

Persisting Vaccine Hesitancy in Africa: The Whys, Global Public Health Consequences and Ways-Out—COVID-19 Vaccination Acceptance Rates as Case-in-Point
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
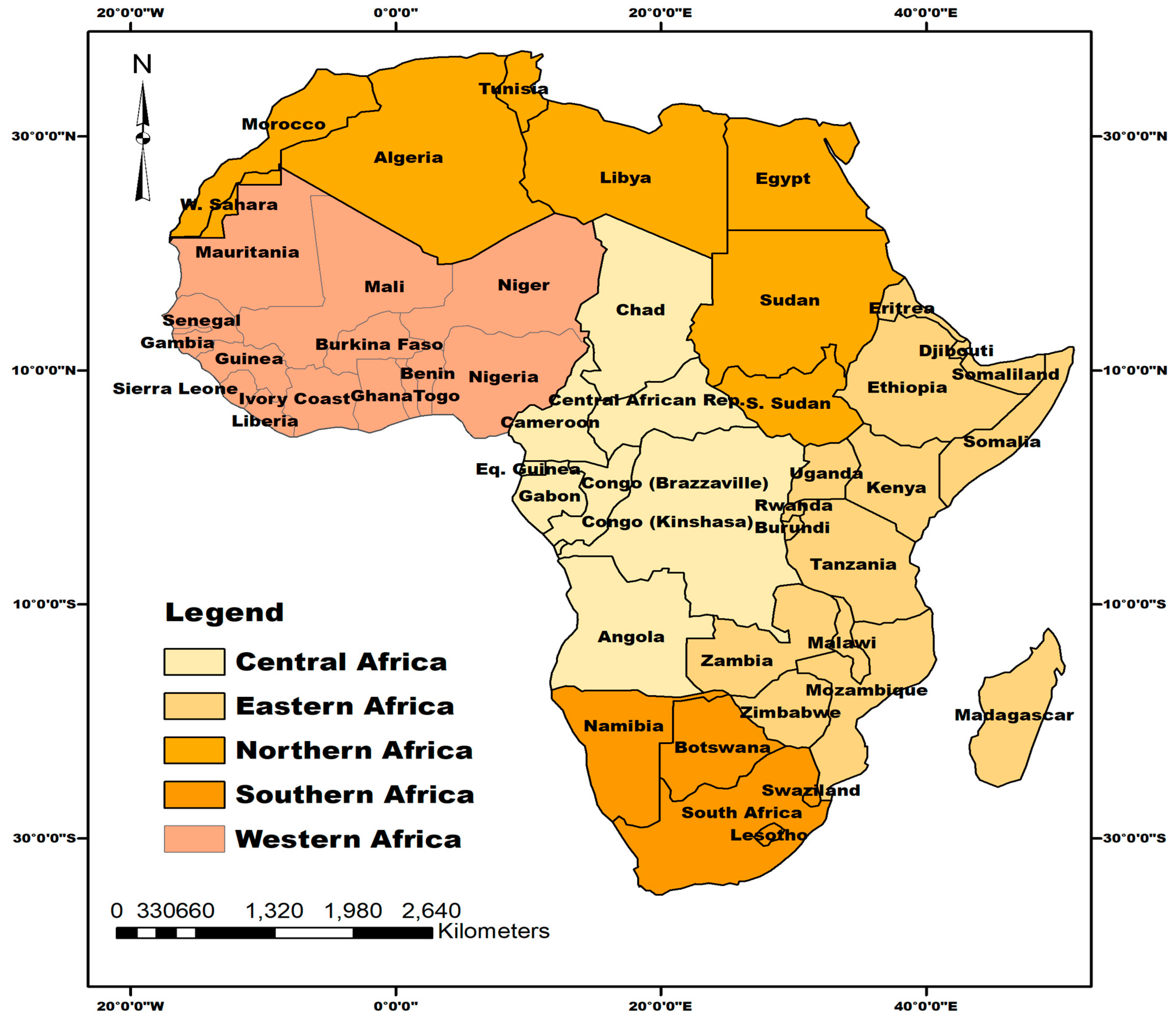
2.1. The Study Area
2.2. Literature Search
2.3. Data Analyses
3. Results
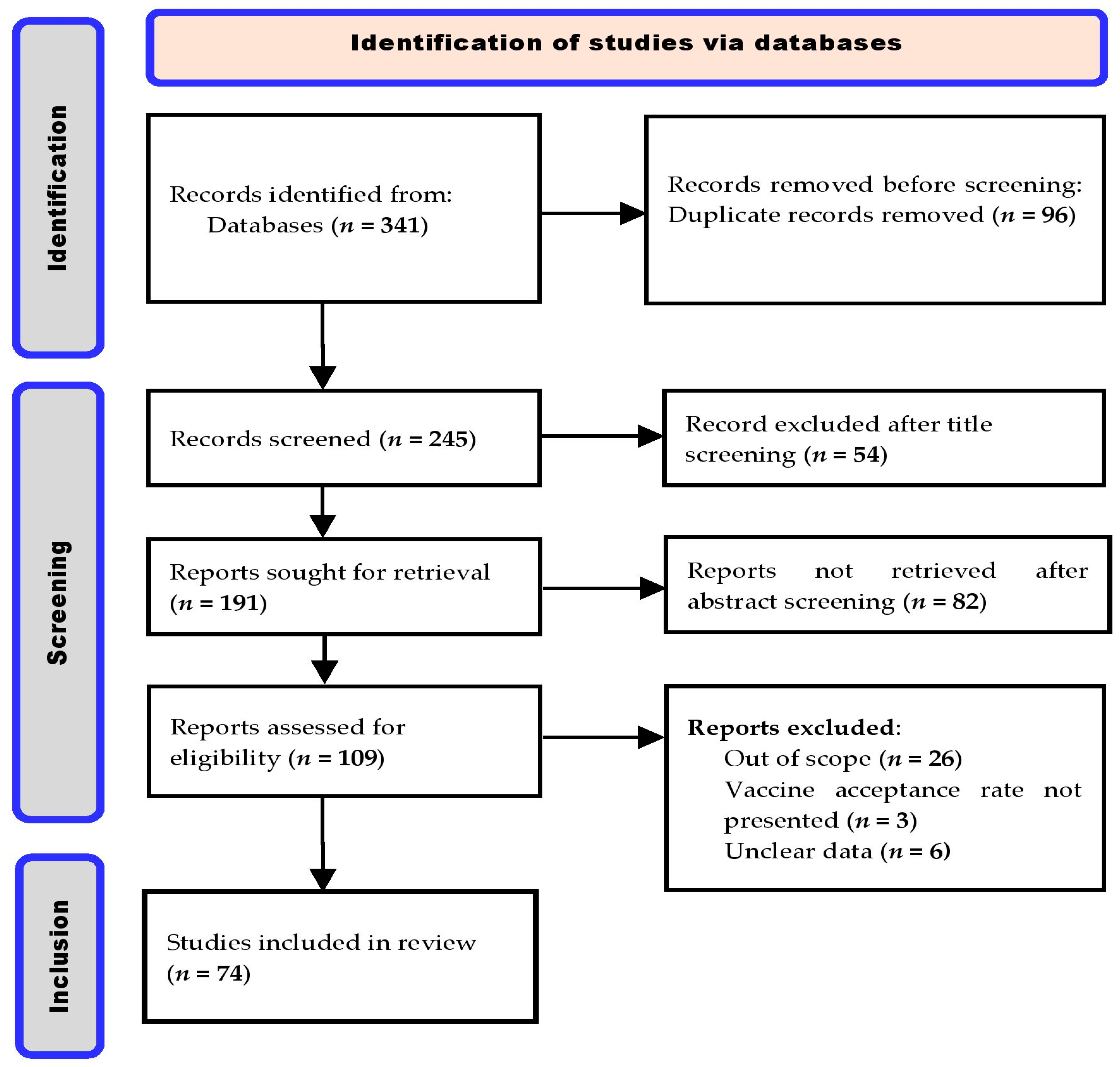
3.1. Literature Review
3.2. Characteristics of the Papers Included in This Review
3.3. Rates of COVID-19 Vaccine Acceptance Found in the Study
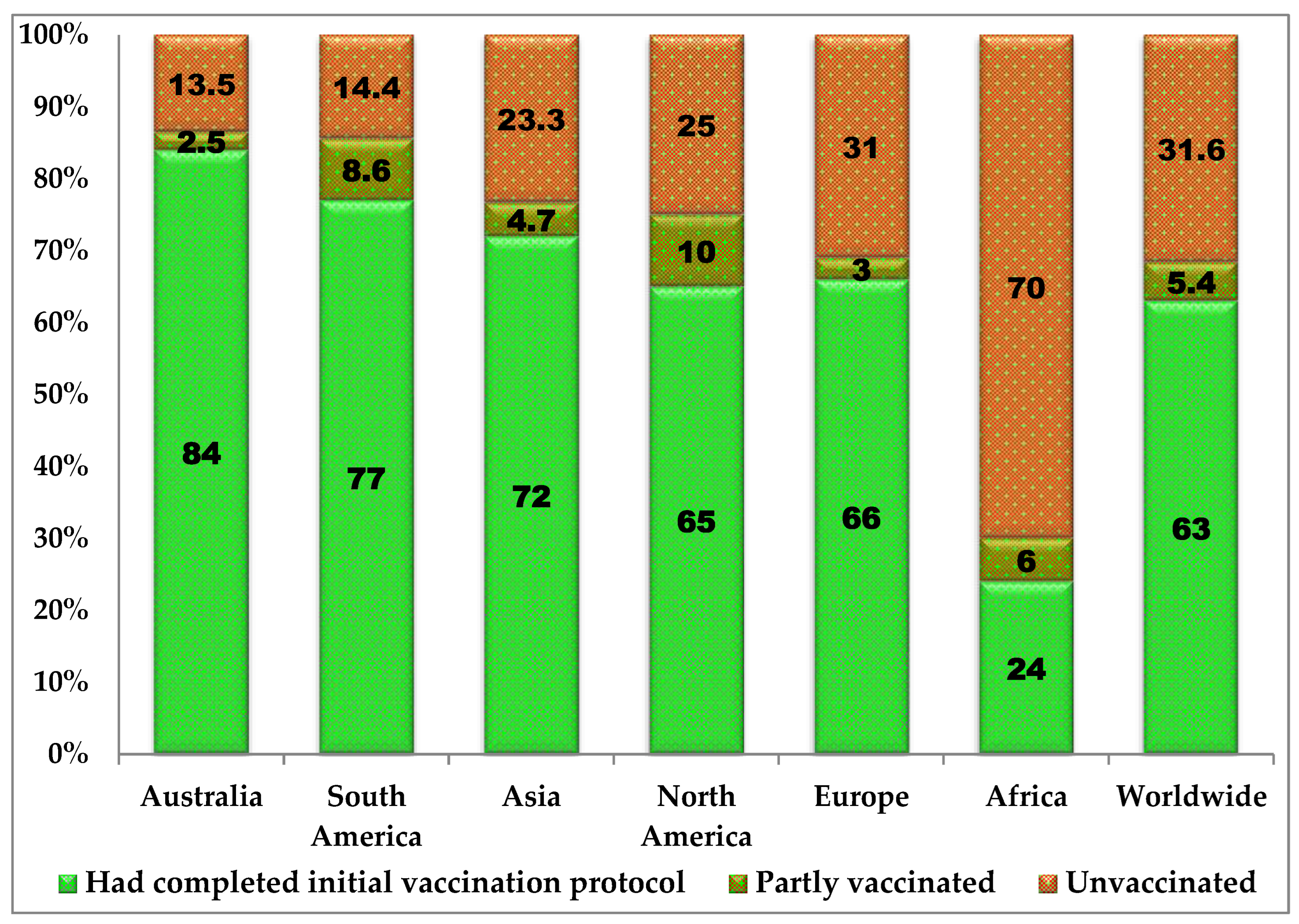
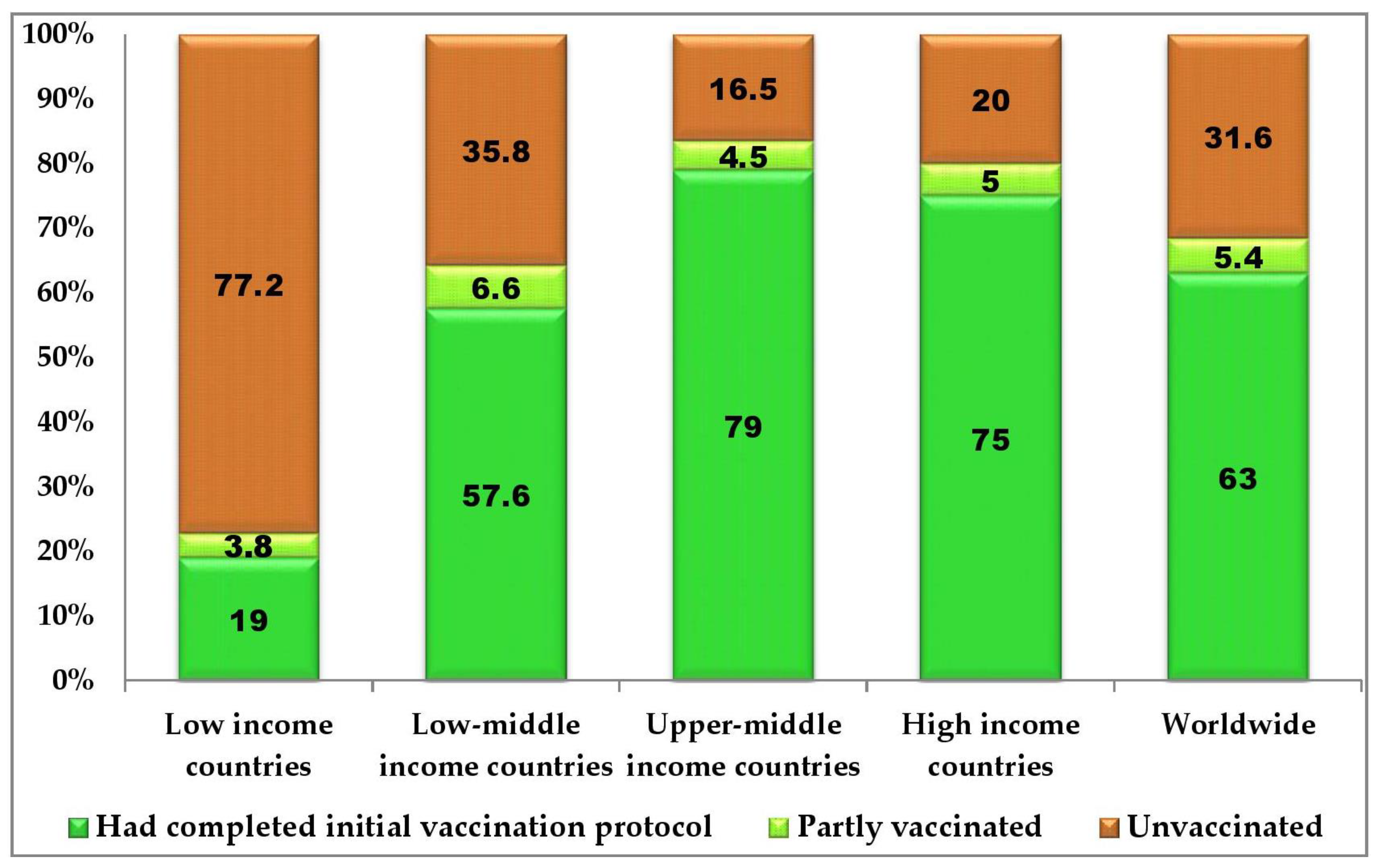
3.4. COVID-19 Infections and Vaccination Rates Extracted from Databases
3.5. Reported Cause of Vaccine Hesitancy in Africa and Ways-Out
4. Discussion
4.1. Causes of COVID-19 Vaccine Hesitance in Africa
4.2. Global Public Health Implication of Africa’s Low COVID-19 Vaccination Rate
4.3. The Ways-Out
5. Conclusions
Limitations of the Study
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 20 September 2022).
- Greenwood, B. The contribution of vaccination to global health: Past, present and future. Philos. Trans. R Soc. Lond. B Biol. Sci. 2014, 369, 20130433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacDonald, N.E.; SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Frenkel, L.D. The global burden of vaccine-preventable infectious diseases in children less than 5 years of age: Implications for COVID-19 vaccination. How can we do better? Allergy Asthma Proc. 2021, 42, 378–385. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/?gclid=Cj0KCQjwguGYBhDRARIsAHgRm48kaolQwV9KOQwpZfstu2LBuD9CUxnOEZvXrPaXXhE1vC5gK0gv4fUaAnjpEALw_wcB (accessed on 25 October 2022).
- Hasan, M.N.; Haider, N.; Stigler, F.L.; Khan, R.A.; McCoy, D.; Zumla, A.; Kock, R.A.; Uddin, M.J. The Global Case-Fatality Rate of COVID-19 Has Been Declining Since May 2020. Am. J. Trop. Med. Hyg. 2021, 104, 2176–2184. [Google Scholar] [CrossRef]
- Talic, S.; Shah, S.; Wild, H.; Gasevic, D.; Maharaj, A.; Ademi, Z.; Li, X.; Xu, W.; Mesa-Eguiagaray, I.; Rostron, J.; et al. Effectiveness of public health measures in reducing the incidence of COVID-19, SARS-CoV-2 transmission, and COVID-19 mortality: Systematic review and meta-analysis. BMJ 2021, 375, e068302. [Google Scholar] [CrossRef]
