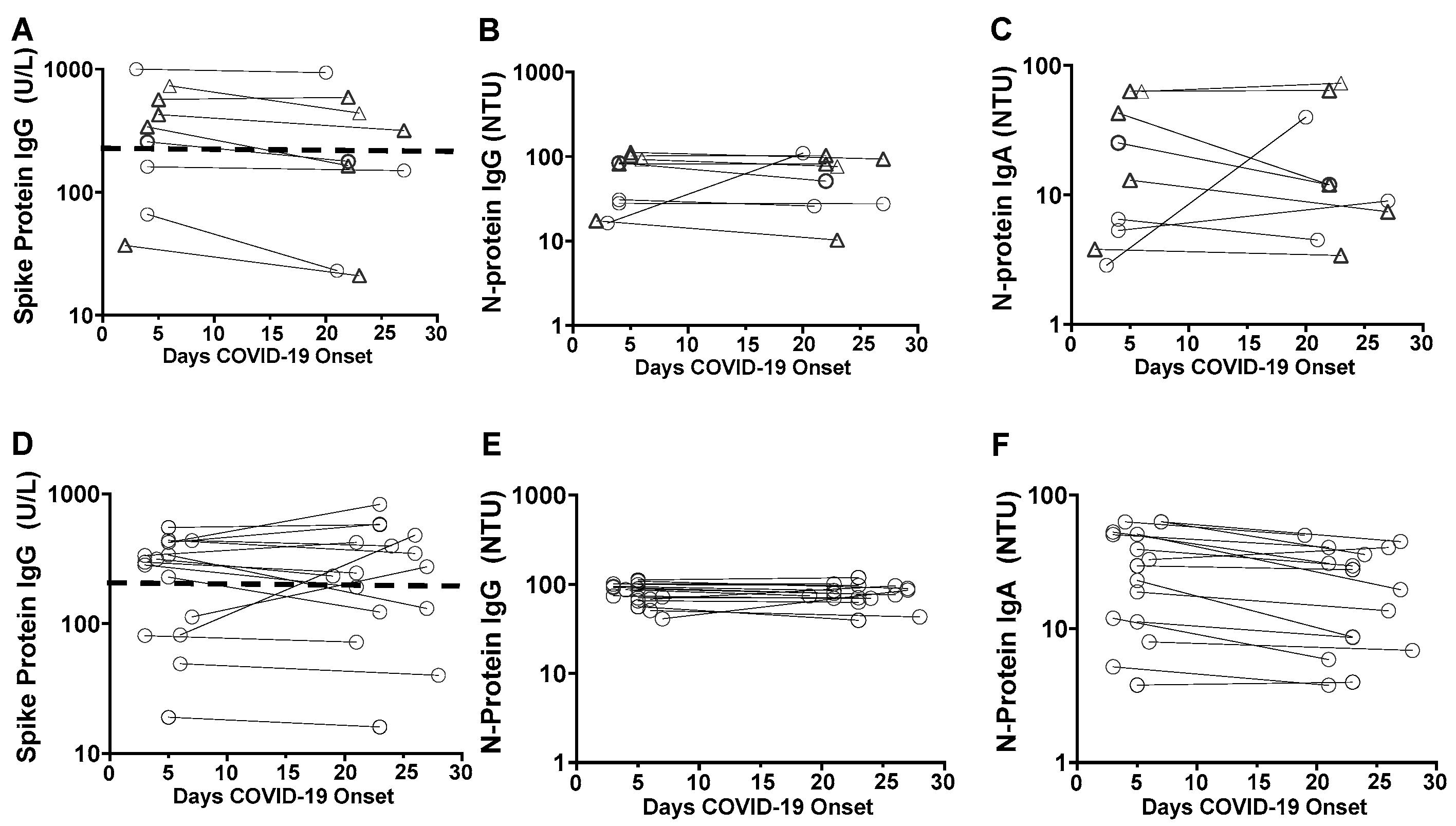
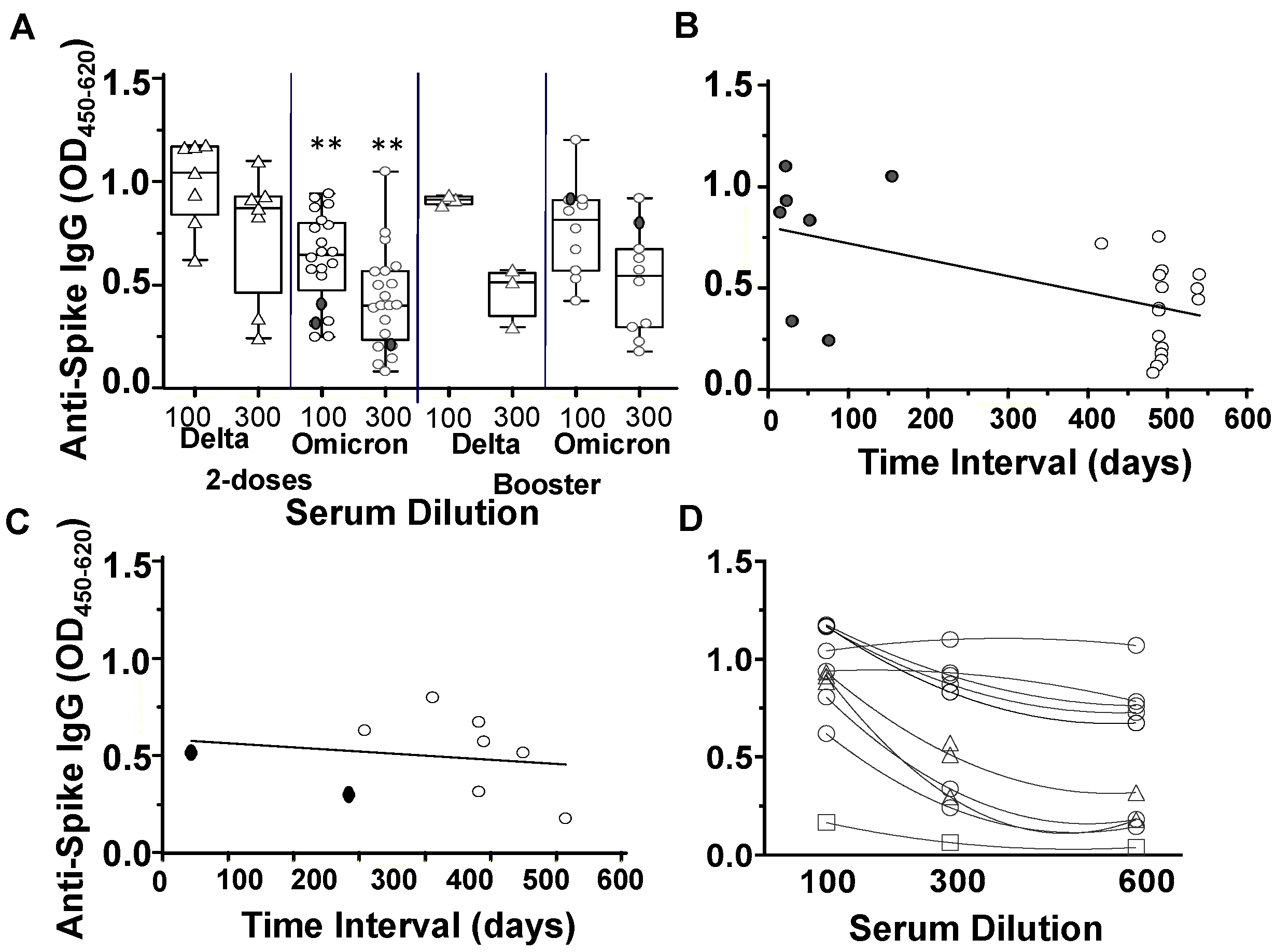
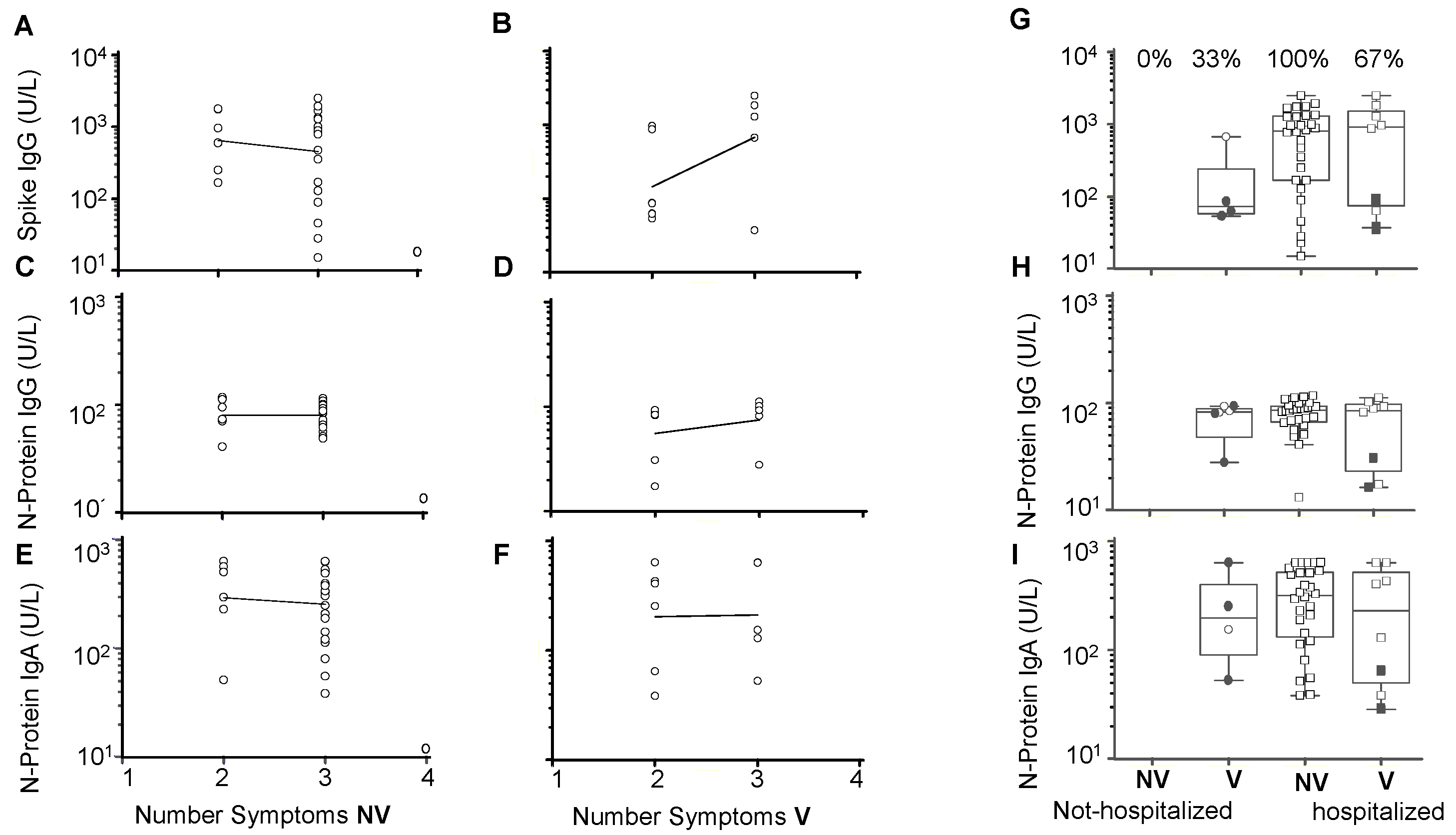
3.3. Antibody Responses in SARS-CoV-2 Variants
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Islam, M.R.; Hoque, M.N.; Rahman, M.S.; Alam, A.S.M.R.U.; Akther, M.; Puspo, J.A.; Akter, S.; Sultana, M.; Crandall, K.A.; Hossain, M.A. Genome-wide analysis of SARS-CoV-2 virus strains circulating worldwide implicates heterogeneity. Sci. Rep. 2020, 10, 14004. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Tracking SARS-CoV-2 Variants. Available online: https://www.who.int/activities/tracking-SARS-CoV-2-variants (accessed on 29 June 2022).
- Pango Network. Rules for the Designation and Naming of Pango Lineages. Available online: https://www.pango.network/the-pangonomenclature-system/statement-of-nomenclature-rules/ (accessed on 29 June 2022).
