Relationship between Ischemic Stroke and Pulse Rate Variability as a Surrogate of Heart Rate Variability

Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Protocol and Data Acquisition
2.2. Data Processing
2.3. Statistical Analysis
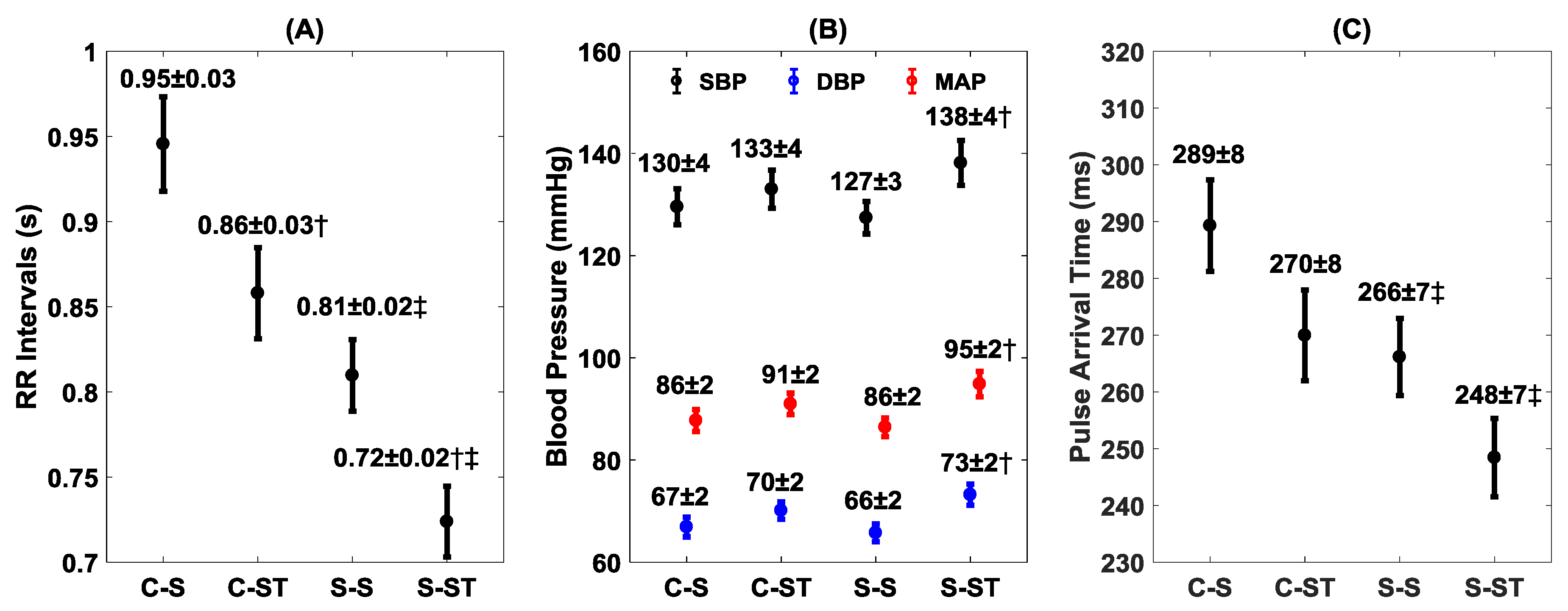
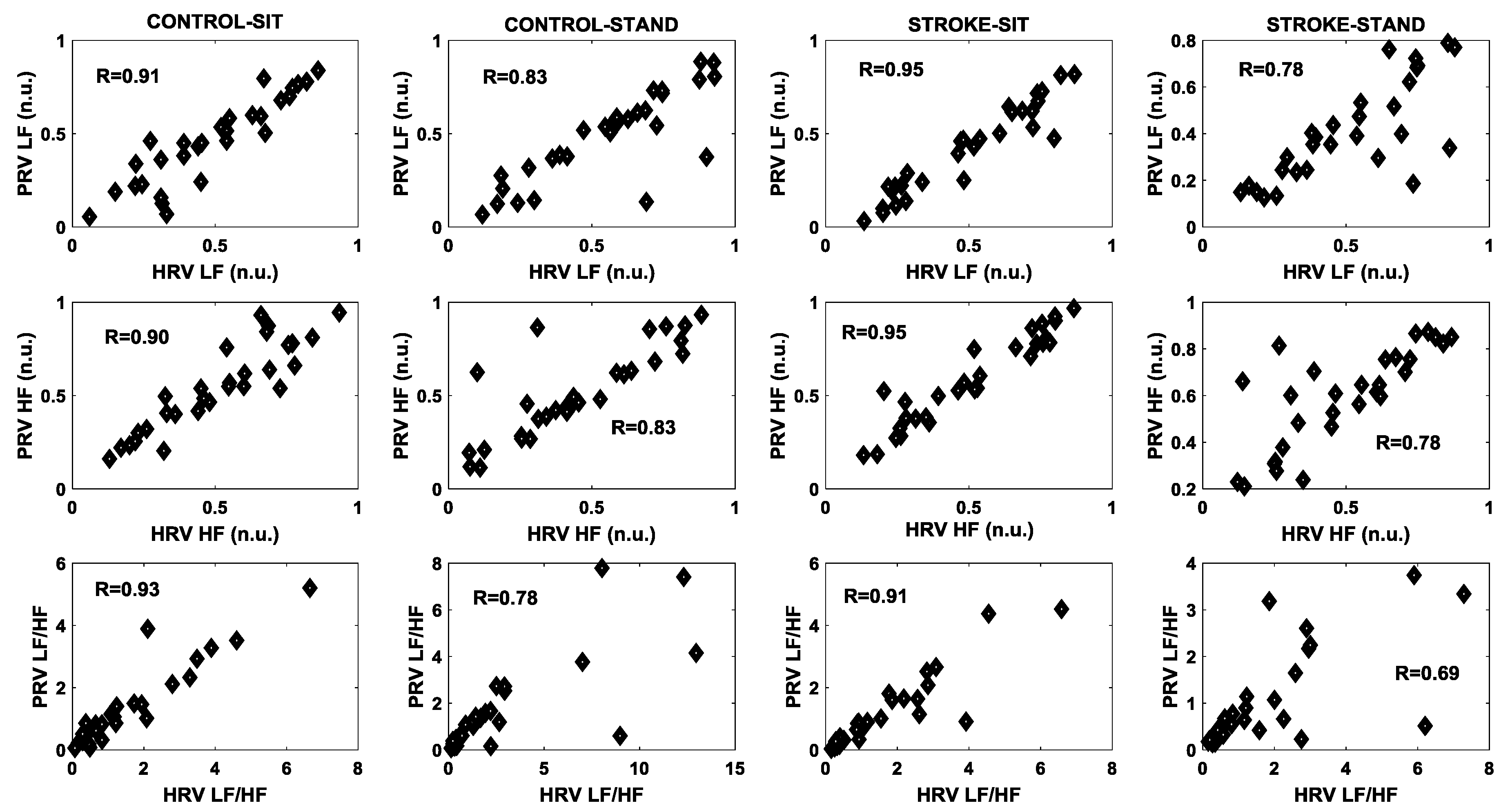
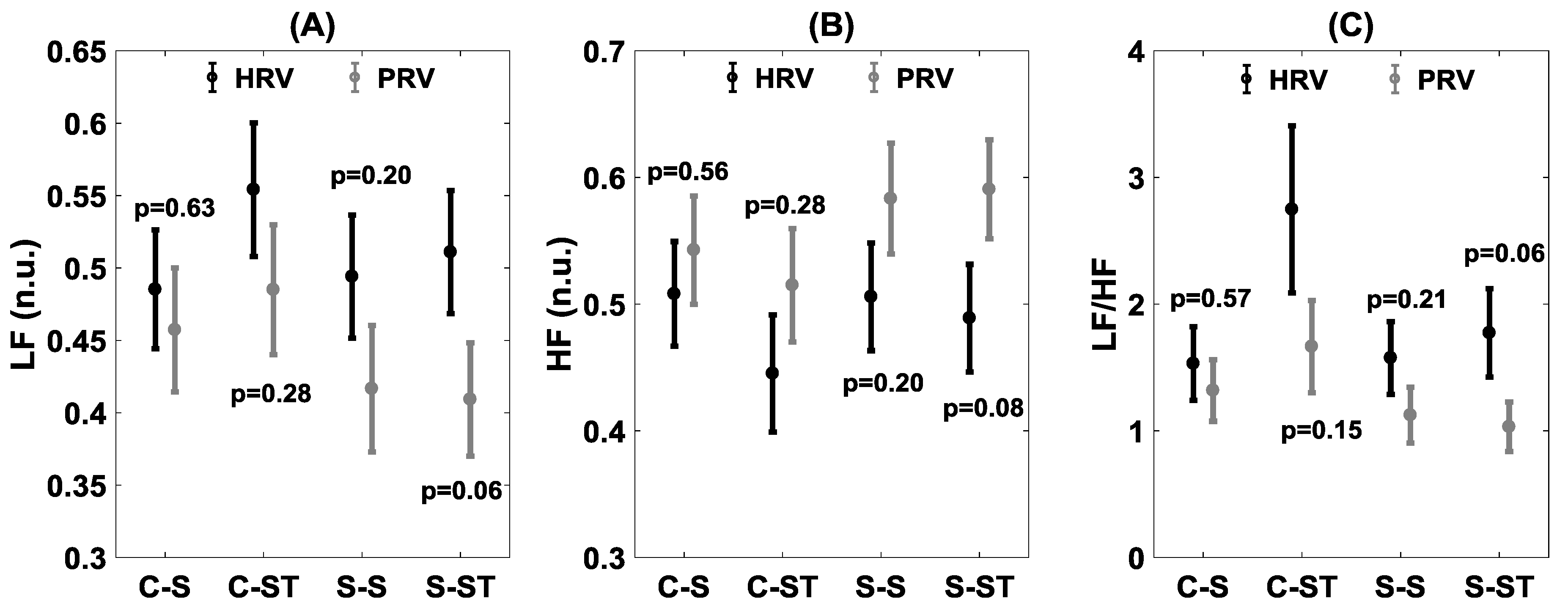
3. Results
4. Discussion
5. Conclusions and Limitations
Author Contributions
Funding
Acknowledgment
Conflicts of Interest
References
- De Raedt, S.; De Vos, A.; De Keyser, J. Autonomic dysfunction in acute ischemic stroke: An underexplored therapeutic area? J. Neurol. Sci. 2015, 348, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Yperzeele, L.; Van Hooff, R.-J.; Nagels, G.; De Smedt, A.; De Keyser, J.; Brouns, R. Heart Rate Variability and Baroreceptor Sensitivity in Acute Stroke: A Systematic Review. Int. J. Stroke 2015, 10, 796–800. [Google Scholar] [CrossRef] [PubMed]
- Robinson, T.G.; Dawson, S.L.; Eames, P.J.; Panerai, R.B.; Potter, J.F.; Oppenheimer, S. Cardiac Baroreceptor Sensitivity Predicts Long-Term Outcome After Acute Ischemic Stroke. Stroke 2003, 34, 705–712. [Google Scholar] [CrossRef] [PubMed]
- Tzeng, Y.C.; Ainslie, P.N. Blood pressure regulation IX: Cerebral autoregulation under blood pressure challenges. Eur. J. Appl. Physiol. 2014, 114, 545–559. [Google Scholar] [CrossRef] [PubMed]