- Ogunleye, O.O.; Basu, D.; Mueller, D. Response to the Novel Corona Virus (COVID-19) Pandemic Across Africa: Successes, Challenges, and Implications for the Future. Front. Pharmacol. 2020, 11, 1205. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Tracking SARS-CoV-2 Variants. Available online: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/ (accessed on 10 September 2022).
- Barton, M.I.; MacGowan, S.A.; Kutuzov, M.A.; Dushek, O.; Barton, G.J.; van der Merwe, P.A. Effects of common mutations in the SARS-CoV-2 Spike RBD and its ligand, the human ACE2 receptor on binding affinity and kinetics. eLife 2021, 10, e70658. [Google Scholar] [CrossRef]
- Torbati, E.; Krause, K.L.; Ussher, J.E. The Immune Response to SARS-CoV-2 and Variants of Concern. Viruses 2021, 13, 1911. [Google Scholar] [CrossRef]
- World Health Organisation (WHO). The Vaccines Success Story Gives Us Hope for the Future. Available online: https://www.who.int/news-room/feature-stories/detail/the-vaccines-success-story-gives-us-hope-for-the-future (accessed on 10 September 2022).
- Mas-Bermejo, P.I.; Dickinson-Meneses, F.O.; Almenares-Rodríguez, K.; Sanchez-Valdes, L.; Guinovart-Díaz, R.; Vidal-Ledo, M.; Galban-García, E.; Olivera-Nodarse, Y.; Morgado-Vega, I.; Duenas-Carrera, S.; et al. Cuban Abdala vaccine: Effectiveness in preventing severe disease and death from COVID-19 in Havana, Cuba; A cohort study. Lancet Reg. Health Am. 2022, 16, 100366. [Google Scholar]
- Lytras, T.; Kontopidou, F.; Lambrou, A.; Tsiodras, S. Comparative effectiveness and durability of COVID-19vaccination against death and severe disease in an on-going nationwide mass vaccination campaign. J. Med. Virol. 2022, 94, 5044–5050. [Google Scholar] [CrossRef]
- Mohammed, I.; Nauman, A.; Paul, P.; Ganesan, S.; Chen, K.H.; Jalil, S.; Jaouni, S.H.; Kawas, H.; Khan, W.A.; Vattoth, A.L.; et al. The efficacy and effectiveness of the COVID-19 vaccines in reducing infection, severity, hospitalization, and mortality: A systematic review. Hum. Vaccines Immunother. 2022, 18, 1. [Google Scholar] [CrossRef] [PubMed]
- Mathieu, E.; Ritchie, H.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Hasell, J.; Macdonald, B.; Dattani, S.; Beltekian, D.; Ortiz-Ospina, E.; et al. Coronavirus Pandemic (COVID-19). Available online: https://ourworldindata.org/coronavirus (accessed on 25 September 2022).
