

How Motives Related to Benefits for Oneself and Others Would Affect COVID-19 Vaccination in a Hong Kong Chinese General Adult Population?


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Data Collection
2.2. Development of the Questionnaire
2.3. Measurements
2.3.1. Background Information
2.3.2. Completed or Scheduled First-Dose COVID-19 Vaccination (CSFCV)
2.3.3. Personal POE
- Physical benefit (protection): Three items assessed the levels of agreement with the statements that COVID-19 vaccination behavior could (i) effectively protect oneself from COVID-19 infection, (ii) effectively protect family members from COVID-19 infection, and iii) reduce the risk of developing severe harms and deaths, in the case of having COVID-19 infection (1 = totally disagree to 5 = totally agree; Cronbach’s alpha = 0.96; CFA results: χ2/df = 0, CFI = 1.00, TLI = 1.00, SRMR = 0.00).
- Practical benefit: Four items assessed the levels of agreement with the statements that COVID-19 vaccination behavior could facilitate (i) visits to relevant public venues (e.g., restaurants and pubs), (ii) traveling with ‘vaccine passports’, (iii) fulfillment of the need/requirement related to work, and (iv) restoration of ‘normal social life’ (1 = totally disagree to 5 = totally agree; Cronbach’s alpha = 0.97; CFA results: χ2/df = 8.99, CFI = 0.99, TLI = 0.97, SRMR = 0.02).