- Rowell, L.B. Human Cardiovascular Control; Oxford University Press: New York, NY, USA, 1993; ISBN 0195073622. [Google Scholar]
- Halliwill, J.R.; Sieck, D.C.; Romero, S.A.; Buck, T.M.; Ely, M.R. Blood pressure regulation X: What happens when the muscle pump is lost? Post-exercise hypotension and syncope. Eur. J. Appl. Physiol. 2014, 114, 561–578. [Google Scholar] [CrossRef] [PubMed]
- Goswami, N.; Blaber, A.P.; Hinghofer-Szalkay, H.; Montani, J.-P. Orthostatic Intolerance in Older Persons: Etiology and Countermeasures. Front. Physiol. 2017, 8, 803. [Google Scholar] [CrossRef]
- Tang, A.; Eng, J.J.; Krassioukov, A. Application of the Sit-Up Test for orthostatic hypotension in individuals with stroke. Auton. Neurosci. 2012, 168, 82–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eigenbrodt, M.L.; Rose, K.M.; Couper, D.J.; Arnett, D.K.; Smith, R.; Jones, D. Orthostatic hypotension as a risk factor for stroke: The atherosclerosis risk in communities (ARIC) study, 1987–1996. Stroke 2000, 31, 2307–2313. [Google Scholar] [CrossRef]
- Rodriguez, J.; Blaber, A.P.; Kneihsl, M.; Trozic, I.; Ruedl, R.; Green, D.A.; Broadbent, J.; Xu, D.; Rössler, A.; Hinghofer-Szalkay, H.; et al. Poststroke alterations in heart rate variability during orthostatic challenge. Medicine 2017, 96, e5989. [Google Scholar] [CrossRef] [Green Version]
