
Emerging Socioeconomic Disparities in COVID-19 Vaccine Second-Dose Completion Rates in the United States


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Vaccine Initiation and Completion
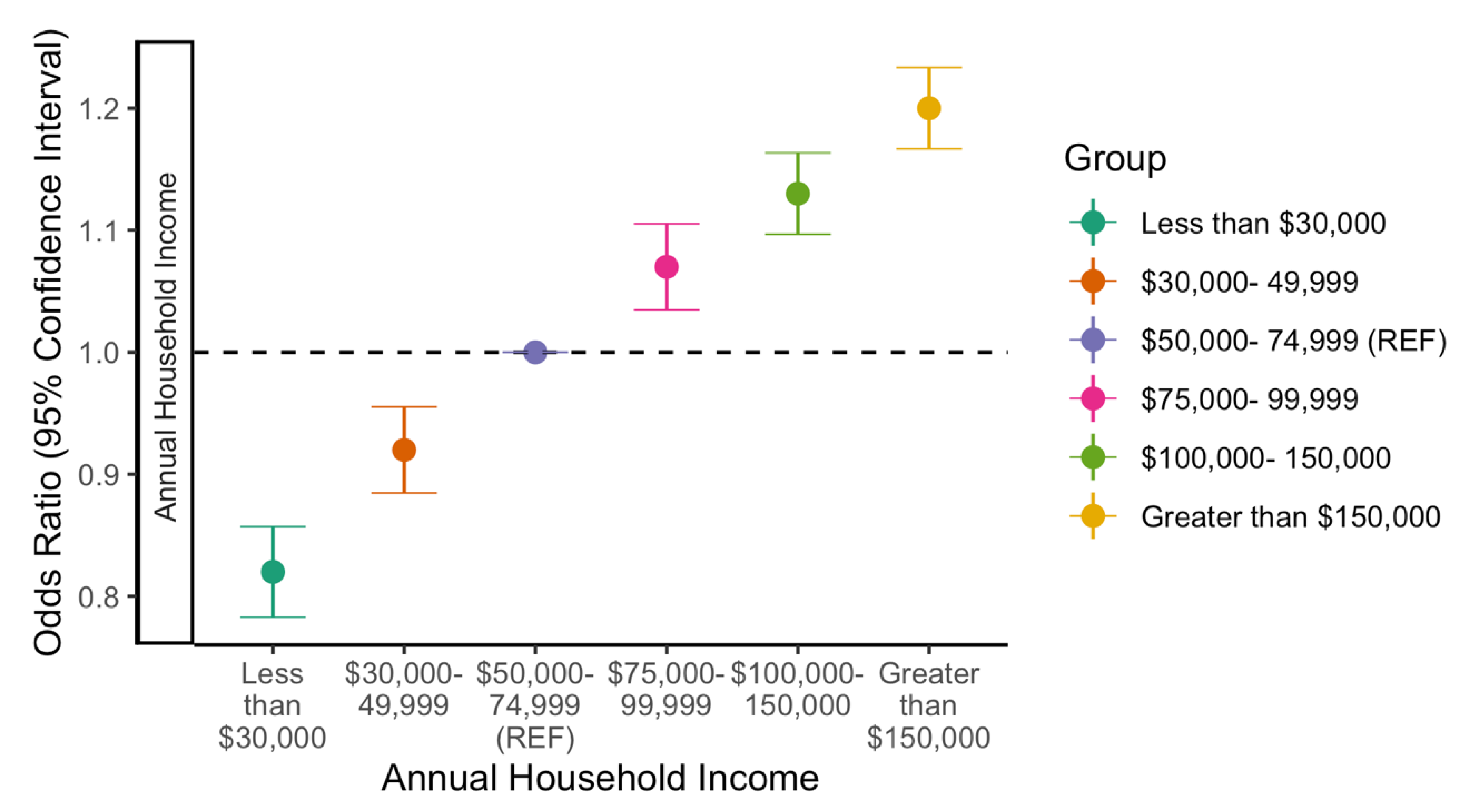
3.2. Likelihood to Complete Vaccination by Income
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jean-Jacques, M.; Bauchner, H. Vaccine Distribution—Equity Left Behind? JAMA 2021, 325, 829–830. [Google Scholar] [CrossRef] [PubMed]
- Walker, A.S.; Singhvi, A.; Holder, J.; Gebeloff, R.; Avila, Y.; Pandemic’s Racial Disparities Persist in Vaccine Rollout. The New York Times. Available online: https://www.nytimes.com/interactive/2021/03/05/us/vaccine-racial-disparities.html (accessed on 10 March 2021).