- Emotional benefit: Two items assessed the levels of agreement with the statements that COVID-19 vaccination behavior could relief oneself from worries about (i) COVID-19 infection, and (ii) severe harms or death in the case of having COVID-19 infection (1 = totally disagree to 5 = totally agree; Cronbach’s alpha = 0.95).
- Interpersonal benefit: Two items assessed the levels of agreement with the statements that COVID-19 vaccination behavior could (i) remove social pressure when the participant’s friends ask about his/her COVID-19 vaccination status, and (ii) increase the participant’s friends’ willingness to have social gathering with him/her (1 = totally disagree to 5 = totally agree; Cronbach’s alpha = 0.89).
- Summative scale of POE (the Overall Personal Positive Outcome Expectancy Scale; OPPOES): It was formed by adding up all the 11 aforementioned item scores (Cronbach’s alpha = 0.94; CFA results: χ2/df = 5.64, CFI = 0.95, TLI = 0.92, SRMR = 0.05).
2.3.4. Personal NOE
2.3.5. Societal POE
2.3.6. Prosociality
2.4. Sample Size Planning
2.5. Statistical Analysis
3. Results
3.1. Descriptive Statistics
3.2. Correlation Analysis
3.3. Factors of CSFCV
3.4. Mediation Analysis
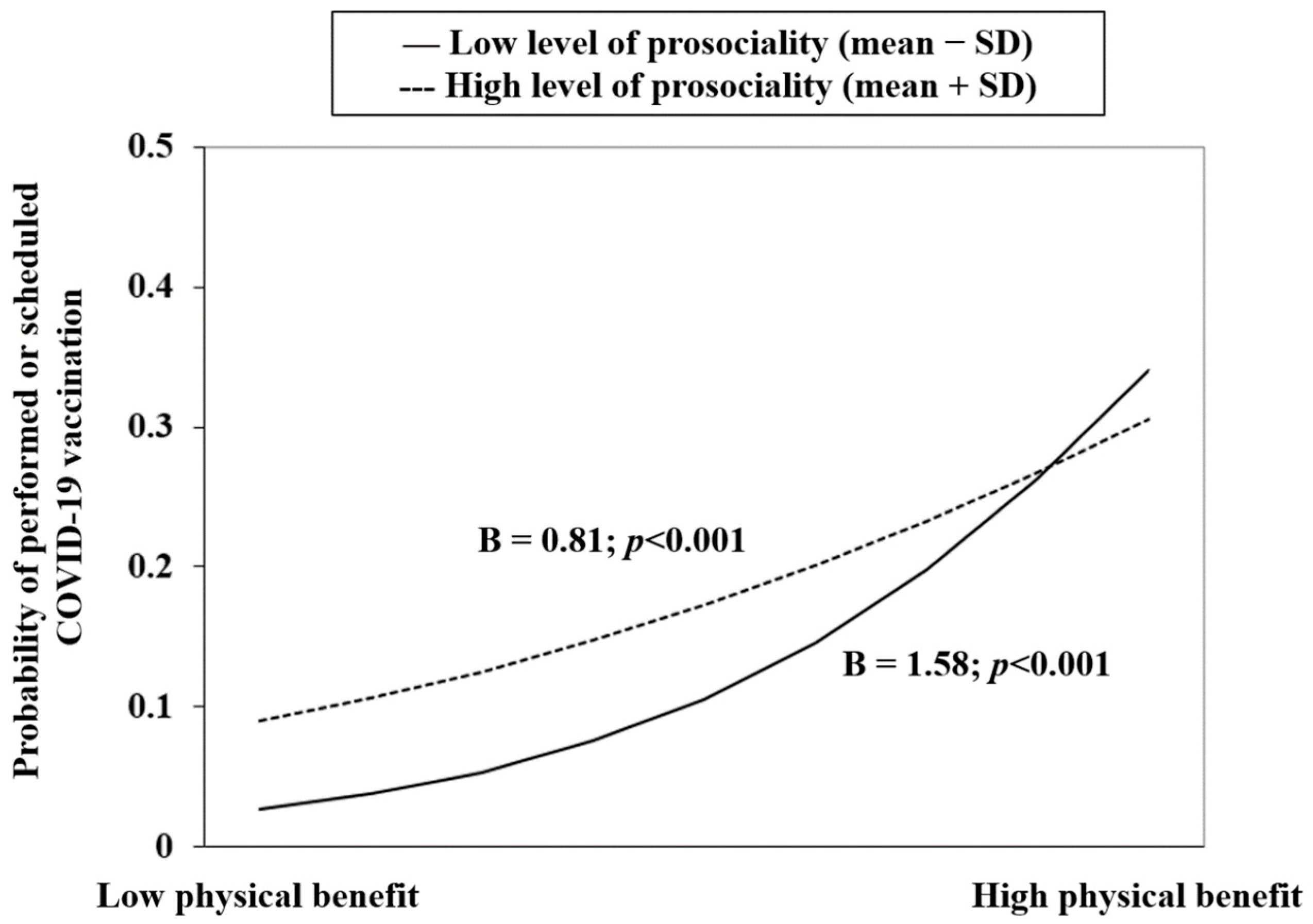
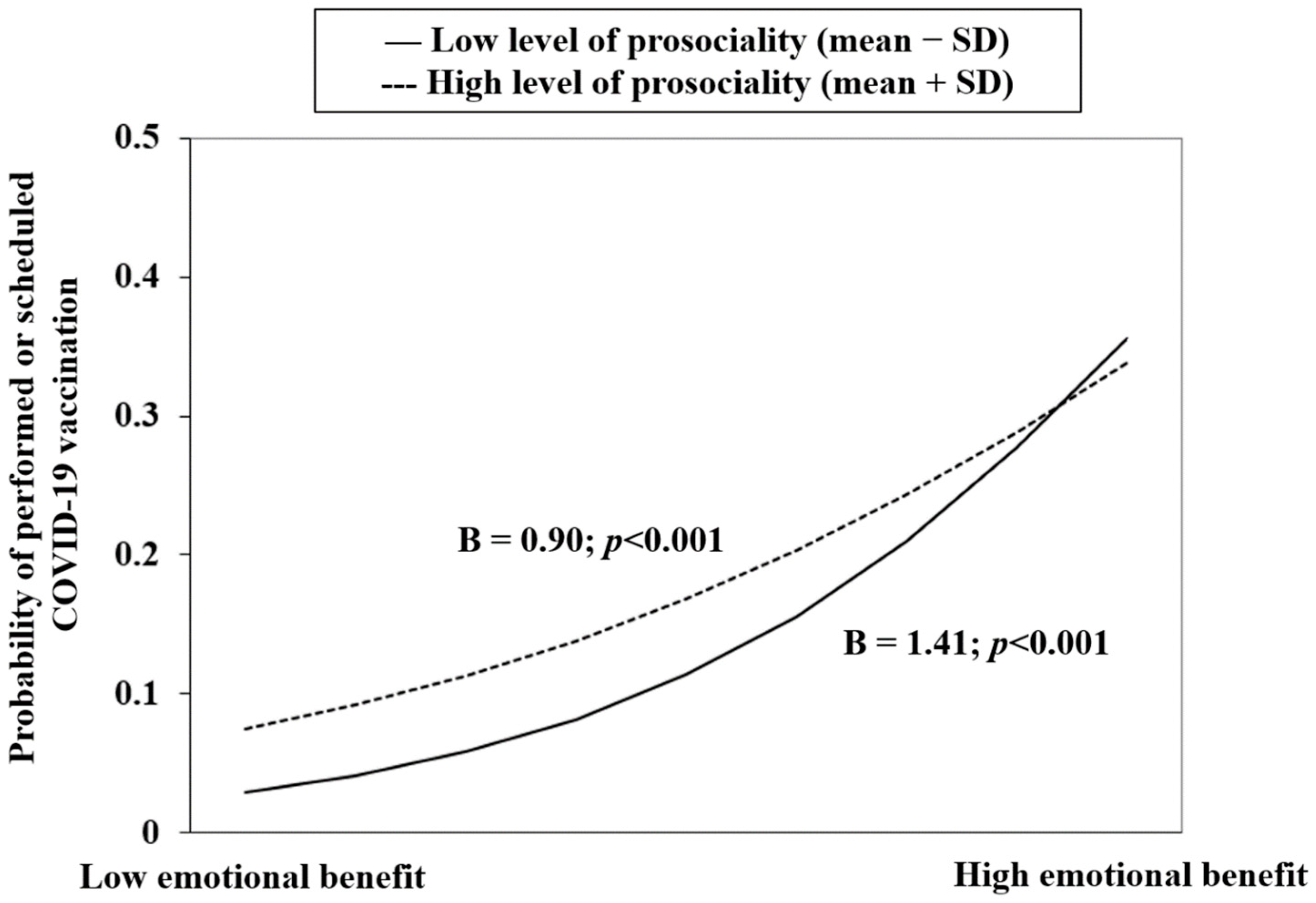
3.5. Moderation Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barchielli, B.; Cricenti, C.; Gallè, F.; Sabella, E.A.; Liguori, F.; Da Molin, G.; Liguori, G.; Orsi, G.B.; Giannini, A.M.; Ferracuti, S. Climate Changes, Natural Resources Depletion, COVID-19 Pandemic, and Russian-Ukrainian War: What Is the Impact on Habits Change and Mental Health? Int. J. Environ. Res. Public Health 2022, 19, 11929. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Vaccine Efficacy, Effectiveness and Protection. 2021. Available online: https://www.who.int/news-room/feature-stories/detail/vaccine-efficacy-effectiveness-and-protection (accessed on 22 August 2022).
- World Health Organization. Statement for Healthcare Professionals: How COVID-19 Vaccines Are Regulated for Safety And Effectiveness (Revised March 2022). 2022. Available online: https://www.who.int/news/item/17-05-2022-statement-for-healthcare-professionals-how-covid-19-vaccines-are-regulated-for-safety-and-effectiveness (accessed on 22 August 2022).
