
Safety after BBIBP-CorV (Sinopharm) COVID-19 Vaccine in Adolescents Aged 10–17 Years in Thailand
 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Interventions
2.2. Safety Measurement
2.3. Outcome
2.4. Sample Size
2.5. Statistical Analysis
3. Results
3.1. Participants
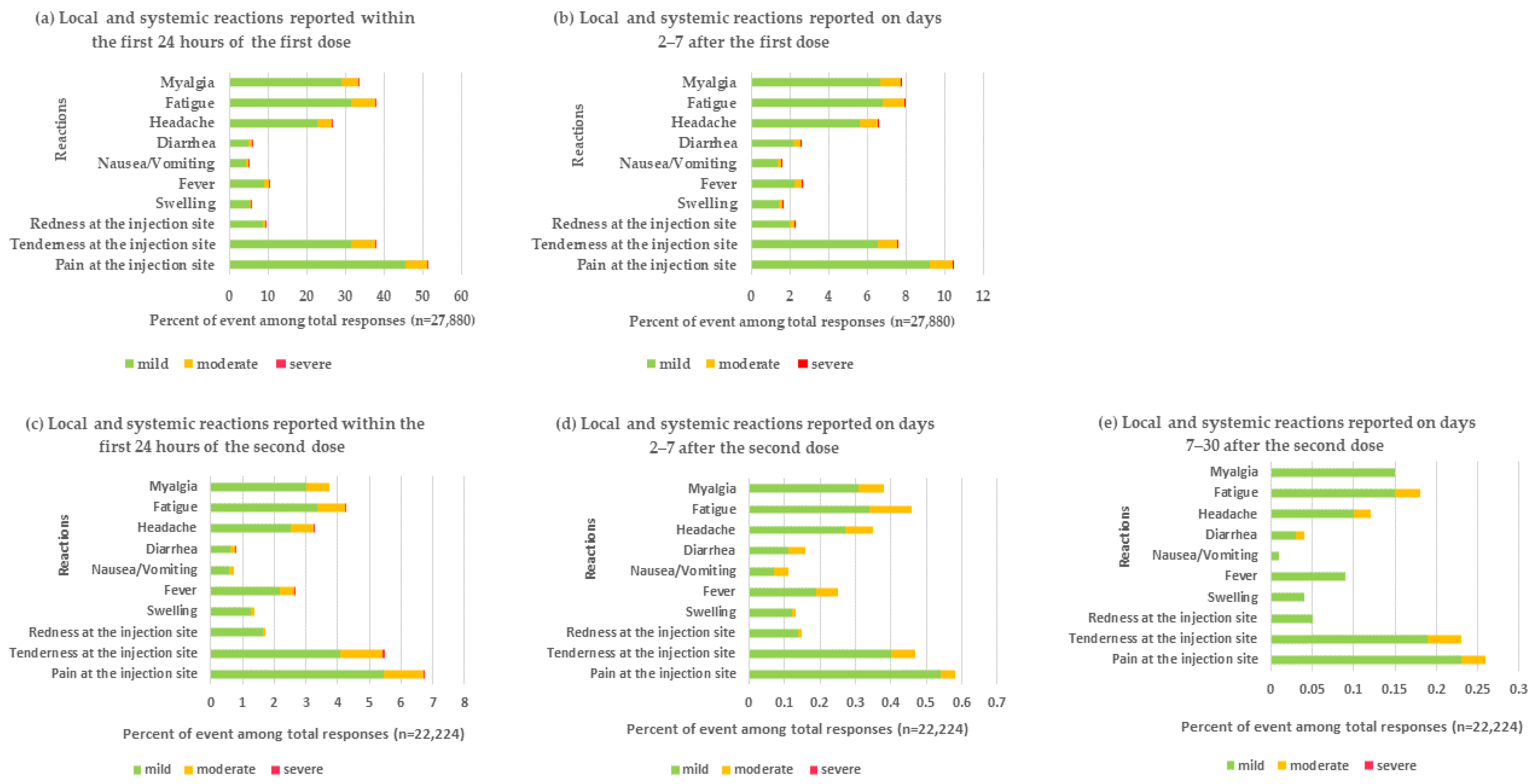
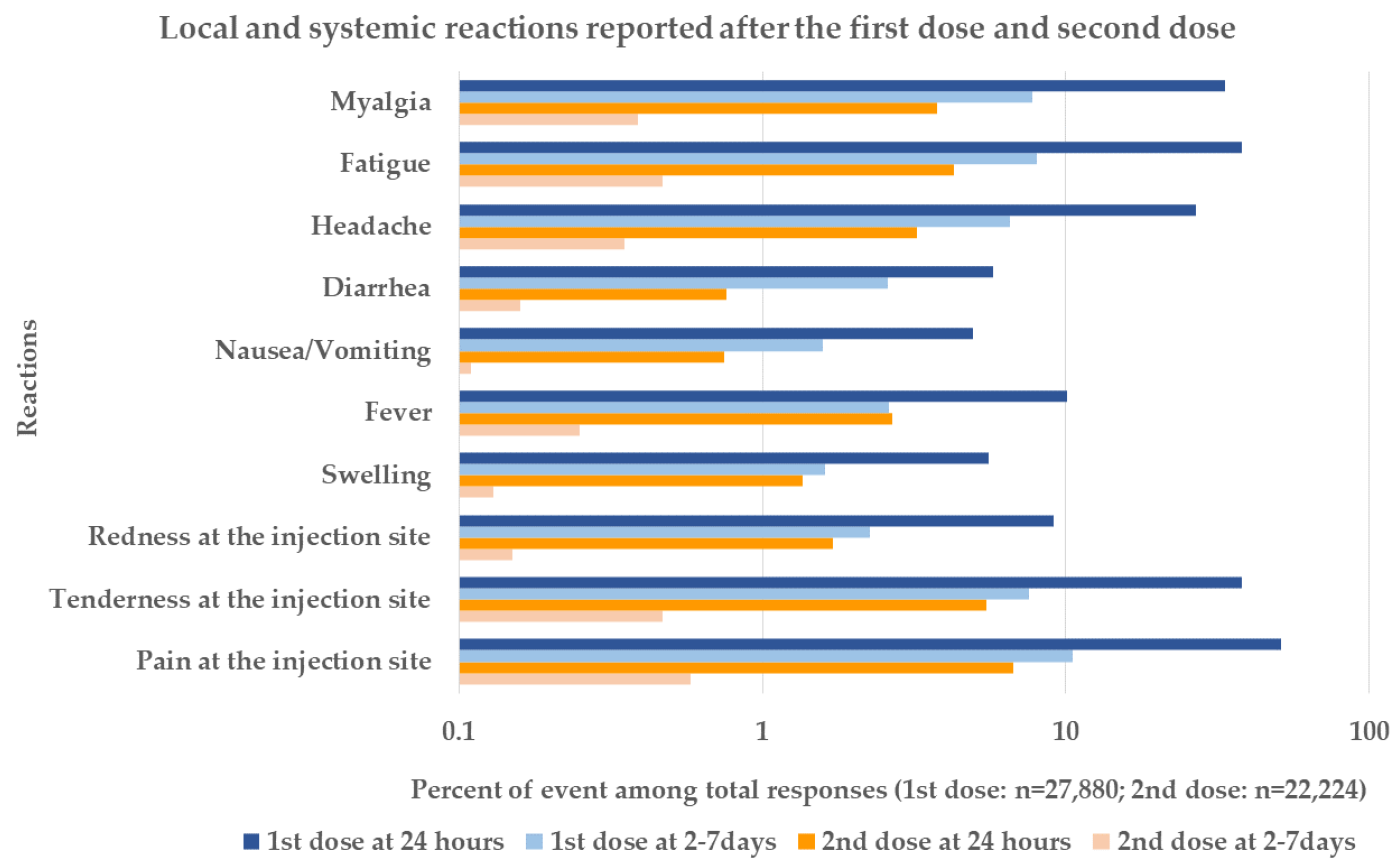
3.2. Safety and Reactogenicity
3.3. Unsolicited Events
3.3.1. Neurological Events
3.3.2. Cardiovascular Events
3.3.3. Allergic Reactions
3.3.4. Infectious Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.-L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Elharake, J.A.; Akbar, F.; Malik, A.A.; Gilliam, W.; Omer, S.B. Mental Health Impact of COVID-19 among Children and College Students: A Systematic Review. Child Psychiatry Hum. Dev. 2022, 11, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Bruce, C.; Gearing, M.E.; DeMatteis, J.; Levin, K.; Mulcahy, T.; Newsome, J.; Wivagg, J. Financial vulnerability and the impact of COVID-19 on American households. PLoS ONE 2022, 17, e0262301. [Google Scholar] [CrossRef]
- Arons, M.M.; Hatfield, K.M.; Reddy, S.C.; Kimball, A.; James, A.; Jacobs, J.R.; Taylor, J.; Spicer, K.; Bardossy, A.C.; Oakley, L.P.; et al. Presymptomatic SARS-CoV-2 Infections and Transmission in a Skilled Nursing Facility. N. Engl. J. Med. 2020, 382, 2081–2090. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Pei, S.; Chen, B.; Song, Y.; Zhang, T.; Yang, W.; Shaman, J. Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV-2). Sci. (Am. Assoc. Adv. Sci.) 2020, 368, 489–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Weekly Epidemiological Update on COVID-19–25 January 2022. 2022. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---25-january-2022 (accessed on 31 January 2022).
