
Determinants of COVID-19 Vaccination Intention among Health Care Workers in France: A Qualitative Study
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
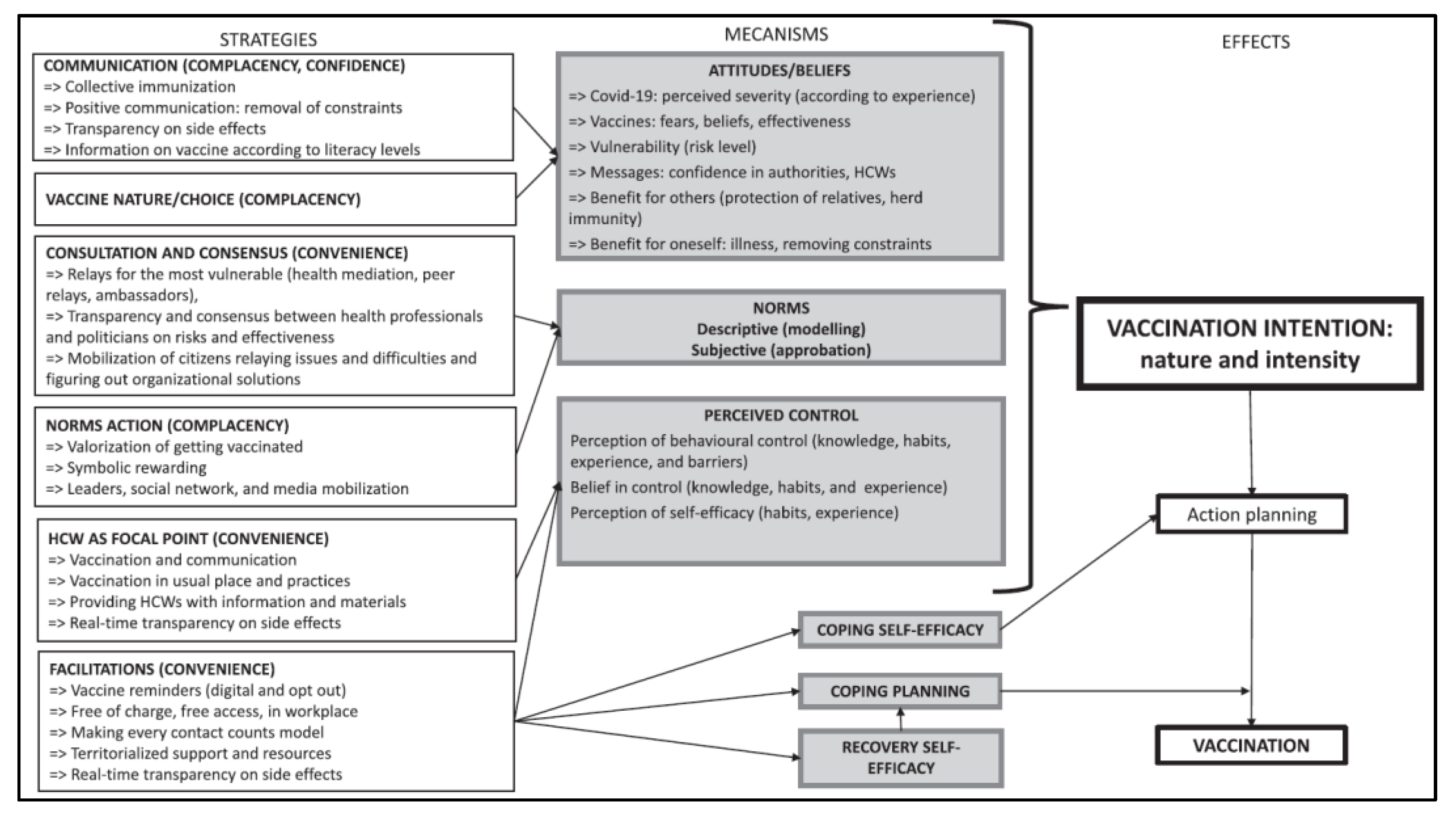
2.2. Comprehensive Behavioral Model of Pandemic Vaccination
2.3. Corpus Recruitment
2.4. Data Collection
2.5. Data Processing and Analysis
3. Results
3.1. Description of the Population
3.2. Determinants of COVID-19 Vaccination Intention
3.2.1. Confidence in the Vaccines Being Offered
3.2.2. Experience Effect
3.2.3. The Opinions and Immunization Status of Others
3.2.4. Media Influence on Public Opinion
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kiem, C.T.; Massonnaud, C.R.; Levy-Bruhl, D.; Poletto, C.; Colizza, V.; Bosetti, P.; Fontanet, A.; Gabet, A.; Olié, V.; Zanetti, L.; et al. A modelling study investigating short and medium-term challenges for COVID-19 vaccination: From prioritisation to the relaxation of measures. EClinicalMedicine 2021, 38, 101001. [Google Scholar] [CrossRef] [PubMed]
- Fontanet, A.; Cauchemez, S. COVID-19 herd immunity: Where are we? Nat. Rev. Immunol. 2020, 20, 583–584. [Google Scholar] [CrossRef] [PubMed]
- Coelho, F.C.; Lana, R.M.; Cruz, O.G.; Villela, D.A.M.; Bastos, L.S.; Pastore YPiontti, A.; Davis, J.T.; Vespignani, A.; Codeço, C.T.; Gomes, M.F.C. Assessing the spread of COVID-19 in Brazil: Mobility, morbidity and social vulnerability. PLoS ONE 2020, 15, e0238214. [Google Scholar] [CrossRef] [PubMed]
- Haute Autorité de Santé. Stratégie de vaccination contre le SARS-CoV-2-Recommandations préliminaires sur la stratégie de priorisation des populations à vacciner. Haute Autorité de Santé. 2020. Available online: https://www.has-sante.fr/jcms/p_3221338/fr/strategie-de-vaccination-contre-le-sars-cov-2-recommandations-preliminaires-sur-la-strategie-de-priorisation-des-populations-a-vacciner (accessed on 29 September 2022).
- Santé Publique France. COVID-19: Point épidémiologique du 18 février 2021. 2021. Available online: https://www.santepubliquefrance.fr/maladies-et-traumatismes/maladies-et-infections-respiratoires/infection-a-coronavirus/documents/bulletin-national/covid-19-point-epidemiologique-du-18-fevrier-2021 (accessed on 29 September 2022).
- Yaqub, O.; Castle-Clarke, S.; Sevdalis, N.; Chataway, J. Attitudes to vaccination: A critical review. Soc. Sci. Med. 2014, 112, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Schwarzinger, M.; Verger, P.; Guerville, M.A.; Aubry, C.; Rolland, S.; Obadia, Y.; Moatti, J.P. Positive attitudes of French general practitioners towards A/H1N1 influenza-pandemic vaccination: A missed opportunity to increase vaccination uptakes in the general public? Vaccine 2010, 28, 2743–2748. [Google Scholar] [CrossRef] [Green Version]
