2.1. Study Design
This seasonal influenza vaccination study was conducted at a local university in Hong Kong with three campuses during the 2021–22 flu season (September 2021 to March 2022). The intervention programme was conducted campus-wide in the self-financed unit of the university with 9533 undergraduate students located on two campuses. The third campus offering government-funded tertiary university programs with 15,151 undergraduate students was taken as the control group. Since there are no cross-campus activities between the intervention campuses and the control campus, students in the control campus were not exposed to any intervention materials throughout the research period. All three campuses offer similar disciplines of programs except that the control campus also offers health programs (e.g., nursing, physiotherapy, and occupational therapy) in which students will usually be required to receive flu vaccine prior to clinical internship. Since social marketing studies focus to influence ‘voluntary’ behaviour, the campus with health programs was used as the control campus.
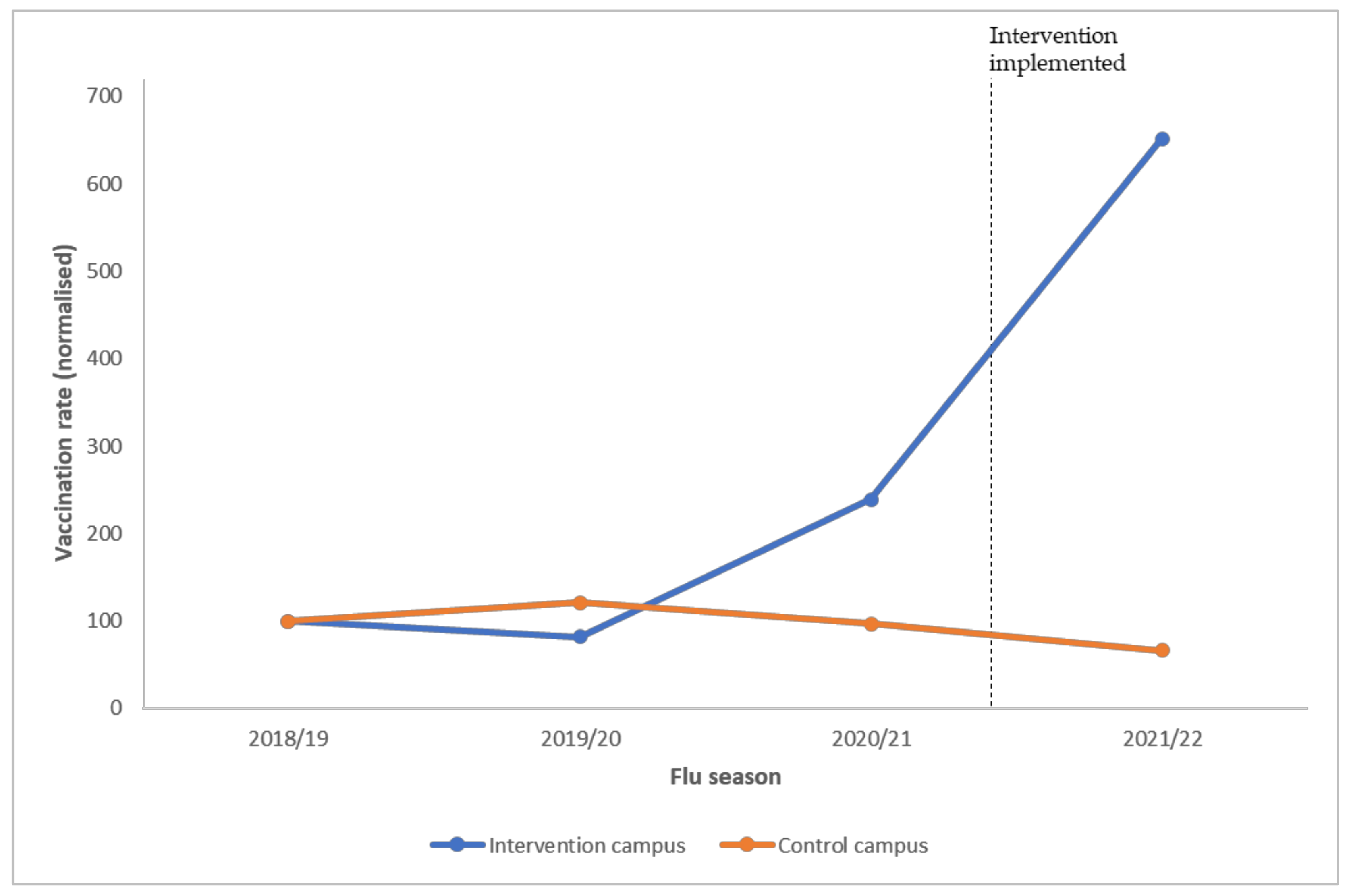
In previous years, all three campuses have promoted seasonal flu vaccination using the same promotion activities. In the intervention year, additional promotional materials developed for this study would only be presented in two intervention campus groups. Usual promotion tactics that were used in previous years were also delivered across all campuses (ie., both intervention campuses and the control campus). Besides comparison with the control group, flu vaccine uptake during the 2021–2022 season would also be compared with data from the 2018–2019, 2019–2020, and 2020–2021 seasons as a baseline measure. This is to ensure that the reference point to which the programme’s effectiveness was compared would not be affected by external and environmental factors, such as the 2019 social movement and the COVID-19 pandemic that caused campus close-downs and suspension of on-campus health centre services.
