Comparative Volumetric Analysis of the Brain and Cerebrospinal Fluid in Chiari Type I Malformation Patients: A Morphological Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Control Subjects
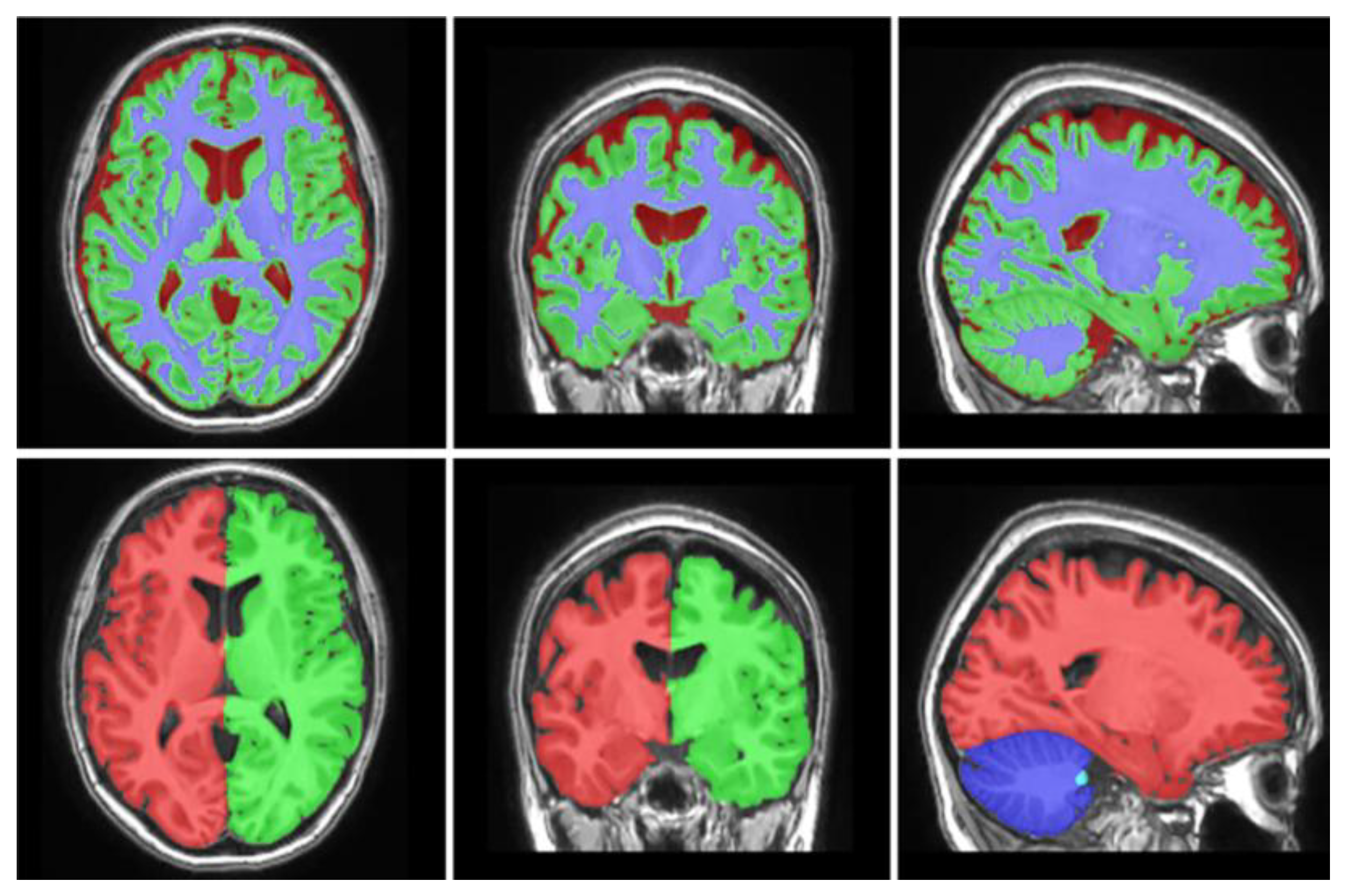
2.2. Imaging and Morphometrical Data Collection
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Aboulezz, A.O.; Sartor, K.; Geyer, C.A.; Gado, M.H. Position of cerebellar tonsils in the normal population and in patients with chiari malformation: A quantitative approach with MR imaging. J. Comput. Assist. Tomogr. 1985, 9, 1033–1036. [Google Scholar] [CrossRef]
- Aydin, S.; Hanimoglu, H.; Tanriverdi, T.; Yentur, E.; Kaynar, M.Y. Chiari type I malformations in adults: A morphometric analysis of the posterior cranial fossa. Surg. Neurol. 2005, 64, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Barkovich, A.J.; Wippold, F.J.; Sherman, J.L.; Citrin, C.M. Significance of cerebellar tonsillar position on MR. Am. J. Neuroradiol. 1986, 7, 795–799. [Google Scholar] [PubMed]
- Aitken, L.A.; Lindan, C.E.; Sidney, S.; Gupta, N.; Barkovich, A.J.; Sorel, M.; Wu, Y.W. Chiari Type I Malformation in a Pediatric Population. Pediatr. Neurol. 2009, 40, 449–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milhorat, T.H.; Nishikawa, M.; Kula, R.W.; Dlugacz, Y.D. Mechanisms of cerebellar tonsil herniation in patients with Chiari malformations as guide to clinical management. Acta. Neurochir. (Wien). 2010, 152, 1117–1127. [Google Scholar] [CrossRef] [Green Version]
- Badie, B.; Mendoza, D.; Batzdorf, U. Posterior fossa volume and response to suboccipital decompression in patients with chiari i malformation. Neurosurgery 1995, 37, 214–218. [Google Scholar] [CrossRef] [PubMed]
- Elster, A.D.; Chen, M.Y. Chiari I malformations: clinical and radiologic reappraisal. Radiology 2014, 183, 347–353. [Google Scholar] [CrossRef]
- Gardner, W.J. Hydrodynamic mechanism of syringomyelia: İts relationship to myelocele. J. Neurol. Neurosurg. Psychiatry 1965, 28, 247–259. [Google Scholar] [CrossRef] [PubMed]
- Levy, W.J.; Mason, L.; Hahn, J.F. Chiari malformation presenting in adults: A surgical experience in 127 cases. Neurosurgery 1983, 12, 377–390. [Google Scholar] [CrossRef]
- Milhorat, T.H.; Chou, M.W.; Trinidad, E.M.; Kula, R.W.; Mandell, M.; Wolpert, C.; Speer, M.C. Chiari I malformation redefined: Clinical and radiographic findings for 364 symptomatic patients. Neurosurgery 1999, 44, 1005–1017. [Google Scholar] [CrossRef]