- MacDonald, N.E.; SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and Receptivity for COVID-19 Vaccines: A Rapid Systematic Review. Vaccines 2020, 9, 16. [Google Scholar] [CrossRef]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- Verger, P.; Fressard, L.; Collange, F.; Gautier, A.; Jestin, C.; Launay, O.; Raude, J.; Pulcine, C.; Peretti-Watel, P. Vaccine Hesitancy Among General Practitioners and Its Determinants During Controversies: A National Cross-sectional Survey in France. EBioMedicine 2015, 2, 891–897. [Google Scholar] [CrossRef] [Green Version]
- Machingaidze, S.; Wiysonge, C.S. Understanding COVID-19 vaccine hesitancy. Nat. Med. 2021, 27, 1338–1339. [Google Scholar] [CrossRef]
- Rosen, B.; Waitzberg, R.; Israeli, A.; Hartal, M.; Davidovitch, N. Addressing vaccine hesitancy and access barriers to achieve persistent progress in Israel’s COVID-19 vaccination program. Isr. J. Health Policy Res. 2021, 10, 43. [Google Scholar] [CrossRef] [PubMed]
- Detoc, M.; Bruel, S.; Frappe, P.; Tardy, B.; Botelho-Nevers, E.; Gagneux-Brunon, A. Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. Vaccine 2020, 38, 7002–7006. [Google Scholar] [CrossRef] [PubMed]
- Jarrett, C.; Wilson, R.; O’Leary, M.; Eckersberger, E.; Larson, H.J.; SAGE Working Group on Vaccine Hesitancy. Strategies for addressing vaccine hesitancy-A systematic review. Vaccine 2015, 33, 4180–4190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cambon, L.; Schwarzinger, M.; Alla, F. Increasing acceptance of a vaccination program for coronavirus disease 2019 in France: A challenge for one of the world’s most vaccine-hesitant countries. Vaccine 2022, 40, 178–182. [Google Scholar] [CrossRef]
- Schwarzinger, M.; Watson, V.; Arwidson, P.; Alla, F.; Luchini, S. COVID-19 vaccine hesitancy in a representative working-age population in France: A survey experiment based on vaccine characteristics. Lancet Public Health. 2021, 6, e210–e221. [Google Scholar] [CrossRef]
- Xiao, X.; Wong, R.M. Vaccine hesitancy and perceived behavioral control: A meta-analysis. Vaccine. 2020, 38, 5131–5138. [Google Scholar] [CrossRef]
- Schmid, P.; Rauber, D.; Betsch, C.; Lidolt, G.; Denker, M.L. Barriers of Influenza Vaccination Intention and Behavior-A Systematic Review of Influenza Vaccine Hesitancy, 2005–2016. PLoS ONE 2017, 12, e0170550. [Google Scholar]
- Schwarzinger, M.; Flicoteaux, R.; Cortarenoda, S.; Obadia, Y.; Moatti, J.P. Low acceptability of A/H1N1 pandemic vaccination in French adult population: Did public health policy fuel public dissonance? PLoS ONE 2010, 5, e10199. [Google Scholar] [CrossRef]