2.2. Intervention Programme Design Following the CBE Framework
The flu vaccination social marketing programme in this study was developed, implemented, and evaluated following the co-create-build-engage (CBE) framework [
14]. The social marketing benchmark criteria were firstly proposed by Andreasen [
15] and were further expanded into the eight benchmark criteria by the National Social Marketing Centre [
16], these were supposed to serve as the principles for social marketers to qualify their interventions as social marketing. Realising there is still little effort made toward applying the principles which set social marketing apart from other behavioural science approaches, Rundle-Thiele et al. [
14] developed the CBE framework to serve as a three-step guide for the design, implementation, and evaluation of a genuine social marketing programme. Founded on top of the social marketing benchmark criteria, the CBE framework provides those who would like to design and implement a social marketing programme with more than just an overall checklist delivering a step-by-step guide with instructions on exactly when the eight elements from the benchmark criteria should be involved during the whole process of developing an intervention for the first time. The following sections (
Section 2.2.1,
Section 2.2.2 and
Section 2.2.3) delineate how the social marketing flu vaccination programme in this study was developed and implemented with the guidance of the CBE process.
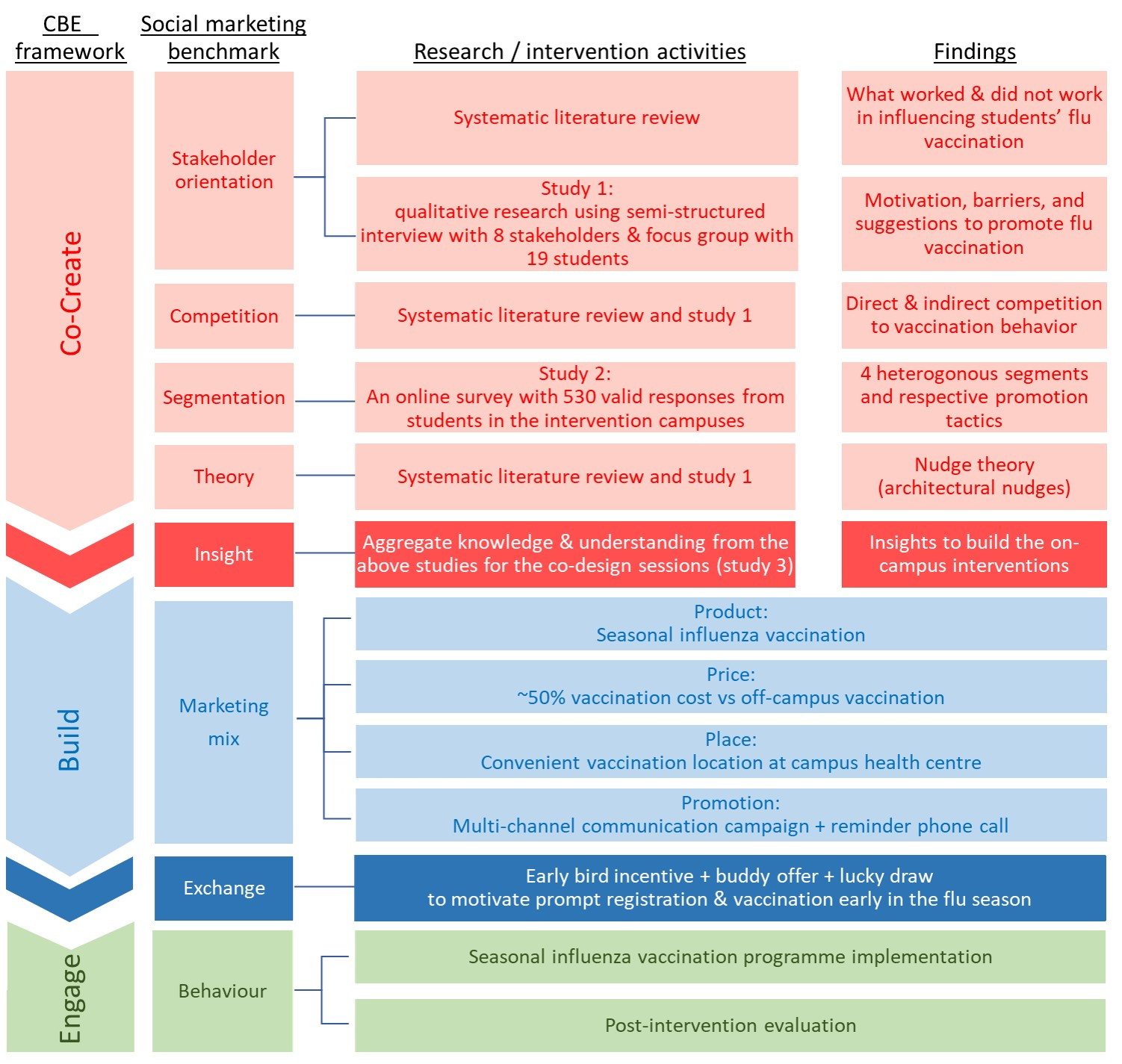
Figure 1 visualises the study design.
