
Immunogenicity of a Two-Dose Human Papillomavirus Vaccine Schedule in HIV-Infected Adolescents with Immune Reconstitution

 , ,
, ,
Abstract
:1. Introduction
2. Methods and Participants
2.1. Study Participants and Design
2.2. Immunogenicity Assessments
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sohn, A.H.; Kerr, S.; Hansudewechakul, R.; Gatechompol, S.; Chokephaibulkit, K.; Dang, H.L.D.; Tran, D.N.H.; Achalapong, J.; Teeratakulpisarn, N.; Chalermchockcharoenkit, A.; et al. Risk Factors for Human Papillomavirus Infection and Abnormal Cervical Cytology Among Perinatally Human Immunodeficiency Virus-Infected and Uninfected Asian Youth. Clin. Infect. Dis. 2018, 67, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Phanuphak, N.; Teeraananchai, S.; Hansudewechakul, R.; Gatechompol, S.; Chokephaibulkit, K.; Dang, H.L.D.; Tran, D.N.H.; Achalapong, J.; Teeratakulpisarn, N.; Sohn, A.H. Incidence and Persistence of High-risk Anogenital Human Papillomavirus Infection Among Female Youth With and Without Perinatally Acquired Human Immunodefiency Virus Infection: A 3-year Observational Cohort Study. Clin. Infect. Dis. 2020, 71, e270–e280. [Google Scholar] [CrossRef] [PubMed]
- Gatechompol, S.; Teeratakulpisarn, N.; Wittawatmongkol, O.; Teeraananchai, S.; Kerr, S.J.; Chalermchockcharoenkit, A.; Thamkhantho, M.; Singtoroj, T.; Phanuphak, N.; Sohn, A.H.; et al. Incidence, persistence, and factors associated with HPV infection among male adolescents with and without perinatally acquired HIV infection. JAIDS J. Acquir. Immune Defic. Syndr. 2020, 85, 553–560. [Google Scholar] [CrossRef]
- Zhan, Y.; Liu, X.; Feng, Y.; Wu, S.; Jiang, Y. Safety and efficacy of human papillomavirus vaccination for people living with HIV: A systematic review and meta-analysis. Int. J. STD AIDS 2019, 30, 1105–1115. [Google Scholar] [CrossRef]
- Garland, S.M.; Hernandez-Avila, M.; Wheeler, C.M.; Perez, G.; Harper, D.M.; Leodolter, S.; Tang, G.W.; Ferris, D.G.; Steben, M.; Bryan, J.; et al. Quadrivalent Vaccine against Human Papillomavirus to Prevent Anogenital Diseases. N. Engl. J. Med. 2007, 356, 1928–1943. [Google Scholar] [CrossRef] [Green Version]
- FUTURE II Study Group. Quadrivalent vaccine against human papillomavirus to prevent high-grade cervical lesions. N. Engl. J. Med. 2007, 356, 1915–1927. [Google Scholar] [CrossRef]
- Lehtinen, M.; Paavonen, J.; Wheeler, C.M.; Jaisamrarn, U.; Garland, S.M.; Castellsagué, X.; Skinner, S.R.; Dan, A.; Naud, P.; Salmerón, J.; et al. Overall efficacy of HPV-16/18 AS04-adjuvanted vaccine against grade 3 or greater cervical intraepithelial neoplasia: 4-year end-of-study analysis of the randomised, double-blind PATRICIA trial. Lancet Oncol. 2012, 13, 89–99. [Google Scholar] [CrossRef]
