
COVID-19 Vaccine Hesitancy and Associated Factors among Diabetes Patients: A Cross-Sectional Survey in Changzhi, Shanxi, China

Abstract
:1. Introduction
2. Materials and Methods
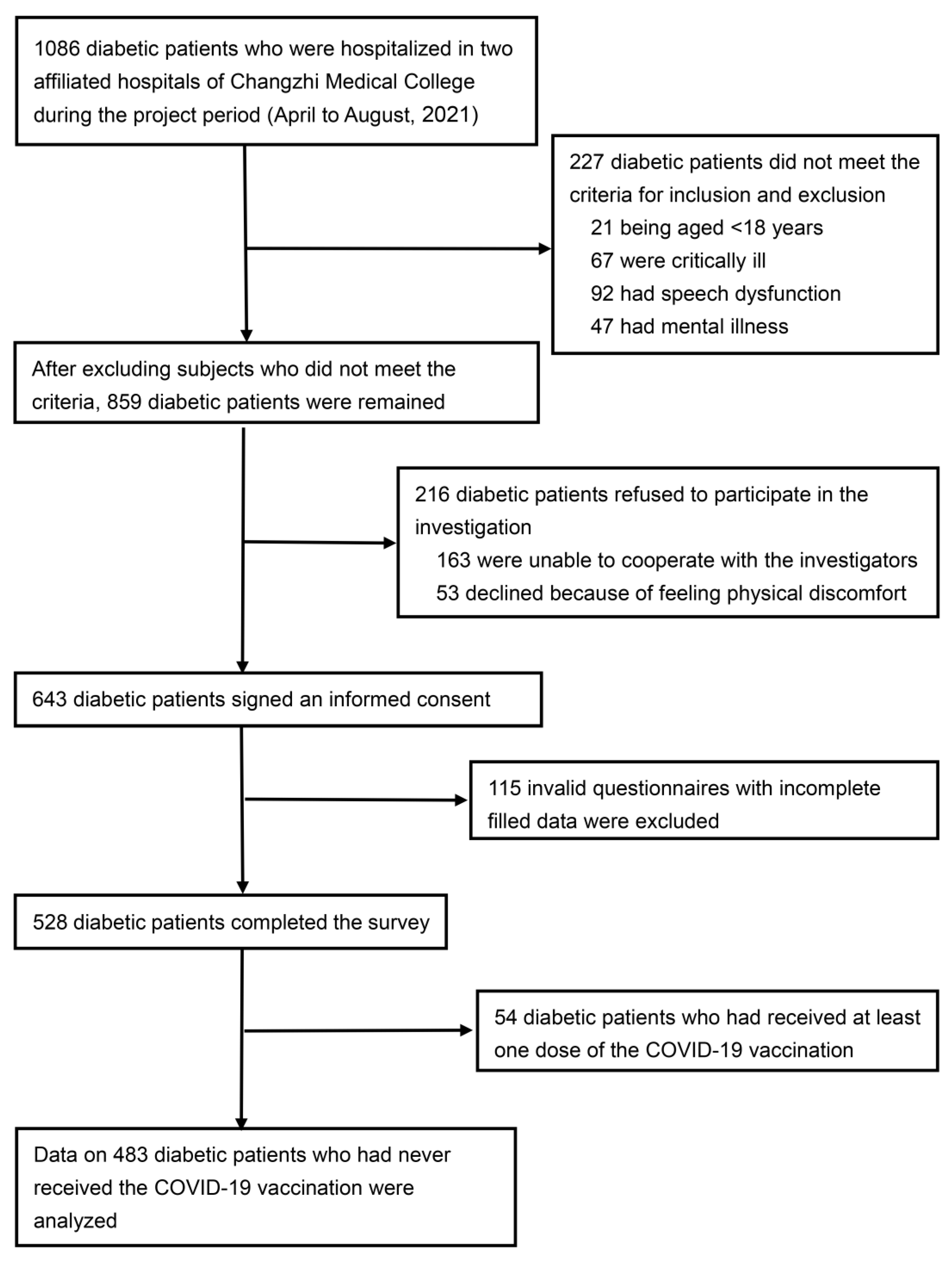
2.1. Study Design
2.2. Inclusion and Exclusion Criteria
2.3. Sample Size Calculation
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. SARS-CoV-2 Vaccination Variables for the HBM
3.3. SARS-CoV-2 Vaccine Hesitancy and Associated Factors
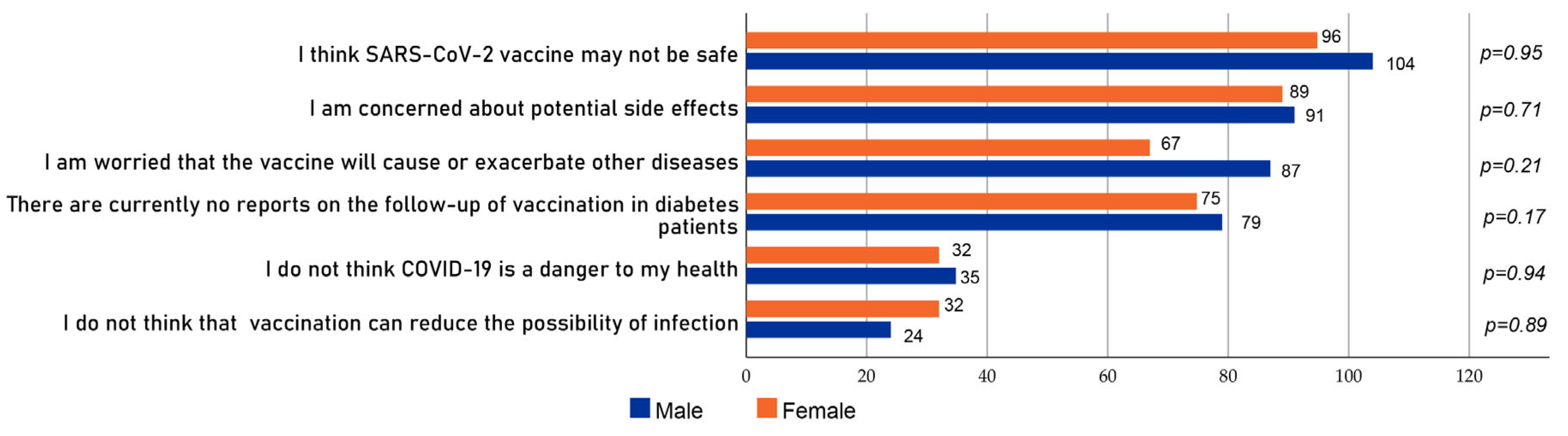
3.4. Reasons for Diabetes Patients’ Hesitancy to Receive the SARS-CoV-2 Vaccine
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Majeed, J.; Ajmera, P.; Goyal, R.K. Delineating clinical characteristics and comorbidities among 206 COVID-19 deceased patients in India: Emerging significance of renin angiotensin system derangement. Diabetes Res. Clin. Pract. 2020, 167, 108349. [Google Scholar] [CrossRef]
- American Diabetes Association. 4. Comprehensive Medical Evaluation and Assessment of Comorbidities: Standards of Medical Care in Diabetes-2020. Diabetes Care 2020, 43, S37–S47. [Google Scholar] [CrossRef] [Green Version]
