
Tetanus Vaccination Status and Vaccine Hesitancy in Amateur Basketball Players (Italy, 2020)



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Questionnaire
2.2.1. Individual Characteristics
2.2.2. Potential Interactions with Tetanus and TeV
2.2.3. Interactions with a Physician
2.2.4. Risk Perception
2.2.5. Knowledge Test
2.2.6. Attitudes and Practices
2.3. Data Analysis
2.4. Ethical Considerations
3. Results
3.1. Descriptive Analysis: General Characteristics of the Sample
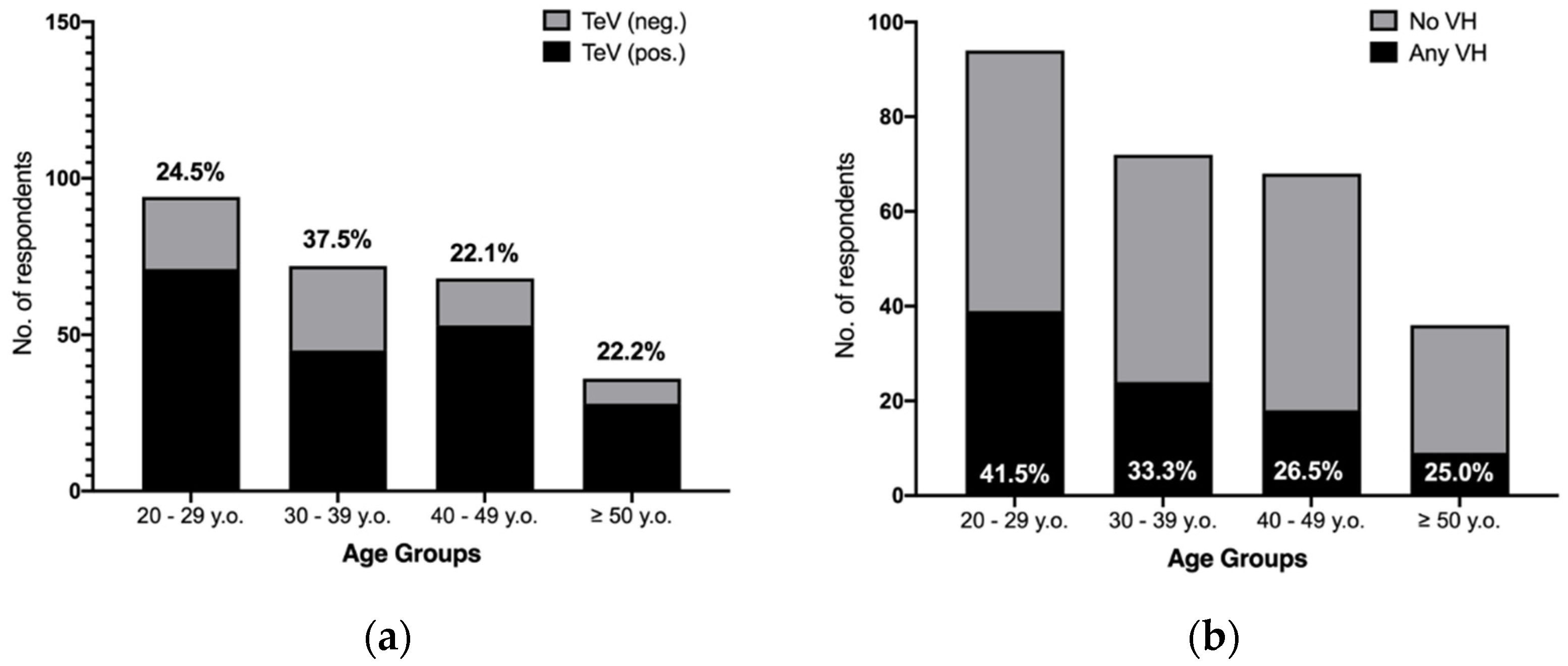
3.2. Previous and Potential Interactions with TeV
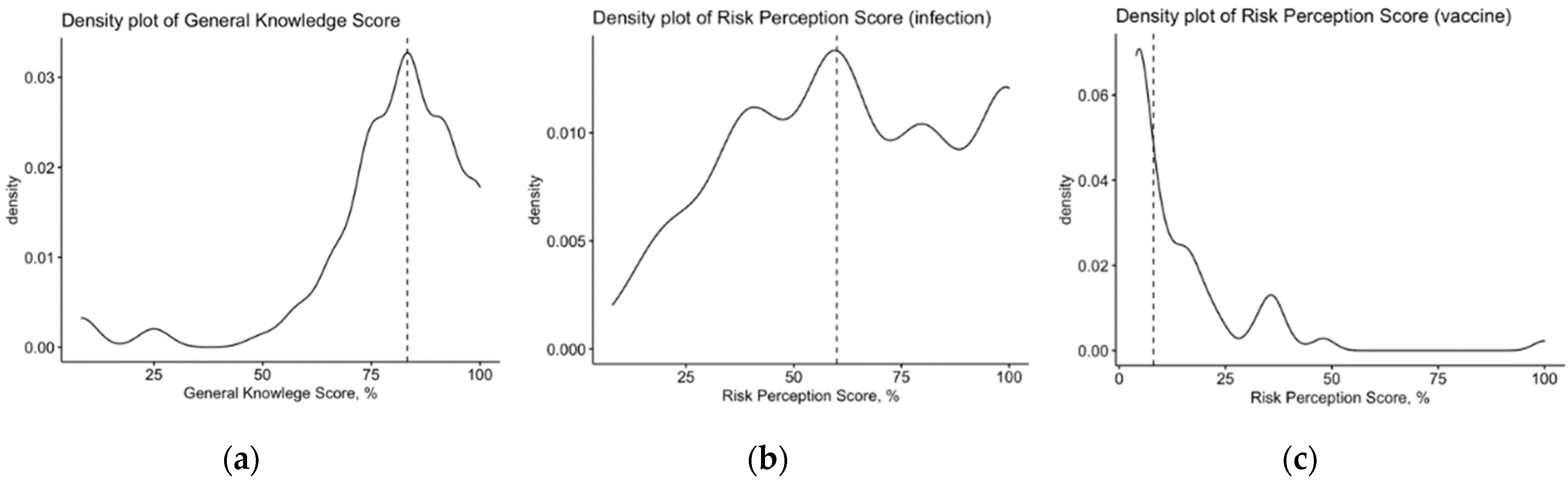
3.3. General Knowledge Test
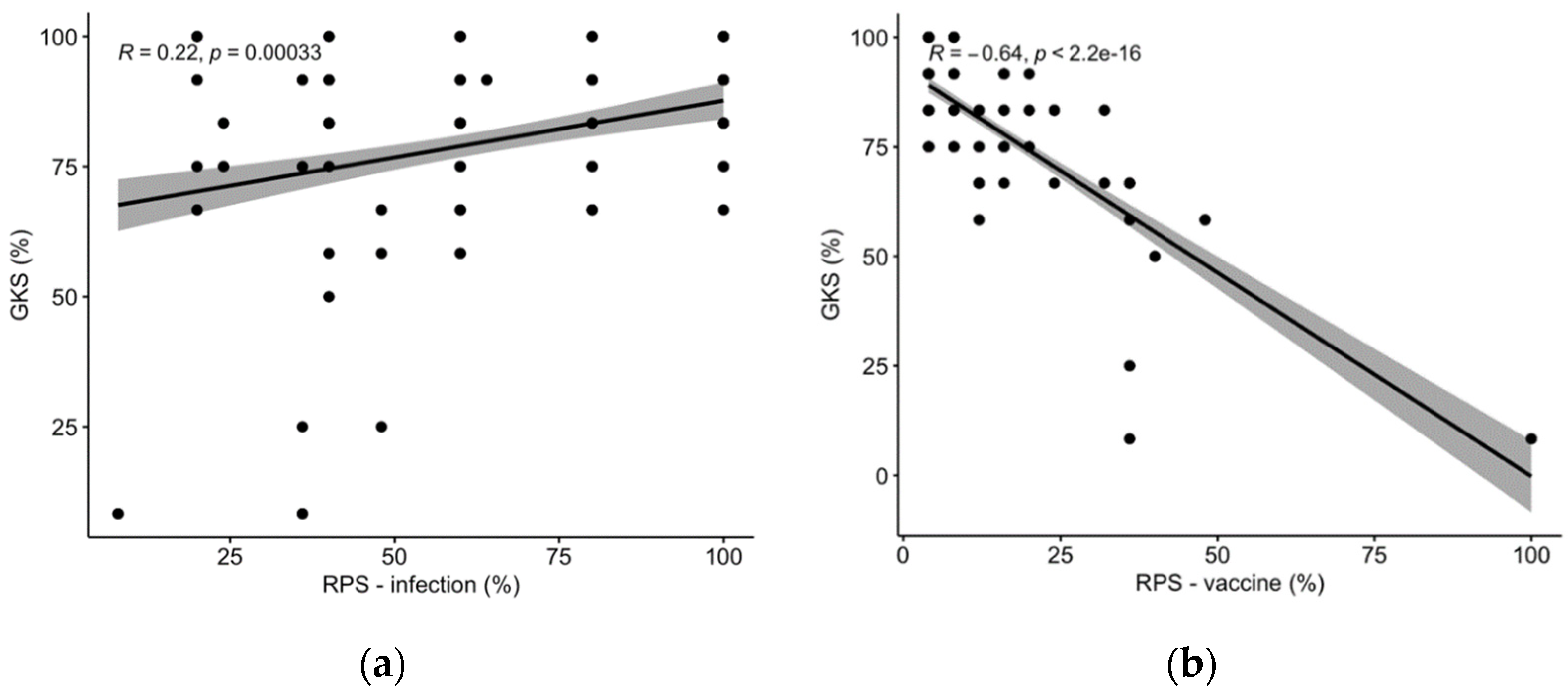
3.4. Risk Perception
3.5. Attitudes and Practices towards TeV
3.6. Univariate Analysis
3.7. Multivariable Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. English Translation of the Questionnaire
| V01 | Tetanus Basket | Authors’ translation |
| Estimated reader, We invite you to take a survey on your knowledge about, attitudes toward and practices regarding the tetanus vaccine. Our aim is to identify the main effectors and barriers towards tetanus vaccination to better understand which interventions may be useful and effective in improving vaccination rates in amateur athletes. This survey is completely voluntary. There are no negative consequences if you do not want to take it. If you start the survey, you can always change your mind and stop at any time. All information that is requested are defined in broad and generic terms, and all data will be handled anonymously. After the completion of the survey, there is no way to associate any questionnaire to any individual, as data such as email address or IP address (of the computer, smartphone, tablet, etc.) from the device employed to fill the questionnaire are neither requested nor collected according to the data-protection law. Regarding the individual data included in this questionnaire, we stress that only strictly necessary demographic information (e.g., gender, age, etc.) will be eventually requested, but as previously reported, there is no way to link this information to the individual. According to the Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016 on the protection of natural persons, we adhere to the following:
| ||
| Do you agree to participate in this survey? | YES ( ) NO ( )  end of questionnaire end of questionnaire |
| Do you live in Italy? | YES ( ) NO ( ) end of questionnaire |
| Are you practicing basketball in any amateur division? (In other words, are you practicing basketball in a formally registered basketball team, irrespective of division, geographic area and level of competition? If you play basketball on a regular basis but you are not affiliated with a formally registered basketball team, please answer “no”) | YES ( ) NO ( ) end of questionnaire |
| Do you benefit from a salary/any economic wage/economic benefits from your team? | YES ( ) NO ( ) end of questionnaire |
| Have any of your friends/neighbors/relatives ever been diagnosed with tetanus? | YES ( ) NO ( ) |
| Do you have any of the following occupations or hobbies? [see Appendix B] | YES ( ) NO ( ) |
| Has your employer enforced any requirement or recommendations for tetanus vaccination? | YES ( ) NO ( ) |