- Joura, E.A.; Giuliano, A.R.; Iversen, O.-E.; Bouchard, C.; Mao, C.; Mehlsen, J.; Moreira, E.D.; Ngan, Y.; Petersen, L.K.; Lazcano-Ponce, E.; et al. A 9-Valent HPV Vaccine against Infection and Intraepithelial Neoplasia in Women. N. Engl. J. Med. 2015, 372, 711–723. [Google Scholar] [CrossRef]
- Markowitz, E.L.; Dunne, E.F.; Saraiya, M.; Chesson, H.W.; Curtis, C.R.; Gee, J.; A. Bocchini, J.; Unger, E.R. Human papillomavirus vaccination: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR. Recomm. Rep. 2014, 63, 1–30. [Google Scholar] [PubMed]
- Robinson, C.L.; Bernstein, H.; Poehling, K.; Romero, J.R.; Szilagyi, P. Advisory Committee on Immunization Practices Recommended Immunization Schedule for Children and Adolescents Aged 18 Years or Younger—United States, 2020. MMWR Morb Mortal Wkly Rep. 2020, 69, 130–132. [Google Scholar] [CrossRef] [Green Version]
- Romanowski, B.; Schwarz, T.F.; Ferguson, L.M.; Ferguson, M.; Peters, K.; Dionne, M.; Schulze, K.; Ramjattan, B.; Hillemanns, P.; Behre, U.; et al. Immune response to the HPV-16/18 AS04-adjuvanted vaccine administered as a 2-dose or 3-dose schedule up to 4 years after vaccination: Results from a randomized study. Hum. Vaccine Immunother. 2014, 10, 1155–1165. [Google Scholar] [CrossRef]
- Dobson, S.R.M.; McNeil, S.; Dionne, M.; Dawar, M.; Ogilvie, G.; Krajden, M.; Young, E. Immunogenicity of 2 doses of HPV vaccine in younger adolescents vs. 3 doses in young women: A randomized clinical trial. JAMA 2013, 309, 1793–1802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giacomet, V.; Penagini, F.; Trabattoni, D.; Viganò, A.; Rainone, V.; Bernazzani, G.; Bonardi, C.M.; Clerici, M.; Bedogni, G.; Zuccotti, G.V. Safety and immunogenicity of a quadrivalent human papillomavirus vaccine in HIV-infected and HIV-negative adolescents and young adults. Vaccine 2014, 32, 5657–5661. [Google Scholar] [CrossRef]
- Barzon, L.; Squarzon, L.; Masiero, S.; Pacenti, M.; Marcati, G.; Mantelli, B.; Liliana, G.; Maria, G.P.; Tiziana, L.; Antonella, C.; et al. Neutralizing and cross-neutralizing antibody titres induced by bivalent and quadrivalent human papillomavirus vaccines in the target population of organized vaccination programmes. Vaccine 2014, 32, 5357–5362. [Google Scholar] [CrossRef] [PubMed]
- Denny, L.A.; Franceschi, S.; de Sanjose, S.; Heard, I.; Moscicki, A.B.; Palefsky, J. Human papillomavirus, human immunodeficiency virus and immunosuppression. Vaccine 2012, 30 (Suppl. 5), F168–F174. [Google Scholar] [CrossRef] [Green Version]