- Prins, W.; Butcher, E.; Hall, L.L.; Puckrein, G.; Rosof, B. Improving adult immunization equity: Where do the published research literature and existing resources lead? Vaccine 2017, 35, 3020–3025. [Google Scholar] [CrossRef] [PubMed]
- Murthy, B.P. Disparities in COVID-19 Vaccination Coverage between Urban and Rural Counties—United States, 14 December 2020–10 April 2021. MMWR Morb Mortal Wkly Rep. 2021, 70, 759. [Google Scholar] [CrossRef] [PubMed]
- Diesel, J.; Sterrett, N.; Dasgupta, S. COVID-19 Vaccination Coverage among Adults—United States, 14 December 2020–22 May 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 922–927. [Google Scholar] [CrossRef] [PubMed]
- Bibbins-Domingo, K.; Petersen, M.; Havlir, D. Taking Vaccine to Where the Virus Is—Equity and Effectiveness in Coronavirus Vaccinations. JAMA Health Forum. 2021, 2, e210213. [Google Scholar] [CrossRef]
- Gallagher, K.E.; Kadokura, E.; Eckert, L.O.; Miyake, S.; Mounier-Jack, S.; Aldea, M. Factors Influencing Completion of Multi-Dose Vaccine Schedules in Adolescents: A Systematic Review. BMC Public Health. 2016, 16, 172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- CDC. Different COVID-19 Vaccines Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines.html (accessed on 21 July 2021).
- Whiteman, A. Demographic and Social Factors Associated with COVID-19 Vaccination Initiation among Adults Aged ≥65 Years—United States, 14 December 2020–10 April 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 725. [Google Scholar] [CrossRef] [PubMed]
- Painter, E.M.; Ussery, E.N.; Patel, A. Demographic Characteristics of Persons Vaccinated During the First Month of the COVID-19 Vaccination Program—United States, 14 December 2020–14 January 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 174–177. [Google Scholar] [CrossRef]
- ACIP. COVID-19 Vaccine Recommendations/CDC. Available online: https://www.cdc.gov/vaccines/hcp/acip-recs/vacc-specific/covid-19.html (accessed on 30 November 2021).
- Kriss, J.L.; Reynolds, L.E.; Wang, A.; Stokley, S.; Cole, M.M.; Harris, L.Q. COVID-19 Vaccine Second-Dose Completion and Interval Between First and Second Doses Among Vaccinated Persons—United States, 14 December 2020−14 February 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Treisman, R. Biden Says All Adults Will Be Vaccine Eligible by April 19. Available online: https://www.npr.org/sections/coronavirus-live-updates/2021/04/06/984745020/biden-will-direct-states-to-make-all-adults-vaccine-eligible-by-april-19 (accessed on 28 December 2021).
- Bebinger, M.; Farmer, B.; As COVID Vaccinations Slow, Parts of the U.S. Remain Far Behind 70% Goal. Available online: https://www.npr.org/sections/health-shots/2021/07/05/1013080128/as-covid-vaccinations-slow-parts-of-the-u-s-remain-far-behind-70-goal (accessed on 28 December 2021).