| Do you work in healthcare settings? | YES ( ) NO ( ) |
| To the best of your knowledge, have you received a basic vaccination schedule for tetanus *? | YES ( ) NO ( ) |
| To the best of your knowledge, have you received one booster shot against tetanus within the last 10 years (irrespective of its settings and motivations)? ** | YES ( ) → go to SECTION 1.a NO ( ) → go to SECTION 1.b |
| * = A basic vaccination schedule is defined by all of the required shots for newborns plus another dose at age 6 and another dose at ages 12 to 18 or, in adults without previous TeV or with an unknown vaccination status, four doses (T0, T + 4 weeks, T + 6 months and T + 1 year) plus another dose in the following year. | |
| ** = Please check “yes” if you received the booster dose required for individuals aged 12 to 18 years. | |
| Section 1. Motivators: please report the reasons that motivated you to become vaccinated against tetanus. | |
| Avoiding tetanus | ( ) |
| TeV was recommended by professionals at the emergency departments after an injury | ( ) |
| TeV is required by some personal activities | ( ) |
| TeV is legally required in my workplace | ( ) |
| TeV was recommended by a GP | ( ) |
| TeV is required by my employer | ( ) |
| TeV was recommended by an SP | ( ) |
| TeV was recommended by an OP | ( ) |
| Section 2. Barriers: please report the reasons that caused you to refrain from being vaccinated against tetanus. | |
| Fear of side effects | ( ) |
| Doubts on the efficacy/safety of vaccines | ( ) |
| Doubts on the producers of vaccines | ( ) |
| Forgot periodic shot | ( ) |
| Preference of alternative measures | ( ) |
| Religious motivations | ( ) |
| Other reasons, undisclosed | ( ) |
| Last vaccination shot was performed by | Personnel of a competent local health unit ( ) General practitioner ( ) Occupational physician ( ) Personnel of an emergency department ( ) Unwilling to respond ( ) Unable to recall the last vaccination shot ( ) |
| In recent years, have any of the following medical professionals ever checked your tetanus vaccination status? | General practitioner ( ) Sport physicians ( ) Occupational physician ( ) Any other healthcare provider ( ) |
| According to your understanding and regarding its diffusion in the general population, tetanus is a disease. | 1—Not significant (of no significant concern in daily practice) 2—Slightly significant 3—Somewhat significant 4—Moderately significant 5—Very significant (of very high concern in your daily practice) |
| According to your understanding and regarding its severity in the Italian working population, tetanus is a disease. | 1—Not significant (of no significant concern in daily practice) 2—Slightly significant 3—Somewhat significant 4—Moderately significant 5—Very significant (of very high concern in your daily practice) |
| According to your understanding, tetanus vaccination is potentially associated with side effects that are (frequency) | 1—Not significant (of no significant concern in daily practice) 2—Slightly significant 3—Somewhat significant 4—Moderately significant 5—Very significant (of very high concern in your daily practice) |
| According to your understanding, tetanus vaccination is potentially associated with side effects that are (severity) | 1—Not significant (of no significant concern in daily practice) 2—Slightly significant 3—Somewhat significant 4—Moderately significant 5—Very significant (of very high concern in your daily practice) |