- Nishikawa, M.; Sakamoto, H.; Hakuba, A.; Nakanishi, N.; Inoue, Y. Pathogenesis of Chiari malformation: A morphometric study of the posterior cranial fossa. J. Neurosurg. 2009, 86, 40–47. [Google Scholar] [CrossRef]
- Dagtekin, A.; Avci, E.; Kara, E.; Uzmansel, D.; Dagtekin, O.; Koseoglu, A.; Talas, D.; Bagdatoglu, C. Posterior cranial fossa morphometry in symptomatic adult Chiari I malformation patients: Comparative clinical and anatomical study. Clin. Neurol. Neurosurg. 2011, 113, 399–403. [Google Scholar] [CrossRef]
- Furtado, S.V.; Reddy, K.; Hegde, A.S. Posterior fossa morphometry in symptomatic pediatric and adult Chiari I malformation. J. Clin. Neurosci. 2009, 16, 1449–1454. [Google Scholar]
- Karagoz, F.; Izgi, N.; Sencer, S.K. Morphometric measurements of the cranium in patients with Chiari type I malformation and comparison with the normal population. Acta. Neurochir. (Wien). 2002, 144, 165–171. [Google Scholar]
- Stovner, L.J.; Bergan, U.; Nilsen, G.; Sjaastad, O. Posterior cranial fossa dimensions in the Chiari I malformation: Relation to pathogenesis and clinical presentation. Neuroradiology 1993, 35, 113–118. [Google Scholar] [CrossRef]
- Yan, H.; Han, X.; Jin, M.; Liu, Z.; Xie, D.; Sha, S.; Qiu, Y.; Zhu, Z. Morphometric features of posterior cranial fossa are different between Chiari I malformation with and without syringomyelia. Eur. Spine J. 2016, 25, 2202–2209. [Google Scholar] [CrossRef]
- Chen, Z.; Liu, M.; Ma, L. Gray Matter Volumes Changes over the Whole Brain in the Bulbar- and Spinal-Onset Amyotrophic Lateral Sclerosis: A voxel-based morphometry study. Chin. Med. Sci. J. 2018, 33, 20–28. [Google Scholar]
- Dunet, V.; Deverdun, J.; Charroud, C.; Le Bars, E.; Molino, F.; Menjot de Champfleur, S.; Maury, F.; Charif, M.; Ayrignac, X.; Labauge, P.; et al. Cognitive impairment and basal ganglia functional connectivity in vascular parkinsonism. Am. J. Neuroradiol. 2016, 264, 1511–1519. [Google Scholar] [CrossRef]
- Faria, A.V.; Ratnanather, J.T.; Tward, D.J.; Lee, D.S.; van den Noort, F.; Wu, D.; Brown, T.; Johnson, H.; Paulsen, J.S.; Ross, C.A.; et al. PREDICT-HD Investigators and Coordinators of the Huntington Study Group. Linking white matter and deep gray matter alterations in premanifest Huntington disease. NeuroImage Clin. 2016, 11, 450–460. [Google Scholar] [CrossRef]