- Kim, T.Y.; Kim, E.C.; Agudelo, A.Z.; Friedman, L. COVID-19 hospitalization rate in children across a private hospital network in the United States: COVID-19 hospitalization rate in children. Arch. De Pédiatrie. 2021, 28, 530–532. [Google Scholar] [CrossRef]
- Cui, X.; Zhao, Z.; Zhang, T.; Guo, W.; Guo, W.; Zheng, J.; Zhang, J.; Dong, C.; Na, R.; Zheng, L.; et al. A systematic review and meta-analysis of children with coronavirus disease 2019 (COVID-19). J. Med. Virol. 2021, 93, 1057–1069. [Google Scholar] [CrossRef]
- Santaniello, M.; Matucci-Cerinic, C.; Natoli, V.; Trincianti, C.; Ridella, F.; Ravelli, A.; Luigi Marseglia, G. Childhood multisystem inflammatory syndrome associated with COVID-19 (MIS-C): Distinct from Kawasaki disease or part of the same spectrum? Pediatric Allergy Immunol. 2022, 33, 102–104. [Google Scholar] [CrossRef]
- Khandker, S.S.; Godman, B.; Jawad, M.I.; Meghla, B.A.; Tisha, T.A.; Khondoker, M.U.; Haq, M.A.; Charan, J.; Talukder, A.A.; Azmuda, N.; et al. A Systematic Review on COVID-19 Vaccine Strategies, Their Effectiveness, and Issues. Vaccines 2021, 9, 1387. [Google Scholar] [CrossRef]
- Sharma, K.; Koirala, A.; Nicolopoulos, K.; Chiu, C.; Wood, N.; Britton, P.N. Vaccines for COVID-19: Where do we stand in 2021? Paediatr. Respir. Rev. 2021, 39, 22–31. [Google Scholar] [CrossRef]
- Tsabouri, S.; Makis, A.; Kosmeri, C.; Siomou, E. Risk factors for severity in children with coronavirus disease 2019: A comprehensive literature review. Pediatric. Clin. 2021, 68, 321–338. [Google Scholar]
- Principi, N.; Esposito, S. Reasons in favour of universal vaccination campaign against COVID-19 in the pediatric population. Ital. J. Pediatrics 2022, 48, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Plotkin, S.A.; Levy, O. Considering mandatory vaccination of children for COVID-19. Pediatrics 2021, 147, e2021050531. [Google Scholar] [CrossRef] [PubMed]