- Cerqueira-Silva, T.; Andrews, J.R.; Boaventura, V.S.; Ranzani, O.T.; de Araújo Oliveira, V.; Paixão, E.S.; Júnior, J.B.; Machado, T.M.; Hitchings, M.D.T.; Dorion, M.; et al. Effectiveness of CoronaVac, ChAdOx1 nCoV-19, BNT162b2, and Ad26.COV2.S among individuals with previous SARS-CoV-2 infection in Brazil: A test-negative, case-control study. Lancet Infect. Dis. 2022, 22, 791–801. [Google Scholar] [CrossRef]
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Robertson, C.; Stowe, J.; Tessier, E.; Simmons, R.; Cottrell, S.; Roberts, R.; O’Doherty, M.; et al. Effectiveness of the Pfizer-BioNTech and Oxford-AstraZeneca vaccines on COVID-19 related symptoms, hospital admissions, and mortality in older adults in England: Test negative case-control study. BMJ 2021, 373, n1088. [Google Scholar] [CrossRef] [PubMed]
- Bloomberg. Vaccine Tracker. 2022. Available online: https://www.bloomberg.com/graphics/covid-vaccine-tracker-global-distribution/ (accessed on 14 October 2022).
- Leung, K.; Wu, J.T.; Leung, G.M. Effects of adjusting public health, travel, and social measures during the roll-out of COVID-19 vaccination: A modelling study. Lancet Public Health 2021, 6, e674–e682. [Google Scholar] [CrossRef]
- Fajar, J.K.; Sallam, M.; Soegiarto, G.; Sugiri, Y.J.; Anshory, M.; Wulandari, L.; Kosasih, S.A.P.; Ilmawan, M.; Kusnaeni, K.; Fikri, M. Global Prevalence and Potential Influencing Factors of COVID-19 Vaccination Hesitancy: A Meta-Analysis. Vaccines 2022, 10, 1356. [Google Scholar] [CrossRef]
- Achrekar, G.C.; Batra, K.; Urankar, Y.; Batra, R.; Iqbal, N.; Choudhury, S.A.; Hooda, D.; Khan, R.; Arora, S.; Singh, A. Assessing COVID-19 booster hesitancy and its correlates: An early evidence from India. Vaccines 2022, 10, 1048. [Google Scholar] [CrossRef]
- Galanis, P.; Vraka, I.; Siskou, O.; Konstantakopoulou, O.; Katsiroumpa, A.; Kaitelidou, D. Predictors of COVID-19 vaccination uptake and reasons for decline of vaccination: A systematic review. medRxiv 2021. [Google Scholar] [CrossRef]
- Yu, Y.; Lau, J.T.F.; Lau, M.M.C.; Wong, M.C.S.; Chan, P.K.S. Understanding the Prevalence and Associated Factors of Behavioral Intention of COVID-19 Vaccination Under Specific Scenarios Combining Effectiveness, Safety, and Cost in the Hong Kong Chinese General Population. Int. J. Health Policy Manag. 2022, 11, 1090–1101. [Google Scholar] [CrossRef]
- Janz, N.K.; Becker, M.H. The health belief model: A decade later. Health Educ. Q. 1984, 11, 1–47. [Google Scholar] [CrossRef] [Green Version]
- Lao, C.K.; Li, X.; Zhao, N.; Gou, M.; Zhou, G. Using the health action process approach to predict facemask use and hand washing in the early stages of the COVID-19 pandemic in China. Curr. Psychol. 2021, 1–10. [Google Scholar] [CrossRef]
- Yu, Y.; Jia, W.; Lau, M.M.; Lau, J.T. Levels and factors derived from the Health Action Process Approach of behavioral intentions to take up COVID-19 vaccination: A random population-based study. Vaccine 2022, 40, 612–620. [Google Scholar] [CrossRef] [PubMed]