- Center for Disease Control and Prevention. Available online: https://www.cdc.gov/coronavirus/2019-ncov/variants/ (accessed on 29 June 2022).
- Lin, L.; Liu, Y.; Tang, X.; He, D. The disease severity and clinical outcomes of the SARS-CoV-2 variants of concern. Front. Pub Health 2021, 9, 775224. [Google Scholar] [CrossRef] [PubMed]
- Jassat, W.; Karim, S.S.A.; Mudara, C.; Welch, R.; Ozougwu, L. Clinical severity of COVID-19 in patients admitted to hospital during the omicron wave in South Africa: A retrospective observational study. Lancet 2022, 10, e961–e969. Available online: www.thelancet.com/infection (accessed on 18 October 2022).
- Bager, P.; Wohlfahrt, J.; Bhatt, S.; Stegger, M.; Legarth, R.; Møller, C.H.; Skov, R.L.; Valentiner-Branth, P.; Voldstedlund, M.; Fischer, T.K.; et al. Risk of hospitalisation associated with infection with SARS-CoV-2 omicron variant versus delta variant in Denmark: An observational cohort study. Lancet Infect. Dis. 2022, 22, 967–976. [Google Scholar] [CrossRef]
- Menni, C.; Valdes, A.M.; Polidori, L.; Antonelli, M.; Penamakuri, S.; Nogal, A.; Louca, P.; May, A.; Figueiredo, J.C.; Hu, C.; et al. Symptom prevalence, duration, and risk of hospital admission in individuals infected with SARS-CoV-2 during periods of omicron and delta variant dominance: A prospective observational study from the ZOE COVID Study. Lancet 2022, 399, 1618–1624. [Google Scholar]
- Silva, B.R.O.; Rodrigues, W.F.; Abadia, D.G.P.; da Silva, D.A.A.; e Silva, L.E.A.; Desidério, C.S.; Farnesi-De-Assunção, T.S.; Costa-Madeira, J.C.; Barbosa, R.M.; e Borges, A.V.B.; et al. Clinical-Epidemiology Aspect of Inpatients with Moderate or Severe COVID-19 in a Brazilian Macroregion: Disease and Countermeasures. Front. Cell. Infect. 2022, 12, 1–10. [Google Scholar] [CrossRef]
- Aoki, A.; Adachi, H.; Mori, Y.; Ito, M.; Sato, K.; Okuda, K.; Sakakibara, T.; Okamoto, Y.; Jinno, H. Discrimination of SARS-CoV-2 Omicron sub-lineages BA.1 and BA.2 using a 6 high-resolution melting-based assay: A pilot study. bioRxiv 2022. [Google Scholar] [CrossRef]
- Stang, A.; Robers, J.; Schonert, B.; Jöckel, K.-H.; Spelsberg, A.; Keil, U.; Cullen, P. The performance of the SARS-CoV-2 RT-PCR test as a tool for detecting SARS-CoV-2 infection in the population. J. Infect. 2021, 83, 237–279. [Google Scholar] [CrossRef]
- Sit, B.H.; Po, K.H.L.; Cheung, Y.-Y.; Tsang, A.K.L.; Leung, P.K.L.; Zheng, J.; Lam, A.Y.T.; Lam, E.T.K.; Ng, K.H.L.; Chan, R.C.W. Detection of SARS-CoV-2 VOC-Omicron using commercial sample-to-answer real-time RT-PCR platforms and melting curve-based SNP assays. J. Clin. Virol. Plus 2022, 2. [Google Scholar] [CrossRef]
- TIB-MOLBIOL. SARS Kits and VirSNiP Assays RT-PCR Test Kits and VirSNiP Mutation Assays for Strain Surveillance. Available online: https://www.tib-molbiol.de/covid-19. (accessed on 29 June 2022).
- Souza da Costa, C.H.; Beltrão de Freitas, C.A.; Alves, C.N.; Lameira, J. Assessment of mutations on RBD in the Spike protein of SARS-CoV-2 Alpha, Delta and Omicron variants. Nat. Sci. Rep. 2022, 12, 8540. [Google Scholar] [CrossRef]
- World Health Organization. WHO Coronavirus (COVID-19) Dash board/Global/Bangladesh. 2021. Available online: https://Covid19.who.int/region/searo/country/bd (accessed on 29 January 2022).