- Hessol, N.A.; Holly, E.A.; Efird, J.T.; Minkoff, H.; Weber, K.M.; Darragh, T.M.; Burk, R.D.; Strickler, H.D.; Greenblatt, R.M.; Palefsky, J.M. Concomitant anal and cervical human papillomavirusV infections and intraepithelial neoplasia in HIV-infected and uninfected women. AIDS 2013, 27, 1743–1751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madkan, V.; Cook-Norris, R.; Steadman, M.; Arora, A.; Mendoza, N.; Tyring, S. The oncogenic potential of human papillomaviruses: A review on the role of host genetics and environmental cofactors. Br. J. Dermatol. 2007, 157, 228–241. [Google Scholar] [CrossRef]
- Moscicki, A.B.; Ellenberg, J.H.; Vermund, S.H.; Holland, C.A.; Darragh, T.; Nowick, P.A.C.; Levin, L.; Wilson, C.M. Prevalence of and risks for cervical human papillomavirus infection and squamous intraepithelial lesions in adolescent girls: Impact of infection with human immunodeficiency virus. Arch. Pediatr. Adolesc. Med. 2000, 154, 127–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kahn, J.A.; Xu, J.; Kapogiannis, B.G.; Rudy, B.; Gonin, R.; Liu, N.; Wilson, C.M.; Worrell, C.; Squires, K.E. Immunogenicity and safety of the human papillomavirus 6, 11, 16, 18 vaccine in HIV-infected young women. Clin. Infect. Dis. 2013, 57, 735–744. [Google Scholar] [CrossRef] [Green Version]
- Levin, M.J.; Moscicki, A.B.; Song, L.Y.; Fenton, T.; Meyer, W.A., III; Read, J.S.; Handelsman, E.L.; Nowak, B.; Sattler, C.A.; Saah, A.; et al. Safety and immunogenicity of a quadrivalent human papillomavirus (types 6, 11, 16, and 18) vaccine in HIV-infected children 7 to 12 years old. J. Acquir Immune Defic Syndr. 2010, 55, 197–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Folschweiller, N.; Teixeira, J.; Joshi, S.; Goldani, L.Z.; Supparatpinyo, K.; Basu, P.; Chotpitayasunondh, T.; Chetchotisakd, P.; Ruxrungtham, K.; Roteli-Martins, C.; et al. Immunogenicity and safety of the AS04-HPV-16/18 and HPV-6/11/16/18 human papillomavirus vaccines in asymptomatic young women living with HIV aged 15–25 years: A phase IV randomized comparative study. EClinicalMedicine 2020, 23, 100353. [Google Scholar] [CrossRef] [PubMed]
- Cubas, R.A.; Mudd, J.C.; Savoye, A.-L.; Perreau, M.; Van Grevenynghe, J.; Metcalf, T.; Connick, E.; Meditz, A.; Freeman, G.J.; Abesada-Terk, G.; et al. Inadequate T follicular cell help impairs B cell immunity during HIV infection. Nat. Med. 2013, 19, 494–499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kojic, E.M.; Kang, M.; Cespedes, M.S.; Umbleja, T.; Godfrey, C.; Allen, R.T.; Firnhaber, C.; Grinsztejn, B.; Palefsky, J.M.; Jennifer, Y.; et al. Immunogenicity and safety of a quadrivalent human papillomavirus vaccine in HIV-1-infected women. Clin. Infect. Dis. 2014, 59, 127–135. [Google Scholar] [CrossRef] [Green Version]