- Cooper, S.; Betsch, C.; Sambala, E.Z.; Mchiza, N.; Wiysonge, C.S. Vaccine hesitancy—A potential threat to the achievements of vaccination programmes in Africa. Hum. Vaccin. Immunother. 2018, 14, 2355–2357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aborode, A.T.; Fajemisin, E.A.; Ekwebelem, O.C.; Tsagkaris, C.; Taiwo, E.A.; Uwishema, O.; Awoniyi, O.O.; Ahmad, S.; Essar, M.Y.; Adanur, I.; et al. Vaccine hesitancy in Africa: Causes and strategies to the rescue. Ther. Adv. Vaccines Immunother. 2021, 9, 25151355211047514. [Google Scholar] [CrossRef] [PubMed]
- Lawal, L.; Aminu Bello, M.; Murwira, T.; Avoka, C.; Yusuf Ma′aruf, S.; Harrison Omonhinmin, I.; Maluleke, P.; Tsagkaris, C.; Onyeaka, H. Low coverage of COVID-19 vaccines in Africa: Current evidence and the way forward. Hum. Vaccin. Immunother. 2022, 18, 2034457. [Google Scholar] [CrossRef]
- World Atlas. African Region. Available online: https://www.worldatlas.com/geography/regions-of-africa.html (accessed on 23 September 2022).
- Worldometer. COVID-19 Coronavirus Pandemic. Available online: https://www.worldometers.info/coronavirus/ (accessed on 25 September 2022).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Wang, M.W.; Wen, W.; Wang, N.; Zhou, M.Y.; Wang, C.Y.; Ni, J.; Jiang, J.J.; Zhang, X.W.; Feng, Z.H.; Cheng, Y.R. COVID-19 Vaccination Acceptance Among Healthcare Workers and Non-healthcare Workers in China: A Survey. Front. Public Health 2021, 9, 709056. [Google Scholar] [CrossRef]
- Ackah, M.; Ameyaw, L.; Gazali, S.M.; Afi-Asubonteng, D.P.; Osei Yeboah, C.; Narkotey Annor, E.; Abena Kwartemaa Ankapong, E.; Boakye, H. COVID-19 vaccine acceptance among health care workers in Africa: A systematic review and meta-analysis. PLoS ONE 2022, 17, e0268711. [Google Scholar] [CrossRef]
- Reuben, R.C.; Danladi, M.M.A.; Saleh, D.A.; Ejembi, P.E. Knowledge, Attitudes and Practices towards COVID-19: An Epidemiological Survey in North-Central Nigeria. J. Community Health 2021, 46, 457. [Google Scholar] [CrossRef]
- Aemro, A.; Amare, N.S.; Shetie, B.; Chekol, B.; Wassie, M. Determinants of COVID-19 Vaccine Hesitancy among Health Care Workers in Amhara Region Referral Hospitals, Northwest Ethiopia: A Cross-Sectional Study. Epidemiol. Infect. 2021, 149, E225. [Google Scholar] [CrossRef]
- Ahmed, M.A.M.; Colebunders, R.; Gele, A.A.; Farah, A.A.; Osman, S.; Guled, I.A.; Abdullahi, A.A.M.; Hussein, A.M.; Ali, A.M.; Siewe Fodjo, J.N. COVID-19 Vaccine Acceptability and Adherence to Preventive Measures in Somalia: Results of an Online Survey. Vaccines 2021, 9, 543. [Google Scholar] [CrossRef]
- Angelo, A.T.; Alemayehu, D.S.; Dachew, A.M. Health Care Workers Intention to Accept COVID-19 Vaccine and Associated Factors in Southwestern Ethiopia, 2021. PLoS ONE 2021, 16, e0257109. [Google Scholar] [CrossRef] [PubMed]
- Kanyanda, S.; Markhof, Y.; Wollburg, P.; Zezza, A. Acceptance of COVID-19 Vaccines in Sub-Saharan Africa: Evidence from Six National Phone Surveys. BMJ Open 2021, 11, e055159. [Google Scholar] [CrossRef]
- Mohammed, R.; Nguse, T.M.; Habte, B.M.; Fentie, A.M.; Gebretekle, G.B. COVID-19 Vaccine Hesitancy among Ethiopian Healthcare Workers. PLoS ONE 2021, 16, e0261125. [Google Scholar] [CrossRef] [PubMed]
- Elgendy, M.O.; Abdelrahim, M.E.A. Public Awareness about Coronavirus Vaccine, Vaccine Acceptance, and Hesitancy. J. Med. Virol. 2021, 93, 6535–6543. [Google Scholar] [CrossRef] [PubMed]
- El-Sokkary, R.H.; El Seifi, O.S.; Hassan, H.M.; Mortada, E.M.; Hashem, M.K.; Gadelrab, M.R.M.A.; Tash, R.M.E. Predictors of COVID-19 Vaccine Hesitancy among Egyptian Healthcare Workers: A Cross-Sectional Study. BMC Infect. Dis. 2021, 21, 762. [Google Scholar] [CrossRef]
- Fares, S.; Elmnyer, M.M.; Mohamed, S.S.; Elsayed, R. COVID-19 Vaccination Perception and Attitude among Healthcare Workers in Egypt. J. Prim. Care Community Health 2021, 12. [Google Scholar] [CrossRef]
- El-Kefi, H.; Kefi, K.; Krir, M.W.; Brahim, C.B.; Baatout, A.; Bouzouita, I.; Ben Azaiz, M.; Bouguerra, C.; Khoufi, M.T.; Gharsallah, H.; et al. Acceptability of COVID-19 Vaccine: A Cross-Sectional Study in a Tunisian General Hospital. Pan Afr. Med. J. 2021, 39, 245. [Google Scholar] [CrossRef]
- Khalis, M.; Boucham, M.; Luo, A.; Marfak, A.; Saad, S.; Aboubacar, C.M.; El Haj, S.A.; Jallal, M.; Aazi, F.Z.; Charaka, H.; et al. COVID-19 Vaccination Acceptance among Health Science Students in Morocco: A Cross-Sectional Study. Vaccines 2021, 9, 1451. [Google Scholar] [CrossRef]
- Khalis, M.; Hatim, A.; Elmouden, L.; Diakite, M.; Marfak, A.; Ait El Haj, S.; Farah, R.; Jidar, M.; Conde, K.K.; Hassouni, K.; et al. Acceptability of COVID-19 vaccination among health care workers: A cross-sectional survey in Morocco. Hum. Vaccin. Immunother. 2021, 17, 5076–5081. [Google Scholar] [CrossRef]
- Omar, D.I.; Hani, B.M. Attitudes and Intentions towards COVID-19 Vaccines and Associated Factors among Egyptian Adults. J. Infect. Public Health 2021, 14, 1481–1488. [Google Scholar] [CrossRef]
- Saied, S.M.; Saied, E.M.; Kabbash, I.A.; Abdo, S.A.E.F. Vaccine Hesitancy: Beliefs and Barriers Associated with COVID-19 Vaccination among Egyptian Medical Students. J. Med. Virol. 2021, 93, 4280–4291. [Google Scholar] [CrossRef] [PubMed]
- Adeniyi, O.V.; Stead, D.; Singata-Madliki, M.; Batting, J.; Wright, M.; Jelliman, E.; Abrahams, S.; Parrish, A. Acceptance of COVID-19 Vaccine among the Healthcare Workers in the Eastern Cape, South Africa: A Cross Sectional Study. Vaccines 2021, 9, 666. [Google Scholar] [CrossRef] [PubMed]
- Kollamparambil, U.; Oyenubi, A.; Nwosu, C. COVID19 Vaccine Intentions in South Africa: Health Communication Strategy to Address Vaccine Hesitancy. BMC Public Health 2021, 21, 2113. [Google Scholar] [CrossRef] [PubMed]
- McAbee, L.; Tapera, O.; Kanyangarara, M. Factors Associated with COVID-19 Vaccine Intentions in Eastern Zimbabwe: A Cross-Sectional Study. Vaccines 2021, 9, 1109. [Google Scholar] [CrossRef]
- Oduwole, E.O.; Esterhuizen, T.M.; Mahomed, H.; Wiysonge, C.S. Estimating Vaccine Confidence Levels among Healthcare Staff and Students of a Tertiary Institution in South Africa. Vaccines 2021, 9, 1246. [Google Scholar] [CrossRef]
- Carpio, C.E.; Sarasty, O.; Hudson, D.; Macharia, A.; Shibia, M. The Demand for a COVID-19 Vaccine in Kenya. Hum. Vaccin. Immunother. 2021, 17, 3463–3471. [Google Scholar] [CrossRef]
- Echoru, I.; Ajambo, P.D.; Keirania, E.; Bukenya, E.E.M. Sociodemographic Factors Associated with Acceptance of COVID-19 Vaccine and Clinical Trials in Uganda: A Cross-Sectional Study in Western Uganda. BMC Public Health 2021, 21, 1–8. [Google Scholar] [CrossRef]
- Isah, A.; Ubaka, C.M. Pharmacists’ Readiness to Receive, Recommend and Administer COVID-19 Vaccines in an African Country: An Online Multiple-Practice Settings Survey in Nigeria. Malawi Med. J. 2021, 33, 210–220. [Google Scholar] [CrossRef]
- Acheampong, T.; Akorsikumah, E.A.; Osae-Kwapong, J.; Khalid, M.; Appiah, A.; Amuasi, J.H. Examining Vaccine Hesitancy in Sub-Saharan Africa: A Survey of the Knowledge and Attitudes among Adults to Receive COVID-19 Vaccines in Ghana. Vaccines 2021, 9, 814. [Google Scholar] [CrossRef]
- Adebisi, Y.A.; Alaran, A.J.; Bolarinwa, O.A.; Akande-Sholabi, W.; Lucero-Prisno, D.E. When It Is Available, Will We Take It? Social Media Users’ Perception of Hypothetical COVID-19 Vaccine in Nigeria. Pan Afr. Med. J. 2021, 38, 230. [Google Scholar] [CrossRef]