| True | False | Do Not Know | |
| Tetanus may be acquired through improperly managed burns. | [ ] | [ ] | [ ] |
| Tetanus may be acquired through injuries contaminated by earth and dusts. | [ ] | [ ] | [ ] |
| Additives contained in vaccine formulates may elicit severe health effects. | [ ] | [ ] | [ ] |
| Some immunizations may elicit auto-immune diseases. | [ ] | [ ] | [ ] |
| Some vaccines increase the risk for developing allergic disorders. | [ ] | [ ] | [ ] |
| Vaccines are nowadays useless; infectious diseases can be treated through specific drugs. | [ ] | [ ] | [ ] |
| Without vaccines, smallpox would still exist. | [ ] | [ ] | [ ] |
| The efficacy of vaccines has been repetitively proven. | [ ] | [ ] | [ ] |
| In Italy, tetanus vaccines are associated with specific legal requirements. | [ ] | [ ] | [ ] |
| Children would be more resistant to natural infections if unvaccinated. | [ ] | [ ] | [ ] |
| Some vaccinations are administered too early. | [ ] | [ ] | [ ] |
| The immune system may be overloaded by current frequency of vaccines required for school. | [ ] | [ ] | [ ] |
| Tetanus vaccine is required for sport activities, even for basketball. | [ ] | [ ] | [ ] |
| I am not interested in obtaining the tetanus vaccine, ever. | ( ) |
| I am not interested in obtaining the tetanus vaccine with the next 6 months. | ( ) |
| I am uncertain whether I am interested in obtaining the tetanus vaccine. | ( ) |
| I am considering discussing tetanus vaccine with a physician. | ( ) |
| I am interested in obtaining the tetanus vaccine within the next 6 months but have no appointment booked yet. | ( ) |
| I am interested in obtaining the tetanus vaccine within the next 30 days but have no appointment booked yet. | ( ) |
| I have booked a vaccination appointment. | ( ) |
| I have received my first vaccination shot but have no plans for further shots. | ( ) |
| I have received my first vaccination shot; I have noted the need for further shots. | ( ) |
| I have received first vaccination shot; I have made appointments for further shots. | ( ) |
| I’ve completed the vaccination schedule, I have noted the need for further shots | ( ) |
| Eventually, we will request some personal information from you. | |
| You are (by your personal understanding) | |
| Male | ( ) |
| Female | ( ) |
| Rather not answer | ( ) |
| Year of birth | ___________ |
| Your highest achievement in terms of education: | ( ) Primary school (<8 years of formal education) ( ) Secondary school (8–13 years of formal education) ( ) University or higher |
| Were you or any of your parents born abroad? | YES ( ) NO ( ) |
| Do you live with subjects aged 12 years or less? | YES ( ) NO ( ) |
Appendix B
- Farmers and agricultural workers;
- Shepherds;
- Cattle breeders;
- Hostlers;
- Horse riders;
- Tanners;
- Janitors and personnel managing hippodromes;
- Scavengers/(street) sweepers;
- Road maintenance workers;
- Diggers/laborers;
- Miners;
- Kilnsmen;
- Construction workers;
- All railway workers;
- Ragmen;
- Garbage collectors/people managing wastewater;
- Workers from the industry of paper and cardboard;
- Carpenters and joiners;
- Workers from metallurgical industries.