- Wang, W.; Lu, J.; Gu, W.; Zhang, Y.; Liu, J.; Ning, G. Care for diabetes with COVID-19: Advice from China. J. Diabetes 2020, 12, 417–419. [Google Scholar] [CrossRef] [Green Version]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72,314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Vamos, E.P.; Pape, U.J.; Curcin, V.; Harris, M.J.; Valabhji, J.; Majeed, A.; Millett, C. Effectiveness of the influenza vaccine in preventing admission to hospital and death in people with type 2 diabetes. Can. Med. Assoc. J. 2016, 188, E342–E351. [Google Scholar] [CrossRef] [Green Version]
- Wang, I.K.; Lin, C.L.; Chang, Y.C.; Lin, P.C.; Liang, C.C.; Liu, Y.L.; Chang, C.T.; Yen, T.H.; Huang, C.C.; Sung, F.C. Effectiveness of influenza vaccination in elderly diabetic patients: A retrospective cohort study. Vaccine 2013, 31, 718–724. [Google Scholar] [CrossRef]
- Zhang, J.Y.; Shang, T.; Ahn, D.; Chen, K.; Coté, G.; Espinoza, J.; Mendez, C.E.; Spanakis, E.K.; Thompson, B.; Wallia, A. How to Best Protect People with Diabetes from the Impact of SARS-CoV-2: Report of the International COVID-19 and Diabetes Summit. J. Diabetes Sci. Technol. 2021, 15, 478–514. [Google Scholar] [CrossRef]
- IDF Diabetes Atlas 10th Edition 2021. China Diabetes Report 2000–2045. Available online: https://diabetesatlas.org/data/en/country/42/cn.html (accessed on 13 December 2021).