2.2.1. Co-Creation
The first step of the CBE process is co-creation. As the name co-creation literally implies, the essence of a social marketing campaign is that the programme should be designed “together with” the target group instead of solely by experts or researchers who then feed the planned intervention to the target group. A deep understanding of the target group should be acquired through listening and learning from the people we are targeting and the other concerned parties surrounding the target audience group [
14]. This listening and learning process involves four of the eight social marketing benchmark criteria: stakeholder orientation, competition, segmentation, and theory. The understanding gained from this process generates insights for the programme design, fulfilling the fifth benchmark criteria. To achieve the aforementioned, a systematic review of the literature and three studies (study 1—a qualitative study including stakeholder interviews and student focus groups; study 2—a quantitative segmentation study; and study 3—co-design sessions with students) were carried out.
Stakeholder Orientation
Upon completion of a systematic review of the literature and meta-analysis of previous flu vaccination programmes on university students, study 1 was developed as a qualitative study including semi-structured interviews with major stakeholders and focus groups with students. An interview protocol was developed based on the systematic literature review [
8] to explore the knowledge, attitudes, and behaviours of students towards influenza vaccination, along with possible motivation, barriers, and suggestions for future on-campus flu vaccination promotion. Eight people who were heavily involved in the planning, implementation, and administration of on-campus flu vaccination programs were invited to participate in stakeholder interviews. Interviewees included one health centre director, three staff, two student affairs officers who support the campus health centre to disseminate vaccination promotion materials, and two school managers who oversee health centre service quality. Moreover, 6 online focus groups were conducted with 19 students.
Competition
Competition to the flu vaccination behaviour was identified from the systematic literature review and qualitative research in study 1. The direct competition was primarily off-campus flu vaccinations provided by private clinics located near students’ homes which operate with more flexible hours. However, the flu vaccine price at private clinics is usually much more expensive than the on-campus option. The indirect competition was comprised of activities such as exercises that are perceived to enhance one’s immunization and these may be considered as a substitution to vaccination.
Segmentation
Study 2 was a segmentation study. Audience segmentation is one of the critical parts of a social marketing campaign. Instead of presuming students from the same college are homogeneous, segmentation studies identify distinctive subsets and the common characteristics exhibited by each sub-set of students. Each segment demonstrates unique characteristics in terms of flu vaccination attitudes, involvement in decision-making, and behaviour. A divide-and-conquer approach can therefore be applied to tackle vaccine hesitancy in each segment, increasing the effectiveness of a behaviour intervention program.
Based on the interview with stakeholders (study 1), a self-administered online questionnaire survey was designed. Full-time students in the intervention campuses were recruited to participate through a school mass email featuring a description of the research project and a link to the survey four months before the vaccination programme was implemented on campus. A total of 530 valid responses were obtained for segmentation analysis. Data analysed included their past influenza vaccination behaviour, level of involvement in flu vaccination decisions, seasonal influenza-related information search behaviour, and their attention to influenza-related information. According to this segmentation study [
17], four heterogeneous segments were identified: (1) convinced, (2) informed unconvinced, (3) open to persuasion, and (4) disengaged sceptics. The “convinced” segment consists of students who are highly receptive to seasonal influenza vaccine programmes and who were planning to receive flu vaccines in the coming flu season. The “open to persuasion” segment featured students who are indifferent to seasonal influenza and flu vaccination. They do not actively search for influenza-related information, but they still pay high attention when they are exposed to such information. Students among the “informed unconvinced” segment have the highest attention to influenza-related information and are characterised by their active searching of such information but they are not necessarily convinced they should receive vaccinations. Lastly, unlike students from the previous three segments, some students see vaccination as unimportant and unnecessary. They have never received flu vaccinations, they do not search for influenza-related information, and they pay little attention even if they are exposed to such information. These students belong to the “disengaged sceptics” segment. The segmentation study revealed that nearly half of the students are receptive to flu vaccination with “convinced” and “open to persuasion” segments comprising 9% and 40% of the student population, respectively. The remaining 51% of students have strong flu vaccine hesitancy and they may refuse to uptake flu vaccines voluntarily.
Theory
Theory application is a core element in social marketing as it enables social marketers to gain a deeper understanding of their audience and design interventions according to the theory, thereby bridging the intention-behaviour gap in vaccine uptake [
18,
19]. According to the systematic literature review [
8] and qualitative study with students, incentives were indicated as a mechanism that could be used to nudge students to receive flu vaccines. Thus, this flu vaccination intervention programme was developed using the nudge theory. While education nudges are found to be less effective, architectural nudges were embedded in programme design to enhance salience and simplify vaccination decision-making, registration, and behavioural action.
Insight
Through the systematic review [
8], qualitative, and segmentation studies [
17] the following major insights were acquired, which guided the co-design of the social marketing programme with students.
The “informed unconvinced” and “disengaged sceptics” held strong disbelief in the necessity of preventing flu complications through vaccination, indicating these groups would not be motivated to receive a flu vaccine by an intervention program.