- Xiong, L.; Leung, H.; Chen, X.Y.; Han, J.H.; Leung, T.; Soo, Y.; Wong, E.; Chan, A.; Lau, A.; Wong, K.S.; et al. Preliminary findings of the effects of autonomic dysfunction on functional outcome after acute ischemic stroke. Clin. Neurol. Neurosurg. 2012, 114, 316–320. [Google Scholar] [CrossRef]
- Béjot, Y.; Bailly, H.; Durier, J.; Giroud, M. Epidemiology of stroke in Europe and trends for the 21st century. La Presse Médicale 2016, 45, e391–e398. [Google Scholar] [CrossRef] [PubMed]
- Krueger, H.; Koot, J.; Hall, R.E.; O’Callaghan, C.; Bayley, M.; Corbett, D. Prevalence of Individuals Experiencing the Effects of Stroke in Canada: Trends and Projections. Stroke. 2015, 46, 2226–2231. [Google Scholar] [CrossRef] [PubMed]
- Ortman, B.J.M.; Velkoff, V.A.; Hogan, H. An Aging Nation: The Older Population in the United States. Available online: http://bowchair.com/uploads/9/8/4/9/98495722/agingcensus.pdf (accessed on 28 June 2019).
- Heesch, C.M. Reflexes that control cardiovascular function. Adv. Physiol. Educ. 1999, 277, 234. [Google Scholar] [CrossRef] [PubMed]