Appendix C. List of Acronyms
| BP | basketball player |
| GKS | general knowledge score |
| GP | general practitioner |
| OP | occupational physician |
| RPS | risk perception score |
| RPS-T | risk perception score, tetanus |
| RPS-V | risk perception score, vaccine |
| SP | sport physician |
| TeV | tetanus vaccine |
| TTM | transtheoretical model |
References
- Yen, L.M.; Thwaites, C.L. Tetanus. Lancet 2019, 393, 1657–1668. [Google Scholar] [CrossRef]
- Mori, Y.; Katasako, A.; Matsunaga, S.; Matono, T. Tetanus: Remember to Vaccinate. Lancet 2019, 393, 2331. [Google Scholar] [CrossRef]
- Filia, A.; Bella, A.; von Hunolstein, C.; Pinto, A.; Alfarone, G.; Declich, S.; Rota, M.C. Tetanus in Italy 2001-2010: A Continuing Threat in Older Adults. Vaccine 2014, 32, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Pedalino, B.; Cotter, B.; Ciofi degli Atti, M.; Mandolini, D.; Parroccini, S.; Salmaso, S. Epidemiology of Tetanus in Italy in Years 1971–2000. Eurosurveillance 2002, 7, 103–110. [Google Scholar] [CrossRef]
- Valentino, M.; Rapisarda, V. Tetanus in a Central Italian Region: Scope for More Effective Prevention among Unvaccinated Agricultural Workers. Occup. Med. 2001, 51, 114–117. [Google Scholar] [CrossRef] [Green Version]
- Filia, A.; Bella, A.; D’Ancona, F.; Fabiani, M.; Giambi, C.; Rizzo, C.; Ferrara, L.; Pascucci, M.G.; Rota, M.C. Childhood Vaccinations: Knowledge, Attitudes and Practices of Paediatricians and Factors Associated with Their Confidence in Addressing Parental Concerns, Italy, 2016. Eurosurveillance 2019, 24, 1800275. [Google Scholar] [CrossRef] [Green Version]
- Ricco, M.; Cattani, S.; Veronesi, L.; Colucci, M.E. Knowledge, Attitudes, Beliefs and Practices of Construction Workers towards Tetanus Vaccine in Northern Italy. Ind. Health 2016, 54, 554–563. [Google Scholar] [CrossRef] [Green Version]
- Law No. 292/1963. Official Gazette of the Italian Republic; Istituto Poligrafico e Zecca dello Stato: Rome, Italy, 1963; p. 83. [Google Scholar]
- Riccò, M.; Razio, B.; Panato, C.; Poletti, L.; Signorelli, C. Knowledge, Attitudes and Practices of Agricultural Workers towards Tetanus Vaccine: A Field Report. Ann. Ig. 2017, 29, 239–255. [Google Scholar] [CrossRef]
- Riccò, M.; Vezzosi, L.; Cella, C.; Pecoraro, M.; Novembre, G.; Moreo, A.; Ognibeni, E.M.; Schellenberg, G.; Maranelli, G. Tetanus Vaccination Status in Construction Workers: Results from an Institutional Surveillance Campaign. Acta Biomed. 2019, 90, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Prospero, E.; Appignanesi, R.; D’Errico, M.M.; Carle, F. Epidemiology of Tetanus in the Marches Regions of Italy, 1992–1995. Bull. World Health Organ 1998, 76, 47–54. [Google Scholar] [PubMed]
- European Centre for Disease Prevention and Control (ECDC). Surveillance Report-Tetanus Annual Epidemiological Report for 2017; ECDC: Stockholm, Sweden, 2019; Volume 393. [Google Scholar]
- Bonanni, P.; Ferrero, A.; Guerra, R.; Iannazzo, S.; Odone, A.; Pompa, M.; Rizzuto, E.; Signorelli, C. Vaccine Coverage in Italy and Assessment of the 2012–2014 National Immunization Prevention Plan. Epidemiol. Prev. 2015, 39, 146–158. [Google Scholar] [CrossRef]
- Biasio, L.R.; Corsello, G.; Costantino, C.; Fara, G.M.; Giammanco, G.; Signorelli, C.; Vecchio, D.; Vitale, F. Communication about Vaccination: A Shared Responsibility. Hum. Vaccines Immunother. 2016, 12, 2984–2987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Signorelli, C.; Guerra, R.; Siliquini, R.; Ricciardi, W. Italy’s Response to Vaccine Hesitancy: An Innovative and Cost Effective National Immunization Plan Based on Scientific Evidence. Vaccine 2017, 35, 4057–4059. [Google Scholar] [CrossRef] [PubMed]
- Casasco, M.; Gianfelici, A.; Icardi, G.; Milicia, G.M.; Odone, A.; Parisi, A.; Pasquarella, C.; Signorelli, C.; Veicsteinas, A.; Vezzosi, L. Raccomandazioni Delle Associazioni Scientifiche per Le Vaccinazioni Negli Atleti Professionisti. Med. Dello Sport 2017, 70, 389–409. [Google Scholar] [CrossRef]
- Karpinos, A.R.; Rizzone, K.H.; Cribbs, S.P.; Roumie, C.L. Low Proportion of High School Senior Athletes Receiving Recommended Immunizations. Physician Sportsmed. 2014, 42, 71–79. [Google Scholar] [CrossRef]
- Conway, J.J.; Toresdahl, B.G.; Ling, D.I.; Boniquit, N.T.; Callahan, L.R.; Kinderknecht, J.J. Prevalence of Inadequate Immunity to Measles, Mumps, Rubella, and Varicella in MLB and NBA Athletes. Sports Health 2018, 10, 406–411. [Google Scholar] [CrossRef]
- Michael Kaskey-Blomain Unvaccinated NBA Players Won’t Be Paid for Every Game Missed Due to Local COVID-19 Mandates. Available online: https://www.cbssports.com/nba/news/unvaccinated-nba-players-wont-be-paid-for-every-game-missed-due-to-local-covid-19-mandates/ (accessed on 4 October 2021).
- Deb, S. NBA Vaccine Skeptics Speak Out-The New York Times. The New York Times. 4 October 2021. Available online: https://www.nytimes.com/2021/09/27/sports/basketball/nba-vaccine-kyrie-irving.html (accessed on 14 January 2021).
- Nielsen Sports. Basketball Italia 2017; Nielsen Company LLC–Nielsen Italia SpA: Milan, Italy, 2017; pp. 1–6. Available online: https://www.nielsen.com/wp-content/uploads/sites/3/2019/04/Nielsen20Sports20-20Basket20in20Italia202017.pdf (accessed on 14 January 2021).
- Istituto Nazionale di Statistica (ISTAT). La Pratica Sportiva in Italia; ISTAT: Rome, Italy, 2016; Available online: https://www.istat.it/it/archivio/204663 (accessed on 14 January 2021).