- Bish, A.; Yardley, L.; Nicoll, A.; Michie, S. Factors associated with uptake of vaccination against pandemic influenza: A systematic review. Vaccine 2011, 29, 6472–6484. [Google Scholar] [CrossRef]
- Bone, A.; Guthmann, J.P.; Nicolau, J.; Lévy-Bruhl, D. Population and risk group uptake of H1N1 influenza vaccine in mainland France 2009–2010: Results of a national vaccination campaign. Vaccine 2010, 28, 8157–8161. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Achtziger, A.; Gollwitzer, P.M. Motivation and Volition in the Course of Action. In Motivation and Action; Heckhausen, J., Heckhausen, H., Eds.; Springer: Berlin/Heidelberg, Germany, 2018; pp. 485–527. [Google Scholar] [CrossRef] [Green Version]
- Rosenstock, I.M. Historical Origins of the Health Belief Model. Health Educ. Monographs. 1974, 2, 328–335. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychologist. 2000, 55, 68–78. [Google Scholar] [CrossRef]
- Balard, F.; Kivits, J.; Schrecker, C.; Voléry, I. L’analyse qualitative en santé. In Les Recherches Qualitatives en Santé [Internet]; Arman. Colin, 2016; pp. 167–185. Available online: https://www.cairn.info/les-recherches-qualitatives-en-sante--9782200611897-p-167.htm (accessed on 29 September 2022).
- Hara, M.; Ishibashi, M.; Nakane, A.; Nakano, T.; Hirota, Y. Differences in COVID-19 Vaccine Acceptance, Hesitancy, and Confidence between Healthcare Workers and the General Population in Japan. Vaccines 2021, 9, 1389. [Google Scholar] [CrossRef]
- Aw, J.; Seng, J.J.B.; Seah, S.S.Y.; Low, L.L. COVID-19 Vaccine Hesitancy—A Scoping Review of Literature in High-Income Countries. Vaccines 2021, 9, 900. [Google Scholar] [CrossRef] [PubMed]
- Baccolini, V.; Renzi, E.; Isonne, C.; Migliara, G.; Massimi, A.; De Vito, C.; Marzuillo, C.; Villari, P. COVID-19 Vaccine Hesitancy among Italian University Students: A Cross-Sectional Survey during the First Months of the Vaccination Campaign. Vaccines 2021, 9, 1292. [Google Scholar] [CrossRef]
- Walsh, J.C.; Comar, M.; Folan, J.; Williams, S.; Kola-Palmer, S. The psychological and behavioural correlates of COVID-19 vaccine hesitancy and resistance in Ireland and the UK. Acta Psychol. 2022, 225, 103550. [Google Scholar] [CrossRef]
- Askarian, M.; Semenov, A.; Llopis, F.; Rubulotta, F.; Dragovac, G.; Pshenichnaya, N.; Assadian, O.; Ruch, Y.; Shayan, Z.; Padilla Fortunatti, C.; et al. The COVID-19 Vaccination Acceptance/Hesitancy Rate and Its Determinants among Healthcare Workers of 91 Countries: A Multicenter Cross-Sectional Study. EXCLI. 2022. Available online: https://www.excli.de/index.php/excli/article/view/4439 (accessed on 29 September 2022).