Receptive audiences who are “convinced” or “open to persuasion” usually respond to vaccination programs promptly at the beginning of the flu season as soon as they are exposed or reminded to get vaccinated. Thus, a short one to two months vaccination promotion programme will serve the needs of these segment groups. Interventions that last for a few months are intended to remind those who have not been vaccinated in the first 1 to 2 months to act, and this was indicated as an approach that would have minimal effect on increasing vaccination rates.
For the other segments who have stronger vaccine acceptance, architectural nudges including free vaccines, incentives to receive vaccinations, and convenience—including simplifying registration and vaccination processes—would support increases in vaccination rates. Non-monetary nudges were indicated as being ineffective.
Multi-channel promotion that exposes students to the vaccination programme at all possible on-campus touch points is needed.
Visual design of the promotion communication should cut through the clutter to attract students’ attention as students are bombarded with piles of information across all of the school’s communication channels.
Peer and parental influence work better than healthcare professionals in influencing vaccination decisions.
Post-registration reminders are needed to reinforce vaccination behaviour.
While students are exposed to a pile of COVID-19 vaccine information during the pandemic, some students were concerned about the co-administration of COVID-19 and flu vaccines. Hence, the provision of information about the co-administration of these vaccines is required. Communication channels such as the university website, learning portal, and emails are expected to be more effective in reaching students.
Although these insights enable the research team to design an effective vaccination programme, a great uncertainty will remain regarding whether the interventions could effectively engage the students if the programme is solely designed by researchers. Co-design has therefore been employed in this study to involve individuals from the target audience in the designing of strategies and interventions which would be endorsed by the students themselves. Co-design ensured programme design goes beyond the researchers’ limited imagination and incorporates the students’ innovative ideas.
Considering the fundamental differences in the needs and wants of students between different segments [
17], not a one-size-fits-all approach but a divide-and-conquer approach could maximise the size of audience that our vaccination programme could effectively engage with. According to insight #1, our programme targeted segments who are receptive to vaccination, aiming to remind and reinforce intention and activate vaccination behaviour. Student segments who are “disengaged sceptics” about flu vaccination were excluded. Our segmentation study has found that most students from this segment have expressed no intention to be vaccinated for the coming season and would not be motivated to do otherwise by any of the tested messages [
17]. In addition, previous flu vaccination interventions have found that vaccination rates could be significantly increased by closing the intention–behaviour gap among those who are already willing to be vaccinated [
8]. Consequently, the strategy of this social marketing programme prioritized promotion efforts across three segments to normalise vaccination among them so that the “disengaged sceptics” might consider vaccination in future intervention periods as vaccine uptake is more normalised.
Two co-design sessions were conducted with students recruited from the intervention campuses. A total of 15 students were recruited, composed of 8 male and 7 female students. The first co-design session consisted of 10 students belonging to the “low involvement, open to persuasion” segment, which was the largest segment identified from the segmentation study [
17]. The second session consisted of 3 students from the “convinced” segment and 2 from the “informed unconvinced” segment. Flu vaccination is considered a high involvement decision among these two segments. Each co-design session lasted for 1.5 h, consisting of four parts. In the first two parts, students were asked to write down their barriers to vaccination and to identify what could motivate them to be vaccinated, respectively. In the third part, students were invited to break into smaller groups to brainstorm a few promotion messages among themselves, and then design the key promotion visuals. Afterwards, they voted for the most appealing one among the items their fellow schoolmates have created. Next, students brainstormed a few email subjects for the vaccination programme before they voted for the most eye-catching one.
The insights generated in the “co-create” step would become the backbone for the next step “build” of the CBE process.
2.2.2. Build
In the second step of the CBE process, the social marketing programme is built based on the insights gained previously and applies the sixth social marketing benchmark criteria—marketing mix. Commonly known as the “4 Ps” in commercial marketing, the marketing mix is composed of product, price, place, and promotion. Social marketing is more than simply communicating to motivate people. When applied to its fullest extent social marketing seeks to build a new solution which takes account of all the elements in the marketing mix offering additional choices to people [
14]. The offered choice should be presented to the people such that the desired behaviour has higher perceived benefits than costs. In that case, exchange (the seventh social marketing benchmark criteria) would take place.