- Hedderich, D.M.; Spiro, J.E.; Goldhardt, O.; Kaesmacher, J.; Wiestler, B.; Yakushev, I.; Zimmer, C.; Boeckh-Behrens, T.; Grimmer, T. Increasing Diagnostic Accuracy of Mild Cognitive Impairment due to Alzheimer’s Disease by User-Independent, Web-Based Whole-Brain Volumetry. J. Alzheimer’s Dis. 2018, 65, 1459–1467. [Google Scholar] [CrossRef]
- Hong, S.J.; Bernhardt, B.C.; Schrader, D.S.; Bernasconi, N.; Bernasconi, A. Whole-brain MRI phenotyping in dysplasia-related frontal lobe epilepsy. Neurology 2016, 86, 643–650. [Google Scholar] [CrossRef] [Green Version]
- Larvie, M.; Fischl, B. Volumetric and fiber-tracing MRI methods for gray and white matter. Handb. Clin. Neurol. 2016, 135, 39–60. [Google Scholar]
- Alperin, N.; Loftus, J.R.; Oliu, C.J.; Bagci, A.M.; Lee, S.H.; Ertl-Wagner, B.; Green, B.; Sekula, R. Magnetic resonance imaging measures of posterior cranial fossa morphology and cerebrospinal fluid physiology in chiari malformation type I. Neurosurgery 2014, 75, 515–522. [Google Scholar] [CrossRef]
- Bagci, A.M.; Lee, S.H.; Nagornaya, N.; Green, B.A.; Alperin, N. Automated posterior cranial fossa volumetry by MRI: Applications to Chiari malformation type I. Am. J. Neuroradiol. 2013, 34, 1758–1763. [Google Scholar] [CrossRef]
- Manjón, J.V.; Coupé, P. volBrain: An Online MRI Brain Volumetry System. Front. Neuroinform. 2016, 10, 30. [Google Scholar] [CrossRef] [Green Version]
- Frič, R.; Eide, P.K. Comparative observational study on the clinical presentation, intracranial volume measurements, and intracranial pressure scores in patients with either Chiari malformation Type I or idiopathic intracranial hypertension. J. Neurosurg. 2017, 126, 1312–1322. [Google Scholar] [CrossRef] [Green Version]
- Trigylidas, T.; Baronia, B.; Vassilyadi, M.; Ventureyra, E.C.G. Posterior fossa dimension and volume estimates in pediatric patients with Chiari I malformations. Child’s Nerv. Syst. 2008, 24, 329–336. [Google Scholar] [CrossRef]
- Hayhurst, C.; Osman-Farah, J.; Das, K.; Mallucci, C. Initial management of hydrocephalus associated with Chiari malformation Type I–syringomyelia complex via endoscopic third ventriculostomy: An outcome analysis. J. Neurosurg. 2008, 108, 1211–1214. [Google Scholar] [CrossRef]
- Mancarella, C.; Delfini, R.; Landi, A. Chiari Malformations. In New Trends in Craniovertebral Junction Surgery; Visocchi, M., Ed.; Springer: Cham, Germany, 2019; Volum 125, pp. 89–95. [Google Scholar]