- Betsch, C.; Böhm, R. Detrimental effects of introducing partial compulsory vaccination: Experimental evidence. Eur. J. Public Health 2016, 26, 378–381. [Google Scholar] [CrossRef] [Green Version]
- Soares, P.; Rocha, J.V.; Moniz, M.; Gama, A.; Laires, P.A.; Pedro, A.R.; Dias, S.; Leite, A.; Numes, C. Factors Associated with COVID-19 Vaccine Hesitancy. Vaccines 2021, 9, 300. [Google Scholar] [CrossRef]
- Larson, H.J.; de Figueiredo, A.; Xiahong, Z.; Schulz, W.S.; Verger, P.; Johnston, I.G.; Cook, A.R.; Jones, N.S. The State of Vaccine Confidence 2016: Global Insights Through a 67-Country Survey. EBioMedicine 2016, 12, 295–301. [Google Scholar] [CrossRef]
- Paris, C.; Bénézit, F.; Geslin, M.; Polard, E.; Baldeyrou, M.; Turmel, V.; Tadié, E.; Garlantezec, R.; Tattevin, P. COVID-19 vaccine hesitancy among healthcare workers. Infect. Dis. Now. 2021, 51, 484–487. [Google Scholar] [CrossRef] [PubMed]
- Paul, E.; Brown, G.W.; Ridde, V. COVID-19: Time for paradigm shift in the nexus between local, national and global health. BMJ Glob. Health. 2020, 5, e002622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Black, S.; Rappuoli, R. A crisis of public confidence in vaccines. Sci. Transl. Med. 2010, 2, 61mr1. [Google Scholar] [CrossRef] [PubMed]
- Paterson, P.; Meurice, F.; Stanberry, L.R.; Glismann, S.; Rosenthal, S.L.; Larson, H.J. Vaccine hesitancy and healthcare providers. Vaccine 2016, 34, 6700–6706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karafillakis, E.; Dinca, I.; Apfel, F.; Cecconi, S.; Wűrz, A.; Takacs, J.; Suc, J.; Pastore Celentano, L.; Kramarz, P.; Larson, H.J. Vaccine hesitancy among healthcare workers in Europe: A qualitative study. Vaccine 2016, 34, 5013–5020. [Google Scholar] [CrossRef]
- Pal, S.; Shekhar, R.; Kottewar, S.; Upadhyay, S.; Singh, M.; Pathak, D.; Kapuria, D.; Barrett, E.; Sheil, A.B. COVID-19 Vaccine Hesitancy and Attitude toward Booster Doses among US Healthcare Workers. Vaccines 2021, 9, 1358. [Google Scholar] [CrossRef]
- Gagneux-Brunon, A.; Detoc, M.; Bruel, S.; Tardy, B.; Rozaire, O.; Frappe, P.; Botelho-Nebers, E. Intention to get vaccinations against COVID-19 in French healthcare workers during the first pandemic wave: A cross-sectional survey. J. Hosp. Infect. 2021, 108, 168–173. [Google Scholar] [CrossRef]
- Biswas, N.; Mustapha, T.; Khubchandani, J.; Price, J.H. The Nature and Extent of COVID-19 Vaccination Hesitancy in Healthcare Workers. J. Community Health 2021, 46, 1244–1251. [Google Scholar] [CrossRef]
- Ciardi, F.; Menon, V.; Jensen, J.L.; Shariff, M.A.; Pillai, A.; Venugopal, U.; Kasubhai, M.; Dimitrov, V.; Kanna, B.; Poole, B.D. Knowledge, Attitudes and Perceptions of COVID-19 Vaccination among Healthcare Workers of an Inner-City Hospital in New York. Vaccines 2021, 9, 516. [Google Scholar] [CrossRef]
- Shim, E.; Chapman, G.; Townsend, J.; Galvani, A. The influence of altruism on influenza vaccination decisions. J. R. Soc. Interface 2012, 9, 2234–2243. [Google Scholar] [CrossRef]
- Burke, P.F.; Masters, D.; Massey, G. Enablers and barriers to COVID-19 vaccine uptake: An international study of perceptions and intentions. Vaccine 2021, 39, 5116–5128. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Hepatitis B Vaccination and Multiple Sclerosis (MS). 2002. Available online: https://www.who.int/groups/global-advisory-committee-on-vaccine-safety/topics/hepatitis-b-vaccines/multiple-sclerosis (accessed on 29 September 2022).