- Meuris, C.; Kremer, C.; Geerinck, A.; Locquet, M.; Bruyère, O.; Defêche, J.; Meex, C.; Hayette, M.-P.; Duchene, L.; Dellot, P. Transmission of SARS-CoV-2 after COVID-19 screening and mitigation measures for primary school children attending School in Liège, Belgium. JAMA Netw. Open 2021, 4, e2128757. [Google Scholar] [CrossRef] [PubMed]
- Dionne, A.; Sperotto, F.; Chamberlain, S.; Baker, A.L.; Powell, A.J.; Prakash, A.; Castellanos, D.A.; Saleeb, S.F.; de Ferranti, S.D.; Newburger, J.W. Association of myocarditis with BNT162b2 messenger RNA COVID-19 vaccine in a case series of children. JAMA Cardiol. 2021, 6, 1446–1450. [Google Scholar] [CrossRef]
- Oster, M.E.; Shay, D.K.; Su, J.R.; Gee, J.; Creech, C.B.; Broder, K.R.; Edwards, K.; Soslow, J.H.; Dendy, J.M.; Schlaudecker, E. Myocarditis Cases Reported After mRNA-Based COVID-19 Vaccination in the US From December 2020 to August 2021. JAMA 2022, 327, 331–340. [Google Scholar] [CrossRef]
- Jahromi, M.; Al Sheikh, M.H. Partial protection of Sinopharm vaccine against SARS COV2 during recent outbreak in Bahrain. Microb. Pathog. 2021, 158, 105086. [Google Scholar] [CrossRef]
- Ndwandwe, D.; Wiysonge, C.S. COVID-19 vaccines. Curr. Opin. Immunol. 2021, 71, 111–116. [Google Scholar] [CrossRef]
- Mallapaty, S. China’s COVID vaccines are going global—But questions remain. Nature 2021, 593, 178–179. [Google Scholar] [CrossRef]
- Tawinprai, K.; Siripongboonsitti, T.; Porntharukchareon, T.; Vanichsetakul, P.; Thonginnetra, S.; Niemsorn, K.; Promsena, P.; Tandhansakul, M.; Kasemlawan, N.; Ruangkijpaisal, N. Safety and Immunogenicity of the BBIBP-CorV Vaccine in Adolescents Aged 12 to 17 Years in the Thai Population: An Immunobridging Study. Vaccines 2022, 10, 807. [Google Scholar] [CrossRef]