- Sayeed, M.A.; Ferdous, J.; Saha, O.; Islam, S.; Choudhury, S.D.; Abedin, J.; Hassan, M.M.; Islam, A. Transmission Dynamics and Genomic Epidemiology of Emerging Variants of SARS-CoV-2 in Bangladesh. Trop. Med. Infect. Dis. 2022, 7, 197. [Google Scholar] [CrossRef]
- Bangladesh Institute of Epidemiology, Disease Control and Research (IEDCR) SARS-CoV-2 Variants in Bangladesh Technical briefing Report. Available online: https://iedcr.gov.bd/nbph/issue-sections/e4c1ceb2-00b4-463b-98d8-cad2701c4f2f (accessed on 18 October 2022).
- Bin Manjur, O.H.; Afrad, M.H.; Khan, M.H.; Hossain, M.; Kawser, Z.; Alam, A.N.; Banik, N.; Alam, S.; Billah, M.M.; Afreen, N.; et al. Genome Sequences of 25 SARS-CoV-2 Sublineage B.1.1.529 Omicron Strains in Bangladesh. Microbiol. Resour. Announc. 2022, 11, 1–3. [Google Scholar] [CrossRef] [PubMed]
- John Hopkins University of Medicine Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/ (accessed on 18 October 2022).
- Islam, S.; Islam, T.; Islam, M.R. New Coronavirus Variants are Creating More Challenges to Global Healthcare System: A Brief Report on the Current Knowledge. Clin. Pathol. 2022, 15, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Islam, R. The SARS-CoV-2 Omicron (B.1.1.529) variant and the re-emergence of COVID-19 in Europe: An alarm for Bangladesh. Health Sci. Rep. 2022, 5, e545. [Google Scholar] [CrossRef] [PubMed]
- Daria, S.; Bhuiyan, M.A.; Islam, M.R. Detection of highly muted coronavirus variant Omicron (B.1.1.529) is triggering the alarm for South Asian countries: Associated risk factors and preventive actions. J. Med. Virol. 2022, 94, 1267–1268. [Google Scholar] [CrossRef] [PubMed]
- Saha, S.; Gulshan, J. Systematic assessment of COVID-19 pandemic in Bangladesh: Effectiveness of preparedness in the first wave. Frontiers 2021, 9, 1–13. [Google Scholar] [CrossRef]
- Balushi, A.; Al Ajmi, A.; Al Sinani, Q.; Menon, V.; Al Berieki, Z.; Al Shezawi, A.; Al Rashdi, A.; Al Jardani, A.; Al Baluki, T.; Al Ghaithi, S.; et al. COVID-19-associated mucomycosis: An opportunistic fungal infection. a case series and review. Int. J. Infect. Dis. 2022, 121, 203–210. [Google Scholar] [CrossRef]
- Salmanton-Garcia, J.; Sprute, R.; Stemler, J.; Bartoletti, M.; Dupont, D.; Valerio, M.; Garcia-Vidal, C.; Falces-Romero, I.; Machado, M.; de la Villa, S.; et al. COVID-19–Associated Pulmonary Aspergillosis, March-August 2020. Emerg. Infect. Dis. 2021, 27, 1078–1086. [Google Scholar] [CrossRef]
- Joshi, G.; Poduri, R. Omicron, a new SARS-CoV-2 variant: Assessing the impact on severity and vaccine efficacy. Hum. Vaccines Immunother. 2022, 18, e2034458. [Google Scholar] [CrossRef]
- Jung, C.; Kmiec, D.; Koepke, L.; Zech, F.; Jacob, T. Omicron: What Makes the Latest SARS-CoV-2 Variant of Concern So Concerning? J. Med. Virol. 2022, 96, e0207721. [Google Scholar] [CrossRef]
- Ghosh, A.K.; Kaiser, M.; Molla, M.A.; Nafisa, T.; Yeasmin, M.; Ratul, R.H.; Sharif, M.M.; Akram, A.; Hosen, N.; Mamunur, R.; et al. Molecular and Serological Characterization of the SARS-CoV-2 Delta Variant in Bangladesh in 2021. Viruses 2021, 13, 2310. [Google Scholar] [CrossRef]