- Guaraldi, F.; Montalti, M.; Di Valerio, Z.; Mannucci, E.; Nreu, B.; Monami, M.; Gori, D. Rate and Predictors of Hesitancy toward SARS-CoV-2 Vaccine among Type 2 Diabetic Patients: Results from an Italian Survey. Vaccines 2021, 9, 460. [Google Scholar] [CrossRef]
- Aldossari, K.K.; Alharbi, M.B.; Alkahtani, S.M.; Alrowaily, T.Z.; Alshaikhi, A.M.; Twair, A.A. COVID-19 vaccine hesitancy among patients with diabetes in Saudi Arabia. Diabetes Metab. Syndr. 2021, 15, 102271. [Google Scholar] [CrossRef]
- Scoccimarro, D.; Panichi, L.; Ragghianti, B.; Silverii, A.; Mannucci, E.; Monami, M. SARS-CoV-2 vaccine hesitancy in Italy: A survey on subjects with diabetes. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 3243–3246. [Google Scholar] [CrossRef]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 Vaccination during the COVID-19 Pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef]
- Wang, J.; Yuan, B.; Lu, X.; Liu, X.; Li, L.; Geng, S.; Zhang, H.; Lai, X.; Lyu, Y.; Feng, H. Willingness to accept COVID-19 vaccine among the elderly and the chronic disease population in China. Hum. Vaccines Immunother. 2021, 1–16. [Google Scholar] [CrossRef]
- Bartsch, S.M.; O′Shea, K.J.; Ferguson, M.C.; Bottazzi, M.E.; Wedlock, P.T.; Strych, U.; McKinnell, J.A.; Siegmund, S.S.; Cox, S.N.; Hotez, P.J. Vaccine Efficacy Needed for a COVID-19 Coronavirus Vaccine to Prevent or Stop an Epidemic as the Sole Intervention. Am. J. Prev. Med. 2020, 59, 493–503. [Google Scholar] [CrossRef]
- Ali, H.; Alterki, A.; Sindhu, S.; Alahmad, B.; Hammad, M.; Al-Sabah, S.; Alghounaim, M.; Jamal, M.H.; Aldei, A.; Mairza, M.J. Robust Antibody Levels in Both Diabetic and Non-Diabetic Individuals After BNT162b2 mRNA COVID-19 Vaccination. Front. Immunol. 2021, 12, 752233. [Google Scholar] [CrossRef]
- Karamese, M.; Tutuncu, E.E. The effectiveness of inactivated SARS-CoV-2 vaccine (CoronaVac) on antibody response in participants aged 65 years and older. J. Med. Virol. 2022, 94, 173–177. [Google Scholar] [CrossRef]
- WHO. Interim Recommendations for Use of the ChAdOx1-S [Recombinant] Vaccine against COVID-19 (AstraZeneca COVID-19 Vaccine AZD1222 Vaxzevria™, SII COVISHIELD™): Interim Guidance, First Issued 10 February 2021, Updated 21 April 2021, Last Updated 30 July 2021. Available online: https://apps.who.int/iris/handle/10665/343388 (accessed on 23 October 2021).
- European Centre for Disease Prevention and Control. COVID-19 Vaccination and Prioritisation Strategies in the EU/EEA. Available online: https://www.ecdc.europa.eu/en/publications-data/covid-19-vaccination-and-prioritisation-strategies-eueea (accessed on 2 September 2021).
- Diabetes UK. Updates: Coronavirus and Diabetes. Available online: https://www.diabetes.org.uk/about_us/news/coronavirus (accessed on 26 October 2021).
- Powers, A.C.; Aronoff, D.M.; Eckel, R.H. COVID-19 vaccine prioritisation for type 1 and type 2 diabetes. Lancet Diabetes Endocrinol. 2021, 9, 140–141. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. The Advisory Committee on Immunization Practices’ Updated Interim Recommendation for Allocation of COVID-19 Vaccine—United States, December 2020. Available online: https://www.cdc.gov/mmwr/volumes/69/wr/mm695152e2.htm (accessed on 26 October 2021).
- Korea Centers for Disease Control and Prevention Who First Gets the COVID-19 Vaccination? 2021. Available online: https://ncv.kdca.go.kr/menu.es?mid=a10117010000 (accessed on 14 August 2021).