- Vayisoglu, S.K.; Zincir, H. The Health Action Process Approach-Based Program’s Effects on Influenza Vaccination Behavior. J. Nurse Pract. 2019, 15, 517–524. [Google Scholar] [CrossRef]
- Bandura, A. Social cognitive theory of self-regulation. Organ. Behav. Hum. Decis. Process. 1991, 50, 248–287. [Google Scholar] [CrossRef]
- Schwarzer, R.; Sniehotta, F.F.; Lippke, S.; Luszczynska, A.; Scholz, U.; Schüz, B.; Wegner, M.; Ziegelmann, J.P. On the assessment and analysis of variables in the health action process approach conducting an investigation. Berlin Freie Universität 2003. [Google Scholar] [CrossRef]
- Freeman, D.; Loe, B.S.; Chadwick, A.; Vaccari, C.; Waite, F.; Rosebrock, L.; Jenner, L.; Petit, A.; Lewandowsky, S.; Vanderslott, S. COVID-19 vaccine hesitancy in the UK: The Oxford coronavirus explanations, attitudes, and narratives survey (Oceans) II. Psychol. Med. 2020, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Lau, J.T.F.; She, R.; Chen, X.; Li, L.; Li, L.; Chen, X. Prevalence and associated factors of intention of COVID-19 vaccination among healthcare workers in China: Application of the Health Belief Model. Hum. Vaccin. Immunother. 2021, 17, 2894–2920. [Google Scholar] [CrossRef]
- Bandura, A. Social cognitive theory of mass communication. Media Psychol. 2001, 3, 265–299. [Google Scholar] [CrossRef]
- Li, M.; Taylor, E.G.; Atkins, K.E.; Chapman, G.B.; Galvani, A.P. Stimulating influenza vaccination via prosocial motives. PLoS ONE 2016, 11, e0159780. [Google Scholar] [CrossRef] [Green Version]
- Betsch, C.; Böhm, R.; Korn, L.; Holtmann, C. On the benefits of explaining herd immunity in vaccine advocacy. Nat. Hum. Behav. 2017, 1, 56. [Google Scholar] [CrossRef]
- Caprara, G.V.; Alessandri, G.; Eisenberg, N. Prosociality: The contribution of traits, values, and self-efficacy beliefs. J. Pers. Soc. Psychol. 2012, 102, 1289. [Google Scholar] [CrossRef]
- Yu, Y.; Luo, S.; Mo, P.K.; Wang, S.; Zhao, J.; Zhang, G.; Li, L.; Li, L.; Lau, J.T. Prosociality and Social Responsibility Were Associated With Intention of COVID-19 Vaccination among University Students in China. Int. J. Health Policy Manag. 2022, 11, 1562–1569. [Google Scholar] [CrossRef] [PubMed]
- Campos-Mercade, P.; Meier, A.; Schneider, F.; Wengström, E. Prosociality predicts health behaviors during the COVID-19 pandemic. J. Public Econ. 2021, 195, 104367. [Google Scholar] [CrossRef] [PubMed]
- Twardawski, M.; Steindorf, L.; Thielmann, I. Three pillars of physical distancing: Anxiety, prosociality, and rule compliance during the COVID-19-pandemic. Collabra Psychol. 2021, 7, 22511. [Google Scholar] [CrossRef]
- Rieger, M.O. Triggering altruism increases the willingness to get vaccinated against COVID-19. Soc. Health Behav. 2020, 3, 78. [Google Scholar] [CrossRef]
- Hong Kong S.A.R. Goverment. Hong Kong Vaccination Dashboard. 2022. Available online: https://www.covidvaccine.gov.hk/en/ (accessed on 8 October 2022).
- Office of the Communication Authority. Key Communication Statistics. 2022. Available online: https://www.ofca.gov.hk/en/news_info/data_statistics/key_stat/ (accessed on 15 September 2022).