- Almufty, H.B.; Mohammed, S.A.; Abdullah, A.M.; Merza, M.A. Potential adverse effects of COVID19 vaccines among Iraqi population; a comparison between the three available vaccines in Iraq; a retrospective cross-sectional study. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 102207. [Google Scholar] [CrossRef] [PubMed]
- Cai, C.; Peng, Y.; Shen, E.; Huang, Q.; Chen, Y.; Liu, P.; Guo, C.; Feng, Z.; Gao, L.; Zhang, X.; et al. A comprehensive analysis of the efficacy and safety of COVID-19 vaccines. Mol. Ther. 2021, 29, 2794–2805. [Google Scholar] [CrossRef] [PubMed]
- Xia, S.; Zhang, Y.; Wang, Y.; Wang, H.; Yang, Y.; Gao, G.F.; Tan, W.; Wu, G.; Xu, M.; Lou, Z.; et al. Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBIBP-CorV: A randomised, double-blind, placebo-controlled, phase 1/2 trial. Lancet Infect. Dis. 2021, 21, 39–51. [Google Scholar] [CrossRef]
- Suthar, A.B.; Wang, J.; Seffren, V.; Wiegand, R.E.; Griffing, S.; Zell, E. Public health impact of COVID-19 vaccines in the US: Observational study. BMJ 2022, 377, e069317. [Google Scholar] [CrossRef] [PubMed]
- Zambrano, L.D.; Newhams, M.M.; Olson, S.M.; Halasa, N.B.; Price, A.M.; Boom, J.A.; Sahni, L.C.; Kamidani, S.; Tarquinio, K.M.; Maddux, A.B. Effectiveness of BNT162b2 (Pfizer-BioNTech) mRNA vaccination against multisystem inflammatory syndrome in children among persons aged 12–18 years—United States, July–December 2021. Morb. Mortal. Wkly. Rep. 2022, 71, 52. [Google Scholar] [CrossRef]
- World Health Organization. Interim Statement on COVID-19 Vaccination for Children. 2022. Available online: https://www.who.int/news/item/11-08-2022-interim-statement-on-covid-19-vaccination-for-children (accessed on 4 September 2022).