- Alhassan, R.K.; Owusu-Agyei, S.; Ansah, E.K.; Gyapong, M. COVID-19 Vaccine Uptake among Health Care Workers in Ghana: A Case for Targeted Vaccine Deployment Campaigns in the Global South. Hum. Resour. Health 2021, 19, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Amuzie, C.I.; Odini, F.; Kalu, K.U.; Izuka, M.; Nwamoh, U.; Emma-Ukaegbu, U.; Onyike, G. COVID-19 Vaccine Hesitancy among Healthcare Workers and Its Socio-Demographic Determinants in Abia State, Southeastern Nigeria: A Cross-Sectional Study. Pan Afr. Med. J. 2021, 40, 10. [Google Scholar] [CrossRef] [PubMed]
- Habib, M.A.; Dayyab, F.M.; Iliyasu, G.; Habib, A.G. Knowledge, Attitude and Practice Survey of COVID-19 Pandemic in Northern Nigeria. PLoS ONE 2021, 16, e0245176. [Google Scholar] [CrossRef] [PubMed]
- Mustapha, M.; Lawal, B.K.; Sha’aban, A.; Jatau, A.I.; Wada, A.S.; Bala, A.A.; Mustapha, S.; Haruna, A.; Musa, A.; Ahmad, M.H.; et al. Factors Associated with Acceptance of COVID-19 Vaccine among University Health Sciences Students in Northwest Nigeria. PLoS ONE 2021, 16, e0260672. [Google Scholar] [CrossRef]
- Okafor, U.G.; Isah, A.; Onuh, J.C.; Mgbemena, C.B.; Ubaka, C.M. Community Acceptance and Willingness to Pay for Hypothetical COVID-19 Vaccines in a Developing Country: A Web-Based Nationwide Study in Nigeria. Pan Afr. Med. J. 2021, 40, 112. [Google Scholar] [CrossRef]
- Uzochukwu, I.C.; Eleje, G.U.; Nwankwo, C.H.; Chukwuma, G.O.; Uzuke, C.A.; Uzochukwu, C.E.; Mathias, B.A.; Okunna, C.S.; Asomugha, L.A.; Esimone, C.O. COVID-19 Vaccine Hesitancy among Staff and Students in a Nigerian Tertiary Educational Institution. Ther. Adv. Infect. Dis. 2021, 8. [Google Scholar] [CrossRef]
- Yeboah, P.; Daliri, D.B.; Abdin, A.Y.; Appiah-Brempong, E.; Pitsch, W.; Panyin, A.B.; Adusei, E.B.A.; Razouk, A.; Nasim, M.J.; Jacob, C. Knowledge into the Practice against COVID-19: A Cross-Sectional Study from Ghana. Int. J. Environ. Res. Public Health 2021, 18, 12902. [Google Scholar] [CrossRef]
- Carcelen, A.C.; Prosperi, C.; Mutembo, S.; Chongwe, G.; Mwansa, F.D.; Ndubani, P.; Simulundu, E.; Chilumba, I.; Musukwa, G.; Thuma, P.; et al. COVID-19 Vaccine Hesitancy in Zambia: A Glimpse at the Possible Challenges ahead for COVID-19 Vaccination Rollout in Sub-Saharan Africa. Hum. Vaccines Immunother. 2022, 18, 1–6. [Google Scholar] [CrossRef]
- Wiysonge, C.S.; Alobwede, S.M.; de Marie, C.; Katoto, P.; Kidzeru, E.B.; Lumngwena, E.N.; Cooper, S.; Goliath, R.; Jackson, A.; Shey, M.S. COVID-19 Vaccine Acceptance and Hesitancy among Healthcare Workers in South Africa. Expert Rev. Vaccines 2022, 21, 549–559. [Google Scholar] [CrossRef]
- Botwe, B.O.; Antwi, W.K.; Adusei, J.A.; Mayeden, R.N.; Akudjedu, T.N.; Sule, S.D. COVID-19 Vaccine Hesitancy Concerns: Findings from a Ghana Clinical Radiography Workforce Survey. Radiography 2022, 28, 537–544. [Google Scholar] [CrossRef]
- Ajonina-Ekoti, I.U.; Ware, K.B.; Nfor, C.K.; Akomoneh, E.A.; Djam, A.; Chia-Garba, M.; Wepnyu, G.N.; Awambeng, D.; Abendong, K.; Manjong, F.T.; et al. COVID-19 Perceptions and Vaccine Hesitancy: Acceptance, Attitude, and Barriers among Cameroonians. J. Am. Pharm. Assoc. 2022, 62, 1823–1829. [Google Scholar] [CrossRef] [PubMed]
- Abay, E.S.; Belew, M.D.; Ketsela, B.S.; Mengistu, E.E.; Getachew, L.S.; Teferi, Y.A.; Zerihun, A.B. Assessment of Attitude towards COVID-19 Vaccine and Associated Factors among Clinical Practitioners in Ethiopia: A Cross-Sectional Study. PLoS ONE 2022, 17, e0269923. [Google Scholar] [CrossRef] [PubMed]
- Adane, M.; Ademas, A.; Kloos, H. Knowledge, Attitudes, and Perceptions of COVID-19 Vaccine and Refusal to Receive COVID-19 Vaccine among Healthcare Workers in Northeastern Ethiopia. BMC Public Health 2022, 22, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Aynalem, B.Y.; Melesse, M.; Zeleke, L. COVID-19 Vaccine Acceptability and Determinants among Pregnant Mothers Attending Antenatal Care Services at Debre Markos Town Public Health Institutions, Debre Markos Northwest Ethiopia: Mixed Study. Pan Afr. Med. J. 2022, 41, 293. [Google Scholar] [CrossRef]
- Berhe, E.T.; Shama, A.T.; Ahmed, M.M.; Gesesew, H.A.; Ward, P.R.; Gebremeskel, T.G. Assessment of COVID-19 Vaccination Refusal among Healthcare Workers in Ethiopia. Front. Public Health 2022, 10, 2533. [Google Scholar] [CrossRef]
- Boche, B.; Kebede, O.; Damessa, M.; Gudeta, T.; Wakjira, D. Health Professionals’ COVID-19 Vaccine Acceptance and Associated Factors in Tertiary Hospitals of South-West Ethiopia: A Multi-Center Cross-Sectional Study. Inquiry 2022, 59. [Google Scholar] [CrossRef]
- Dereje, N.; Tesfaye, A.; Tamene, B.; Alemeshet, D.; Abe, H.; Tesfa, N.; Gedion, S.; Biruk, T.; Lakew, Y. COVID-19 Vaccine Hesitancy in Addis Ababa, Ethiopia: A Mixed-Method Study. BMJ Open 2022, 12, e052432. [Google Scholar] [CrossRef]
- Mose, A.; Haile, K.; Timerga, A. COVID-19 Vaccine Hesitancy among Medical and Health Science Students Attending Wolkite University in Ethiopia. PLoS ONE 2022, 17, e0263081. [Google Scholar] [CrossRef]
- Strupat, C.; Shigute, Z.; Bedi, A.S.; Rieger, M. Willingness to Take COVID-19 Vaccination in Low-Income Countries: Evidence from Ethiopia. PLoS ONE 2022, 17, e0264633. [Google Scholar] [CrossRef]
- Tolossa, T.; Fetensa, G.; Ayala, D.; Wakuma, B. Health Professionals’ COVID-19 Vaccine Acceptance and Associated Factors in Wollega University Referral Hospital, Western Ethiopia: A Cross-Sectional Study. Hum. Vaccin. Immunother. 2022, 18, 2069960. [Google Scholar] [CrossRef]
- Yilma, D.; Mohammed, R.; Abdela, S.G.; Enbiale, W.; Seifu, F.; Pareyn, M.; Liesenborghs, L.; van Griensven, J.; van Henten, S. COVID-19 Vaccine Acceptability among Healthcare Workers in Ethiopia: Do We Practice What We Preach? Trop. Med. Int. Health 2022, 27, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Raja, S.M.; Osman, M.E.; Musa, A.O.; Hussien, A.A.; Yusuf, K. COVID-19 Vaccine Acceptance, Hesitancy, and Associated Factors among Medical Students in Sudan. PLoS ONE 2022, 17, e0266670. [Google Scholar] [CrossRef]
- Salem, G.M.; Said, R.M.; Abdelsalam, A.E. Acceptance Rate of COVID-19 Vaccination and Its Predictors in Egypt: An Online Survey. J. Infect. Dev. Ctries. 2022, 16, 993–1000. [Google Scholar] [CrossRef] [PubMed]
- Yassin, E.O.M.; Faroug, H.A.A.; Ishaq, Z.B.Y.; Mustafa, M.; Idris, M.; Widatallah, S.; Abd El-Raheem, G.; Suliman, M.Y. COVID-19 Vaccination Acceptance among Healthcare Staff in Sudan, 2021. J. Immunol. Res. 2022, 2022, 3392667. [Google Scholar] [CrossRef] [PubMed]
- Zammit, N.; El Gueder, A.; Brahem, A.; Ayouni, I.; Ghammam, R.; Fredj, S.B.; Sridi, C.; Chouchene, A.; Kalboussi, H.; Maalel, O.E.; et al. Studying SARS-CoV-2 Vaccine Hesitancy among Health Professionals in Tunisia. BMC Health Serv. Res. 2022, 22, 1–14. [Google Scholar] [CrossRef]
- Engelbrecht, M.; Heunis, C.; Kigozi, G. COVID-19 Vaccine Hesitancy in South Africa: Lessons for Future Pandemics. Int. J. Environ. Res. Public Health 2022, 19, 6694. [Google Scholar] [CrossRef]
- Govere-Hwenje, S.; Jarolimova, J.; Yan, J.; Khumalo, A.; Zondi, G.; Ngcobo, M.; Wara, N.J.; Zionts, D.; Bogart, L.M.; Parker, R.A.; et al. Willingness to Accept COVID-19 Vaccination among People Living with HIV in a High HIV Prevalence Community. BMC Public Health 2022, 22, 1–11. [Google Scholar] [CrossRef]
- Kahn, K.; Pettifor, A.; Mataboge, P.; Kelly, N.K.; Kelly, N.K.; Mashinini, D.P.; Nair, H.; Campbell, H.; Cohen, C.; Gómez-Olivé, F.X.; et al. COVID-19 Vaccine Hesitancy in Rural South Africa: Deepening Understanding to Increase Uptake and Access. J. Glob. Health 2022, 12, 1–7. [Google Scholar] [CrossRef]