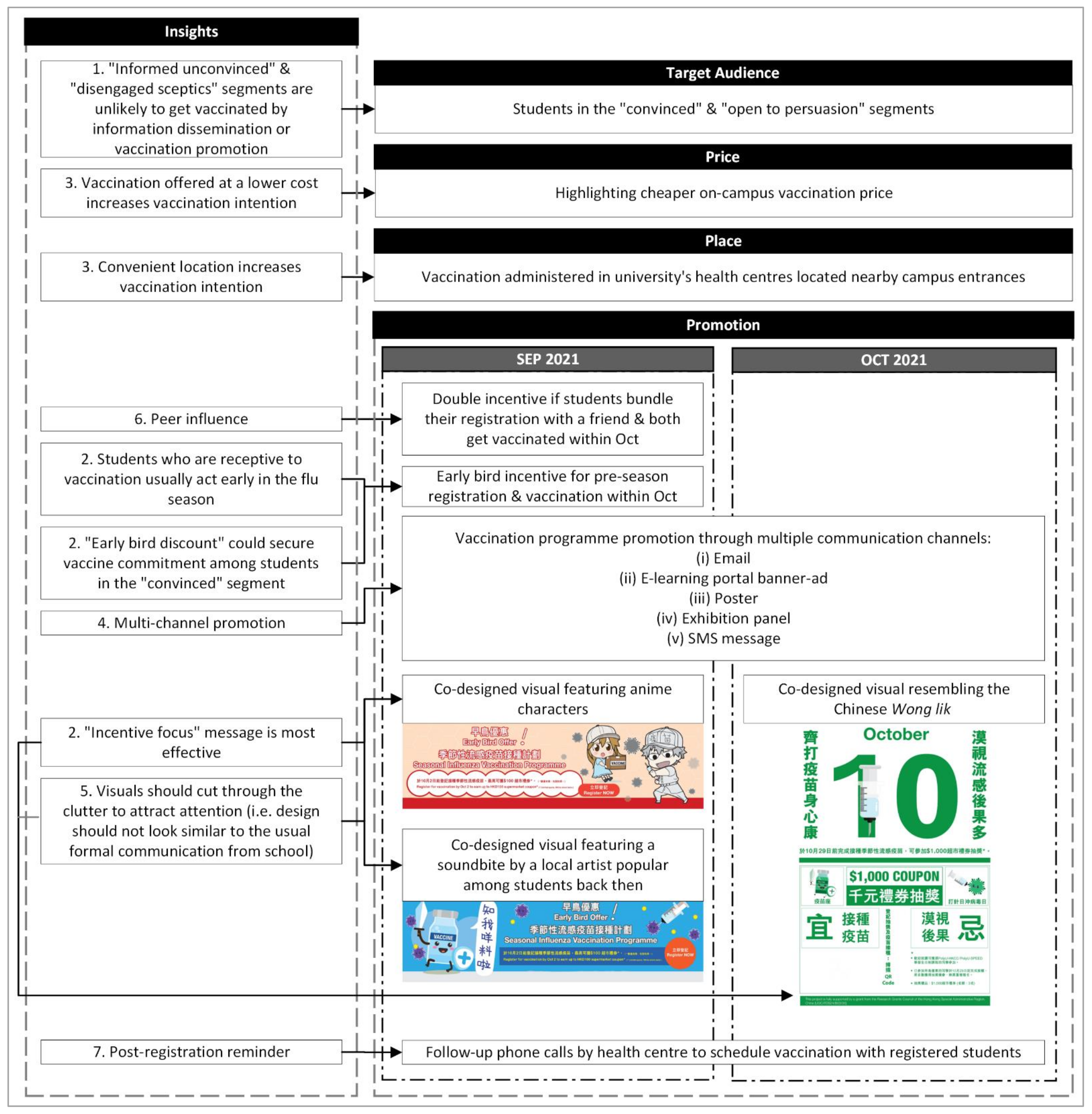
Figure 2 illustrates how the marketing-mix in this vaccination programme was built from the insights identified and listed in Section Insight above.
Marketing-Mix: Product
The product in this social marketing vaccination programme is the seasonal influenza vaccine. Based on the insights identified, a vaccine from a trustworthy country of origin is crucial even to those who are receptive to flu vaccination. Despite the availability of a newer administration method (i.e., intranasal administration), this campaign would only provide intramuscular injection following the university’s practice.
Marketing-Mix: Price
The vaccination service is provided through the on-campus health centres. The service is subsidised by the university so the vaccination price for students would be 50% less than off-campus vaccination. However, students reported in the focus groups that they were not aware of the lower price of vaccination services on campus. According to insight #3, the cost of the flu vaccine is an important factor influencing vaccination decisions. The programme prominently highlighted the price information on communications.
Marketing-Mix: Place
Within both intervention campuses, the health centres are located in a prominent location easily accessed by students en route to other campus facilities. According to insight #3, it is found that studies succeeded in promoting vaccination uptake by providing the service in easily accessible locations where the target group could conveniently visit (e.g., mobile clinics). The location where students could receive their vaccination in this programme should therefore be convenient enough as they could always visit the health centre on their way to class, before they left, or whenever they are free between classes. Moreover, students will prioritize other school activities over vaccination so the availability of vaccination services at a time convenient to students is also detrimental. In this programme, health centres will pre-arrange a timeslot convenient to the students while they call and confirm the vaccination service with those who have registered.
Exchange
Prior interventions have found that tangible exchange in the form of an incentive is highly effective in maximising the benefits of flu vaccination (insight #3). Moreover, according to insight #6, peer influence is also effective in motivating flu vaccination among students. In this social marketing programme, three types of incentives were utilised to motivate students to engage in vaccination behaviour early in the flu season.