- Lambert, E.; Lambert, G.W. Sympathetic dysfunction in vasovagal syncope and the postural orthostatic tachycardia syndrome. Front. Physiol. 2014, 5, 280. [Google Scholar] [CrossRef] [PubMed]
- Malik, M.; Bigger, J.T.; Camm, A.J.; Kleiger, R.E.; Malliani, A.; Moss, A.J.; Schwartz, P.J. Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. Eur. Hear. J. 1996, 17, 354–381. [Google Scholar] [CrossRef] [Green Version]
- Acharya, U.R.; Joseph, K.P.; Kannathal, N.; Lim, C.M.; Suri, J.S. Heart rate variability: A review. Med. Biol. Eng. Comput. 2006, 44, 1031–1051. [Google Scholar] [CrossRef] [PubMed]
- Cooke, W.H.; Salinas, J.; Convertino, V.A.; Ludwig, D.A.; Hinds, D.; Duke, J.H.; Moore, F.A.; Holcomb, J.B. Heart Rate Variability and Its Association with Mortality in Prehospital Trauma Patients. J. Trauma: Inj. Infect. Crit. Care 2006, 60, 363–370. [Google Scholar] [CrossRef]
- Verma, A.K.; Cabrera, S.D.; Fazel-Rezai, R. Continuous Balance Assessment of Autonomic Nervous System Using Time-Varying Analysis of Heart Rate Variability 1. J. Med Devices 2016, 10, 020933. [Google Scholar] [CrossRef]
- Ishikawa, T.; Hyodo, Y.; Miyashita, K.; Yoshifuji, K.; Komoriya, Y.; Imai, Y. Wearable Motion Tolerant PPG Sensor for Instant Heart Rate in Daily Activity. Available online: https://www.scitepress.org/Papers/2017/61099/61099.pdf (accessed on 28 June 2019).