- Yates, N.; Daniel, S.; David, S.; Starnes, N. The Practice of Statistics; Freeman Press: New York, NY, USA, 2008. [Google Scholar]
- Kim, J.H.; Lee, S.; Chow, J.; Lau, J.; Tsang, A.; Choi, J.; Griffiths, S.M. Prevalence and the factors associated with binge drinking, alcohol abuse, and alcohol dependence: A population-based study of Chinese adults in Hong Kong. Alcohol Alcohol. 2008, 43, 360–370. [Google Scholar] [CrossRef] [Green Version]
- Lau, J.T.; Kim, Y.; Wu, A.M.; Wang, Z.; Huang, B.; Mo, P.K. The Occupy Central (Umbrella) movement and mental health distress in the Hong Kong general public: Political movements and concerns as potential structural risk factors of population mental health. Soc. Psychiatry Psychiatr. Epidemiol. 2017, 52, 525–536. [Google Scholar] [CrossRef]
- Tsui, H.Y.; Lau, J.T.; Wang, Z.; Gross, D.L.; Wu, A.M.; Cao, W.; Gu, J.; Li, S. Applying the pre-intentional phase of the Health Action Process Approach (HAPA) Model to investigate factors associated with intention on consistent condom use with various types of female sex partners among males who inject drugs in China. AIDS Care 2016, 28, 1079–1088. [Google Scholar] [CrossRef]
- Mo, P.K.; Yu, Y.; Luo, S.; Wang, S.; Zhao, J.; Zhang, G.; Li, L.; Li, L.; Lau, J.T. Dualistic Determinants of COVID-19 Vaccination Intention among University Students in China: From Perceived Personal Benefits to External Reasons of Perceived Social Benefits, Collectivism, and National Pride. Vaccines 2021, 9, 1323. [Google Scholar] [CrossRef]
- Baumsteiger, R.; Siegel, J.T. Measuring prosociality: The development of a prosocial behavioral intentions scale. J. Pers. Assess. 2019, 101, 305–314. [Google Scholar] [CrossRef]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1192. [Google Scholar] [CrossRef]
- Lleras, C. Path analysis. Encycl. Soc. Meas. 2005, 3, 25–30. [Google Scholar]
- Palmer, P.B.; O’Connell, D.G. Regression analysis for prediction: Understanding the process. Cardiopulm. Phys. Ther. J. 2009, 20, 23. [Google Scholar] [CrossRef] [PubMed]
- Toyoshima, K.; Inoue, T.; Shimura, A.; Masuya, J.; Fujimura, Y.; Higashi, S.; Kusumi, I. The relationship among sleep reactivity, job-related stress, and subjective cognitive dysfunction: A cross-sectional study using path analysis. Ind. Health 2021, 59, 2020-0251. [Google Scholar] [CrossRef]
- Doba, K.; Berna, G.; Constant, E.; Nandrino, J.-L. Self-differentiation and eating disorders in early and middle adolescence: A cross-sectional path analysis. Eat. Behav. 2018, 29, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.-S.; Lee, J.-E. Factors Affecting Depression in Middle-Aged and Elderly Men Living Alone: A Cross-Sectional Path Analysis Model. Am. J. Men’s Health 2022, 16, 15579883221078134. [Google Scholar] [CrossRef]
- Greiner, B.; Ottwell, R.; Nicks, S.; Lee, A.; Hartwell, M. A Path Analysis of Physical Activity Intensity and Waist Circumference on the Lipid Profile: A Cross-sectional Study of NHANES Data. Am. J. Health Educ. 2020, 51, 310–317. [Google Scholar] [CrossRef]
- Roohafza, H.; Feizi, A.; Afshar, H.; Mazaheri, M.; Behnamfar, O.; Hassanzadeh-Keshteli, A.; Adibi, P. Path analysis of relationship among personality, perceived stress, coping, social support, and psychological outcomes. World J. Psychiatry 2016, 6, 248. [Google Scholar] [CrossRef] [Green Version]
- Maxwell, S.E.; Cole, D.A. Bias in cross-sectional analyses of longitudinal mediation. Psychol. Methods 2007, 12, 23. [Google Scholar] [CrossRef] [Green Version]
- Maxwell, S.E.; Cole, D.A.; Mitchell, M.A. Bias in cross-sectional analyses of longitudinal mediation: Partial and complete mediation under an autoregressive model. Multivar. Behav. Res. 2011, 46, 816–841. [Google Scholar] [CrossRef] [Green Version]
- Desabato, D. The Double Standard against Cross-Sectional Mediation. 2016. Available online: http://www.daviddisabato.com/blog/2016/5/22/the-double-standard-against-cross-sectional-mediation (accessed on 23 October 2022).