- Larson, H.J.; Cooper, L.Z.; Eskola, J.; Katz, S.L.; Ratzan, S. Addressing the vaccine confidence gap. Lancet. 2011, 378, 526–535. [Google Scholar] [CrossRef]
- Islam, M.S.; Sarkar, T.; Khan, S.H.; Mostofa Kamal, A.H.; Hasan, S.M.M.; Kabir, A.; Yeasmon, D.; Islam, M.A.; Chowdhury, K.; Anwar, K.S.; et al. COVID-19-Related Infodemic and Its Impact on Public Health: A Global Social Media Analysis. Am. J. Trop Med. Hyg. 2020, 103, 1621–1629. [Google Scholar] [CrossRef] [PubMed]
- Roozenbeek, J.; Schneider, C.R.; Dryhurst, S.; Kerr, J.; Freeman, A.L.J.; Recchia, G.; Van der Bles, A.M.; Van der Linden, S. Susceptibility to misinformation about COVID-19 around the world. R. Soc. Open Sci. 2020, 7, 201199. [Google Scholar] [CrossRef]
- Stahl, J.P.; Cohen, R.; Denis, F.; Gaudelus, J.; Martinot, A.; Lery, T.; Lepetit, H. The impact of the web and social networks on vaccination. New challenges and opportunities offered to fight against vaccine hesitancy. Med. Mal. Infect. 2016, 46, 117–122. [Google Scholar] [CrossRef]
- Ward, J.K.; Peretti-Watel, P.; Larson, H.J.; Raude, J.; Verger, P. Vaccine-criticism on the internet: New insights based on French-speaking websites. Vaccine 2015, 33, 1063–1070. [Google Scholar] [CrossRef] [Green Version]
- Betsch, C.; Brewer, N.T.; Brocard, P.; Davies, P.; Gaissmaier, W.; Haase, N.; Leask, J.; Renkewitz, F.; Renner, B.; Reyna, V.F.; et al. Opportunities and challenges of Web 2.0 for vaccination decisions. Vaccine 2012, 30, 3727–3733. [Google Scholar] [CrossRef] [Green Version]
- Goldstein, S.; MacDonald, N.E.; Guirguis, S.; SAGE Working Group on Vaccine Hesitancy. Health communication and vaccine hesitancy. Vaccine 2015, 33, 4212–4214. [Google Scholar] [CrossRef] [Green Version]
- LOI n 2021-1040 du 5 août 2021 Relative à la Gestion de la Crise Sanitaire. 2021. Available online: https://www.legifrance.gouv.fr/jorf/id/JORFTEXT000043909676 (accessed on 29 September 2022).
- Rimal, R.N.; Storey, J.D. Construction of Meaning during a Pandemic: The Forgotten Role of Social Norms. Health Commun. 2020, 35, 1732–1734. [Google Scholar] [CrossRef]
- Sparkman, G.; Walton, G.M. Dynamic Norms Promote Sustainable Behavior, Even if It Is Counternormative. Psychol Sci. 2017, 28, 1663–1674. [Google Scholar] [CrossRef]
- Iten, A.; Bonfillon, C.; Bouvard, T.; Siegrist, C.A.; Pittet, D. P039: A new method to assess compliance with measures to prevent nosocomial influenza transmission. Antimicrob. Resist. Infect. Control 2013, 2, 39. [Google Scholar] [CrossRef] [Green Version]
- Donzel Godinot, L.; Sicsic, J.; Lachatre, M.; Bouvet, E.; Abiteboul, D.; Rouveix, E.; Pellissier, G.; Raude Mueller, J.E. Quantifying preferences around vaccination against frequent, mild disease with risk for vulnerable persons: A discrete choice experiment among French hospital health care workers. Vaccine 2021, 39, 805–814. [Google Scholar] [CrossRef] [PubMed]
- Seanehia, J.; Treibich, C.; Holmberg, C.; Müller-Nordhorn, J.; Casin, V.; Raude JMueller, J.E. Quantifying population preferences around vaccination against severe but rare diseases: A conjoint analysis among French university students, 2016. Vaccine 2017, 35, 2676–2684. [Google Scholar] [CrossRef] [PubMed]
- Verelst, F.; Willem, L.; Kessels, R.; Beutels, P. Individual decisions to vaccinate one’s child or oneself: A discrete choice experiment rejecting free-riding motives. Soc. Sci. Med. 2018, 207, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Lindner-Pawłowicz, K.; Mydlikowska-Śmigórska, A.; Łampika, K.; Sobieszczańska, M. COVID-19 Vaccination Acceptance among Healthcare Workers and General Population at the Very Beginning of the National Vaccination Program in Poland: A Cross-Sectional, Exploratory Study. Vaccines 2022, 10, 66. [Google Scholar] [CrossRef] [PubMed]