- World Health Organization. Coronavirus Disease 2019 (COVID-19) WHO Thailand Situation Update No. 202. 2021. Available online: https://cdn.who.int/media/docs/default-source/searo/thailand/2021_09_23_eng-sitrep-202-covid19.pdf?sfvrsn=7723bbd1_5 (accessed on 14 October 2022).
- Kitro, A.; Sirikul, W.; Dilokkhamaruk, E.; Sumitmoh, G.; Pasirayut, S.; Wongcharoen, A.; Panumasvivat, J.; Ongprasert, K.; Sapbamrer, R. COVID-19 vaccine hesitancy and influential factors among Thai parents and guardians to vaccinate their children. Vaccine X 2022, 11, 100182. [Google Scholar] [CrossRef] [PubMed]
- Xia, S.; Zhang, Y.; Wang, Y.; Wang, H.; Yang, Y.; Gao, G.F.; Tan, W.; Wu, G.; Xu, M.; Lou, Z.; et al. Safety and immunogenicity of an inactivated COVID-19 vaccine, BBIBP-CorV, in people younger than 18 years: A randomised, double-blind, controlled, phase 1/2 trial. Lancet Infect. Dis. 2022, 22, 196–208. [Google Scholar] [CrossRef]
- Han, B.; Song, Y.; Li, C.; Yang, W.; Ma, Q.; Jiang, Z.; Li, M.; Lian, X.; Jiao, W.; Wang, L.; et al. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine (CoronaVac) in healthy children and adolescents: A double-blind, randomised, controlled, phase 1/2 clinical trial. Lancet Infect. Dis. 2021, 21, 1645–1653. [Google Scholar] [CrossRef]
- Gao, P.; Cai, S.; Liu, Q.; Du, M.; Liu, J.; Liu, M. Effectiveness and Safety of SARS-CoV-2 Vaccines among Children and Adolescents: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 421. [Google Scholar] [CrossRef]
- Frenck, R.W.; Klein, N.P.; Kitchin, N.; Gurtman, A.; Absalon, J.; Lockhart, S.; Perez, J.L.; Walter, E.B.; Senders, S.; Bailey, R.; et al. Safety, Immunogenicity, and Efficacy of the BNT162b2 Covid-19 Vaccine in Adolescents. N. Engl. J. Med. 2021, 385, 239–250. [Google Scholar] [CrossRef]
- Rosa Duque, J.S.; Wang, X.; Leung, D.; Cheng, S.M.S.; Cohen, C.A.; Mu, X.; Hachim, A.; Zhang, Y.; Chan, S.M.; Chaothai, S.; et al. Immunogenicity and reactogenicity of SARS-CoV-2 vaccines BNT162b2 and CoronaVac in healthy adolescents. Nat. Commun. 2022, 13, 3700. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Immunization Stress-Related Response: A Manual for Program Managers and Health Professionals to Prevent, Identify and Respond to Stress-Related Responses Following Immunization. 2019. Available online: https://apps.who.int/iris/bitstream/handle/10665/330277/9789241515948-eng.pdf (accessed on 31 March 2022).