- Du Boulay, G.; Shah, S.H.; Currie, J.C.; Logue, V. The mechanism of hydromyelia in Chiari type 1 malformations. Br. J. Radiol. 1974, 47, 579–587. [Google Scholar] [CrossRef]
- Hofmann, E.; Warmuth-Metz, M.; Bendszus, M.; Solymosi, L. Phase-contrast MR imaging of the cervical CSF and spinal cord: Volumetric motion analysis in patients with Chiari I malformation. Am. J. Neuroradiol. 2000, 21, 151–158. [Google Scholar]
- Di Rocco, C.; Rende, M. Neural tube defects—Some remarks on the possible role of glycosaminoglycans in the genesis of the dysraphic state, the anomaly in the configuration of the posterior cranial fossa, and hydrocephalus. Child. Nerv. Syst. 1987, 3, 334–341. [Google Scholar] [CrossRef]
- Francis, P.M.; Beals, S.; Rekate, H.L.; Pittman, H.W.; Manwaring, K.; Reiff, J. Chronic tonsillar herniation and Crouzon’s syndrome. Pediatr. Neurosurg. 1992, 18, 202–206. [Google Scholar]
- Gripp, K.W.; Hopkins, E.; Doyle, D.; Dobyns, W.B. High incidence of progressive postnatal cerebellar enlargement in Costello syndrome: Brain overgrowth associated with HRAS mutations as the likely cause of structural brain and spinal cord abnormalities. Am. J. Med. Genet. Part A 2010, 152, 1161–1168. [Google Scholar] [CrossRef]
- Martínez-Lage, J.F.; Guillén-Navarro, E.; Almagro, M.J.; Felipe-Murcia, M.; López López-Guerrero, A.; Galarza, M. Hydrocephalus and Chiari type 1 malformation in macrocephaly-cutis marmorata telangiectatica congenita: A case-based update. Child. Nerv. Syst. 2010, 26, 13–18. [Google Scholar] [CrossRef]
- Decq, P.; Le Guérinel, C.; Sol, J.C.; Brugières, P.; Djindjian, M.; Nguyen, J.P. Chiari I malformation: A rare cause of noncommunicating hydrocephalus treated by third ventriculostomy. J. Neurosurg. 2009, 95, 783–790. [Google Scholar] [CrossRef]
- Di Rocco, C.; Di Trapani, G.; Pettorossi, V.E.; Caldarelli, M. On the pathology of experimental hydrocephalus induced by artificial increase in endoventricular CSF pulse pressure. Child’s Brain. 1979, 5, 81–95. [Google Scholar] [CrossRef]
- Di Rocco, C.; Pettorossi, V.E.; Caldarelli, M.; Mancinelli, R.; Velardi, F. Communicating hydrocephalus induced by mechanically increased amplitude of the intraventricular cerebrospinal fluid pressure: Experimental studies. Exp. Neurol. 1978, 59, 40–52. [Google Scholar] [CrossRef]
