
Atypical Kawasaki Disease after COVID-19 Vaccination: A New Form of Adverse Event Following Immunization

 ,
, 
Abstract
:1. Introduction
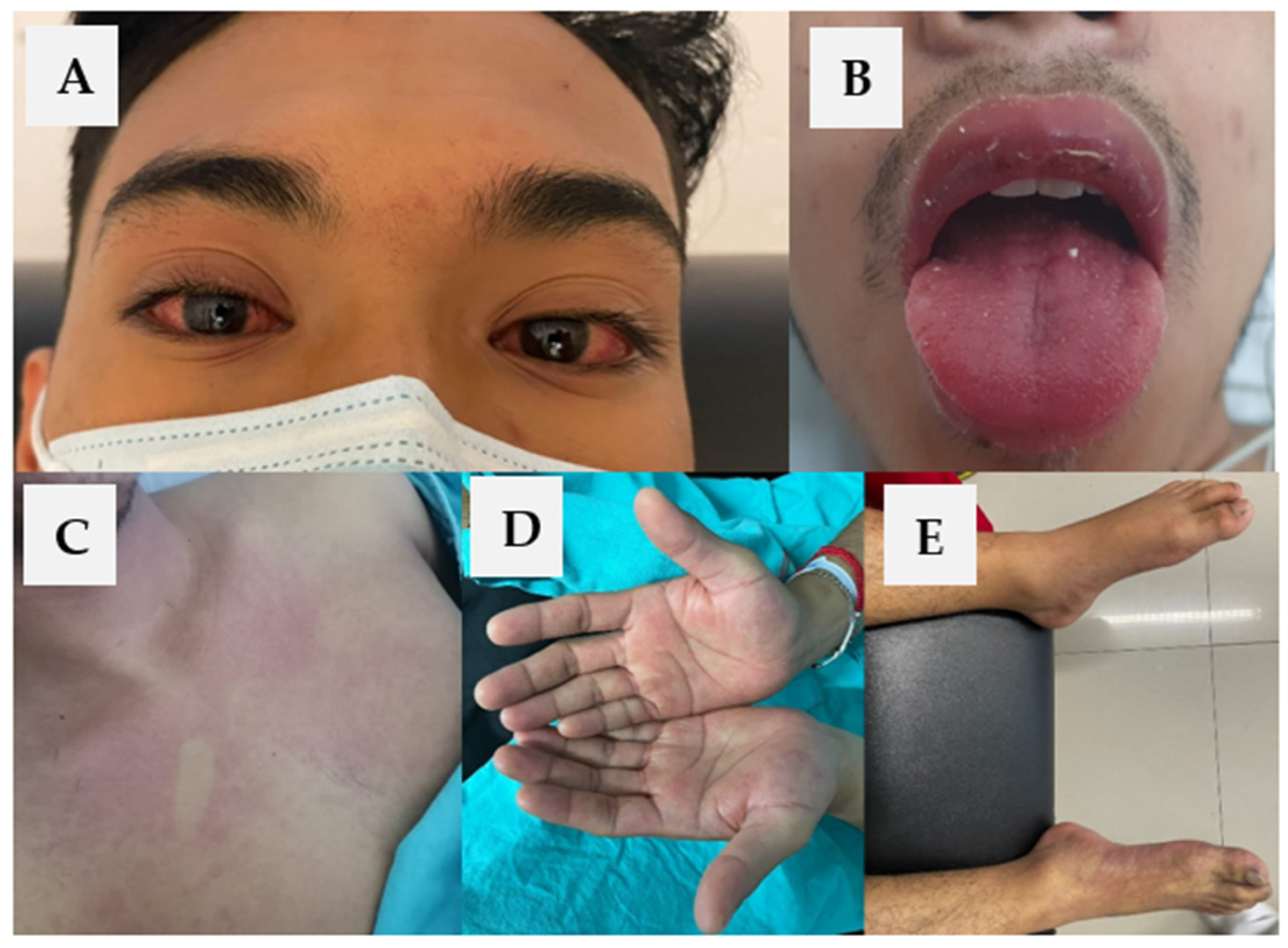
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Moghadas, S.M.; Vilches, T.N.; Zhang, K.; Wells, C.R.; Shoukat, A.; Singer, B.H.; Meyers, L.A.; Neuzil, K.M.; Langley, J.M.; Fitzpatrick, M.C.; et al. The Impact of Vaccination on Coronavirus Disease 2019 (COVID-19) Outbreaks in the United States. Clin. Infect. Dis. 2021, 73, 2257–2264. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.J.; Moreira, E.D., Jr.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Polack, F.P.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine through 6 Months. N. Engl. J. Med. 2021, 385, 1761–1773. [Google Scholar] [CrossRef] [PubMed]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Puliyel, J.; Naik, P. Revised World Health Organization (WHO)’s causality assessment of adverse events following immunization—A critique. F1000Research 2018, 7, 243. [Google Scholar] [CrossRef] [PubMed]
- Radice, A.; Carli, G.; Macchia, D.; Farsi, A. Allergic reactions after vaccination: Translating guidelines into clinical practice. Eur. Ann. Allergy Clin. Immunol. 2018, 51, 51–61. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Causality Assessment of an Adverse Event Following Immunization (AEFI): User Manual for the Revised WHO Classification, 2nd ed.; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- European Medicines Agency. Pharmacovigilance Plan of the EU Regulatory Network for COVID-19 Vaccines. Published 13 November 2020. Available online: https://www.ema.europa.eu/en/documents/other/pharmacovigilance-plan-eu-regulatory-network-covid-19-vaccines_en.pdf (accessed on 11 December 2021).