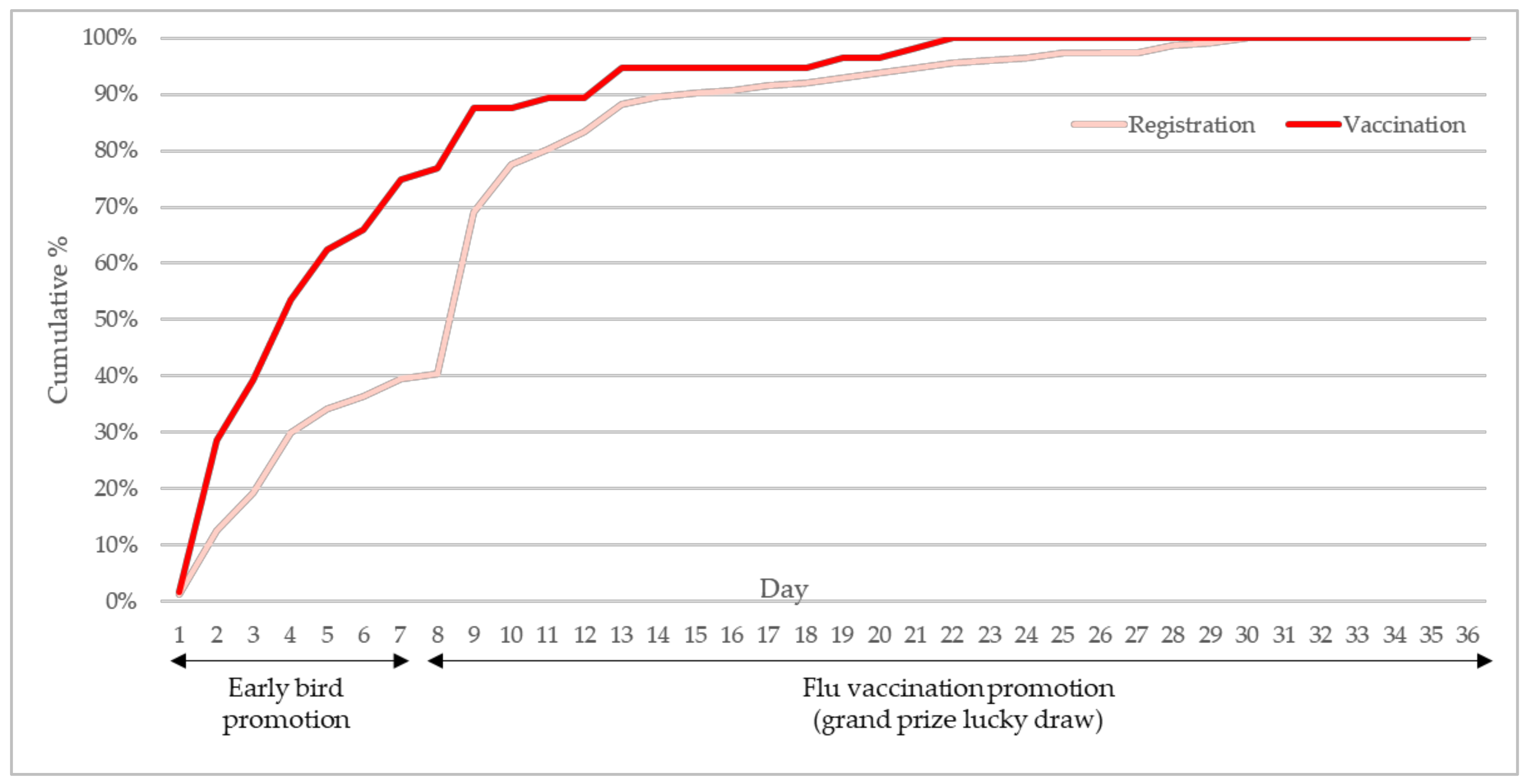
First, an early bird incentive of HKD50 was offered to students who registered for flu vaccination one week before the availability of the flu vaccine. The early bird incentive reduced the actual cost of receiving the vaccine by about 30%. The early bird promotion aimed to secure vaccination commitment among the “convinced” segment of students who have planned to get vaccinated [
17].