- Trabacchi, V.; Odone, A.; Lillo, L.; Pasquarella, C.; Signorelli, C. Immunization Practices in Athletes. Acta Biomed. 2015, 86, 181–188. [Google Scholar] [PubMed]
- Grosset-Janin, A.; Nicolas, X.; Saraux, A. Sport and Infectious Risk: A Systematic Review of the Literature over 20 Years. Med. Et Mal. Infect. 2012, 42, 533–544. [Google Scholar] [CrossRef]
- World Health Organization Tetanus Vaccines: WHO Position Paper. Wkly. Epidemiol. Rec. 2017, 92, 53–76. [CrossRef]
- Betsch, C.; Wicker, S. Personal Attitudes and Misconceptions, Not Official Recommendations Guide Occupational Physicians’ Vaccination Decisions. Vaccine 2014, 32, 4478–4484. [Google Scholar] [CrossRef]
- Zingg, A.; Siegrist, M. Measuring People’s Knowledge about Vaccination: Developing a One-Dimensional Scale. Vaccine 2012, 30, 3771–3777. [Google Scholar] [CrossRef]
- Salmon, D.A.; Moulton, L.H.; Omer, S.B.; Chace, L.M.; Klassen, A.; Talebian, P.; Halsey, N.A. Knowledge, Attitudes, and Beliefs of School Nurses and Personnel and Associations with Nonmedical Immunization Exemptions. Pediatrics 2004, 113, e552–e559. [Google Scholar] [CrossRef] [Green Version]
- Lipschitz, J.M.; Fernandez, A.C.; Elsa Larson, H.; Blaney, C.L.; Meier, K.S.; Redding, C.A.; Prochaska, J.O.; Paiva, A.L. Validation of Decisional Balance and Self-Efficacy Measures for HPV Vaccination in College Women. Am. J. Health Promot. 2013, 27, 299–307. [Google Scholar] [CrossRef]
- Fernandez, A.C.; Amoyal, N.R.; Paiva, A.L.; Prochaska, J.O. Motivation for HPV Vaccination among Young Adult Men: Validation of TTM Decisional Balance and Self-Efficacy Constructs. Am. J. Health Promot. 2016, 30, 163–171. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, N.E.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; Goldstein, S.; Larson, H.; Manzo, M.L.; Reingold, A.; et al. Vaccine Hesitancy: Definition, Scope and Determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Corace, K.M.; Srigley, J.A.; Hargadon, D.P.; Yu, D.; MacDonald, T.K.; Fabrigar, L.R.; Garber, G.E. Using Behavior Change Frameworks to Improve Healthcare Worker Influenza Vaccination Rates: A Systematic Review. Vaccine 2016, 34, 3235–3242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piltch-Loeb, R.; Diclemente, R. The Vaccine Uptake Continuum: Applying Social Science Theory to Shift Vaccine Hesitancy. Vaccines 2020, 8, 76. [Google Scholar] [CrossRef] [Green Version]
- Aldossri, M.; Okoronkwo, C.; Dodd, V.; Manson, H.; Singhal, S. Determinants of Dentists’ Readiness to Assess HPV Risk and Recommend Immunization: A Transtheoretical Model of Change-Based Cross-Sectional Study of Ontario Dentists. PLoS ONE 2021, 16, e0247043. [Google Scholar] [CrossRef]
- Prochaska, J.O.; Velicer, W.F. The Transtheoretical Model of Health Behavior Change. Am. J. Health Promot. 1997, 12, 38–48. [Google Scholar] [CrossRef]
- Tafuri, S.; Sinesi, D.; Gallone, M.S. Vaccinations among Athletes: Evidence and Recommendations. Expert Rev. Vaccines 2017, 16, 867–869. [Google Scholar] [CrossRef]
- Boston, C.D.; Bryan, J.J. Immunizations in Athletes. Sports Health 2018, 10, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Signorelli, C.; Odone, A.; Miduri, A.; Cella, P.; Pasquarella, C.; Gozzini, A.; Tamburrino, P.; Castellacci, E. Flu Vaccination in Elite Athletes: A Survey among Serie a Soccer Teams. Acta Biomed. 2016, 87, 117–120. [Google Scholar]
- Rea, N.; di Reggiero, G. La Prevenzione Del Tetano Nell’attività Sportiva [Prevention of Tetanus among Athletes]. Med. Dello Sport 2001, 54, 157–163. [Google Scholar]
- Decreto Ministeriale 18 Febbraio 1982-Norme per La Tutela Sanitaria Dell’attività Sportiva Agonistica [Ministerial Decree, 18 February 1982-Standards for the Health Surveillance in Sport Practice]. Off. Gaz. Ital. Repub. 1982, 63, 233–247.
- Regional Law n.35, 9 July 2003 of the Regional Parliament of Tuscany. Off. Bull. Tuscany Reg. 2003, 29, 3–9.