- Sampath, V.; Rabinowitz, G.; Shah, M.; Jain, S.; Diamant, Z.; Jesenak, M.; Rabin, R.; Vieths, S.; Agache, I.; Akdis, M.; et al. Vaccines and allergic reactions: The past, the current COVID-19 pandemic, and future perspectives. Allergy 2021, 76, 1640–1660. [Google Scholar] [CrossRef] [PubMed]
- Hua, W.; Izurieta, H.S.; Slade, B.; Belay, E.D.; Haber, P.; Tiernan, R.; Woo, E.J.; Iskander, J.; Braun, M.M.; Ball, R. Kawasaki Disease after Vaccination: Reports to the vaccine adverse event reporting system 1990–2007. Pediatr. Infect. Dis. J. 2009, 28, 943–947. [Google Scholar] [CrossRef] [PubMed]
- Drago, F.; Javor, S.; Ciccarese, G.; Cozzani, E.; Parodi, A. A Case of Complete Adult-Onset Kawasaki Disease: A Review of Pathogenesis and Classification. Dermatology 2015, 231, 5–8. [Google Scholar] [CrossRef] [PubMed]
- Newburger, J.W.; Takahashi, M.; Burns, J.C. Kawasaki Disease. J. Am. Coll. Cardiol. 2016, 67, 1738–1749. [Google Scholar] [CrossRef]
- Sève, P.; Stankovic, K.; Smail, A.; Durand, D.V.; Marchand, G.; Broussolle, C. Adult Kawasaki Disease: Report of Two Cases and Literature Review. Semin. Arthritis Rheum. 2005, 34, 785–792. [Google Scholar] [CrossRef]
- Burgner, D.; Harnden, A. Kawasaki disease: What is the epidemiology telling us about the etiology? Int. J. Infect. Dis. 2005, 9, 185–194. [Google Scholar] [CrossRef] [Green Version]
- Nasr, I.; Tometzki, A.J.P.; Schofield, O.M.V. Kawasaki disease: An update. Clin. Exp. Dermatol. 2001, 26, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Tseng, H.F.; Sy, L.S.; Liu, I.-L.A.; Qian, L.; Marcy, S.M.; Weintraub, E.; Yih, K.; Baxter, R.; Glanz, J.M.; Donahue, J.; et al. Postlicensure surveillance for pre-specified adverse events following the 13-valent pneumococcal conjugate vaccine in children. Vaccine 2013, 31, 2578–2583. [Google Scholar] [CrossRef] [PubMed]
- Stowe, J.; Andrews, N.J.; Turner, P.J.; Miller, E. The risk of Kawasaki disease after pneumococcal conjugate & meningococcal B vaccine in England: A self-controlled case-series analysis. Vaccine 2020, 38, 4935–4939. [Google Scholar] [CrossRef] [PubMed]
- Bellavite, P. Causality assessment of adverse events following immunization: The problem of multifactorial pathology. F1000Research 2020, 9, 170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, S.; Zimba, O.; Gasparyan, A.Y. COVID-19 and the clinical course of rheumatic manifestations. Clin. Rheumatol. 2021, 40, 2611–2619. [Google Scholar] [CrossRef] [PubMed]
- Watad, A.; De Marco, G.; Mahajna, H.; Druyan, A.; Eltity, M.; Hijazi, N.; Haddad, A.; Elias, M.; Zisman, D.; Naffaa, M.; et al. Immune-Mediated Disease Flares or New-Onset Disease in 27 Subjects Following mRNA/DNA SARS-CoV-2 Vaccination. Vaccines 2021, 9, 435. [Google Scholar] [CrossRef] [PubMed]
- Vera-Lastra, O.; Navarro, A.O.; Domiguez, M.P.C.; Medina, G.; Valadez, T.I.S.; Jara, L.J. Two Cases of Graves’ Disease Following SARS-CoV-2 Vaccination: An Autoimmune/Inflammatory Syndrome Induced by Adjuvants. Thyroid 2021, 31, 1436–1439. [Google Scholar] [CrossRef] [PubMed]
- Sharma, C.; Ganigara, M.; Galeotti, C.; Burns, J.; Berganza, F.M.; Hayes, D.A.; Singh-Grewal, D.; Bharath, S.; Sajjan, S.; Bayry, J. Multisystem inflammatory syndrome in children and Kawasaki disease: A critical comparison. Nat. Rev. Rheumatol. 2021, 17, 731–748. [Google Scholar] [CrossRef] [PubMed]