- Fall, A.; Eldesouki, R.E.; Sachithanandham, J.; Morris, C.P.; Norton, J.M.; Gaston, D.C.; Forman, M.; Abdullah, O.; Gallagher, N.; Li, M.; et al. The Displacement of the SARS-CoV-2 Variant Delta with Omicron: An Investigation of Hospital Admissions and Upper Respiratory Viral Loads. eBioMedicine 2022, 79, 104008. [Google Scholar] [CrossRef] [PubMed]
- Kirsebom, F.C.M.; Andrews, N.; Stowe, J.; Toffa, S.; Sachdeva, R.; Gallagher, E.; Groves, N.; O’Connell, A.-M.; Chand, M.; Ramsay, M.; et al. COVID-19 vaccine effectiveness against the omicron (BA.2) variant in England. Lancet Infect. Dis. 2022, 22, 931–933. [Google Scholar] [CrossRef]
- Hsu, L.; Kossow, A.; Hoffmann, D.; Schildgen, O.; Schildgen, V. Limited protection against SARS-CoV-2 infection and virus transmission after mRNA vaccination. J. Infect. 2022, 84, 94–118. [Google Scholar] [CrossRef] [PubMed]
- Collier, A.Y.; Brown, C.M.; McMahan, C.A.; Yu, J.; Liu, J.; Jacob-Dolan, C.; Chandrashekar, A.; Tierney, D.; Ansel, J.L.; Rowe, M.; et al. Characterization of immune responses in fully vaccinated individuals after breakthrough infection with the SARS-CoV-2 delta variant. Sci. Transl. Med. 2022, 14, 1–10. [Google Scholar] [CrossRef]
- Barouch, D.H. Covid-19 Vaccines-Immunity, Variants, Boosters. N. Engl. J. Med. 2022, 387, 1011–1020. [Google Scholar] [CrossRef]
- McCallum, M.; Czudnochowski, N.; Rosen, L.E.; Zepeda, S.K.; Bowen, J.E.; Walls, A.C.; Hauser, K.; Joshi, A.; Stewart, C.; Dillen, J.R.; et al. Structural basis of SARS-CoV-2 Omicron immune evasion and receptor engagement. Science 2022, 375, 864–868. [Google Scholar] [CrossRef]
- Gopinath, S.; Ishak, A.; Dhawan, N.; Poudel, S.; Shrestha, P.S.; Singh, P.; Xie, E.; Tahir, P.; Marzaban, S.; Michel, J.; et al. Characteristics of COVID-19 Breakthrough Infections among Vaccinated Individuals and Associated Risk Factors: A Systematic Review. Trop. Med. Infect. Dis. 2022, 7, 81. [Google Scholar] [CrossRef]
- Townsend, J.P.; Hasslera, H.B.; Sahe, P.; Galvani, A.P.l.; Dornburg, A. The durability of natural infection and vaccine-induced immunity against future infection by SARS-CoV-2. Proc. Nat. Acad. Sci. USA 2022, 119, 1–8. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | SARS-CoV-2 RT-PCR Positive 2021 Group 1 | SARS-CoV-2 RT-PCR Positive 2022 Group 2 | p Value (1) | p Value (2) | |||
|---|---|---|---|---|---|---|---|
| No Vaccine | 1-dose | 2-dose | No Vaccine | 2-dose | |||
| Number of cases enrolled | 28 | 7 | 5 | 6 | 84 | ||
| Age Median (range) years | 50 (23–85) | 50 (24–62) | 50 (27–68) | 12 (7–95) | 37 (19–66) | 0.002 | 0.09 |
| Gender M/F | 11/17 | 4/3 | 5/0 | 2/4 | 73/11 | <0.0001 | 0.5 |
| Days POCS median (range) | 5 (1–7) | 4 (2–6) | 4 (3–6) | 3 (1–4) | 2 (1–4) | 0.0001 | 0.0001 |
| Hospitalized n (%) | 28 (100) | 6 (86) | 2 (40) | 0 (0) | 0 (0) | 0.0001 | 0.0001 |