- Apiwattanakul, M.; Suanprasert, N.; Rojana-Udomsart, A.; Termglinchan, T.; Sinthuwong, C.; Tantirittisak, T.; Hanchaiphiboolkul, S.; Angchaisuksiri, P.; Srimahachota, S.; Wongsawat, J. Good recovery of immunization stress-related responses presenting as cluster of stroke-like events following CoronaVac and ChAdOx1 vaccinations. medRxiv 2022, 17, e0266118. [Google Scholar] [CrossRef]
- Suwanwela, N.; Kijpaisalratana, N.; Tepmongkol, S.; Vorasayan, P.; Charnnarong, C.; Tantivatana, J.; Rattanawong, W.; Roongruang, S.; Ongphichetmetha, T.; Akarathanawat, W.; et al. Immunization related focal neurological syndrome after coronavac vaccination. J. Neurol. Sci. 2021, 429, 119916. [Google Scholar] [CrossRef]
- Vestergaard, M.; Hviid, A.; Madsen, K.M.; Wohlfahrt, J.; Thorsen, P.; Schendel, D.; Melbye, M.; Olsen, J. MMR Vaccination and Febrile Seizures: Evaluation of Susceptible Subgroups and Long-term Prognosis. JAMA J. Am. Med. Assoc. 2004, 292, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Scheffer, I.E. Vaccination Triggers, Rather than Causes, Seizures: Vaccination Triggers, Rather Than Causes, Seizures. Epilepsy Curr. 2015, 15, 335–337. [Google Scholar] [CrossRef] [Green Version]
- Aliasin, M.M.; Yazdanpanah, N.; Rezaei, N. Neurological and neuropsychological adverse effects of SARS-CoV-2 vaccines–where do we stand? Rev. Neurosci. 2022, 33, 721–743. [Google Scholar] [CrossRef] [PubMed]
- Wan, E.Y.F.; Chui, C.S.L.; Lai, F.T.T.; Chan, E.W.Y.; Li, X.; Yan, V.K.C.; Gao, L.; Yu, Q.; Lam, I.C.H.; Chun, R.K.C.; et al. Bell’s palsy following vaccination with mRNA (BNT162b2) and inactivated (CoronaVac) SARS-CoV-2 vaccines: A case series and nested case-control study. Lancet Infect. Dis. 2022, 22, 64–72. [Google Scholar] [CrossRef]
- Garg, R.K.; Paliwal, V.K. Spectrum of neurological complications following COVID-19 vaccination. Neurol. Sci. 2021, 43, 3–40. [Google Scholar] [CrossRef]
- Pitaro, J.; Waissbluth, S.; Daniel, S.J. Do children with Bell’s palsy benefit from steroid treatment? A systematic review. Int. J. Pediatric Otorhinolaryngol. 2012, 76, 921–926. [Google Scholar] [CrossRef]
- Yoo, H.W.; Yoon, L.; Kim, H.Y.; Kwak, M.J.; Park, K.H.; Bae, M.H.; Lee, Y.; Nam, S.O.; Kim, Y.M. Comparison of conservative therapy and steroid therapy for Bell’s palsy in children. Korean J. Pediatrics 2018, 61, 332–337. [Google Scholar] [CrossRef]
- Ismail, A.Q.; Alake, O.; Kallappa, C. Do Oral Steroids Aid Recovery in Children With Bell’s Palsy? J. Child Neurol. 2014, 29, NP96–NP97. [Google Scholar] [CrossRef] [PubMed]
- Mussatto, C.C.; Sokol, J.; Alapati, N. Bell’s palsy following COVID-19 vaccine administration in HIV+ patient. Am. J. Ophthalmol. Case Rep. 2022, 25, 101259. [Google Scholar] [CrossRef]
- Gómez de Terreros Caro, G.; Gil Díaz, S.; Pérez Alé, M.; Martínez Gimeno, M.L. Bell’s palsy following COVID-19 vaccination: A case report. Neurol. (Barc. Engl. Ed.) 2021, 36, 567–568. [Google Scholar] [CrossRef] [PubMed]