- National Health Commission of the People’s Republic of China. New Coronavirus Vaccination Technical Guide (First Edition). Available online: https://xueshu.baidu.com/usercenter/paper/show?paperid=1a4x02c0rb0q0p00786n0mf0bj229634&site=xueshu_se (accessed on 30 April 2021).
- Syed Alwi, S.A.R.; Rafidah, E.; Zurraini, A.; Juslina, O.; Brohi, I.B.; Lukas, S. A survey on COVID-19 vaccine acceptance and concern among Malaysians. BMC Public Health 2021, 21, 1129. [Google Scholar] [CrossRef]
- Bongomin, F.; Olum, R.; Andia-Biraro, I.; Nakwagala, F.N.; Hassan, K.H.; Nassozi, D.R.; Kaddumukasa, M.; Byakika-Kibwika, P.; Kiguli, S.; Kirenga, B.J. COVID-19 vaccine acceptance among high-risk populations in Uganda. Ther. Adv. Infect. Dis. 2021, 8, 20499361211024376. [Google Scholar] [CrossRef]
- Carico, R.R., Jr.; Sheppard, J.; Thomas, C.B. Community pharmacists and communication in the time of COVID-19: Applying the health belief model. Res. Soc. Adm. Pharm. 2021, 17, 1984–1987. [Google Scholar] [CrossRef]
- Carpenter, C.J. A meta-analysis of the effectiveness of health belief model variables in predicting behavior. Health Commun. 2010, 25, 661–669. [Google Scholar] [CrossRef] [Green Version]
- Harrison, J.A.; Mullen, P.D.; Green, L.W. A meta-analysis of studies of the Health Belief Model with adults. Health Educ. Res. 1992, 7, 107–116. [Google Scholar] [CrossRef]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef]
- Wong, M.C.S.; Wong, E.L.Y.; Huang, J.; Cheung, A.W.L.; Law, K.; Chong, M.K.C.; Ng, R.W.Y.; Lai, C.K.C.; Boon, S.S.; Lau, J.T.F. Acceptance of the COVID-19 vaccine based on the health belief model: A population-based survey in Hong Kong. Vaccine 2021, 39, 1148–1156. [Google Scholar] [CrossRef]
- Wong, L.P.; Alias, H.; Wong, P.F.; Lee, H.Y.; AbuBakar, S. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Hum. Vaccines Immunother. 2020, 16, 2204–2214. [Google Scholar] [CrossRef]
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.; Fouayzi, H.; Mazor, K.M. Attitudes Toward a Potential SARS-CoV-2 Vaccine: A Survey of U.S. Adults. Ann. Intern. Med. 2020, 173, 964–973. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Al-Hanawi, M.K.; Ahmad, K.; Haque, R.; Keramat, S.A. Willingness to receive COVID-19 vaccination among adults with chronic diseases in the Kingdom of Saudi Arabia. J. Infect. Public Health 2021, 14, 1489–1496. [Google Scholar] [CrossRef]
- Robinson, E.; Jones, A.; Lesser, I.; Daly, M. International estimates of intended uptake and refusal of COVID-19 vaccines: A rapid systematic review and meta-analysis of large nationally representative samples. Vaccine 2021, 39, 2024–2034. [Google Scholar] [CrossRef]
- Bi, X.; Zhang, Q.; Fan, K.; Tang, S.; Guan, H.; Gao, X.; Cui, Y.; Ma, Y.; Wu, Q.; Hao, Y. Risk Culture and COVID-19 Protective Behaviors: A Cross-Sectional Survey of Residents in China. Front. Public Health 2021, 9, 686705. [Google Scholar] [CrossRef]
- Al-Hasan, A.; Khuntia, J.; Yim, D. Does Seeing What Others Do Through Social Media Influence Vaccine Uptake and Help in the Herd Immunity Through Vaccination? A Cross-Sectional Analysis. Front. Public Health 2021, 9, 715931. [Google Scholar] [CrossRef]