- Di Rocco, C.; Frassanito, P.; Massimi, L.; Peraio, S. Hydrocephalus and Chiari type I malformation. Child’s Nerv. Syst. 2011, 27, 1653–1664. [Google Scholar] [CrossRef]
- Kriebel, R.M.; Shah, A.B.; McAllister, J.P. The Microstructure of Cortical Neuropil before and after Decompression in Experimental Infantile Hydrocephalus. Exp. Neurol. 1993, 119, 89–98. [Google Scholar]
- McLone, D.G.; Bondareff, W.; Raimondi, A.J. Hydrocephalus-3, a Murine mutant. II. Changes in the brain extracellular space. Surg. Neurol. 1973, 1, 233–242. [Google Scholar]
- Mori, K.; Raimondi, A.J. Submicroscopic changes in the periventricular white matter of hydrocephalic Ch Mouse. Arch. Jap. Chir. 1975, 4, 159–168. [Google Scholar]
- Weller, R.O.; Mitchell, J.; Griffin, R.L.; Gardner, M.J. The effects of hydrocephalus upon the developing brain. Histological and quantitative studies of the ependyma and subependyma in hydrocephalic rats. J. Neurol. Sci. 1978, 36, 383–402. [Google Scholar] [CrossRef]
- Castejón, O.J. Submicroscopic pathology of human and experimental hydrocephalic cerebral cortex. Folia Neuropathol. 2010, 48, 159–174. [Google Scholar] [PubMed]
- McAllister, J.P.; Cohen, M.I.; O’Mara, K.A.; Johnson, M.H.; Rekate, H.L. Progression of experimental infantile hydrocephalus and effects of ventriculoperitoneal shunts: An analysis correlating magnetic resonance imaging with gross morphology. Neurosurgery 1991, 29, 329–340. [Google Scholar] [CrossRef] [PubMed]
- Olopade, F.E.; Shokunbi, M.T.; Sirén, A.L. The relationship between ventricular dilatation, neuropathological and neurobehavioural changes in hydrocephalic rats. Fluids Barriers CNS 2012, 9, 19. [Google Scholar] [CrossRef] [PubMed]
- Wünschmann, A.; Oglesbee, M. Periventricular changes associated with spontaneous canine hydrocephalus. Vet. Pathol. 2001, 38, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, J.M.; McCauley, S.R.; Brandt, M.E.; Bohan, T.P.; Kramer, L.A.; Francis, D.J.; Thorstad, K.; Brookshire, B.L. Regional brain tissue composition in children with hydrocephalus: Relationships with cognitive development. Arch. Neurol. 1996, 53, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Ye, X.; Bai, G.; Fu, Y.; Mao, C.; Wu, A.; Liu, X.; Yan, Z. Alterations in Cortical Thickness and White Matter Integrity in Mild-to-Moderate Communicating Hydrocephalic School-Aged Children Measured by Whole-Brain Cortical Thickness Mapping and DTI. Neural Plast. 2017, 5167973. [Google Scholar] [CrossRef]