- Munro, C. Covid-19: Boys are more at risk of myocarditis after vaccination than of hospital admission for covid. BMJ 2021, 374, n2251. [Google Scholar] [CrossRef]
- Bozkurt, B.; Kamat, I.; Hotez, P.J. Myocarditis with COVID-19 mRNA vaccines. Circulation 2021, 144, 471–484. [Google Scholar] [CrossRef] [PubMed]
- Fleming-Nouri, A.; Haimovich, A.D.; Yang, D.; Schulz, W.L.; Coppi, A.; Taylor, R.A. Myopericarditis in young adults presenting to the emergency department after receiving a second COVID-19 mRNA vaccine. Acad. Emerg. Med. 2021, 28, 802. [Google Scholar] [CrossRef]
- Mevorach, D.; Anis, E.; Cedar, N.; Bromberg, M.; Haas, E.J.; Nadir, E.; Olsha-Castell, S.; Arad, D.; Hasin, T.; Levi, N. Myocarditis after BNT162b2 mRNA vaccine against Covid-19 in Israel. N. Engl. J. Med. 2021, 385, 2140–2149. [Google Scholar] [CrossRef]
- Husby, A.; Hansen, J.V.; Fosbøl, E.; Thiesson, E.M.; Madsen, M.; Thomsen, R.W.; Sørensen, H.T.; Andersen, M.; Wohlfahrt, J.; Gislason, G.; et al. SARS-CoV-2 vaccination and myocarditis or myopericarditis: Population based cohort study. BMJ 2021, 375, e068665. [Google Scholar] [CrossRef]
- Cui, G.; Li, R.; Zhao, C.; Wang, D.W. Case Report: COVID-19 Vaccination Associated Fulminant Myocarditis. Front. Cardiovasc. Med. 2022, 8, 769616. [Google Scholar] [CrossRef]
- Ling, R.R.; Ramanathan, K.; Tan, F.L.; Tai, B.C.; Somani, J.; Fisher, D.; MacLaren, G. Myopericarditis following COVID-19 vaccination and non-COVID-19 vaccination: A systematic review and meta-analysis. Lancet Respir. Med. 2022, 10, 679–688. [Google Scholar] [CrossRef]
- Raj, S.R.; Fedorowski, A.; Sheldon, R.S. Diagnosis and management of postural orthostatic tachycardia syndrome. Can. Med. Assoc. J. 2022, 194, E378–E385. [Google Scholar] [CrossRef] [PubMed]
- Ståhlberg, M.; Reistam, U.; Fedorowski, A.; Villacorta, H.; Horiuchi, Y.; Bax, J.; Pitt, B.; Matskeplishvili, S.; Lüscher, T.F.; Weichert, I.; et al. Post-COVID-19 Tachycardia Syndrome: A Distinct Phenotype of Post-Acute COVID-19 Syndrome. Am. J. Med. 2021, 134, 1451–1456. [Google Scholar] [CrossRef] [PubMed]
- Reddy, S.; Reddy, S.; Arora, M. A case of postural orthostatic tachycardia syndrome secondary to the messenger RNA COVID-19 vaccine. Cureus 2021, 13, e14837. [Google Scholar] [CrossRef] [PubMed]
- Greenhawt, M.; Abrams, E.M.; Shaker, M.; Chu, D.K.; Kahn, D.; Akin, C.; Alqurashi, W.; Arkwright, P.; Baldwin, J.L.; Ben-Shoshan, M.; et al. The risk of allergic reaction to SARS-CoV-2 vaccines and recommended evaluation and management: A systematic review, meta-analysis, GRADE assessment, and international consensus approach. Rev. Feature Artic. 2021, 9, 3546–3567. [Google Scholar] [CrossRef]
- Alhumaid, S.; Al Mutair, A.; Al Alawi, Z.; Rabaan, A.A.; Tirupathi, R.; Alomari, M.A.; Alshakhes, A.S.; Alshawi, A.M.; Ahmed, G.Y.; Almusabeh, H.M.; et al. Anaphylactic and nonanaphylactic reactions to SARS-CoV-2 vaccines: A systematic review and meta-analysis. Allergy Asthma Clin. Immunol. 2021, 17, 1–109. [Google Scholar] [CrossRef]