- Lau, A.Y.; Sintchenko, V.; Crimmins, J.; Magrabi, F.; Gallego, B.; Coiera, E. Impact of a web-based personally controlled health management system on influenza vaccination and health services utilization rates: A randomized controlled trial. J. Am. Med. Inform. Assoc. 2012, 19, 719–727. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristic | All Participants (n = 483) x ± S | Participants Willing to Receive SARS-CoV-2 Vaccine (n = 210) x ± S | Participants Hesitant to Receive SARS CoV-2 Vaccine (n = 273) x ± S | Hesitant vs. Willing Participants, c OR/t (95% CI) | p-Value |
|---|---|---|---|---|---|
| Sex | |||||
| Male | 252 (52.2) | 114 (54.3) | 138 (50.5) | 1.0 | Ref |
| Female | 231 (47.8) | 96 (45.7) | 135 (49.5) | 0.86 (0.60–1.24) | 0.42 |
| Average age, years | |||||
| 56.43 ± 13.03 | 56.41 ± 12.37 | 56.45 ± 13.54 | −0.03 (−2.39–2.31) | 0.97 | |
| Age group, years | |||||
| 18–39 | 50 (10.4) | 19 (9.0) | 31 (11.4) | 1.0 | Ref |
| 40–49 | 78 (16.1) | 43 (20.5) | 35 (12.8) | 1.21 (0.56–2.49) | 0.61 |
| 50–59 | 143 (29.6) | 59 (28.1) | 84 (30.8) | 0.60 (0.32–1.13) | 0.11 |
| 60–69 | 132 (27.3) | 55 (26.2) | 77 (28.2) | 1.05 (0.60–1.83) | 0.86 |
| ≥70 | 80 (16.6) | 34 (16.2) | 46 (16.8) | 1.03 (0.59–1.82) | 0.91 |
| Ethnicity | |||||
| Han | 475 (98.3) | 209 (99.5) | 266 (97.4) | 1.0 | Ref |
| Other | 8 (1.7) | 1 (0.5) | 7 (2.6) | 0.18 (0.02–1.49) | 0.11 |
| Education level | |||||
| Below high school | 288 (59.6) | 114 (54.3) | 174 (63.7) | 1.0 | Ref |
| High school | 95 (19.7) | 45 (21.4) | 50 (18.3) | 1.59 (1.01–2.51) | 0.05 |
| College and above | 100 (20.7) | 51 (24.3) | 49 (17.9) | 1.16 (0.66–2.03) | 0.61 |
| Marital status | |||||
| Unmarried, divorced, separated, or widowed | 59 (12.2) | 22 (10.5) | 37 (13.6) | 1.0 | Ref |
| Married or cohabitating | 424 (87.8) | 188 (89.5) | 236 (86.4) | 1.34 (0.76–2.35) | 0.31 |
| Occupation type | |||||
| Farmer | 210 (43.5) | 92 (43.8) | 118 (43.2) | 1.0 | Ref |
| Public institution personnel | 90 (18.6) | 49 (23.3) | 41 (15.0) | 0.65 (0.40–1.07) | 0.09 |
| Business staff | 55 (11.4) | 17 (8.1) | 38 (13.9) | 1.74 (0.93–3.28) | 0.08 |
| Worker | 74 (15.3) | 32 (15.2) | 42 (15.4) | 1.02 (0.60–1.75) | 0.93 |
| Transportation staff | 29 (6.0) | 11 (5.2) | 18 (6.6) | 1.28 (0.57–2.83) | 0.55 |
| Other | 25 (5.2) | 9 (4.3) | 16 (5.9) | 1.39 (0.59–3.28) | 0.46 |
| Residence | |||||
| Urban | 267 (55.3) | 115(54.8) | 152 (55.7) | 1.0 | Ref |
| Rural | 216 (44.7) | 95 (45.2) | 121 (44.3) | 1.04 (0.72–1.49) | 0.84 |
| Monthly personal income (Chinese yuan †) | |||||
| <2000 | 205 (42.4) | 85 (40.5) | 120 (44.0) | 1.0 | Ref |
| 2000–3499 | 142 (29.4) | 58 (27.6) | 84 (30.8) | 0.92 (0.47–1.81) | 0.82 |
| 3500–4999 | 93 (19.3) | 50 (23.8) | 43 (15.8) | 0.95 (0.47–1.90) | 0.88 |
| ≥5000 | 43 (8.9) | 17 (8.1) | 26 (9.5) | 0.56 (0.27–1.17) | 0.13 |
| Type of insurance | |||||
| Urban worker | 228 (47.2) | 108 (51.4) | 120 (44.0) | 1.0 | Ref |