- Hozé, N.; Paireau, J.; Lapidus, N.; Tran Kiem, C.; Salje, H.; Severi GTouvier, M.; Zins, M.; Lamballerie, X.; Lévy-Bruhl, D.; Carrat, F.; et al. Monitoring the proportion of the population infected by SARS-CoV-2 using age-stratified hospitalisation and serological data: A modelling study. Lancet Public Health 2021, 6, e408–e415. [Google Scholar] [CrossRef]
- Wang, J.; Ji, Q.; Dong, S.; Zhao, S.; Li, X.; Zhu, Q.; Long, S.; Zhang, J.; Jin, H. Factors Influencing Vaccine Hesitancy in China: A Qualitative Study. Vaccines 2021, 9, 1291. [Google Scholar] [CrossRef]
- Manby, L.; Dowrick, A.; Karia, A.; Maio, L.; Buck, C.; Singleton, G.; Lewis-Jackson, S.; Uddin, I.; Vanderslott, S.; Martin, S.; et al. Healthcare workers’ perceptions and attitudes towards the UK’s COVID-19 vaccination programme: A rapid qualitative appraisal. BMJ Open 2022, 12, e051775. [Google Scholar] [CrossRef]


{kind=link}
| Topics | Example of Questions and Reminders |
|---|---|
| General representations of vaccination | What do you think of vaccination in general? What is your relationship with vaccination in general? What about the influenza vaccine? |
| Knowledge of and attitudes to the available COVID-19 vaccines | What do you think of the COVID-19 vaccines being offered? How do you relate to these vaccines? |
| Vaccination intention for COVID-19 vaccines | Do you plan to get vaccinated in the coming months? Why/why not? What are the reasons, the advantages? If negative vaccination intention: What would make you change your mind? |
| Expectations of and obstacles to vaccination campaign | Could you tell me about the organization of the vaccination campaign? What are your expectations regarding the organization of this campaign? |
| Influence of peers and the context | What do your family/friends/work colleagues think about this vaccination? What does the vaccination of others mean to you? Can you tell me about your role in this vaccination campaign? What approach do you take with those around you? And with your patients? |
| Characteristics | N (%) | |
|---|---|---|
| Sex | ||
| Men | 9 (36) | |
| Women | 16 (64) | |
| Age | ||
| Under 50 years old | 16 (64) | |
| Over 50 years old | 5 (20) | |
| Unknown | 4 (16) | |
| Profession | ||
| Physician | 4 (16) | |
| Nurse | 4 (16) | |
| Healthcare assistant | 6 (24) | |
| Physiotherapist | 2 (8) | |
| Porter | 2 (8) | |
| Senior nurse | 1 (4) | |
| Administrative staff | 3 (12) | |
| Medico-technical and technical staff | 3 (12) | |
| Total | 25 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bourreau, C.; Baron, A.; Schwarzinger, M.; Alla, F.; Cambon, L.; Donzel Godinot, L.; CoVaMax Study Group. Determinants of COVID-19 Vaccination Intention among Health Care Workers in France: A Qualitative Study. Vaccines 2022, 10, 1661. https://doi.org/10.3390/vaccines10101661
Bourreau C, Baron A, Schwarzinger M, Alla F, Cambon L, Donzel Godinot L, CoVaMax Study Group. Determinants of COVID-19 Vaccination Intention among Health Care Workers in France: A Qualitative Study. Vaccines. 2022; 10(10):1661. https://doi.org/10.3390/vaccines10101661
Chicago/Turabian StyleBourreau, Coline, Angela Baron, Michaël Schwarzinger, François Alla, Linda Cambon, Léo Donzel Godinot, and CoVaMax Study Group. 2022. "Determinants of COVID-19 Vaccination Intention among Health Care Workers in France: A Qualitative Study" Vaccines 10, no. 10: 1661. https://doi.org/10.3390/vaccines10101661