- Charlot, K.; Cornolo, J.; Brugniaux, J.V.; Richalet, J.P.; Pichon, A. Interchangeability between heart rate and photoplethysmography variabilities during sympathetic stimulations. Physiol. Meas. 2009, 30, 1357–1369. [Google Scholar] [CrossRef]
- Moraes, J.L.; Rocha, M.X.; Vasconcelos, G.G.; Filho, J.V.; De Albuquerque, V.H.C.; Alexandria, A.R. Advances in Photopletysmography Signal Analysis for Biomedical Applications. Sensors 2018, 18, 1894. [Google Scholar] [CrossRef]
- Schäfer, A.; Vagedes, J. How accurate is pulse rate variability as an estimate of heart rate variability?: A review on studies comparing photoplethysmographic technology with an electrocardiogram. Int. J. Cardiol. 2013, 166, 15–29. [Google Scholar] [CrossRef] [PubMed]
- McKinley, P.S.; Shapiro, P.A.; Bagiella, E.; Myers, M.M.; De Meersman, R.E.; Grant, I.; Sloan, R.P. Deriving heart period variability from blood pressure waveforms. J. Appl. Physiol. 2003, 95, 1431–1438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bulte, C.S.; Keet, S.W.; Boer, C.; Bouwman, R.A. Level of agreement between heart rate variability and pulse rate variability in healthy individuals. Eur. J. Anaesthesiol. 2011, 28, 34–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pernice, R.; Member, I.; Javorka, M.; Krohova, J.; Czippelova, B.; Turianikova, Z.; Busacca, A.; Faes, L. Comparison of short-term heart rate variability indexes evaluated through electrocardiographic and continuous blood pressure monitoring. Med. Boil. Eng. 2019, 57, 1247–1263. [Google Scholar] [CrossRef] [PubMed]
- Reisner, A.; Shaltis, P.A.; McCombie, D.; Asada, H.H. Utility of the Photoplethysmogram in Circulatory Monitoring. Anesthesiology 2008, 108, 950–958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verma, A.K.; Xu, D.; Bruner, M.; Garg, A.; Goswami, N.; Blaber, A.P.; Tavakolian, K. Comparison of Autonomic Control of Blood Pressure During Standing and Artificial Gravity Induced via Short-Arm Human Centrifuge. Front. Physiol. 2018, 9, 712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, S.; Zhao, H.; Ju, K.; Shin, K.; Lee, M.; Shelley, K.; Chon, K.H. Can Photoplethysmography Variability Serve as an Alternative Approach to Obtain Heart Rate Variability Information? J. Clin. Monit. 2007, 22, 23–29. [Google Scholar] [CrossRef]
- Lu, G.; Yang, F.; Taylor, J.A.; Stein, J.F. A comparison of photoplethysmography and ECG recording to analyse heart rate variability in healthy subjects. J. Med. Eng. Technol. 2009, 33, 634–641. [Google Scholar] [CrossRef]
- Giardino, N.D.; Lehrer, P.M.; Edelberg, R. Comparison of finger plethysmograph to ECG in the measurement of heart rate variability. Psychophysiology 2002, 39, 246–253. [Google Scholar] [CrossRef]
- Vescio, B.; Salsone, M.; Gambardella, A.; Quattrone, A. Comparison between Electrocardiographic and Earlobe Pulse Photoplethysmographic Detection for Evaluating Heart Rate Variability in Healthy Subjects in Short- and Long-Term Recordings. Sensors 2018, 18, 844. [Google Scholar] [CrossRef]
- Wong, J.-S.; Lu, W.-A.; Wu, K.-T.; Liu, M.; Chen, G.-Y.; Kuo, C.-D. A comparative study of pulse rate variability and heart rate variability in healthy subjects. J. Clin. Monit. 2012, 26, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Gil, E.; Orini, M.; Bailón, R.; Vergara, J.M.; Mainardi, L.; Laguna, P. Photoplethysmography pulse rate variability as a surrogate measurement of heart rate variability during non-stationary conditions. Physiol. Meas. 2010, 31, 1271–1290. [Google Scholar] [CrossRef] [PubMed]
- Dehkordi, P.; Garde, A.; Karlen, W.; Wensley, D.; Ansermino, J.M.; Dumont, G.A. Pulse Rate Variability in Children with Disordered Breathing during Different Sleep Stages. In Proceedings of the Computing in Cardiology 2013, Zaragoza, Spain, 22–25 September 2013; IEEE: New York, NY, USA, 2013. [Google Scholar]