| Urban residents | 113 (23.4) | 41 (19.5) | 72 (26.4) | 0.84 (0.55–1.28) | 0.41 |
| New Rural Cooperative Medical Scheme | 142 (29.4) | 61 (29.0) | 81 (29.7) | 1.32 (0.80-2.20) | 0.28 |
| Condition | All Participants (n = 483) x ± S | Participants Willing to Receive SARS-CoV-2 Vaccine x ± S (n = 210) | Participants Hesitant to Receive SARS-CoV-2 Vaccine x ± S (n = 273) | Hesitant vs. Willing Participants, c OR/t (95% CI) | p-Value |
|---|---|---|---|---|---|
| Current smoker | |||||
| No | 145 (30.0) | 61 (29.0) | 84 (30.8) | 1.0 | Ref |
| Yes | 338 (70.0) | 149 (71.0) | 189 (69.2) | 1.10 (0.73–1.61) | 0.68 |
| Current drinker | |||||
| No | 121 (25.1) | 52 (24.8) | 69 (25.3) | 1.0 | Ref |
| Yes | 362 (74.9) | 158 (75.2) | 204 (74.7) | 1.03 (0.68–1.56) | 0.90 |
| Average self-reported BMI, kg/m2 | |||||
| 25.27 ± 4.85 | 25.16 ± 5.28 | 25.36 ± 4.50 | −0.44 (−1.07–0.68) | 0.66 | |
| Self–reported BMI, kg/m2 | |||||
| <18.5 | 55 (11.4) | 23 (11.0) | 32 (11.7) | 1.0 | Ref |
| 18.5–23.9 | 186 (38.5) | 88 (41.9) | 98 (35.9) | 0.86 (0.43–1.73) | 0.68 |
| 24.0–27.9 | 161 (33.3) | 68 (32.4) | 93 (34.1) | 0.69 (0.41–1.18) | 0.17 |
| ≥28 | 81 (16.8) | 31 (14.8) | 50 (18.3) | 0.85 (0.49–1.46) | 0.55 |
| Other chronic diseases | |||||
| No | 67 (13.9) | 35 (16.7) | 32 (11.7) | 1.0 | Ref |
| Yes | 416 (86.1) | 175 (83.3) | 241 (88.3) | 0.66 (0.40–1.11) | 0.12 |
| Diabetes complications | |||||
| No | 159 (32.9) | 73 (34.8) | 86 (31.5) | 1.0 | Ref |
| Yes | 324 (67.1) | 137 (65.2) | 187 (68.5) | 0.86 (0.59–1.27) | 0.45 |
| Controlled blood glucose level | |||||
| No | 262 (54.2) | 109 (51.9) | 153 (56.0) | 1.0 | Ref |
| Yes | 221 (45.8) | 101 (48.1) | 120 (44.0) | 1.18 (0.82–1.70) | 0.37 |
| Family history of diabetes | |||||
| No | 173 (35.8) | 74 (35.2) | 99 (36.3) | 1.0 | Ref |
| Yes | 310 (64.2) | 136 (64.8) | 174 (63.7) | 1.05 (0.72–1.52) | 0.82 |
| Average time since diabetes diagnosis, years | |||||
| 7.72 ± 7.29 | 7.58 ± 7.49 | 7.83 ± 7.14 | −0.37 (−1.57–1.07) | 0.71 | |
| Time since diabetes diagnosis, years | |||||
| ≤1 | 141 (29.2) | 63 (30.0) | 78 (28.6) | 1.0 | Ref |
| 2–10 | 196 (40.6) | 84 (40.0) | 112 (41.0) | 0.94 (0.59–1.50) | 0.79 |
| >10 | 146 (30.2) | 63 (30.0) | 83 (30.4) | 1.01 (0.66–1.56) | 0.96 |
| Average fasting blood glucose at most recent testing, mmol/L | |||||
| 8.67 ± 4.99 | 8.68 ± 6.75 | 8.66 ± 3.02 | 0.04 (−0.89–0.92) | 0.97 | |
| Fasting blood glucose at most recent testing, mmol/L | |||||
| <7 | 169 (35.0) | 77 (36.7) | 92 (33.7) | 1.0 | Ref |
| 7–13.9 | 276 (57.1) | 120 (57.1) | 156 (57.1) | 0.62 (0.30–1.30) | 0.21 |
| >13.9 | 38 (7.9) | 13 (6.2) | 25 (9.2) | 0.68 (0.33–1.38) | 0.28 |
| Average postprandial blood glucose at most recent testing, mmol/L | |||||
| 12.74 ± 11.60 | 12.32 ± 9.81 | 13.06 ± 12.83 | −0.69 (−2.84–1.36) | 0.49 | |
| Postprandial blood glucose at most recent testing, mmol/L | |||||
| <10 | 159 (32.9) | 68 (32.4) | 91 (33.3) | 1.0 | Ref |
| 10–11.1 | 87 (18.0) | 46 (21.9) | 41 (15.0) | 0.91 (0.61–1.37) | 0.65 |
| >11.1 | 237 (49.1) | 96 (45.7) | 141 (51.6) | 0.66 (0.35–1.24) | 0.19 |