- Abara, W.; Annang, L.; Spencer, S.M.; Fairchild, A.J.; Billings, D. Understanding internet sex-seeking behaviour and sexual risk among young men who have sex with men: Evidences from a cross-sectional study. Sex. Transm. Infect. 2014, 90, 596–601. [Google Scholar] [CrossRef]
- Yu, Y.; Lau, J.T.; Lau, M.M. Development and validation of the conservation of resources scale for COVID-19 in the Chinese adult general population. Curr. Psychol. 2021, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Xin, M.; Luo, S.; She, R.; Yu, Y.; Li, L.; Wang, S.; Ma, L.; Tao, F.; Zhang, J.; Zhao, J.; et al. Negative cognitive and psychological correlates of mandatory quarantine during the initial COVID-19 outbreak in China. Am. Psychol. 2020, 75, 607. [Google Scholar] [CrossRef] [PubMed]
- Pfefferbaum, B.; North, C.S. Mental health and the COVID-19 pandemic. N. Engl. J. Med. 2020, 383, 510–512. [Google Scholar] [CrossRef] [PubMed]
- Hong Kong S.A.R. Goverment. Together, We Fight the Virus. 2020. Available online: https://www.coronavirus.gov.hk/sim/ (accessed on 27 July 2021).
- Bonafide, K.E.; Vanable, P.A. Male human papillomavirus vaccine acceptance is enhanced by a brief intervention that emphasizes both male-specific vaccine benefits and altruistic motives. Sex. Transm. Dis. 2015, 42, 76–80. [Google Scholar] [CrossRef]
- Mehta, P.; Sharma, M.; Lee, R.C. Designing and evaluating a health belief model-based intervention to increase intent of HPV vaccination among college males. Int. Q. Community Health Educ. 2014, 34, 101–117. [Google Scholar] [CrossRef]
- Betsch, C.; Böhm, R. Moral values do not affect prosocial vaccination. Nat. Hum. Behav. 2018, 2, 881–882. [Google Scholar] [CrossRef]
- Limbu, Y.B.; Gautam, R.K.; Pham, L. The Health Belief Model Applied to COVID-19 Vaccine Hesitancy: A Systematic Review. Vaccines 2022, 10, 973. [Google Scholar] [CrossRef]
- Batra, K.; Sharma, M.; Dai, C.-L.; Khubchandani, J. COVID-19 Booster Vaccination Hesitancy in the United States: A Multi-Theory-Model (MTM)-Based National Assessment. Vaccines 2022, 10, 758. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| n | % | |
|---|---|---|
| Background factors | ||
| Sex | ||
| Female | 303 | 60.6 |
| Male | 197 | 39.4 |
| Age groups (years) | ||
| 18–50 | 280 | 56.0 |
| 51–75 | 220 | 44.0 |
| Educational attainment | ||
| Below college | 353 | 70.6 |
| College or above | 139 | 27.8 |
| Missing response | 8 | 1.6 |
| Chronic disease status | ||
| No | 370 | 74.0 |
| Yes | 130 | 26.0 |
| History of influenza vaccination | ||
| No | 373 | 74.6 |
| Yes | 127 | 25.4 |
| Completed or scheduled first-dose COVID-19 vaccination (CSFCV) | ||