- Kousoulis, A.A.; Sergentanis, T.N.; Tsiodras, S. 2009 H1N1 Flu Pandemic among Professional Basketball Players: Data from 18 Countries. Infez. Med. 2014, 4, 302–308. [Google Scholar]
- Stewart, A. Influenza a Vaccination Knowledge, Attitude, Practice of Athletes Competing in Canadian Interuniversity Sport in Calgary, Alberta. Int. J. Kinesiol. Sports Sci. 2016, 4, 10–17. [Google Scholar] [CrossRef] [Green Version]
- Luke, A.; d’Hemecourt, P. Prevention of Infectious Diseases in Athletes. Clin. Sports Med. 2007, 26, 321–344. [Google Scholar] [CrossRef]
- Schmid, P.; Rauber, D.; Betsch, C.; Lidolt, G.; Denker, M.L. Barriers of Influenza Vaccination Intention and Behavior-A Systematic Review of Influenza Vaccine Hesitancy, 2005–2016. PLoS ONE 2017, 12, e0170550. [Google Scholar] [CrossRef]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond Confidence: Development of a Measure Assessing the 5C Psychological Antecedents of Vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef] [Green Version]
- Yoon, Y.H.; Moon, S.W.; Choi, S.H.; Cho, Y.D.; Kim, J.Y.; Kwak, Y.H. Clinician Awareness of Tetanus-Diphtheria Vaccination in Trauma Patients: A Questionnaire Study. Scand. J. Trauma Resusc. Emerg. Med. 2012, 20, 35. [Google Scholar] [CrossRef] [Green Version]
- Gualano, M.R.; Olivero, E.; Voglino, G.; Corezzi, M.; Rossello, P.; Vicentini, C.; Bert, F.; Siliquini, R. Knowledge, Attitudes and Beliefs towards Compulsory Vaccination: A Systematic Review. Hum. Vaccines Immunother. 2019, 15, 918–931. [Google Scholar] [CrossRef] [Green Version]
- Gualano, M.R.; Bert, F.; Voglino, G.; Buttinelli, E.; D’Errico, M.M.; de Waure, C.; di Giovanni, P.; Fantini, M.P.; Giuliani, A.R.; Marranzano, M.; et al. Attitudes towards Compulsory Vaccination in Italy: Results from the NAVIDAD Multicentre Study. Vaccine 2018, 36, 3368–3374. [Google Scholar] [CrossRef] [Green Version]
- Manzoli, L.; Sotgiu, G.; Magnavita, N.; Durando, P.; Barchitta, M.; Carducci, A.; Conversano, M.; de Pasquale, G.; Dini, G.; Firenze, A.; et al. Evidence-Based Approach for Continuous Improvement of Occupational Health. Epidemiol. E Prev. 2015, 39, 81–85. [Google Scholar]
- European Centre For Disease Prevention and Control (ECDC). Vaccine Hesitancy among Healthcare Workers and Their Patients in Europe; ECDC: Stockholm, Sweden, 2015; ISBN 9789291937226. [Google Scholar]
- Brunelli, L.; Antinolfi, F.; Malacarne, F.; Cocconi, R.; Brusaferro, S. A Wide Range of Strategies to Cope with Healthcare Workers’ Vaccine Hesitancy in A North-Eastern Italian Region: Are They Enough? Healthcare 2020, 9, 4. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Poland, G.A. Vaccination Policies for Healthcare Workers in Europe. Vaccine 2014, 32, 4876–4880. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Theodoridou, K.; Ledda, C.; Rapisarda, V.; Theodoridou, M. Vaccination of Healthcare Workers: Is Mandatory Vaccination Needed? Expert Rev. Vaccines 2019, 18, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Bloom, B.R.; Marcuse, E.; Mnookin, S. Addressing Vaccine Hesitancy. Science 2014, 344, 339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salmon, D.A.; Dudley, M.Z.; Glanz, J.M.; Omer, S.B. Vaccine Hesitancy: Causes, Consequences, and a Call to Action. Am. J. Prev. Med. 2015, 49, S391–S398. [Google Scholar] [CrossRef] [PubMed]
- Jarrett, C.; Wilson, R.; O’Leary, M.; Eckersberger, E.; Larson, H.J.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; et al. Strategies for Addressing Vaccine Hesitancy-A Systematic Review. Vaccine 2015, 33, 4180–4190. [Google Scholar] [CrossRef] [Green Version]
- Biasio, L.R.; Bonaccorsi, G.; Lorini, C.; Mazzini, D.; Pecorelli, S. Italian Adults’ Likelihood of Getting COVID-19 Vaccine: A Second Online Survey. Vaccines 2021, 9, 268. [Google Scholar] [CrossRef]
- Gualano, M.R.; lo Moro, G.; Voglino, G.; Bert, F.; Siliquini, R. Is the Pandemic Leading to a Crisis of Trust? Insights from an Italian Nationwide Study. Public Health 2021, 202, 32–34. [Google Scholar] [CrossRef]
- Riccò, M.; Gualerzi, G.; Ranzieri, S.; Ferraro, P.; Bragazzi, N.L. Knowledge, Attitudes, Practices (KAP) of Italian Occupational Physicians towards Tick Borne Encephalitis. Trop. Med. Infect. Dis. 2020, 5, 117. [Google Scholar] [CrossRef]
- Heiervang, E.; Goodman, R. Advantages and Limitations of Web-Based Surveys: Evidence from a Child Mental Health Survey. Soc. Psychiat. Epidemiol. 2011, 46, 69–76. [Google Scholar] [CrossRef]
- Huang, Y.; Xu, S.; Lei, W.; Zhao, Y.; Liu, H.; Yao, D.; Xu, Y.; Lv, Q.; Hao, G.; Xu, Y.; et al. Knowledge, Attitudes, and Practices Regarding Zika: Paper and Internet Based Survey in Zhejiang, China. JMIR Public Health Surveill 2017, 3, e81. [Google Scholar] [CrossRef]
- Riccò, M.; Ferraro, P.; Peruzzi, S.; Balzarini, F.; Ranzieri, S. Hantaviruses in Agricultural and Forestry Workers: Knowledge, Attitudes and Practices in Italian Physicians. Trop. Med. Infect. Dis. 2021, 6, 169. [Google Scholar] [CrossRef]
- Riccò, M.; Cattani, S.; Casagranda, F.; Gualerzi, G.; Signorelli, C. Knowledge, Attitudes, Beliefs and Practices of Occupational Physicians towards Vaccinations of Health Care Workers: A Cross Sectional Pilot Study in North-Eastern Italy. Int. J. Occup. Med. Environ. Health 2017, 30, 775–790. [Google Scholar] [CrossRef]
- Auffret, Y.; Rousseaux, J.Y.; Gatineau, F.; Hamoniaux, F.; Gouillou, M.; Abalea Le Dreff, L.; Pina Silas, S.; Rakatobe, F.; Alavi, Z. Should We Believe Emergency Department Patients Self-Reported Tetanus Vaccine Status? Am. J. Emerg. Med. 2019, 37, 983–990. [Google Scholar] [CrossRef]