| Variable | All Participants (n = 483) | Participants Willing to Receive SARS-CoV-2 Vaccine (n = 210) | Participants Hesitant to Receive SARS-CoV-2 Vaccine (n = 273) | Hesitant vs. Willing Participant, c OR (95% CI) | p-Value |
|---|---|---|---|---|---|
| Willing to receive SARS-CoV-2 vaccine | |||||
| No (unwilling or unsure) | 273 (56.4) | 0 (0) | 273 (100) | N/A | N/A |
| Yes (willing) | 210 (43.6) | 210 (100) | 0 (0) | N/A | N/A |
| Perceived susceptibility | |||||
| Risk of acquiring SARS-CoV-2 is high | |||||
| No (strongly disagree or disagree or neutral) | 371 (76.8) | 157 (74.8) | 214 (78.4) | 1.0 | Ref |
| Yes (agree or strongly agree) | 112 (23.2) | 53 (25.2) | 59 (21.6) | 1.22 (0.80–1.87) | 0.35 |
| Perceived severity | |||||
| SARS-CoV-2 syndrome is severe | |||||
| No (strongly disagree or disagree or neutral) | 329 (68.1) | 177 (84.3) | 152 (55.7) | 1.0 | Ref |
| Yes (agree or strongly agree) | 154 (31.9) | 33 (15.7) | 121 (44.3) | 4.27 (2.75–6.64) | <0.001 |
| Perceived benefits | |||||
| Vaccination reduces the risk of infection | |||||
| Yes (agree or strongly agree) | 164 (34.0) | 89 (42.4) | 75 (27.5) | 1.0 | Ref |
| No (strongly disagree or disagree or neutral) | 319 (66.0) | 121 (57.6) | 198 (72.5) | 1.94 (1.33–2.84) | 0.001 |
| Vaccination reduces the risk of transmission to other people | |||||
| Yes (agree or very agree) | 297 (61.5) | 149 (71.0) | 148 (54.2) | 1.0 | Ref |
| No (strongly disagree or disagree or neutral) | 186 (38.5) | 61 (29.0) | 125 (45.8) | 2.06 (1.41–3.02) | <0.001 |
| Vaccination is good for myself and others | |||||
| Yes (agree or strongly agree) | 463 (95.9) | 202 (96.2) | 261 (95.6) | 1.0 | Ref |
| No (strongly disagree or disagree or neutral) | 20 (4.1) | 8 (3.8) | 12 (4.4) | 1.16 (0.47–2.89) | 0.75 |
| Perceived barriers | |||||
| As a person with diabetes, I worry about the safety of the SARS-CoV-2 vaccine | |||||
| No (strongly disagree or disagree or neutral) | 146 (30.2) | 95 (45.2) | 51 (18.7) | 1.0 | Ref |
| Yes (agree or strongly agree) | 337 (69.8) | 115 (54.8) | 222 (81.3) | 3.60 (2.39–5.41) | <0.001 |
| I am worried about side effects of vaccination | |||||
| No (strongly disagree or disagree or neutral) | 200 (41.4) | 116 (55.2) | 84 (30.8) | 1.0 | Ref |
| Yes (agree or strongly agree) | 283 (58.6) | 94 (44.8) | 189 (69.2) | 2.77 (1.91–4.04) | <0.001 |
| Action clues | |||||
| Relatives’ vaccination status will affect my vaccination behavior | |||||
| Yes (agree or strongly agree) | 85 (17.6) | 52 (24.8) | 33 (12.1) | 1.0 | Ref |
| No (strongly disagree or disagree or neutral) | 398 (82.4) | 158 (75.2) | 240 (87.9) | 2.40 (1.48–3.87) | <0.001 |
| I accept physicians’ view that vaccination can reduce the risk of infection | |||||
| Yes (agree or strongly agree) | 253 (52.4) | 150 (71.4) | 103 (37.7) | 1.0 | Ref |
| No (strongly disagree or disagree or neutral) | 230 (47.6) | 60 (28.6) | 170 (62.3) | 4.13 (2.80–6.07) | <0.001 |
| I have received advice on vaccination from the internet/media | |||||
| Yes (agree or strongly agree) | 233 (48.2) | 124 (59.0) | 109 (39.9) | 1.0 | Ref |