- Forsey, J.; Mertens, L. Atypical Kawasaki disease—A clinical challenge. Eur. J. Nucl. Med. Mol. Imaging 2011, 171, 609–611. [Google Scholar] [CrossRef] [PubMed]
- Ueda, Y.; Kenzaka, T.; Noda, A.; Yamamoto, Y.; Matsumura, M. Adult-onset Kawasaki disease (mucocutaneous lymph node syndrome) and concurrent Coxsackievirus A4 infection: A case report. Int. Med. Case Rep. J. 2015, 8, 225–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stefanizzi, P.; Bianchi, F.P.; Spinelli, G.; Amoruso, F.; Ancona, D.; Stella, P.; Tafuri, S. Postmarketing surveillance of adverse events following meningococcal B vaccination: Data from Apulia Region, 2014–19. Hum. Vaccines Immunother. 2021, 1–6. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Blood Test | Value | Reference Ranges |
|---|---|---|
| Kidney Function | ||
| Creatinine | 2.7 mg/dL | 0.5–0.9 mg/dL |
| Liver Function | ||
| Lactate dehydrogenase (LDH) | 1069 U/L | 300 U/L |
| Alanine aminotransferase (ALT) | 155 U/L | 13–40 U/L |
| Aspartate aminotransferase (AST) | 286 U/L | 15–48 U/L |
| GGT | 688 U/L | 250 U/L |
| Total Bilirrubin | 14.9 mg/dL | 0.2–1.2 mg/dL |
| Direct Bilirrubin | 11.7 mg/dL | 0.0–0.3 mg/dL |
| Albumin | 2.6 g/dL | 3.5–4.5 mg/dL |
| Coagulation Tests | ||
| Prothrombin time (PT) | 28.8 s | 11 s |
| Partial thromboplastin time (PTT) | 35.6 s | 33 s |
| Complete Blood Count | ||
| Hemoglobin | 14.9 g/dL | 12–18 g/dL |
| Platelets | 39,400 per mL | 150,000–450,000 per mL |
| Leukocyte | 19.6 K/mcl | 4.5–10 K/mcl |
| Neutrophils | 88.2% | 50–70% |
| Lymphocytes | 2.8% | 17–45% |
| Monocytes | 2.5% | 4–12% |
| Eosinophils | 5.9% | 1–4% |
| Basophils | 0.5% | 1–2% |
| C-reactive protein (CRP) | 80.8 mg/dL | 0.00–5.00 mg/dL |
| Autoimmune Tests | ||
| Antinuclear antibodies (ANA) | 1:80 | Negative |
| Anticardiolipin IgM, IgG antibodies | Negative | Negative |
| Lupus Anticoagulant (LA) | Negative | Negative |
| Serological Markers | ||
| HIV | Negative | Negative |
| Hepatitis B (HBV) | Negative | Negative |
| Hepatitis C (HCV) | Negative | Negative |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peralta-Amaro, A.L.; Tejada-Ruiz, M.I.; Rivera-Alvarado, K.L.; Cobos-Quevedo, O.d.J.; Romero-Hernández, P.; Macías-Arroyo, W.; Avendaño-Ponce, A.; Hurtado-Díaz, J.; Vera-Lastra, O.; Lucas-Hernández, A. Atypical Kawasaki Disease after COVID-19 Vaccination: A New Form of Adverse Event Following Immunization. Vaccines 2022, 10, 126. https://doi.org/10.3390/vaccines10010126
Peralta-Amaro AL, Tejada-Ruiz MI, Rivera-Alvarado KL, Cobos-Quevedo OdJ, Romero-Hernández P, Macías-Arroyo W, Avendaño-Ponce A, Hurtado-Díaz J, Vera-Lastra O, Lucas-Hernández A. Atypical Kawasaki Disease after COVID-19 Vaccination: A New Form of Adverse Event Following Immunization. Vaccines. 2022; 10(1):126. https://doi.org/10.3390/vaccines10010126
Chicago/Turabian StylePeralta-Amaro, Ana Lilia, Melina Ivone Tejada-Ruiz, Karen Lilian Rivera-Alvarado, Orestes de Jesús Cobos-Quevedo, Patricia Romero-Hernández, Wiliams Macías-Arroyo, Alberto Avendaño-Ponce, Jorge Hurtado-Díaz, Olga Vera-Lastra, and Abihai Lucas-Hernández. 2022. "Atypical Kawasaki Disease after COVID-19 Vaccination: A New Form of Adverse Event Following Immunization" Vaccines 10, no. 1: 126. https://doi.org/10.3390/vaccines10010126