- Riccò, M.; Vezzosi, L.; Balzarini, F.; Gualerzi, G.; Ranzieri, S.; Khamisy-Farah, R.; Bragazzi, N. Vaccines are underused in pregnancy: What about knowledge, attitudes and practices of providers? Acta Biomed. 2020, 91S3, 55–62. [Google Scholar] [CrossRef]
- Bert, F.; Olivero, E.; Rossello, P.; Gualano, M.R.; Castaldi, S.; Damiani, G.; D’Errico, M.M.; di Giovanni, P.; Fantini, M.P.; Fabiani, L.; et al. Knowledge and Beliefs on Vaccines among a Sample of Italian Pregnant Women: Results from the NAVIDAD Study. Eur. J. Public Health 2019, 30, 286–292. [Google Scholar] [CrossRef]
- Rapisarda, V.; Bracci, M.; Nunnari, G.; Ferrante, M.; Ledda, C. Tetanus Immunity in Construction Workers in Italy. Occup. Med. 2014, 64, 217–219. [Google Scholar] [CrossRef] [Green Version]
- Sutton, S. Interpreting Cross-Sectional Data on Stages of Change. Psychol. Health 2000, 15, 163–171. [Google Scholar] [CrossRef]
- Sestili, C.; Grazina, I.; la Torre, G. HBV Vaccine and Risk of Developing Multiple Sclerosis: A Systematic Review and Meta-Analysis. Hum. Vaccines Immunother. 2021, 17, 2273–2278. [Google Scholar] [CrossRef]
- Levi, M.; Sinisgalli, E.; Lorini, C.; Santomauro, F.; Chellini, M.; Bonanni, P. The “Fluad Case” in Italy: Could It Have Been Dealt Differently? Hum. Vaccines Immunother. 2017, 13, 379–384. [Google Scholar] [CrossRef]
- Mahroum, N.; Watad, A.; Rosselli, R.; Brigo, F.; Chiesa, V.; Siri, A.; Ben-Ami Shor, D.; Martini, M.; Bragazzi, N.L.; Adawi, M. An Infodemiological Investigation of the So-Called “Fluad Effect” during the 2014/2015 Influenza Vaccination Campaign in Italy: Ethical and Historical Implications. Hum. Vaccines Immunother. 2018, 14, 712–718. [Google Scholar] [CrossRef]
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and Receptivity for COVID-19 Vaccines: A Rapid Systematic Review. Vaccines 2021, 9, 16. [Google Scholar] [CrossRef]
- Riccò, M.; Ferraro, P.; Peruzzi, S.; Balzarini, F.; Ranzieri, S. Mandate or Not Mandate: Knowledge, Attitudes, and Practices of Italian Occupational Physicians towards SARS-CoV-2 Immunization at the Beginning of Vaccination Campaign. Vaccines 2021, 9, 889. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| No./270, % | Average ± S.D. | |
|---|---|---|
| Age (years) | 36.9 ± 12.0 | |
| Age > 50 years | 36, 13.3% | |
| Gender | ||
| Male | 115, 42.6% | |
| Female | 155, 57.4% | |
| Formal education | ||
| Primary school | 6, 2.2% | |
| Secondary school | 103, 38.2% | |
| University or higher | 161, 59.6% | |
| Migration background | 5, 1.9% | |
| Living with children | 85, 31.5% | |
| Working in healthcare settings or affiliate | 93, 34.4% | |
| Working in settings requiring TeV | 35, 13.0% | |
| Potential exposure to tetanus in hobbies/personal activities | 123, 45.6% | |
| Previous interaction with tetanus case(s) | 19, 7.0% | |
| Appropriate tetanus vaccination status | 197, 73.0% | |
| Last vaccination shot performed by one of the following: | ||
| Personnel of the competent Local Health Unit | 128, 47.4% | |
| General Practitioner | 20, 7.4% | |
| Occupational Physician | 9, 3.3% | |
| Personnel of an Emergency Department | 8, 3.0% | |
| Information not provided | 32, 11.9% | |
| Unable to recall the last vaccination shot | 73, 27.0% | |
| General practitioner checked TeV (ever) | 73, 27.0% | |
| Sport physician checked TeV (ever) | 47, 17.4% | |
| Occupational physician checked TV (ever) | 69, 25.6% | |
| Previously checked by an healthcare provider | 100, 37.0% | |
| Any hesitancy towards TeV | 90, 33.3% | |
| General Knowledge Score (%) | 79.8 ± 16.6 | |
| General Knowledge Score > median (83.3%) | 94, 34.8% | |
| Tetanus is a severe/very severe disease | 246, 91.1% | |
| Tetanus is a common/very common disease | 161, 59.6% | |
| TeV is potentially associated with severe/very severe side effects | 13, 1.1% | |
| TeV is associated with common/very common side effects | 39, 6.3% | |
| Risk Perception Score—natural infection (%) | 63.9 ± 26.6 | |
| Risk Perception Score—vaccine (%) | 14.0 ± 15.4 | |
| Risk Perception Score—natural infection > median (60.0%) | 114, 42.2% | |
| Risk Perception Score—vaccine > median (8.0%) | 116, 43.0% |
| Statement | Correct Answer | No., % |
|---|---|---|
| Tetanus may be acquired through improperly managed burns. | True | 93, 34.4% |
| Tetanus may be acquired through injuries contaminated by earth and dusts. | True | 244, 90.4% |
| Additives contained in vaccine formulates may elicit severe health effects. | False | 207, 76.7% |
| Some immunizations may elicit auto-immune diseases. | False | 270, 100% |
| Some vaccines increase the risk for developing allergic disorders. | False | 216, 80.0% |
| Vaccines are nowadays useless; infectious diseases can be treated through specific drugs. | False | 239, 88.5% |
| Without vaccines, smallpox would still exist. | True | 254, 94.1% |
| The efficacy of vaccines has been repetitively proven. | True | 257, 95.2% |
| In Italy, tetanus vaccines are associated with specific legal requirements. | True | 167, 61.9% |
| Children would be more resistant to natural infections if unvaccinated. | False | 239, 88.5% |
| Some vaccinations are administered too early. | False | 207, 76.7% |
| The immune system may be overloaded by the current frequency of vaccines required for school. | False | 192, 71.1% |
| Tetanus vaccine is required for sport activities, even for basketball. | True | 82, 30.4% |