- Walter, E.B.; Talaat, K.R.; Sabharwal, C.; Gurtman, A.; Lockhart, S.; Paulsen, G.C.; Barnett, E.D.; Muñoz, F.M.; Maldonado, Y.; Pahud, B.A.; et al. Evaluation of the BNT162b2 Covid-19 Vaccine in Children 5 to 11 Years of Age. N. Engl. J. Med. 2022, 386, 35–46. [Google Scholar] [CrossRef]
- Kounis, N.G.; Koniari, I.; de Gregorio, C.; Velissaris, D.; Petalas, K.; Brinia, A.; Assimakopoulos, S.F.; Gogos, C.; Kouni, S.N.; Kounis, G.N.; et al. Allergic Reactions to Current Available COVID-19 Vaccinations: Pathophysiology, Causality, and Therapeutic Considerations. Vaccines 2021, 9, 221. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Anastassopoulou, C.; Hatziantoniou, S.; Poland, G.A.; Tsakris, A. Anaphylaxis rates associated with COVID-19 vaccines are comparable to those of other vaccines. Vaccine 2022, 40, 183–186. [Google Scholar] [CrossRef]
- Iwanaga, J.; Fukuoka, H.; Fukuoka, N.; Yutori, H.; Ibaragi, S.; Tubbs, R.S. A narrative review and clinical anatomy of herpes zoster infection following COVID-19 vaccination. Clin. Anat. 2022, 35, 45–51. [Google Scholar] [CrossRef]
- Thonginnetra, S.; Limtanyakul, P.; Tawinprai, K. Herpes zoster after COVID-19 vaccination in an adolescent. Dermatol. Online J. 2022, 28, 17. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Dose 1 N (%) | Dose 2 N (%) | |
|---|---|---|
| Total participants | 27,880 | 22,224 |
| Sex | ||
| male | 14,852 (53.27) | 11,717 (52.72) |
| female | 13,028 (46.73) | 10,507 (47.28) |
| Age (mean ± SD *) | 13.00 ± 2.33 | 12.59 ± 2.24 |
| System | Symptoms/Diseases | Number of Cases |
|---|---|---|
| Transient left hemiparesis and paresthesia/immunization-related focal neurological syndrome | 1 |
| Seizure | 1 | |
| Bell’s palsy | 1 | |
| Arrhythmia (transient tachycardia and premature atrial contraction) | 2 |
| Postural orthostatic tachycardia syndrome | 2 | |
| Myocarditis | 1 | |
| Anaphylaxis | 1 |
| Herpes Zoster | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thonginnetra, S.; Tawinprai, K.; Niemsorn, K.; Promsena, P.; Tandhansakul, M.; Kasemlawan, N.; Ruangkijpaisal, N.; Banomyong, N.; Phattraprayoon, N.; Rangkakulnuwat, P.; et al. Safety after BBIBP-CorV (Sinopharm) COVID-19 Vaccine in Adolescents Aged 10–17 Years in Thailand. Vaccines 2022, 10, 1765. https://doi.org/10.3390/vaccines10101765
Thonginnetra S, Tawinprai K, Niemsorn K, Promsena P, Tandhansakul M, Kasemlawan N, Ruangkijpaisal N, Banomyong N, Phattraprayoon N, Rangkakulnuwat P, et al. Safety after BBIBP-CorV (Sinopharm) COVID-19 Vaccine in Adolescents Aged 10–17 Years in Thailand. Vaccines. 2022; 10(10):1765. https://doi.org/10.3390/vaccines10101765
Chicago/Turabian StyleThonginnetra, Saraiorn, Kriangkrai Tawinprai, Krongkwan Niemsorn, Pathariya Promsena, Manunya Tandhansakul, Naruporn Kasemlawan, Natthanan Ruangkijpaisal, Narin Banomyong, Nanthida Phattraprayoon, Pisuttikan Rangkakulnuwat, and et al. 2022. "Safety after BBIBP-CorV (Sinopharm) COVID-19 Vaccine in Adolescents Aged 10–17 Years in Thailand" Vaccines 10, no. 10: 1765. https://doi.org/10.3390/vaccines10101765