| Difficulty breathing n (%) | 23 (82) | 4 (57) | 2 (40) | 0 (0) | 10 (12) | 0.0001 | 0.001 |
| Oxygen support n (%) | 23 (82) | 4 (57) | 2 (40) | 0 (0) | 0 (0) | 0.0001 | 0.0001 |
| Variant n (%) | |||||||
| Delta | 28 (100) | 7 (100) | 5 (100) | 0 (0) | 0 (0) | 0.0001 | 0.0001 |
| Omicron BA.1 | 0 (0) | 0 (0) | 0 (0) | 1 (17) | 22 (26) | ||
| Omicron BA.2 | 0 (0) | 0 (0) | 0 (0) | 5 (83) | 60 (72) | ||
| * Omicron mixed | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 2 (2) | ||
| COVID-19 symptoms n (%) | |||||||
| No symptoms | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 38 (45) | 0.0001 | 0.008 |
| Rhinitis | 0 (0) | 0 (0) | 0 (0) | 4 (67) | 27 (32) | 0.02 | 0.05 |
| Chest pain | 0 (0) | 2 (3) | 0 (0) | 0 (0) | 0 (0) | 0.9 | 0.9 |
| Breathlessness | 22 (79) | 4 (6) | 2 (40) | 0 (0) | 8 (10) | 0.0001 | 0.001 |
| Muscle or body pain or headache | 1 (3) | 1 (1.5) | 3 (60) | 1 (17) | 12 (14) | 0.25 | 0.21 |
| Nausea | 1 (3) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0.56 | 0.99 |
| Loss of smell and/or taste | 4 (14) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0.02 | 0.99 |
| Cough | 24 (86) | 6 (86) | 1 (20) | 4 (67) | 12 (14) | 0.017 | 0.001 |
| Fever | 27 (96) | 5 (71) | 5 (100) | 3 (50) | 32 (38) | 0.0001 | 0.009 |
| Antibody Positivity Days Post Onset of COVID-19 Symptoms (POCS) | SARS-CoV-2 RT-PCR Positive 2021 Group 1 | |||
|---|---|---|---|---|
| Non- Vaccinated | 1-dose Vaccine | 2-dose Vaccine | p Value | |
| SARS-CoV-2 NP IgA n (%) | ||||
| Day 1–7 | 23 (82) | 6 (86) | 2 (40) | 0.12 |
| Day 19–27 | 10 (62) | 5 (60) | 2 (50) | 0.98 |
| SARS-CoV-2 NP IgG n (%) | ||||
| Day 1–7 | 28 (100) | 7 (100) | 5 (100) | - |
| Day 19–27 | 16 (100) | 5 (80) | 4 (100) | - |
| SARS-CoV-2 S IgG Quant n (%) | ||||
| Day 1–7 | 28 (100) | 7 (100) | 5 (100) | - |
| Day 19–27 | 16 (100) | 5 (80) | 4 (100) | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghosh, A.K.; Landt, O.; Yeasmin, M.; Sharif, M.; Ratul, R.H.; Molla, M.A.; Nafisa, T.; Mosaddeque, M.B.; Hosen, N.; Bulbul, M.R.H.; et al. Clinical Presentation of COVID-19 and Antibody Responses in Bangladeshi Patients Infected with the Delta or Omicron Variants of SARS-CoV-2. Vaccines 2022, 10, 1959. https://doi.org/10.3390/vaccines10111959
Ghosh AK, Landt O, Yeasmin M, Sharif M, Ratul RH, Molla MA, Nafisa T, Mosaddeque MB, Hosen N, Bulbul MRH, et al. Clinical Presentation of COVID-19 and Antibody Responses in Bangladeshi Patients Infected with the Delta or Omicron Variants of SARS-CoV-2. Vaccines. 2022; 10(11):1959. https://doi.org/10.3390/vaccines10111959
Chicago/Turabian StyleGhosh, Asish Kumar, Olfert Landt, Mahmuda Yeasmin, Mohiuddin Sharif, Rifat Hossain Ratul, Maruf Ahmed Molla, Tasnim Nafisa, Mymuna Binte Mosaddeque, Nur Hosen, Md. Rakibul Hassan Bulbul, and et al. 2022. "Clinical Presentation of COVID-19 and Antibody Responses in Bangladeshi Patients Infected with the Delta or Omicron Variants of SARS-CoV-2" Vaccines 10, no. 11: 1959. https://doi.org/10.3390/vaccines10111959