| Status According the TTM | No., % | |
|---|---|---|
| I am not interested in obtaining the tetanus vaccine, ever. | Precontemplation | 8, 3.0% |
| I am not interested in obtaining the tetanus vaccine within the next 6 months. | Precontemplation | 31, 11.5% |
| I am uncertain whether I am interested in obtaining the tetanus vaccine. | Contemplation | 7, 2.6% |
| I am considering discussing the tetanus vaccine with a physician. | Contemplation | 4, 1.5% |
| I am interested in obtaining the tetanus vaccine within the next 6 months but have no appointment booked yet. | Contemplation | 40, 14.8% |
| Somewhat hesitant | 90, 33.3% | |
| I am interested in obtaining the tetanus vaccine within the next 30 days but have no appointment booked yet. | Preparation | 9, 3.3% |
| I have booked a vaccination appointment. | Action | 6, 2.2% |
| I have received my first vaccination shot but have no plans for further shots. | Action | 12, 4.4% |
| I have received my first vaccination shot; I have noted the need for further shots. | Maintenance | 76, 28.1% |
| I have received my first vaccination shot; I have appointments for further shots. | Maintenance | 16, 5.9% |
| I have completed the vaccination schedule; I have noted the need further shots. | Termination | 61, 22.6% |
| Somewhat Favorable | 180, 66.7% |
| Barriers | No./73, % |
| Fear of side effects | 46, 63.0% |
| Doubts on the efficacy/safety of vaccines | 12, 16.4% |
| Doubts about the producers of vaccines | 7, 9.6% |
| Forgot periodic shot | 4, 5.5% |
| Preference of alternative measures | 4, 5.5% |
| Personal motivations, undisclosed | 0, - |
| Religious motivations | 0, - |
| Motivators | No./197 |
| Avoiding tetanus | 111, 56.3% |
| TeV was recommended by professionals at emergency departments after an injury | 14, 17.1% |
| TeV is required by some personal activities | 26, 13.2% |
| TeV is legally required in my workplace | 11, 5.6% |
| TeV was recommended by a GP | 9, 4.6% |
| TeV is required by my employer | 3, 1.5% |
| TeV was recommended by an SP | 3, 1.5% |
| TeV was recommended by an OP | 3, 1.5% |
| Appropriate TeV Status | Any Vaccine Hesitancy | |||||
|---|---|---|---|---|---|---|
| Yes (No./197, %) | No (No./73, %) | p Value | Yes (No./90, %) | No (No./180, %) | p Value | |
| Male gender | 72, 36.5% | 43, 58.9% | 0.002 | 52, 57.8% | 63, 35.0% | 0.001 |
| Aged ≥ 40 y.o. | 116, 58.9% | 50, 68.5% | 0.193 | 63, 70.0% | 103, 57.2% | 0.057 |
| Formal education—university or higher | 133, 67.5% | 28, 38.5% | <0.001 | 40, 44.4% | 121, 67.2% | <0.001 |
| Migration background | 3, 1.5% | 2, 2.7% | 0.880 | 2, 2.2% | 3, 1.7% | 1.000 |
| Children in the household | 64, 32.5% | 21, 28.8% | 0.662 | 33, 36.7% | 52, 28.9% | 0.247 |
| Previous interactions with tetanus | 15, 7.6% | 4, 5.5% | 0.733 | 2, 2.2% | 17, 9.4% | 0.053 |
| Working in healthcare settings | 68, 34.5% | 25, 34.2% | 1.000 | 20, 22.2% | 73, 40.6% | 0.004 |
| Occupational requirement for TeV | 20, 10.2% | 15, 20.5% | 0.040 | 15, 16.7% | 20, 11.1% | 0.276 |
| Hobbies at risk for tetanus | 90, 45.7% | 33, 45.2% | 1.000 | 44, 48.9% | 79, 43.9% | 0.517 |
| TeV checked by SP | 23, 11.7% | 24, 32.9% | <0.001 | 25, 27.8% | 22, 12.2% | 0.003 |
| TeV checked by OP | 56, 45.5% | 13, 29.5% | 0.095 | 14, 25.9% | 55, 48.7% | 0.009 |
| TeV checked by GP | 57, 28.9% | 16, 21.9% | 0.318 | 12, 13.3% | 61, 33.9% | 0.001 |
| TeV checked, any healthcare provider | 77, 39.1% | 23, 31.5% | 0.316 | 25, 27.8% | 75, 41.7% | 0.036 |
| GKS > median value | 74, 37.6% | 20, 27.4% | 0.157 | 20, 22.2% | 74, 41.1% | 0.003 |
| RPS-T > median value | 92, 46.7% | 22, 30.1% | 0.021 | 34, 37.8% | 80, 44.4% | 0.360 |
| RPS-V > median value | 74, 37.6% | 42, 57.5% | 0.005 | 45, 50.0% | 71, 39.4% | 0.128 |
| Vaccine hesitancy (any) | 37, 18.8% | 53, 72.6% | <0.001 | - | - | - |
| Appropriate TeV status | - | - | - | 37, 41.1% | 160, 88.9% | <0.001 |
| Appropriate TeV Status | Vaccine Hesitancy | |||
|---|---|---|---|---|
| adjOR | 95%CI | adjOR | 95%CI | |
| Male gender | 0.527 | 0.269; 1.032 | 3.148 | 1.072; 9.244 |
| Formal education—university of higher | 1.784 | 0.886; 3.592 | 0.065 | 0.013; 0.319 |
| Working in healthcare settings | - | - | 0.042 | 0.007; 0.265 |
| Occupational requirement for TeV | 0.645 | 0.235; 1.766 | - | - |
| TeV checked by SP | 0.433 | 0.187; 1.005 | 3.138 | 0.661; 14.910 |
| TeV checked by OP | - | - | 0.181 | 0.024; 1.347 |
| TeV checked by GP | - | - | 0.126 | 0.014; 1.126 |
| TeV checked, any healthcare provider | - | - | 1.199 | 0.110; 13.106 |
| GKS > median value | - | - | 3.099 | 0.790; 12.158 |
| RPS-T > median value | 1.786 | 0.870; 3.666 | - | - |
| RPS-V > median value | 0.641 | 0.321; 1.280 | - | - |
| Vaccine hesitancy (any) | 0.115 | 0.059; 0.225 | - | - |
| Appropriate TeV status | - | - | 0.030 | 0.006; 0.151 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riccò, M.; Peruzzi, S. Tetanus Vaccination Status and Vaccine Hesitancy in Amateur Basketball Players (Italy, 2020). Vaccines 2022, 10, 131. https://doi.org/10.3390/vaccines10010131
Riccò M, Peruzzi S. Tetanus Vaccination Status and Vaccine Hesitancy in Amateur Basketball Players (Italy, 2020). Vaccines. 2022; 10(1):131. https://doi.org/10.3390/vaccines10010131
Chicago/Turabian StyleRiccò, Matteo, and Simona Peruzzi. 2022. "Tetanus Vaccination Status and Vaccine Hesitancy in Amateur Basketball Players (Italy, 2020)" Vaccines 10, no. 1: 131. https://doi.org/10.3390/vaccines10010131