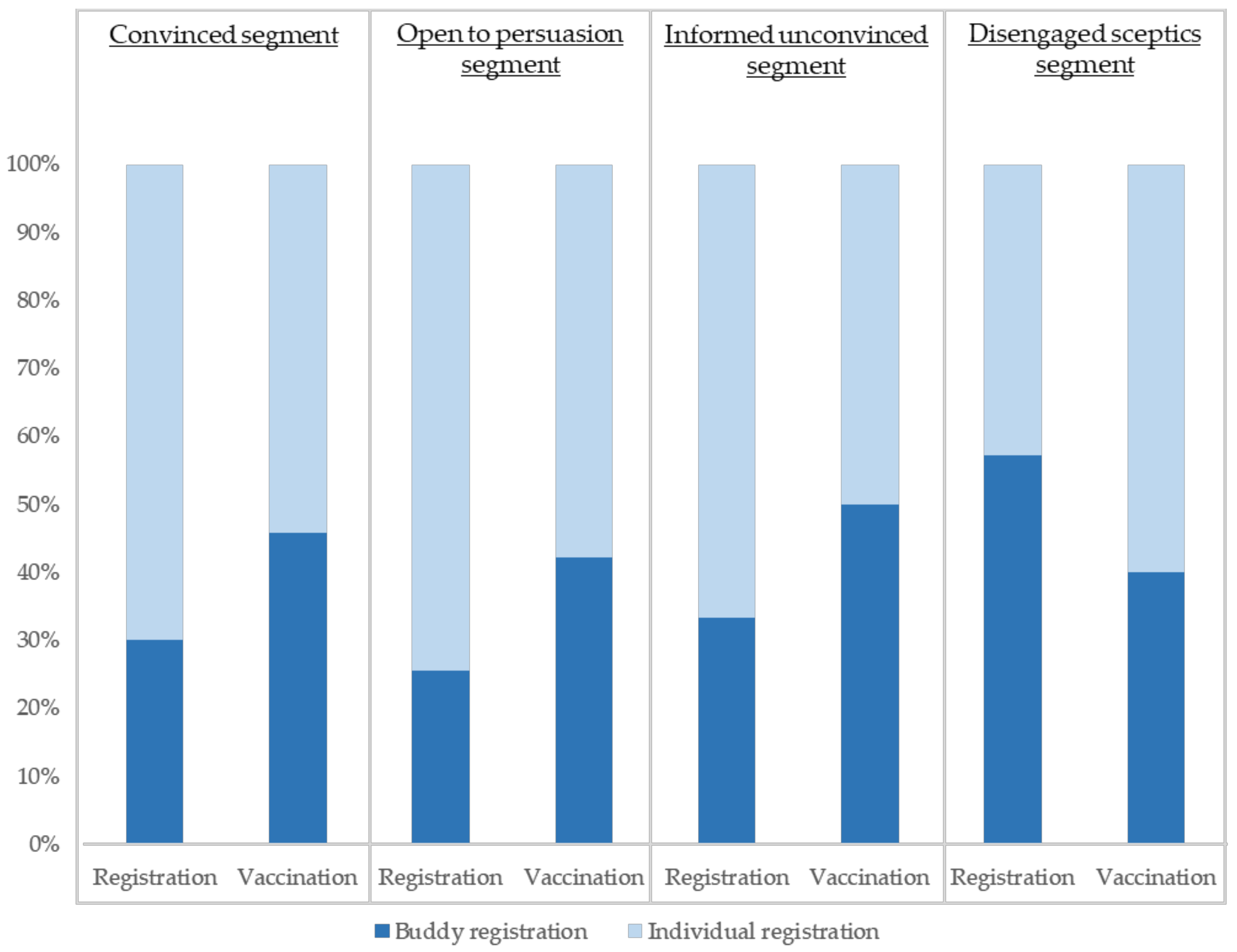
Second, apart from individual registration, students could also register with their friends to obtain an additional buddy offer of HKD50. The early bird and buddy provided a vaccine cost reduction of 55% for each student who registered with a friend within the early bird promotion week.
Third, throughout October 2021 since the start of seasonal flu vaccination services at campus health centres (the second phase of this programme), students registered to be vaccinated could sign up for a lucky draw. Meanwhile, students who had registered for the early bird offer during the first phase were automatically signed up for the lucky draw. The lucky draw prizes were HKD1000 cash coupons (valued at about 6 times the vaccine cost).
To successfully bridge the intention-behaviour gap in health behaviour, students would have to receive the flu vaccine at campus health centres by the end of October to be eligible for receiving any of the early bird incentives, buddy offers, and/or lucky draw prizes. According to insight #7, a booking reminder is important to follow through with students from registration to vaccination.
2.2.3. Engage
The final step of the CBE process was to engage the target group on a full scale with the implementation of the social marketing programme. The awareness of the new solutions built in the previous step has to be broadly raised among the target group and the programme would keep reminding them about the availability of the programme and motivate them to consciously undergo the behaviour change [
14].
Implementation
While on-campus vaccination services are available throughout the full seasonal flu season (October 2021 to March 2022), this intervention programme was implemented for 5 weeks from the end of September to the end of October 2021. According to insight #2, those who have strong vaccine acceptance will act early to achieve immunity at the beginning of the flu season. This intervention programme was implemented for 5 weeks in two phases:
Phase 1—one week at the end of September 2021 before the start of vaccine administration as an early bird promotion.
Phase 2—four weeks in October 2021 from the start date of the vaccination administration service at campus health centres.
To compare the effectiveness of visuals using popular cartoon characters and health-related graphics with popular slang, the following treatment was arranged in phase one. First- and second-year students received an email and were exposed to the Moodle banner ad with the first design for the early bird offer on the first day of the promotion and those with the second design a few days later. Senior years students received emails and were shown the Moodle banner ad with visuals in reverse order. Other promotion materials featuring both designs were displayed throughout the week, including printed A2-size posters in lifts and major hallways where students were passing through frequently, and full-height exhibition panels located at major access points to the campus. SMS containing the text promotion message was also broadcasted to students to remind them of the programme.
During the second phase, promotion materials were sent to the student within the days after the commencement. Throughout the rest of October, promotion materials were visible to students physically on campus as posters and exhibition panels, and virtually as banner ads on the e-learning portal and emails.