- Rader, B.; White, L.F.; Burns, M.R.; Chen, J.; Brilliant, J.; Cohen, J. Mask-wearing, and control of SARS-CoV-2 transmission in the USA: A cross-sectional study. Lancet Digit. Health 2021, 3, 148–157. [Google Scholar] [CrossRef]
- Krammer, F.; Srivastava, K.; Alshammary, H.; Amoako, A.A.; Awawda, M.H.; Beach, K.F. Antibody Responses in Seropositive Persons after a Single Dose of SARS-CoV-2 mRNA Vaccine. N. Engl. J. Med. 2021, 384, 1372–1374. [Google Scholar] [CrossRef] [PubMed]
- CDC. COVID-19 Booster Shot. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/booster-shot.html (accessed on 22 November 2021).
- Commissioner O of the Coronavirus (COVID-19) Update: FDA Expands Eligibility for COVID-19 Vaccine Boosters. FDA. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-expands-eligibility-covid-19-vaccine-boosters (accessed on 29 November 2021).
- Rader, B.; Astley, C.M.; Sewalk, K.; Delamater, P.L.; Cordiano, K.; Wronski, L. Spatial Accessibility Modeling of Vaccine Deserts as Barriers to Controlling SARS-CoV-2. medRxiv 2021, 21252858. [Google Scholar]
- CDC. COVID-19 Vaccination. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/no-cost.html (accessed on 17 December 2021).
- Niccolai, L.M.; Mehta, N.R.; Hadler, J.L. Racial/Ethnic and Poverty Disparities in Human Papillomavirus Vaccination Completion. Am. J. Prev. Med. 2011, 41, 428–433. [Google Scholar] [CrossRef] [PubMed]
- Cavaliere, A.F.; Zaami, S.; Pallottini, M. Flu and Tdap Maternal Immunization Hesitancy in Times of COVID-19: An Italian Survey on Multiethnic Sample. Vaccines 2021, 9, 1107. [Google Scholar] [CrossRef] [PubMed]
- Viswanath, K.; Bekalu, M.; Dhawan, D.; Pinnamaneni, R.; Lang, J.; McLoud, R. Individual and social determinants of COVID-19 vaccine uptake. BMC Public Health 2021, 21, 818. [Google Scholar] [CrossRef] [PubMed]
- Walker, G.; McCabe, T. Psychological defence mechanisms during the COVID-19 pandemic: A case series. Eur. J. Psychiatry 2021, 35, 41–45. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Demographic | Total a No. (%) | Dose Initiation b (95% MOE) c | Dose Completion b (95% MOE) c |
|---|---|---|---|
| Age (years) | |||
| 18–34 | 151,329 (17.9) | 43.1 (42.8–43.4) | 81.5 (81.1–81.9) |
| 35–44 | 134,326 (15.9) | 49.6 (49.2–50.0) | 83.8 (83.4–84.2) |
| 45–54 | 167,946 (19.9) | 59.4 (59.1–59.7) | 85.2 (84.9–85.5) |
| 55–64 | 193,074 (22.9) | 69.3 (69.0–69.6) | 85.7 (85.4–86.0) |
| ≥65 | 185,594 (22.0) | 82.1 (81.9–82.3) | 87.3 (87.1–87.5) |
| Missing | 11,716 (1.4) | Suppressed d | Suppressed d |
| Race | |||
| White | 557,068 (66.0) | 59.9 (59.7–60.1) | 85.7 (85.5–85.9) |
| Black | 115,265 (13.7) | 49.5 (49.0–50.0) | 81.4 (80.9–81.9) |
| Hispanic | 87,105 (10.3) | 52.3 (51.8–52.8) | 81.5 (81.0–82.0) |
| Asian | 40,563 (4.8) | 67.7 (67.0–68.4) | 84.6 (84.0–85.2) |