| No (strongly disagree or disagree or neutral) | 250 (51.8) | 86 (41.0) | 164 (60.1) | 2.17 (1.50–3.13) | <0.001 |
| Variable | a OR (95%CI) † | p-Value |
|---|---|---|
| Perceived susceptibility | ||
| Risk of acquiring SARS-CoV-2 is high | ||
| No (strongly disagree or disagree or neutral) | 1.0 | Ref |
| Yes (agree or strongly agree) | 0.79 (0.47–1.32) | 0.36 |
| Perceived severity | ||
| SARS-CoV-2 syndrome is severe | ||
| No (strongly disagree or disagree or neutral) | 1.0 | Ref |
| Yes (agree or strongly agree) | 3.90 (2.36–6.42) | <0.001 |
| Perceived benefits | ||
| Vaccination reduces the risk of infection | ||
| Yes (agree or strongly agree) | 1.0 | Ref |
| No (strongly disagree or disagree or neutral) | 0.65 (0.41–1.03) | 0.07 |
| Vaccination reduces the risk of transmission to other people | ||
| Yes (agree or very agree) | 1.0 | Ref |
| No (strongly disagree or disagree or neutral) | 1.22 (0.77–1.94) | 0.40 |
| Vaccination is good for myself and others | ||
| Yes (agree or strongly agree) | 1.0 | Ref |
| No (strongly disagree or disagree or neutral) | 1.09 (0.40–2.99) | 0.87 |
| Perceived barriers | ||
| As a person with diabetes, I worry about the safety of the SARS-CoV-2 vaccine | ||
| No (strongly disagree or disagree or neutral) | 1.0 | Ref |
| Yes (agree or strongly agree) | 3.05 (1.89–4.91) | <0.001 |
| I am worried about side effects of vaccination | ||
| No (strongly disagree or disagree or neutral) | 1.0 | Ref |
| Yes (agree or strongly agree) | 0.71 (0.41–1.25) | 0.24 |
| Action clues | ||
| Relatives’ vaccination status will affect my vaccination behavior | ||
| Yes (agree or strongly agree) | 1.0 | Ref |
| No (strongly disagree or disagree or neutral) | 2.43 (1.39–4.25) | 0.002 |
| I accept physicians’ view that vaccination can reduce the risk of infection | ||
| Yes (agree or strongly agree) | 1.0 | Ref |
| No (strongly disagree or disagree or neutral) | 2.25 (1.28–3.95) | 0.005 |
| I have received advice on vaccination from the internet/media | ||
| Yes (agree or strongly agree) | 1.0 | Ref |
| No (strongly disagree or disagree or neutral) | 1.29 (0.83–2.00) | 0.26 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Duan, L.; Li, M.; Wang, J.; Yang, J.; Song, C.; Li, J.; Wang, J.; Jia, J.; Xu, J. COVID-19 Vaccine Hesitancy and Associated Factors among Diabetes Patients: A Cross-Sectional Survey in Changzhi, Shanxi, China. Vaccines 2022, 10, 129. https://doi.org/10.3390/vaccines10010129
Wang Y, Duan L, Li M, Wang J, Yang J, Song C, Li J, Wang J, Jia J, Xu J. COVID-19 Vaccine Hesitancy and Associated Factors among Diabetes Patients: A Cross-Sectional Survey in Changzhi, Shanxi, China. Vaccines. 2022; 10(1):129. https://doi.org/10.3390/vaccines10010129
Chicago/Turabian StyleWang, Ying, Lingrui Duan, Mufan Li, Jiayu Wang, Jianzhou Yang, Congying Song, Jing Li, Jinsheng Wang, Jiantao Jia, and Junjie Xu. 2022. "COVID-19 Vaccine Hesitancy and Associated Factors among Diabetes Patients: A Cross-Sectional Survey in Changzhi, Shanxi, China" Vaccines 10, no. 1: 129. https://doi.org/10.3390/vaccines10010129