| No | 395 | 79.0 |
| Yes | 105 | 21.0 |
| Mediators | IV > M | M > DV | IV > DV | Indirect Effect | Effect Size |
|---|---|---|---|---|---|
| β | β | β | β (95% CI) | ||
| OPPOES | 0.83 *** | 0.57 *** | −0.08 | 0.48 (0.32–0.63) | Full |
| Physical benefit | 0.80 *** | 0.50 *** | −0.01 | 0.40 (0.27–0.53) | Full |
| Practical benefit | 0.76 *** | 0.26 ** | 0.20 * | 0.19 (0.07–0.32) | 49.2% |
| Emotional benefit | 0.64 *** | 0.48 *** | 0.09 | 0.31 (0.22–0.39) | Full |
| Interpersonal benefit | 0.59 *** | 0.07 | 0.35 *** | 0.04 (−0.03–0.11) | NS |
| Completed or Scheduled First-Dose COVID-19 Vaccination (CSFCV) | ||
|---|---|---|
| ORa (95% CI) | p | |
| Model 1 | ||
| OPPOES | 10.61 (1.97–57.01) | 0.006 |
| Prosociality | 2.42 (0.78–7.45) | 0.124 |
| OPPOES × Prosociality | 0.81 (0.60–1.11) | 0.190 |
| Model 2 | ||
| Physical benefit | 18.87 (4.24–83.92) | <0.001 |
| Prosociality | 4.26 (1.46–12.42) | 0.008 |
| Physical benefit × Prosociality | 0.70 (0.54–0.92) | 0.009 |
| Model 3 | ||
| Practical benefit | 2.31 (0.56–9.48) | 0.244 |
| Prosociality | 1.15 (0.39–3.40) | 0.806 |
| Practical benefit × Prosociality | 1.01 (0.77–1.32) | 0.946 |
| Model 4 | ||
| Emotional benefit | 10.51 (2.51–44.03) | 0.001 |
| Prosociality | 2.55 (0.98–6.66) | 0.055 |
| Emotional benefit × Prosociality | 0.79 (0.61–1.02) | 0.073 |
| Model 5 | ||
| Interpersonal benefit | 1.90 (0.63–5.78) | 0.256 |
| Prosociality | 1.37 (0.74–2.55) | 0.319 |
| Interpersonal benefit × Prosociality | 0.98 (0.79–1.21) | 0.836 |
| Model 6 | ||
| Personal NOE | 0.44 (0.12–1.57) | 0.206 |
| Prosociality | 1.38 (0.65–2.96) | 0.405 |
| Personal NOE × Prosociality | 0.92 (0.72–1.17) | 0.502 |
| Model 7 | ||
| Societal POE | 4.73 (1.31–17.10) | 0.018 |
| Prosociality | 2.17 (0.83–5.68) | 0.114 |
| Societal POE × Prosociality | 0.86 (0.68–1.08) | 0.192 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, Y.; Lau, M.M.C.; Lau, J.T.F. How Motives Related to Benefits for Oneself and Others Would Affect COVID-19 Vaccination in a Hong Kong Chinese General Adult Population? Vaccines 2022, 10, 1883. https://doi.org/10.3390/vaccines10111883
Yu Y, Lau MMC, Lau JTF. How Motives Related to Benefits for Oneself and Others Would Affect COVID-19 Vaccination in a Hong Kong Chinese General Adult Population? Vaccines. 2022; 10(11):1883. https://doi.org/10.3390/vaccines10111883
Chicago/Turabian StyleYu, Yanqiu, Mason M. C. Lau, and Joseph T. F. Lau. 2022. "How Motives Related to Benefits for Oneself and Others Would Affect COVID-19 Vaccination in a Hong Kong Chinese General Adult Population?" Vaccines 10, no. 11: 1883. https://doi.org/10.3390/vaccines10111883