| Other | 43,984 (5.2) | 46.0 (45.3–46.7) | 83.5 (82.7–84.3) |
| Essential Worker | |||
| Yes | 379,082 (44.9) | 56.1 (55.9–56.3) | 85.6 (85.4–85.8) |
| No | 200,384 (23.7) | 60.9 (60.6–61.2) | 84.5 (84.2–84.8) |
| Missing | 264,519 (31.3) | 52.2 (50.1–54.3) | 86.3 (84.4–88.2) |
| Industry | |||
| Healthcare | 142,739 (16.9) | 73.3 (72.9–73.7) | 91.4 (91.1–91.7) |
| Education | 66,448 (7.9) | 66.8 (66.2–67.4) | 83.9 (83.4–84.4) |
| Government | 34,742 (4.1) | 66.6 (65.8–67.4) | 86.6 (85.9–87.3) |
| Other | 311,313 (36.9) | 53.8 (53.5–54.1) | 83.9 (83.6–84.2) |
| Missing | 288,743 (34.2) | 57.2 (56.9–57.5) | 83.5 (83.2–83.8) |
| Annual Household Income | |||
| <30,000 | 156,355 (18.5) | 43.6 (43.2–44.0) | 80.1 (79.7–80.5) |
| 30–49,999 | 117,278 (13.9) | 54.8 (54.4–55.2) | 83.3 (82.9–83.7) |
| 50–74,999 | 133,339 (15.8) | 59.4 (59.0–59.8) | 84.8 (84.4–85.2) |
| 75–99,999 | 110,193 (13.1) | 62.6 (62.2–63.0) | 85.7 (85.3–86.1) |
| 100–150,000 | 136,881 (16.2) | 65.7 (65.3–66.1) | 86.4 (86.1–86.7) |
| >150,000 | 134,168 (15.9) | 69.4 (69.0–69.8) | 87.6 (87.6–87.3) |
| Missing | 55,771 (6.6) | 63.5 (62.9–64.1) | 85.5 (85.0–86.0) |
| Health Insurance | |||
| Plan through employer | 399,956 (47.4) | 60.9 (60.7–61.1) | 85.7 (85.5–85.9) |
| Medicare | 171,949 (20.4) | 67.6 (67.3–67.9) | 85.5 (85.2–85.8) |
| Self-purchased plan | 91,780 (10.9) | 57.4 (56.9–57.9) | 84.8 (84.3–85.3) |
| Medicaid or Medi-Cal | 57,940 (6.9) | 41.0 (40.4–41.6) | 79.3 (78.5–80.1) |
| Tricare | 15,560 (1.8) | 59.4 (58.2–60.6) | 85.0 (83.9–86.1) |
| Other | 49,849 (5.9) | 53.9 (53.2–54.6) | 82.2 (81.5–82.9) |
| Uninsured | 45,970 (5.4) | 34.3 (33.6–35.0) | 77.4 (76.5–78.3) |
| Missing | 10,981 (1.3) | 48.1 (46.6–49.6) | 82.5 (81.0–84.0) |
| Political Party | |||
| Republican | 188,701 (22.4) | 53.3 (52.9–53.7) | 85.0 (84.7–85.3) |
| Democrat | 332,426 (39.4) | 68.2 (68.0–68.4) | 84.9 (84.7–85.1) |
| Independent | 281,350 (33.3) | 51.4 (51.1–51.7) | 83.6 (83.3–83.9) |
| Missing | 41,508 (4.9) | 55.1 (54.4–55.9) | 83.3 (83.1–84.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gertz, A.; Rader, B.; Sewalk, K.; Brownstein, J.S. Emerging Socioeconomic Disparities in COVID-19 Vaccine Second-Dose Completion Rates in the United States. Vaccines 2022, 10, 121. https://doi.org/10.3390/vaccines10010121
Gertz A, Rader B, Sewalk K, Brownstein JS. Emerging Socioeconomic Disparities in COVID-19 Vaccine Second-Dose Completion Rates in the United States. Vaccines. 2022; 10(1):121. https://doi.org/10.3390/vaccines10010121
Chicago/Turabian StyleGertz, Autumn, Benjamin Rader, Kara Sewalk, and John S. Brownstein. 2022. "Emerging Socioeconomic Disparities in COVID-19 Vaccine Second-Dose Completion Rates in the United States" Vaccines 10, no. 1: 121. https://doi.org/10.3390/vaccines10010121