- Modi, B.H.; Pretorius, D.; Francis, J.M. A Study on Willingness to Take the COVID-19 Vaccine at a Tertiary Institution Community in Johannesburg, South Africa. Afr. J. Prim. Health Care Fam. Med. 2022, 14. [Google Scholar] [CrossRef]
- Moucheraud, C.; Phiri, K.; Whitehead, H.S.; Songo, J.; Lungu, E.; Chikuse, E.; Phiri, S.; van Oosterhout, J.J.; Hoffman, R.M. Uptake of the COVID-19 Vaccine among Healthcare Workers in Malawi. Int. Health 2022, ihac007. [Google Scholar] [CrossRef]
- Mudenda, S.; Hikaambo, C.N.; Daka, V.; Chileshe, M.; Mfune, R.L.; Kampamba, M.; Kasanga, M.; Phiri, M.; Mufwambi, W.; Banda, M.; et al. Prevalence and Factors Associated with COVID-19 Vaccine Acceptance in Zambia: A Web-Based Cross-Sectional Study. Pan Afr. Med. J. 2022, 41, 112. [Google Scholar] [CrossRef] [PubMed]
- Mundagowa, P.T.; Tozivepi, S.N.; Chiyaka, E.T.; Mukora-Mutseyekwa, F.; Makurumidze, R. Assessment of COVID-19 Vaccine Hesitancy among Zimbabweans: A Rapid National Survey. PLoS ONE 2022, 17, e0266724. [Google Scholar] [CrossRef] [PubMed]
- Katoto, P.D.M.C.; Parker, S.; Coulson, N.; Pillay, N.; Cooper, S.; Jaca, A.; Mavundza, E.; Houston, G.; Groenewald, C.; Essack, Z.; et al. Predictors of COVID-19 Vaccine Hesitancy in South African Local Communities: The VaxScenes Study. Vaccines 2022, 10, 353. [Google Scholar] [CrossRef]
- Burger, R.; Köhler, T.; Golos, A.M.; Buttenheim, A.M.; English, R.; Tameris, M.; Maughan-Brown, B. Longitudinal Changes in COVID-19 Vaccination Intent among South African Adults: Evidence from the NIDS-CRAM Panel Survey, February to May 2021. BMC Public Health 2022, 22, 1–10. [Google Scholar] [CrossRef]
- Tlale, L.B.; Gabaitiri, L.; Totolo, L.K.; Smith, G.; Puswane-Katse, O.; Ramonna, E.; Mothowaeng, B.; Tlhakanelo, J.; Masupe, T.; Rankgoane-Pono, G.; et al. Acceptance Rate and Risk Perception towards the COVID-19 Vaccine in Botswana. PLoS ONE 2022, 17, e0263375. [Google Scholar] [CrossRef] [PubMed]
- Chilongola, J.O.; Rwegoshola, K.M.; Balingumu, O.H.; Semvua, H.S.; Kwigizile, E.T. COVID-19 Knowledge, Attitudes, Practices, and Vaccination Hesitancy in Moshi, Kilimanjaro Region, Northern Tanzania. Tanzan. J. Health Res. 2022, 23, 1–12. [Google Scholar] [CrossRef]
- Osur, J.O.; Chengo, R.; Muinga, E.; Kemboi, J.; Sidibe, M.; Rarieya, M. Determinants of COVID-19 Vaccine Behaviour Intentions among the Youth in Kenya: A Cross-Sectional Study. Arch. Public Heal. 2022, 80, 1–13. [Google Scholar] [CrossRef]
- Adedeji-Adenola, H.; Olugbake, O.A.; Adeosun, S.A. Factors Influencing COVID-19 Vaccine Uptake among Adults in Nigeria. PLoS ONE 2022, 17, e0264371. [Google Scholar] [CrossRef]
- Al-Mustapha, A.I.; Okechukwu, O.; Olayinka, A.; Muhammed, O.R.; Oyewo, M.; Owoicho, S.A.; Abubakar, A.T.; Olabisi, A.; Jibril, A.; Ereh, S.; et al. A National Survey of COVID-19 Vaccine Acceptance in Nigeria. Vaccine 2022, 40, 4726–4731. [Google Scholar] [CrossRef]
- Ba, M.F.; Faye, A.; Kane, B.; Diallo, A.I.; Junot, A.; Gaye, I.; Bonnet, E.; Ridde, V. Factors associated with COVID-19 vaccine hesitancy in Senegal: A mixed study. Hum. Vaccines Immunother. 2022, 18, 2060020. [Google Scholar] [CrossRef]
- Ekowo, O.E.; Manafa, C.; Isielu, R.C.; Okoli, C.M.; Chikodi, I.; Onwuasoanya, A.F.; Echendu, S.T.; Ihedoro, I.; Nwabueze, U.D.; Nwoke, O.C. A Cross-Sectional Regional Study Looking at the Factors Responsible for the Low COVID-19 Vaccination Rate in Nigeria. Pan Afr. Med. J. 2022, 41, 114. [Google Scholar] [CrossRef] [PubMed]
- Ajibola, I.; Samuel, O.A.; Oluseyi, I.K.; Femi, A.A. Acceptance of COVID-19 Vaccine among Adults in Two Urban Local Government Areas of Kwara State, North Central Nigeria. Rwanda J. Med. Health Sci. 2022, 5, 127–140. [Google Scholar] [CrossRef]
- Kyei-Arthur, F.; Kyei-Gyamfi, S.; Agyekum, M.W.; Afrifa-Anane, G.F.; Amoh, B.A. Parents’ and guardians’ acceptability of COVID-19 vaccination for children in Ghana: An online survey. PLoS ONE 2022, 17, e0272801. [Google Scholar] [CrossRef] [PubMed]
- Njoga, E.O.; Mshelbwala, P.P.; Abah, K.O.; Awoyomi, O.J.; Wangdi, K.; Pewan, S.B.; Oyeleye, F.A.; Galadima, H.B.; Alhassan, S.A.; Okoli, C.E.; et al. COVID-19 Vaccine Hesitancy and Determinants of Acceptance among Healthcare Workers, Academics and Tertiary Students in Nigeria. Vaccines 2022, 10, 626. [Google Scholar] [CrossRef] [PubMed]
- Nomhwange, T.; Wariri, O.; Nkereuwem, E.; Olanrewaju, S.; Nwosu, N.; Adamu, U.; Danjuma, E.; Onuaguluchi, N.; Enegela, J.; Nomhwange, E.; et al. COVID-19 Vaccine Hesitancy amongst Healthcare Workers: An Assessment of Its Magnitude and Determinants during the Initial Phase of National Vaccine Deployment in Nigeria. eClinicalMedicine 2022, 50, 101499. [Google Scholar] [CrossRef] [PubMed]
- Nri-Ezedi, C.; Okechukwu, C.; Ofiaeli, O.; Nwaneli, E.; Musa, S.; Kida, I.; Adetola, H.; Ulasi, T. Predictors of COVID-19 Vaccine Acceptance Among Nigerian Medical Doctors. Ann. Heal. Res. 2022, 8, 1–12. [Google Scholar] [CrossRef]
- Okai, G.A.; Abekah-Nkrumah, G. The Level and Determinants of COVID-19 Vaccine Acceptance in Ghana. PLoS ONE 2022, 17, e0270768. [Google Scholar] [CrossRef]
- Onuminya, D.S.; Onuminya, J.E. Acceptance of COVID-19 Vaccines among Health Care Workers in Lokoja, Nigeria. Niger. J. Med. 2022, 31, 339–342. [Google Scholar] [CrossRef]
- Osuagwu, U.L.; Langsi, R.; Ovenseri-Ogbomo, G.; Mashige, K.P.; Abu, E.K.; Envuladu, E.A.; Goson, P.C.; Ekpenyong, B.N.; Oloruntoba, R.; Miner, C.A.; et al. Analysis of Perception, Reasons, and Motivations for COVID-19 Vaccination in People with Diabetes across Sub-Saharan Africa: A Mixed-Method Approach. Int. J. Environ. Res. Public Health 2022, 19, 7875. [Google Scholar] [CrossRef]
- Adebowale, O.O.; Adenubi, O.T.; Adesokan, H.K.; Oloye, A.A.; Bankole, N.O.; Fadipe, O.E.; Ayo-Ajayi, P.O.; Akinloye, O.A. Sociodemographic Predictors Associated with COVID-19 Vaccine Acceptance among Veterinary Professionals in Nigeria. Sokoto J. Vet. Sci. 2022, 20, 134–140. [Google Scholar] [CrossRef]
- Soyannwo, T.; Osinubi, M.O.; Abdulsalam, A.; Ahmed, A.K.; Imhomopi, G.B.; Adebisi, O.I.; Ajadi, O.R.; Mohammed, S.N.; Erinso, M.A.; Alausa, K.O. A Comparative Study of COVID-19 Vaccine Acceptability and Its Determinants among Urban and Rural Community Residents in Ogun State. J. Community Med. Prim. Health Care 2022, 34, 128–151. [Google Scholar] [CrossRef]
- Razai, M.S.; Oakeshott, P.; Esmail, A.; Wiysonge, C.S.; Viswanath, K.; Mills, M.C. COVID-19 vaccine hesitancy: The five Cs to tackle behavioural and sociodemographic factors. J. R. Soc. Med. 2021, 114, 295–298. [Google Scholar] [CrossRef] [PubMed]
- Kabakama, S.; Konje, E.T.; Dinga, J.N.; Kishamawe, C.; Morhason-Bello, I.; Hayombe, P.; Adeyemi, O.; Chimuka, E.; Lumu, I.; Amuasi, J.; et al. Commentary on COVID-19 Vaccine Hesitancy in sub-Saharan Africa. Trop. Med. Infect. Dis. 2022, 7, 130. [Google Scholar] [CrossRef] [PubMed]
- Pelčić, G.; Karačić, S.; Mikirtichan, G.L. Religious exception for vaccination or religious excuses for avoiding vaccination. Croat. Med. J. 2016, 57, 516–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organisation (WHO). Joint Statement on Dose Donations of COVID-19 Vaccines to African Countries. Available online: https://www.who.int/news/item/29-11-2021-joint-statement-on-dose-donations-of-covid-19-vaccines-to-african-countries (accessed on 21 September 2022).