Data Collection and Evaluation
This last step of the CBE process is an evaluation of the implemented programme to identify key success factors and key learnings for the enhancement of future programmes to sustain the behaviour change. Besides the actual vaccination rate, the interaction between students and the promotional tools was monitored so that it could be evaluated to learn whether the programme could maximise its reach with the resources available to create the conditions in favour of the desired behaviour change [
14].
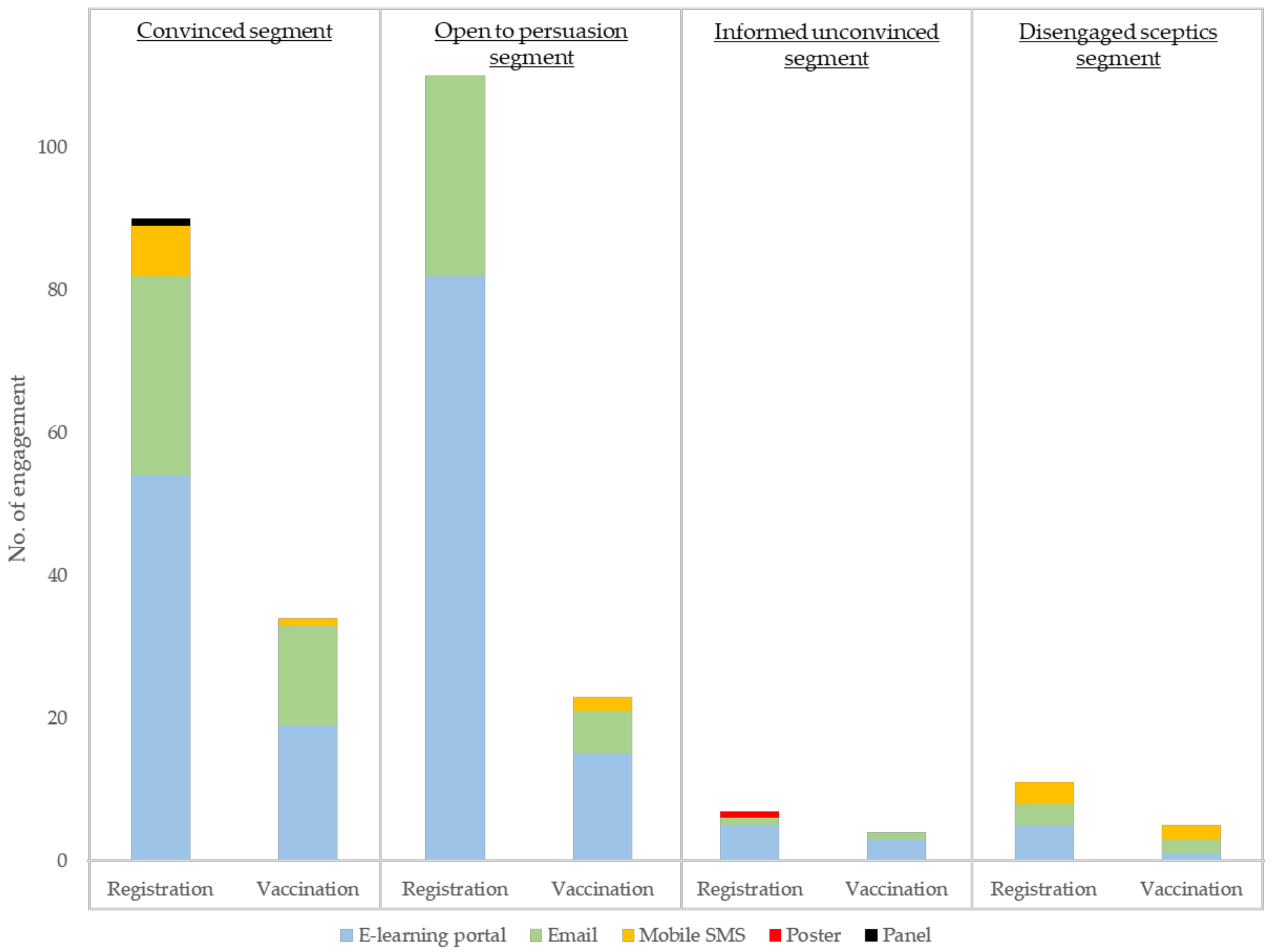
Vaccination numbers were collected from the health centres of both the intervention and control campuses. Health centres also shared the vaccination rate from the previous three years for baseline comparison. QR codes or hyperlinks to access the registration page were assigned to each promotional material, permitting comparisons between communication approaches in the post-campaign evaluation. Students who received their vaccination would be tracked back to see which design successfully motivated them. Similarly, the effectiveness of each promotion channel could also be evaluated. After the intervention programme, students who had participated in either the early bird offer or the lucky draw programme and received vaccination were invited to attend one of the three post-intervention focus groups to understand: (i) students’ unaided recall of promotion materials; (ii) aided awareness of promotion materials; (iii) whether each design had gained their awareness, changed their attitude, intention, and behaviour for vaccination; (iv) why or why not they got vaccinated after registration; and lastly (v) any comments, suggestions, or observations for programme improvement.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}