- Mokri, B. The Monro-Kellie hypothesis: Applications in CSF volume depletion. Neurology 2001, 56, 1746–1748. [Google Scholar] [CrossRef]
- Cropley, V.L.; Klauser, P.; Lenroot, R.K.; Bruggemann, J.; Sundram, S.; Bousman, C.; Pereira, A.; Di Biase, M.A.; Weickert, T.W.; Weickert, C.S.; et al. Accelerated gray and white matter deterioration with age in schizophrenia. Am. J. Psychiatry 2017, 174, 286–295. [Google Scholar] [CrossRef]
- Cwik, J.C.; Vahle, N.; Woud, M.L.; Potthoff, D.; Kessler, H.; Sartory, G.; Seitz, R.J. Reduced gray matter volume in the left prefrontal, occipital, and temporal regions as predictors for posttraumatic stress disorder: A voxel-based morphometric study. Eur. Arch. Psychiatry Clin. Neurosci. 2019, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Nakano, M.; Matsuo, K.; Nakashima, M.; Matsubara, T.; Harada, K.; Egashira, K.; Masaki, H.; Takahashi, K.; Watanabe, Y. Gray matter volume and rapid decision-making in major depressive disorder. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2014, 48, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Sato, W.; Kochiyama, T.; Uono, S.; Yoshimura, S.; Kubota, Y.; Sawada, R.; Sakihama, M.; Toichi, M. Reduced Gray Matter Volume in the Social Brain Network in Adults with Autism Spectrum Disorder. Front. Hum. Neurosci. 2017, 11, 395. [Google Scholar] [CrossRef] [Green Version]
- Wu, C.; Zheng, Y.; Li, J.; She, S.; Peng, H.; Li, L. Cortical gray matter loss, augmented vulnerability to speech-on-speech masking, and delusion in people with schizophrenia. Front. Psychiatry 2018, 9, 287. [Google Scholar] [CrossRef] [PubMed]
- Besteiro González, J.L.; Torres Campa-Santamarina, J.M. Anomalies in the cognitive-executive functions in patients with Chiari Malformation Type I. Psicothema 2018, 30, 316–321. [Google Scholar]
- Rogers, J.M.; Savage, G.; Stoodley, M.A. A systematic review of cognition in Chiari I Malformation. Neuropsychol. Rev. 2018, 28, 176–187. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | CM-I | Control | Mean Difference | 95% Cl | p Value * |
|---|---|---|---|---|---|
| Total ICV (cm3) | 1344.6 ± 133.3 | 1328.9 ± 116.8 | −15.69 | −45.17 to 13.79 | 1.000 |
| Cerebrum Volume (cm3) | 1004.3 ± 119.3 | 1013.9 ± 96.0 | 9.66 | −15.81 to 35.13 | 1.000 |
| Cerebrum Volume Pct (%) | 74.6 ± 4.4 | 76.3 ± 2.2 | 1.64 | 0.82 to 2.47 | 0.052 |