- Einstein, M.H.; Baron, M.; Levin, M.J.; Chatterjee, A.; Fox, B.; Scholar, S.; Rosen, J.; Chakhtoura, N.; Dorothée, M.; Francis, J.D.; et al. Comparative immunogenicity and safety of human papillomavirus (HPV)-16/18 vaccine and HPV-6/11/16/18 vaccine: Follow-up from months 12–24 in a Phase III randomized study of healthy women aged 18–45 years. Hum. Vaccines 2011, 7, 1343–1358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrin, D.M.; Coates, E.E.; Costner, P.J.; Kemp, T.J.; Nason, M.C.; Saharia, K.K.; Pan, Y.; Sarwar, U.N.; Holman, L.; Yamshchikov, G.; et al. Comparison of adaptive and innate immune responses induced by licensed vaccines for human papillomavirus. Hum. Vaccines Immunother. 2014, 10, 3446–3454. [Google Scholar] [CrossRef] [Green Version]
- Ryser, M.; Berlaimont, V.; Karkada, N.; Mihalyi, A.; Rappuoli, R.; van der Most, R. Post-hoc analysis from phase III trials of human papillomavirus vaccines: Considerations on impact on non-vaccine types. Expert Rev. Vaccines 2019, 18, 309–322. [Google Scholar] [CrossRef]
- Levin, M.J.; Huang, S.; Moscicki, A.B.; Song, L.Y.; Read, J.S.; Meyer, W.A.; Kelly, R.; Adriana, W. The IMPAACT P1085 Protocol Team. Four-year persistence of type-specific immunity after quadrivalent human papillomavirus vaccination in HIV-infected children: Effect of a fourth dose of vaccine. Vaccine 2017, 35, 1712–1720. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Male | Female | |||||||
|---|---|---|---|---|---|---|---|---|
| Characteristics | Total (n = 58) | 2-Dose a(n = 20) | 3-Dose a(n = 38) | p-Value | Total (n = 38) | 2-Dose a(n = 10) | 3-Dose a(n = 28) | p-Value |
| Age; n (%) | ||||||||
| ≤15 years | 27 (46.5) | 20 (100.0) | 7 (18.4) | <0.001 | 11 (28.9) | 10 (100.0) | 1 (3.6) | <0.001 |
| >15 years | 31 (53.5) | - | 31 (81.6) | 27 (71.1) | - | 27 (96.4) | ||
| Age at ART start; Median (IQR) | 3.4 (1.0–7.7) | 1.0 (0.3–3.0) | 5.6 (1.4–9.7) | <0.001 | 3.2 (0.6–8.2) | 1.6 (0.3–5.5) | 4.0 (0.7–9.4) | 0.131 |
| Clinical stage | ||||||||
| Worst WHO stage; n (%) | ||||||||
| Stage 1 | 5 (8.6) | 3 (15.0) | 2 (5.3) | 0.251 | 4 (10.5) | 2 (20.0) | 2 (7.1) | 0.785 |
| Stage 2 | 14 (24.1) | 6 (30.0) | 8 (21.0) | 6 (15.8) | 1 (10.0) | 5 (17.9) | ||
| Stage 3 | 22 (37.9) | 8 (40.0) | 14 (36.8) | 15 (39.5) | 4 (40.0) | 11 (39.3) | ||
| Stage 4 | 17 (29.3) | 3 (15.0) | 14 (36.8) | 13 (34.2) | 3 (30.0) | 10 (35.7) | ||
| CD4 | ||||||||
| Nadir CD4 cells/mm3; Median (IQR) | 362 (21–572) | 615 (354–774) | 241 (9–414) | <0.001 | 198 (33–426) | 531 (287–963) | 87 (30–337) | 0.003 |
| At enrollment; Median (IQR) | 626 (501–899) | 866 (639–1061) | 541 (432–743) | <0.001 | 700 (525–1008) | 1152 (702–1359) | 599 (487–746) | 0.009 |