- Mlaba, K. Why Are African Countries Throwing Away COVID-19 Vaccines? Available online: https://www.globalcitizen.org/en/content/african-countries-throwing-away-covid-19-vaccines/ (accessed on 20 September 2022).
- Anonymous. Six African Nations Chosen for mRNA Vaccine Production. 2022. Available online: https://www.devex.com/news/6-african-nations-chosen-for-mrna-vaccine-production-102706 (accessed on 22 September 2022).
- Albrecht, D. Vaccination, politics and COVID-19 impacts. BMC Public Health 2022, 22, 96. [Google Scholar] [CrossRef] [PubMed]
- WHO. UNICEF and WHO Condemn Attacks on Health Workers in Nigeria. 2013. Available online: https://www.who.int/news/item/08-02-2013-unicef-and-who-condemn-attacks-on-health-workers-in-nigeria (accessed on 22 September 2022).
- Amo-Adjei, J.; Nurzhynska, A.; Essuman, R.; Lohiniva, A.L. Trust and willingness towards COVID-19 vaccine uptake: A mixed-method study in Ghana, 2021. Arch. Public Health 2022, 80, 64. [Google Scholar] [CrossRef] [PubMed]
- Aloysius-Michaels, O.; Enyiazu, C.; Nnamani, K.E. Campaign propaganda, electoral outcome and the dynamics of governance in the post-2015 presidential election in Nigeria. Cogent. Soc. Sci. 2021, 7, 1922180. [Google Scholar] [CrossRef]
- Jegede, A.S. What led to the Nigerian boycott of the polio vaccination campaign? PLoS Med. 2007, 4, e73. [Google Scholar] [CrossRef] [Green Version]
- Ghinai, I.; Willott, C.; Dadari, I.; Larson, H.J. Listening to the rumours: What the northern Nigeria polio vaccine boycott can tell us ten years on. Glob. Public Health 2013, 8, 1138–1150. [Google Scholar] [CrossRef] [Green Version]
- Islam, M.S.; Kamal, A.-H.M.; Kabir, A.; Southern, D.L.; Khan, S.H.; Hasan, S.; Sarkar, T.; Sharmin, S.; Das, S.; Roy, T.; et al. COVID-19 vaccine rumours and conspiracy theories: The need for cognitive inoculation against misinformation to improve vaccine adherence. PLoS ONE 2021, 16, e0251605. [Google Scholar] [CrossRef]
- Montagni, I.; Ouazzani-Touhami, K.; Mebarki, A.; Texier, N.; Schück, S.; Tzourio, C.; CONFINS group. Acceptance of a COVID-19 vaccine is associated with ability to detect fake news and health literacy. J. Public Health 2022, 43, 695–702. [Google Scholar] [CrossRef] [PubMed]
- Farzanegan, M.R.; Hofmann, H.P. Effect of public corruption on the COVID-19 immunization progress. Sci Rep. 2022, 11, 23423. [Google Scholar] [CrossRef] [PubMed]
- UNODC (United Nations Office of Drug and Crime). COVID-19 Vaccines and Corruption Risks: Preventing Corruption in the Manufacture, Allocation and Distribution of Vaccines. 2022. Available online: https://www.oecd.org/gov/ethics/Corruption-Public-Procurement-Brochure.pdf (accessed on 22 September 2022).
- Au, J. Higher vaccination rates predict reduction in SARS-CoV-2 transmission across the United States. Infection 2022, 50, 1255–1266. [Google Scholar] [CrossRef]
- Singanayagam, A.; Hakki, S.; Dunning, J.; Madon, K.J.; Crone, M.A.; Koycheva, A.; Derqui-Fernandez, N.; Barnett, J.L.; Whitfield, M.G.; Varro, R.; et al. Community transmission and viral load kinetics of the SARS-CoV-2 delta (B.1.617.2) variant in vaccinated and unvaccinated individuals in the UK: A prospective, longitudinal, cohort study. Lancet 2022, 22, 183–195. [Google Scholar] [CrossRef]
- Shahhosseini, N.; Wong, G.; Kobinger, G.P.; Chinikar, S. SARS-CoV-2 spillover transmission due to recombination event. Gene Rep. 2021, 23, 101045. [Google Scholar] [CrossRef]
- Wei, C.; Shan, K.J.; Wang, W.; Zhang, S.; Huan, Q.; Qian, W. Evidence for a mouse origin of the SARS-CoV-2 Omicron variant. J. Genet. Genomics 2021, 48, 1111–1121. [Google Scholar] [CrossRef]
- Zoccola, R.; Beltramo, C.; Magris, G.; Peletto, S.; Acutis, P.; Bozzetta, E.; Radovic, S.; Zappulla, F.; Porzio, A.M.; Gennero, M.S.; et al. First detection of an Italian human-to-cat outbreak of SARS-CoV-2 Alpha variant—Lineage B.1.1.7. One Health 2021, 13, 100295. [Google Scholar] [CrossRef]
- Li, X.; Liu, H.; Tong, Y. Concerns on the cross-species transmission of SARS-CoV-2 between pets and humans. Front. Mocrobiol. 2022, 13, 985528. [Google Scholar] [CrossRef]
- Parkhe, P.; Verma, S. Evolution, Interspecies Transmission, and Zoonotic Significance of Animal Coronaviruses. Front. Microbiol. 2021, 8, 719834. [Google Scholar] [CrossRef]
- Wilhelm, A.; Widera, M.; Grikscheit, K.; Toptan, T.; Schenk, B.; Pallas, C.; Metzler, M.; Kohmer, N.; Hoehl, S.; Marschalek, R.; et al. Limited neutralisation of the SARS-CoV-2 Omicron sub-variants BA.1 and BA.2 by convalescent and vaccine serum and monoclonal antibodies. eBioMedicine 2022, 82, 104–158. [Google Scholar] [CrossRef]
- Di-Lego, V.; Sánchez-Romero, M.; Prskawetz, A. The impact of COVID-19 vaccines on the Case Fatality Rate: The importance of monitoring breakthrough infections. Int. J. Infect. Dis. 2022, 119, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Annan, K. Africa Literacy Facts. Available online: https://www.africanlibraryproject.org/africa-literacy-facts/ (accessed on 25 September 2022).