| Cerebellum Volume (cm3) | 130.8 ± 74.3 | 128.4 ± 11.9 | −2.39 | −14.91 to 10.14 | 0.657 |
| Cerebellum Volume Pct (%) | 9.3 ± 0.9 | 9.7 ± 0.6 | 0.41 | 0.23 to 0.58 | 0.002 |
| Brainstem Volume (cm3) | 21.7 ± 3.4 | 21.6 ± 2.3 | −0.18 | −0.87 to 0.51 | 1.000 |
| Brainstem Volume Pct (%) | 1.6 ± 0.2 | 1.6 ± 0.1 | 0.00 | −0.05 to 0.04 | 1.000 |
| Variable | CM-I | Control | Mean Difference | 95% Cl | p Value * |
|---|---|---|---|---|---|
| Total CSF Volume (cm3) | 194.2 ± 66.5 | 165.1 ± 35.2 | −29.12 | −41.64 to −16.59 | 0.002 |
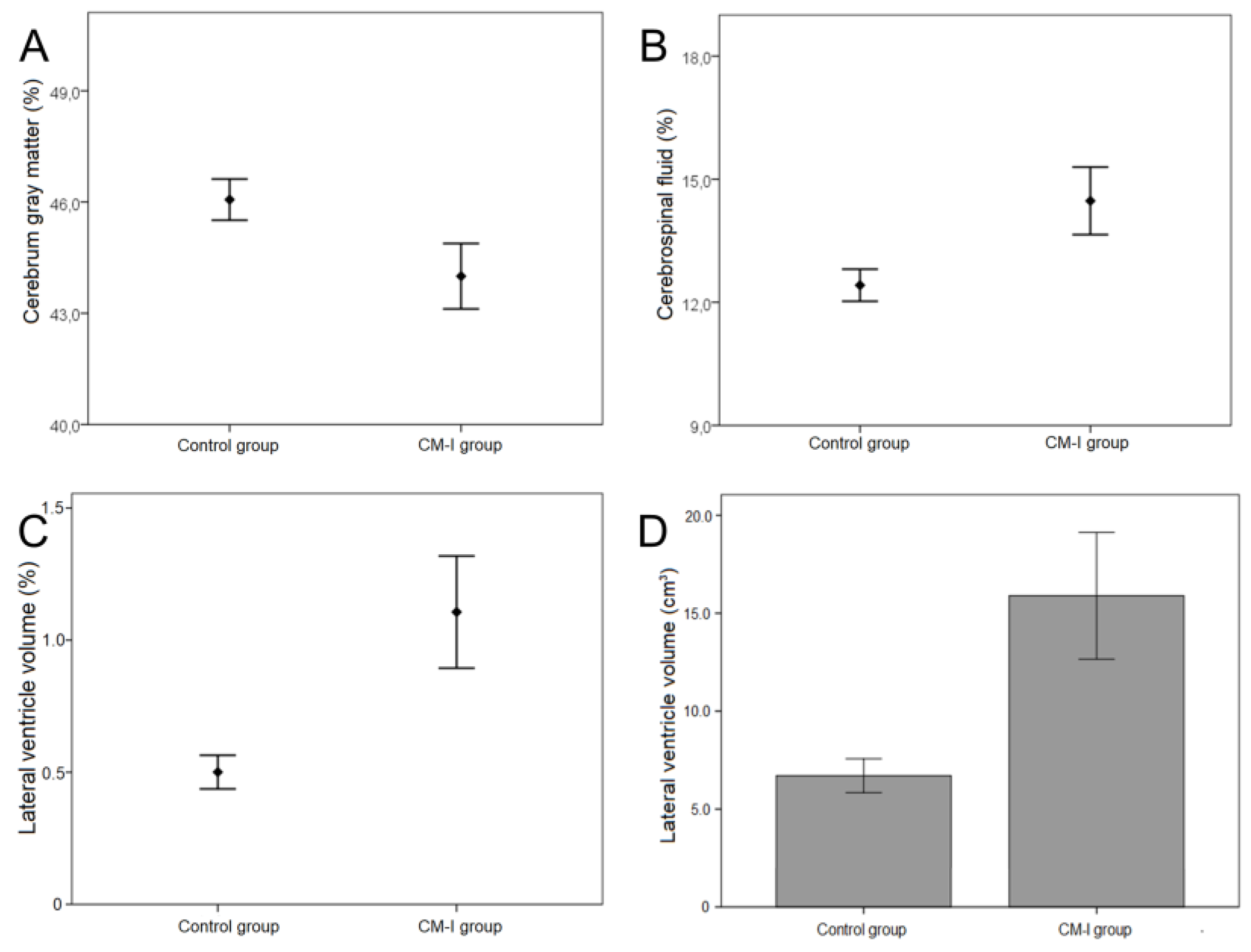
| Total CSF Pct (%) | 14.5 ± 4.9 | 12.4 ± 2.4 | −2.05 | −2.96 to −1.15 | 0.002 |
| Lateral ventricle Volume (cm3) | 15.9 ± 19.4 | 6.7 ± 5.2 | −9.24 | −12.58 to −5.91 | 0.002 |
| Lateral ventricle Pct (%) | 1.1 ± 1.3 | 0.5 ± 0.4 | −0.61 | −0.83 to −0.39 | 0.002 |
| Variables | CM-I | Control | Mean Difference | 95% Cl | p Value * |
|---|---|---|---|---|---|
| Cerebrum GM Volume (cm3) | 592.2 ± 94.3 | 612.3 ± 71.2 | 20.13 | 0.48 to 39.79 | 0.450 |
| Cerebrum GM Volume Pct (%) | 44.0 ± 5.3 | 46.1 ± 3.3 | 2.06 | 1.03 to 3.10 | 0.002 |
| Cerebrum WM Volume (cm3) | 412.1 ± 64.9 | 401.6 ± 53.1 | −10.47 | −24.43 to 3.48 | 1.000 |
| Cerebrum WM Volume Pct (%) | 30.6 ± 3.7 | 30.2 ± 3.0 | −0.42 | −1.22 to 0.37 | 1.000 |
| Cerebellum GM Volume (cm3) | 88.4 ± 15.0 | 90.6 ± 12.0 | 2.19 | −0.99 to 5.38 | 1.000 |
| Cerebellum GM Volume Pct (%) | 6.6 ± 1.0 | 6.8 ± 0.8 | 0.24 | 0.03 to 0.45 | 0.253 |
| Cerebellum WM Volume (cm3) | 36.1 ± 8.5 | 37.8 ± 8.1 | 1.76 | −0.18 to 3.71 | 0.672 |
| Cerebellum WM Volume Pct (%) | 2.7 ± 0.6 | 2.9 ± 0.6 | 0.17 | 0.03 to 0.31 | 0.228 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aydin, S.; Ozoner, B. Comparative Volumetric Analysis of the Brain and Cerebrospinal Fluid in Chiari Type I Malformation Patients: A Morphological Study. Brain Sci. 2019, 9, 260. https://doi.org/10.3390/brainsci9100260
Aydin S, Ozoner B. Comparative Volumetric Analysis of the Brain and Cerebrospinal Fluid in Chiari Type I Malformation Patients: A Morphological Study. Brain Sciences. 2019; 9(10):260. https://doi.org/10.3390/brainsci9100260
Chicago/Turabian StyleAydin, Seckin, and Baris Ozoner. 2019. "Comparative Volumetric Analysis of the Brain and Cerebrospinal Fluid in Chiari Type I Malformation Patients: A Morphological Study" Brain Sciences 9, no. 10: 260. https://doi.org/10.3390/brainsci9100260