| ≤500; n (%) | 14 (24.1) | - | 14 (36.8) | 0.001 | 7 (18.4) | - | 7 (25.0) | 0.156 |
| >500; n (%) | 44 (75.9) | 20 (100.0) | 24 (63.2) | 31 (81.6) | 10 (100.0) | 21 (75.0) | ||
| VL; n (%) | ||||||||
| <50 copies/mL | 49 (84.5) | 20 (100.0) | 29 (76.3) | 0.021 | 34 (89.5) | 10 (100.0) | 24 (85.7) | 0.556 |
| ≥50 copies/mL | 9 (15.5) | - | 9 (23.7) | 4 (10.5) | - | 4 (14.3) | ||
| Duration of VL < 50 copies/mL (months); Median (IQR) | 91.8 (81.9–96.6) | 90.0 (77.5–94.3) | 92.0 (85.3–102.3) | 0.330 | 56.7 (9.4–86.2) | 72.5 (32.6–87.4) | 54.3 (6.6–82.7) | 0.136 |
| Baseline ART Regimen; n (%) | ||||||||
| NNRTI | 33 (56.9) | 14 (70.0) | 19 (50.0) | 0.172 | 23 (60.5) | 10 (100.0) | 13 (46.4) | 0.003 |
| PI | 25 (43.1) | 6 (30.0) | 19 (50.0) | 15 (39.5) | - | 15 (53.6) | ||
| 2 Doses a | 3 Doses a | p-Value | |
|---|---|---|---|
| Male (Gardasil®) | |||
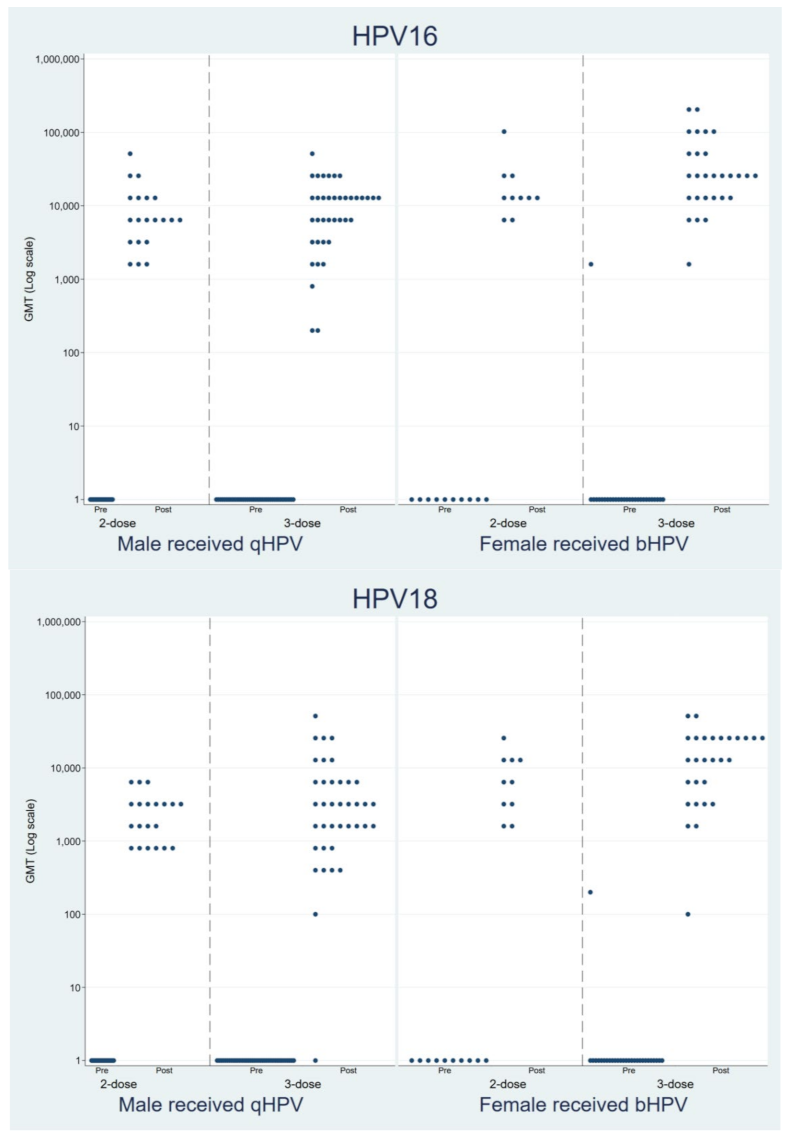
| Type 16 | |||
| Seroconversion; n (%) | 20/20 (100.0) | 38/38 (100.0) | - |
| GMT (95%CI) | 6859.3 (4394.3–10,707.1) | 7011.1 (4648.8–10,573.9) | 0.946 b |
| Type 18 | |||
| Seroconversion; n (%) | 20/20 (100.0) | 37/38 (97.4) | 1.000 |
| GMT (95%CI) | 2039.3 (1432.2–2903.8) | 2859.8 (1810.0–4518.4) | 0.313 b |
| Female (Cervarix®) | |||
| Type 16 | |||
| Seroconversion; n (%) | 10/10 (100.0) | 27/27 (100.0) | - |
| GMT (95%CI) | 15,758.7 (8868.0–28,003.4) | 26,241.6 (16,972.7–40,572.3) | 0.197 b |
| Type 18 | |||
| Seroconversion; n (%) | 10/10 (100.0) | 27/27 (100.0) | - |
| GMT (95%CI) | 5971.4 (3026.8–11,780.6) | 9993.1 (5950.8–16,781.1) | 0.271b |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rungmaitree, S.; Thepthai, C.; Toh, Z.Q.; Musiwiraphat, N.; Maleesatharn, A.; Rermruay, R.; Sungkate, S.; Phongsamart, W.; Lapphra, K.; Wittawatmongkol, O.; et al. Immunogenicity of a Two-Dose Human Papillomavirus Vaccine Schedule in HIV-Infected Adolescents with Immune Reconstitution. Vaccines 2022, 10, 118. https://doi.org/10.3390/vaccines10010118
Rungmaitree S, Thepthai C, Toh ZQ, Musiwiraphat N, Maleesatharn A, Rermruay R, Sungkate S, Phongsamart W, Lapphra K, Wittawatmongkol O, et al. Immunogenicity of a Two-Dose Human Papillomavirus Vaccine Schedule in HIV-Infected Adolescents with Immune Reconstitution. Vaccines. 2022; 10(1):118. https://doi.org/10.3390/vaccines10010118
Chicago/Turabian StyleRungmaitree, Supattra, Charin Thepthai, Zheng Quan Toh, Noppasit Musiwiraphat, Alan Maleesatharn, Rattanachai Rermruay, Sathida Sungkate, Wanatpreeya Phongsamart, Keswadee Lapphra, Orasri Wittawatmongkol, and et al. 2022. "Immunogenicity of a Two-Dose Human Papillomavirus Vaccine Schedule in HIV-Infected Adolescents with Immune Reconstitution" Vaccines 10, no. 1: 118. https://doi.org/10.3390/vaccines10010118