- Khandoker, A.H.; Karmakar, C.K.; Palaniswami, M. Comparison of pulse rate variability with heart rate variability during obstructive sleep apnea. Med. Eng. Phys. 2011, 33, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Chou, Y.; Zhu, P.; Huang, X.; Lin, J.; Liu, J.; Gu, Y. Comparison Between Heart Rate Variability and Pulse Rate Variability for Bradycardia and Tachycardia Subjects. In Proceedings of the 2018 International Conference on Control, Automation and Information Sciences (ICCAIS), Hangzhou, China, 24–27 October 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 1–6. [Google Scholar]
- Paliakaitė, B.; Daukantas, S.; Marozas, V. Assessment of pulse arrival time for arterial stiffness monitoring on body composition scales. Comput. Boil. Med. 2017, 85, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Goldberger, A.L.; Amaral, L.A.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.K.; Stanley, H.E. PhysioBank, PhysioToolkit, and PhysioNet: Components of a new research resource for complex physiologic signals. Circulation 2000, 101, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Novak, V.; Hu, K.; Desrochers, L.; Novak, P.; Caplan, L.; Lipsitz, L.; Selim, M. Cerebral flow velocities during daily activities depend on blood pressure in patients with chronic ischemic infarctions. Stroke 2010, 41, 61–66. [Google Scholar] [CrossRef]
- Pan, J.; Tompkins, W.J. A Real-Time QRS Detection Algorithm. IEEE Trans. Biomed. Eng. 1985, 230–236. [Google Scholar] [CrossRef]
- Mukkamala, R.; Hahn, J.-O.; Inan, O.T.; Mestha, L.K.; Kim, C.-S.; Toreyin, H.; Kyal, S. Towards Ubiquitous Blood Pressure Monitoring via Pulse Transit Time: Theory and Practice. IEEE Trans. Biomed. Eng. 2015, 62, 1879–1901. [Google Scholar] [CrossRef]
- Chen, Y.; Shen, F.; Liu, J.; Yang, G.-Y. Arterial stiffness and stroke: De-stiffening strategy, a therapeutic target for stroke. Stroke Vasc. Neurol. 2017, 2, 65–72. [Google Scholar] [CrossRef]
- Yoshida, K.; Takano, K.; Hatanaka, M. Effect of aging on pulse rate variability for evaluating autonomic nervous system. Jpn. J. Med. Technol. 2018, 67, 289–293. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HRV/PRV Variables | Domain |
|---|---|
| Mean RR/PP intervals (heart period, HP) | Time |
| Standard deviation of RR/PP intervals (SDNN) | Time |
| Root mean square of successive difference between adjacent intervals (RMSSD) | Time |
| Standard deviation of successive difference between adjacent intervals (SDSD) | Time |
| Percentage of adjacent RR/PP intervals that differ by more than 50 ms (pNN50) | Time |
| Normalized Low-Frequency (LF (n.u.)) | Frequency |
| Normalized High-Frequency (HF (n.u.)) | Frequency |
| LF/HF Ratio | Frequency |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Verma, A.K.; Aarotale, P.N.; Dehkordi, P.; Lou, J.-S.; Tavakolian, K. Relationship between Ischemic Stroke and Pulse Rate Variability as a Surrogate of Heart Rate Variability. Brain Sci. 2019, 9, 162. https://doi.org/10.3390/brainsci9070162
Verma AK, Aarotale PN, Dehkordi P, Lou J-S, Tavakolian K. Relationship between Ischemic Stroke and Pulse Rate Variability as a Surrogate of Heart Rate Variability. Brain Sciences. 2019; 9(7):162. https://doi.org/10.3390/brainsci9070162
Chicago/Turabian StyleVerma, Ajay K., Parshuram N. Aarotale, Parastoo Dehkordi, Jau-Shin Lou, and Kouhyar Tavakolian. 2019. "Relationship between Ischemic Stroke and Pulse Rate Variability as a Surrogate of Heart Rate Variability" Brain Sciences 9, no. 7: 162. https://doi.org/10.3390/brainsci9070162