- Roberts, H.A.; Clark, D.A.; Kalina, C.; Sherman, C.; Brislin, S.; Heitzeg, M.M.; Hicks, B.M. To vax or not to vax: Predictors of anti-vax attitudes and COVID-19 vaccine hesitancy prior to widespread vaccine availability. PLoS ONE 2022, 17, e0264019. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | Year of Publication | Target Population | Sample Size | * Acceptance Rate Reported (%) | Study/Reference |
|---|---|---|---|---|---|
| Nigeria | 2021 | Other population | 589 | 29 | Reuben et al. [25] |
| Ethiopia | 2021 | Healthcare workers | 418 | 54.1 | Aemro et al. [26] |
| Somalia | 2021 | Healthcare workers | 4543 | 76.8 | Ahmed et al. [27] |
| Ethiopia | 2021 | Healthcare workers | 405 | 48.4 | Angelo et al. [28] |
| Ethiopia | 2021 | Other population | 2654 | 97.9 | Kanyanda et al. [29] |
| Ethiopia | 2021 | Healthcare workers | 614 | 39.7 | Mohammed et al. [30] |
| Egypt | 2021 | Other population | 871 | 88 | Elgendy et al. [31] |
| Egypt | 2021 | Healthcare workers | 308 | 26 | El-sokkary et al. [32] |
| Egypt | 2021 | Healthcare workers | 385 | 21 | Fares et al. [33] |
| Tunisia | 2021 | Healthcare workers | 398 | 58 | El-Kefi et al. [34] |
| Morocco | 2021 | Other population | 1272 | 26.9 | Khalis et al. [35] |
| Morocco | 2021 | Healthcare workers | 303 | 62 | Khalis et al. [36] |
| Egypt | 2021 | Other population | 1011 | 25 | Omar et al. [37] |
| Egypt | 2021 | Healthcare workers | 2133 | 54 | Saied et al. [38] |
| South Africa | 2021 | Healthcare workers | 1308 | 90.1 | Adeniyi et al. [39] |
| Malawi | 2021 | Other population | 1542 | 82.7 | Kanyanda et al. [29] |
| South Africa | 2021 | Other population | 4440 | 70.8 | Kollamparambil et al. [40] |
| Zimbabwe | 2021 | Other population | 551 | 55.7 | Mcabee et al. [41] |
| South Africa | 2021 | Healthcare workers | 1015 | 89.5 | Oduwole et al. [42] |
| Kenya | 2021 | Other population | 963 | 96 | Carpio et al. [43] |
| Uganda | 2021 | Other population | 1067 | 53.6 | Echoru et al. [44] |
| Uganda | 2021 | Other population | 2106 | 84.5 | Kanyanda et al. [29] |
| Nigeria | 2021 | Healthcare workers | 509 | 37.7 | Isah et al. [45] |
| Ghana | 2021 | Other population | 2345 | 51 | Acheampong et al. [46] |
| Nigeria | 2021 | Other population | 517 | 74.5 | Adebisi et al. [47] |
| Ghana | 2021 | Healthcare workers | 1605 | 70 | Alhassan et al. [48] |
| Nigeria | 2021 | Healthcare workers | 422 | 49.5 | Amuzie et al. [49] |
| Nigeria | 2021 | Other population | 886 | 70 | Habib et al. [50] |
| Burkina Faso | 2021 | Other population | 1742 | 79.5 | Kanyanda et al. [29] |
| Mali | 2021 | Other population | 1591 | 64.5 | Kanyanda et al. [29] |
| Nigeria | 2021 | Other population | 1703 | 86.2 | Kanyanda et al. [29] |
| Nigeria | 2021 | Other population | 440 | 40 | Mustapha et al. [51] |
| Nigeria | 2021 | Other population | 689 | 71.1 | Okafor et al. [52] |
| Nigeria | 2021 | Other population | 349 | 34.7 | Uzochukwu et al. [53] |
| Ghana | 2021 | Other population | 1560 | 35.3 | Yeboah et al. [54] |
| Zambia | 2022 | Other population | 2400 | 66 | Carcelen et al. [55] |
| South Africa | 2022 | Other population | 395 | 59 | Wiysonge et al. [56] |
| Ghana | 2022 | Other population | 108 | 59.3 | Botwe et al. [57] |
| Cameroon | 2022 | Other population | 591 | 13.5 | Ajonina-ekoti et al. [58] |
| Ethiopia | 2022 | Healthcare workers | 461 | 84.4 | Abay et al. [59] |
| Ethiopia | 2022 | Healthcare workers | 404 | 64 | Adane et al. [60] |
| Ethiopia | 2022 | Other population | 350 | 18.5 | Aynalem et al. [61] |
| Ethiopia | 2022 | Healthcare workers | 403 | 61.5 | Berhe et al. [62] |
| Ethiopia | 2022 | Healthcare workers | 319 | 72.7 | Boche et al. [63] |
| Ethiopia | 2022 | Other population | 422 | 80.9 | Dereje et al. [64] |
| Ethiopia | 2022 | Healthcare workers | 420 | 58.8 | Mose et al. [65] |
| Ethiopia | 2022 | Other population | 2317 | 88 | Strupat et al. [66] |
| Ethiopia | 2022 | Healthcare workers | 191 | 65.4 | Tolossa et al. [67] |
| Ethiopia | 2022 | Healthcare workers | 1314 | 74.8 | Yilma et al. [68] |
| Sudan | 2022 | Healthcare workers | 217 | 55.8 | Raja et al. [69] |
| Egypt | 2022 | Other population | 1053 | 31.5 | Salem et al. [70] |
| Sudan | 2022 | Healthcare workers | 400 | 63.8 | Yassin et al. [71] |
| Tunisia | 2022 | Healthcare workers | 493 | 48.1 | Zammit et al. [72] |
| South Africa | 2022 | Other population | 10,465 | 40 | Engelbrecht et al. [73] |
| South Africa | 2022 | Other population | 213 | 57 | Govere-Hwenje et al. [74] |
| South Africa | 2022 | Other population | 1662 | 50.4 | Kahn et al. [75] |
| South Africa | 2022 | Other population | 2364 | 83.3 | Modi et al. [76] |
| Malawi | 2022 | Healthcare workers | 400 | 82.5 | Moucheraud et al. [77] |
| Zambia | 2022 | Other population | 677 | 33.4 | Mudenda et al. [78] |
| Zimbabwe | 2022 | Other population | 1168 | 49.9 | Mundagowa et al. [79] |
| South Africa | 2022 | Other population | 1193 | 68 | Katoto et al. [80] |
| South Africa | 2022 | Other population | 5629 | 70.8 | Burger et al. [81] |
| South Africa | 2022 | Other population | 5862 | 76.1 | Burger et al. [81] |
| Botswana | 2022 | Other population | 5300 | 73.4 | Tlale et al. [82] |
| Tanzania | 2022 | Other population | 232 | 36.2 | Chilongola et al. [83] |
| Kenya | 2022 | Other population | 665 | 42 | Osur et al. [84] |
| Nigeria | 2022 | Other population | 1058 | 80.9 | Adedeji-adenola et al. [85] |
| Nigeria | 2022 | Other population | 3076 | 50.7 | Al-mustapha et al. [86] |
| Senegal | 2022 | Other population | 607 | 54.3 | Ba et al. [87] |
| Nigeria | 2022 | Other population | 1283 | 8.2 | Ekowo et al. [88] |
| Nigeria | 2022 | Other population | 400 | 69.5 | Ajibola et al. [89] |
| Ghana | 2022 | Other population | 415 | 73.3 | Kyei-arthur et al. [90] |
| Nigeria | 2022 | Other population | 1525 | 29 | Njoga et al. [91] |
| Nigeria | 2022 | Healthcare workers | 10,184 | 92 | Nomhwange et al. [92] |
| Nigeria | 2022 | Healthcare workers | 830 | 38.8 | Nri-ezedi et al. [93] |
| Ghana | 2022 | Other population | 362 | 62.7 | Okai and Abekah-Nkrumah, [94] |
| Nigeria | 2022 | Healthcare workers | 420 | 11.4 | Onuminya and Onuminya, [95] |
| Nigeria | 2022 | Other population | 73 | 74 | Osuagwu et al. [96] |
| Nigeria | 2022 | Healthcare workers | 305 | 38.3 | Adebowale et al. [97] |
| Nigeria | 2022 | Other population | 800 | 34.5 | Soyannwo et al. [98] |
| Year of Study | African Region | Number of Studies Found | Number of Respondents per Survey | * COVID-19 Vaccine Acceptance Rate | ||||
|---|---|---|---|---|---|---|---|---|
| Minimum | Maximum | Mean ± SD | Minimum | Maximum | Mean ± SEM | |||
| 2021 | ||||||||
| East | 10 | 405 | 4543 | 1486 ± 1311 | 39.7 | 97.9 | 68.9 ± 6.6 | |
| North | 8 | 303 | 2133 | 835 ± 640 | 21.0 | 88.0 | 45.1 ± 8.5 | |
| South | 3 | 1015 | 4440 | 2254 ± 1096 | 70.8 | 90.1 | 83.5 ± 6.3 | |
| West | 14 | 349 | 2345 | 1067 ± 659 | 29.0 | 86.2 | 56.6 ± 5.1 | |
| Total | 35 | 303 | 4543 | 1235 ± 1038 | 21.0 | 97.9 | 59.8 ± 3.8 | |
| 2022 | ||||||||
| Central | 1 | 591 | 591 | 591 | 13.5 | 13.5 | 13.5 | |
| East | 16 | 191 | 2400 | 758 ± 696 | 18.5 | 88.0 | 61.2 ± 5.1 | |
| North | 4 | 217 | 1053 | 541 ± 360 | 31.5 | 63.8 | 49.8 ± 6.9 | |
| South | 9 | 213 | 10,465 | 3675 ± 3391 | 40.0 | 83.3 | 64.2 ± 4.6 | |
| West | 15 | 73 | 10,184 | 1430 ± 2536 | 8.2 | 92.0 | 51.8 ± 6.4 | |
| Total | 45 | 73 | 10,465 | 1522 ± 2329 | 8.2 | 92.0 | 56.6 ± 3.2 | |
| Grand total | 80 | 73 | 10,465 | 1397 ± 1872 | 8.2 | 97.9 | 58.0 ± 2.4 | |
| Year of Study | African Region | * COVID-19 Vaccine Acceptance Rates Reported | |||
|---|---|---|---|---|---|
| Healthcare Workers | Other Populations | ||||
| Number of Studies Found | Mean ± SEM | Number of Studies Found | Mean ± SEM | ||
| 2021 | |||||
| Central | - | - | - | - | |
| Eastern | 4 | 54.8 ± 7.9 | 6 | 78.4 ± 7.9 | |
| North | 5 | 44.2 ± 8.6 | 3 | 46.6 ± 20.7 | |
| Southern | 2 | 89.8 ± 0.3 | 1 | 70.8.7 ± 0 | |
| West | 3 | 52.4 ± 9.4 | 11 | 57.8 ± 6.2 | |
| Total | 14 | 55.5 ± 5.6 | 21 | 62.7 ± 5.2 | |
| 2022 | |||||
| Central | - | - | 1 | 13.5 ± 0 | |
| Eastern | 8 | 70.5.8 ± 3.4 | 8 | 51.9 ± 8.6 | |
| North | 3 | 55.9 ± 4.5 | 1 | 31.5 ± 0 | |
| Southern | 0 | - | 9 | 64.2 ± 4.6 | |
| West | 4 | 45.1 ± 16.9 | 11 | 54.2 ± 6.7 | |
| Total | 15 | 60.8 ± 5.3 | 30 | 54.5 ± 4.0 | |
| Grand total | 29 | 58.3 ± 3.8 | 51 | 57.9 ± 3.2 | |
| Region | Country | Major Reasons for Hesitancy | Suggested Recommendations | References |
|---|---|---|---|---|
| Central Africa | Cameroon | Lack of confidence in COVID-19 vaccines Discriminatory COVID-19 vaccine distribution patterns in other parts of the world relative to Africa and improper COVID-19 vaccine approval timeline | Debunk myth and address concern for safety and efficacy Equitable distribution of available COVID-19 vaccines to all countries as a global good | Ajonina-ekoti et al. [58] |
| Eastern Africa | Ethiopia | Rumors on the content of the vaccine Concern about safety, effectiveness and adverse effects—teratogenicity Infodemic or disinformation of the public on the safety and efficacy of the vaccine Lack of adequate information about the vaccine Believe that the vaccine may be a biological weapon Concerns about the safety of vaccines due to the speed of the production | Education on side-effects and the importance of the vaccine to address trust deficit Health sector managers should stress awareness creation to alleviate misinformation Provision of clear information about COVID-19 and the vaccine side effects The public should rely on mass media platforms rather than social media Address safety concerns Continuous communication and health education Awareness creation on the safety and adverse effects Communications and training focusing on young health workers Vaccine literacy addressing misconception Targeted information, sensitisation and engagement campaigns bolstering confidence in the safety of approved vaccines | Aynalem et al. [61]; Mohammed et al. [30]; Angelo et al. [28]; Aemro et al. [26]; Mose et al. [65]; Berhe et al. [62]; Adane et al. [60]; Tolossa et al. [67]; Boche et al. [63]; Yilma et al. [68]; Dereje et al. [64]; Abay et al. [59]; Strupat et al. [65]; Kanyanda et al. [29] |
| Eastern Africa | Kenya | Lack of adequate information about the vaccine, concerns around vaccine safety and effectiveness, lack of trust and confidence in the vaccine | Evidence-based engagements | Osur et al. [84]; Carpio et al. [43] |
| Eastern Africa | Malawi | Exposure to negative information about the vaccine The primary reservations were safety concerns about the vaccine in general and its side effects specifically | Targeted information, sensitisation and engagement campaigns bolstering confidence in the benefits and safety of approved vaccines | Moucheraud et al. [77]; Kanyanda et al. [29] |
| Eastern Africa | Somalia | Misconceptions about the vaccine | Sensitization of the general public to dispel any misconceptions | Ahmed et al. [27] |
| Eastern Africa | Tanzania | Concerns on safety and side effects | Education on safety and benefits of the vaccine | Chilongola et al. [83] |
| Eastern Africa | Uganda | Mistrust among most community members regarding COVID-19 vaccines Safety concerns about the vaccine and its side effects | Targeted information, sensitisation and engagement campaigns bolstering confidence in the safety and effectiveness of approved vaccines | Echoru et al. [44] Kanyanda et al. [29] |
| Eastern Africa | Zambia | Doubt about the safety and effectiveness of vaccine | Provide accurate information through trusted sources of information on the benefits of the vaccine | Mudenda et al. [78]; Carcelen et al. [55] |
| Eastern Africa | Zimbabwe | Lack of trust in the government and uncertainty about vaccine effectiveness and safety | Targeted education and communication to address concerns about vaccine safety and country of manufacturer | Mundagowa et al. [79]; Mcabee et al. [41] |
| Northern Africa | Egypt | Absence of enough clinical trials Religious belief and safety concerns Fear of side effects of the vaccine Lack of trust in effectiveness and safety due to speedy production and roll-out of the vaccine. Lack of adequate information about side effects Fear of the hidden infective virus in the vaccine | Provision of sufficient and accurate information about the available vaccines Public health intervention campaigns to change negative attitudes, as an initial step to build trust Promote vaccine confidence with clear, precise, up-to-date information and involve medical personnel Structured awareness campaigns to offer transparent knowledge about the safety and efficacy of the vaccines and the technology | Fares et al. [33]; Omar et al. [37]; El-sokkary et al. [32]; Salem et al. [70]; Saied et al. [38]; Elgendy et al. [31] |
| Northern Africa | Morocco | Fear of the likely side effects and concern about the effectiveness of the vaccine | Assurance on effectiveness Awareness on safety and efficacy | Khalis et al. [35]; Khalis et al. [36] |
| Northern Africa | Sudan | Concerns about vaccine safety and effectiveness The risk of developing acute adverse events | Provide accurate information on vaccine safety and effectiveness Construction of health educational programs and more accurate information distributed and advertised by respective health authorities | Raja et al. [69] Yassin et al. [71] |
| Northern Africa | Tunisia | Fear of vaccine side effects | Effective national information campaign on safety and efficacy | Zammit et al. [72]; El-kefi et al. [34] |
| Southern Africa | Botswana | Religious beliefs and safety concerns | Target education towards hesitant population | Tlale et al. [82] |
| Southern Africa | South Africa | Lack of trust in the government Lack of trust in the safety and effectiveness of the vaccine Concerns about side effects, lack of access to the online vaccine registration platform, distrust of government, belief in conspiracy theories having no monthly income and depending on someone else to make vaccination decision Concerns about side effects, belief in conspiracy theories and speed of production | Easy-to-understand information regarding the safety and broader trust-building measures Increase confidence in vaccine efficacy. Clarify eligibility and ensure access to vaccines at times and places that are convenient Communication strategies reassuring safety and efficacy of COVID-19 vaccines and addressing sources of misinformation Trust-building intervention, intensify awareness to debunk misconception, increase vaccine literacy, awareness on efficacy of the vaccine, vaccination promotion campaigns, reinforce the message of vaccine safety and efficacy | Engelbrecht et al. [73]; Kahn et al. [75]; Govere-Hwenje et al. [74]; Wiysonge et al. [65]; Katoto et al. [80]; Kollamparambil et al. [40]; Burger et al. [81]; Burger et al. [81]; Modi et al. [76]; Oduwole et al. [42]; Adeniyi et al. [39] |
| Western Africa | Burkina Faso | Safety concerns about the vaccine and its side effects, insecurity and political instability | Targeted information, sensitisation and engagement campaigns to encourage confidence in the safety of the approved vaccines | Kanyanda et al. [29] |
| Western Africa | Ghana | Fear of vaccine’s side effects, safety concerns, mistrust, uncertainty, spiritual and religious beliefs Lack of confidence in the safety of the vaccines | Persuasion using public, religious and other influential figures, balanced and open discussion to frontally address the safety and religious concerns Public health educational intervention to address safety and side effects, strategy for attitudinal change, targeted and integrated public health education, intensify education on the benefits and side effects of COVID-19 vaccines | Yeboah et al. [54]; Acheampong et al. [64]; Botwe et al. [57]; Okai and Abekah-Nkrumah, [94]; Alhassan et al. [48]; Kyei-arthur et al. [90] |
| Western Africa | Mali | The primary reservations were safety concerns about the vaccine in general and its side effects specifically | Targeted information, sensitisation and engagement campaigns bolstering confidence in the safety of approved vaccines | Kanyanda et al. [29] |
| Western Africa | Nigeria | Difficulty in the vaccination request/registration protocols Bad feelings towards the vaccines due to negative social media Reports/rumors, personal ideology/religious beliefs against vaccination Concerned about the serious adverse effects of the vaccine Lack of trust in of the government’s policies Lack of confidence in the efficacy of the vaccine Perception of vaccine as being in trial stage, Insecurity and fear of being killed were scaring people from coming out to be vaccinated especially in insurgency-inflicted areas Corruption in procurement and distribution of the vaccines | Address the concerns of the local people rather than dispelling their concerns as merely superstitious and senseless More awareness, health education in indigenous language, targeted awareness creation Health education and promotion for a right attitude Targeted and appropriately designed advocacy and behavioral-change communication messages Liberalize access to vaccine, targeted education to debunk misconception and promote trust Structured educational programs to address safety concerns Improve government trustworthiness, improve health communication, implementation of formulated policies and strategies Awareness on safety and efficacy, provision of education and relevant information, ensure public trust is earned, intensify awareness and health education, national deployment and vaccination plan must be revised and robust enough to address the misinformation on vaccine safety | Ekowo et al. [88]; Onuminya and Onuminya, [95]; Reuben et al. [25]; Njoga et al. [91]; Soyannwo et al. [98]; Uzochukwu et al. [53]; Isah et al. [45]; Adebowale et al. [97]; Nri-ezedi et al. [93]; Mustapha et al. [51]; Amuzie et al. [49]; Al-mustapha et al. [86]; Ajibola et al. [89]; Habib et al. [50]; Okafor et al. [52]; Osuagwu et al. [96]; Adebisi et al. [47]; Adedeji-adenola et al. [85]; Kanyanda et al. [29]; Nomhwange et al. [92] |
| Western Africa | Senegal | Misinformation, fear of adverse effects and lack of adequate information from health workers | Promote vaccine confidence and reduce misinformation | Ba et al. [87] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Njoga, E.O.; Awoyomi, O.J.; Onwumere-Idolor, O.S.; Awoyomi, P.O.; Ugochukwu, I.C.I.; Ozioko, S.N. Persisting Vaccine Hesitancy in Africa: The Whys, Global Public Health Consequences and Ways-Out—COVID-19 Vaccination Acceptance Rates as Case-in-Point. Vaccines 2022, 10, 1934. https://doi.org/10.3390/vaccines10111934
Njoga EO, Awoyomi OJ, Onwumere-Idolor OS, Awoyomi PO, Ugochukwu ICI, Ozioko SN. Persisting Vaccine Hesitancy in Africa: The Whys, Global Public Health Consequences and Ways-Out—COVID-19 Vaccination Acceptance Rates as Case-in-Point. Vaccines. 2022; 10(11):1934. https://doi.org/10.3390/vaccines10111934
Chicago/Turabian StyleNjoga, Emmanuel O., Olajoju J. Awoyomi, Onyinye S. Onwumere-Idolor, Priscilla O. Awoyomi, Iniobong C. I. Ugochukwu, and Stella N. Ozioko. 2022. "Persisting Vaccine Hesitancy in Africa: The Whys, Global Public Health Consequences and Ways-Out—COVID-19 Vaccination Acceptance Rates as Case-in-Point" Vaccines 10, no. 11: 1934. https://doi.org/10.3390/vaccines10111934