
Effects of Transcranial Direct Current Stimulation on Clinical Features of Dizziness and Cortical Activation in a Patient with Vestibular Migraine


Abstract
:1. Introduction
2. Methods
2.1. Subjects
2.2. Transcranial Direct Current Stimulation (tDCS)
2.3. Functional Near-Infrared Spectroscopy (fNIRS)
2.4. Quantitative Electroencephalography (qEEG)
2.5. Dizziness Handicap Inventory (DHI)
2.6. Visual Vertigo Analog Scale (VVAS)
3. Results
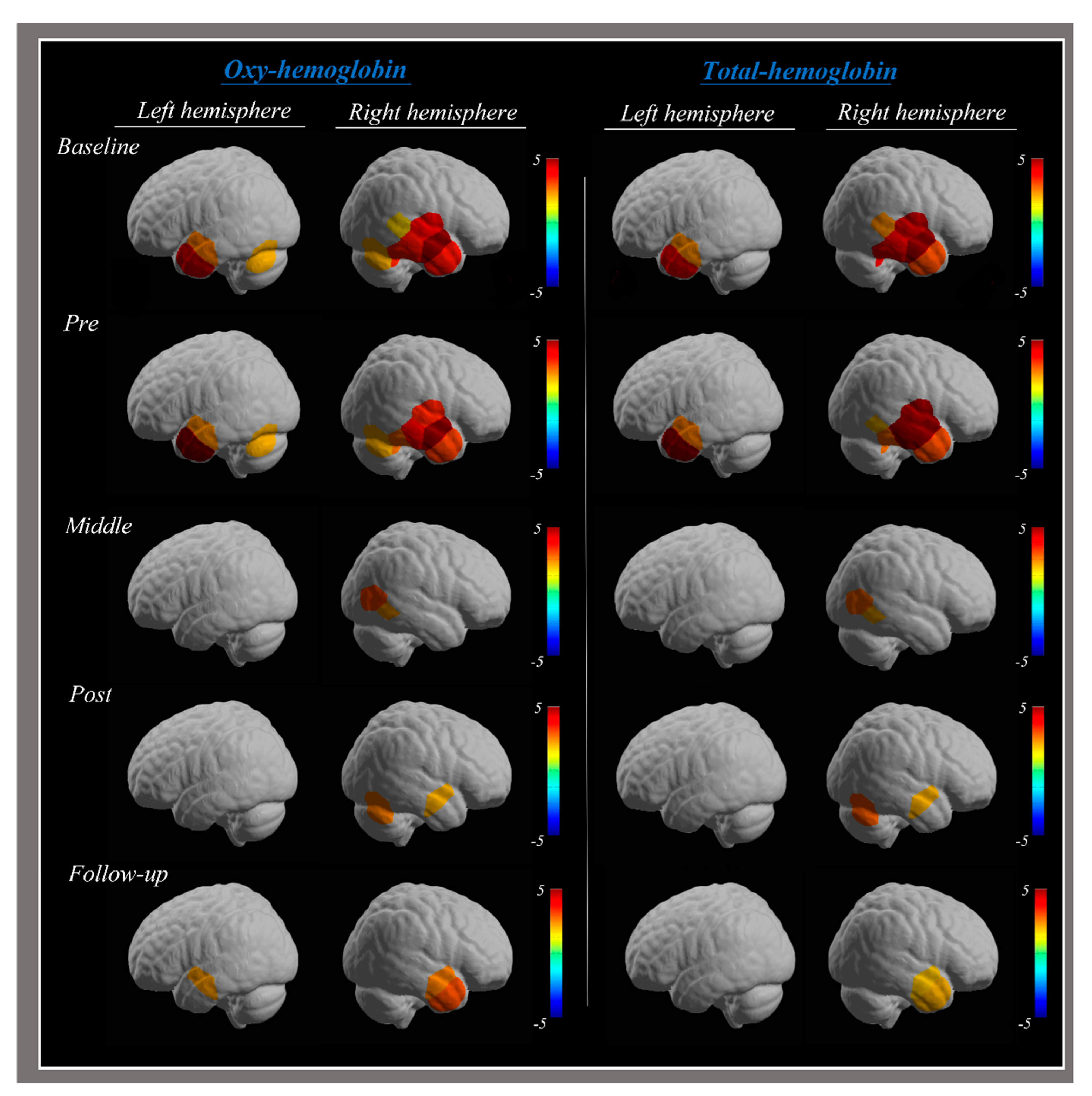
3.1. Functional Near-Infrared Spectroscopy (fNIRS)
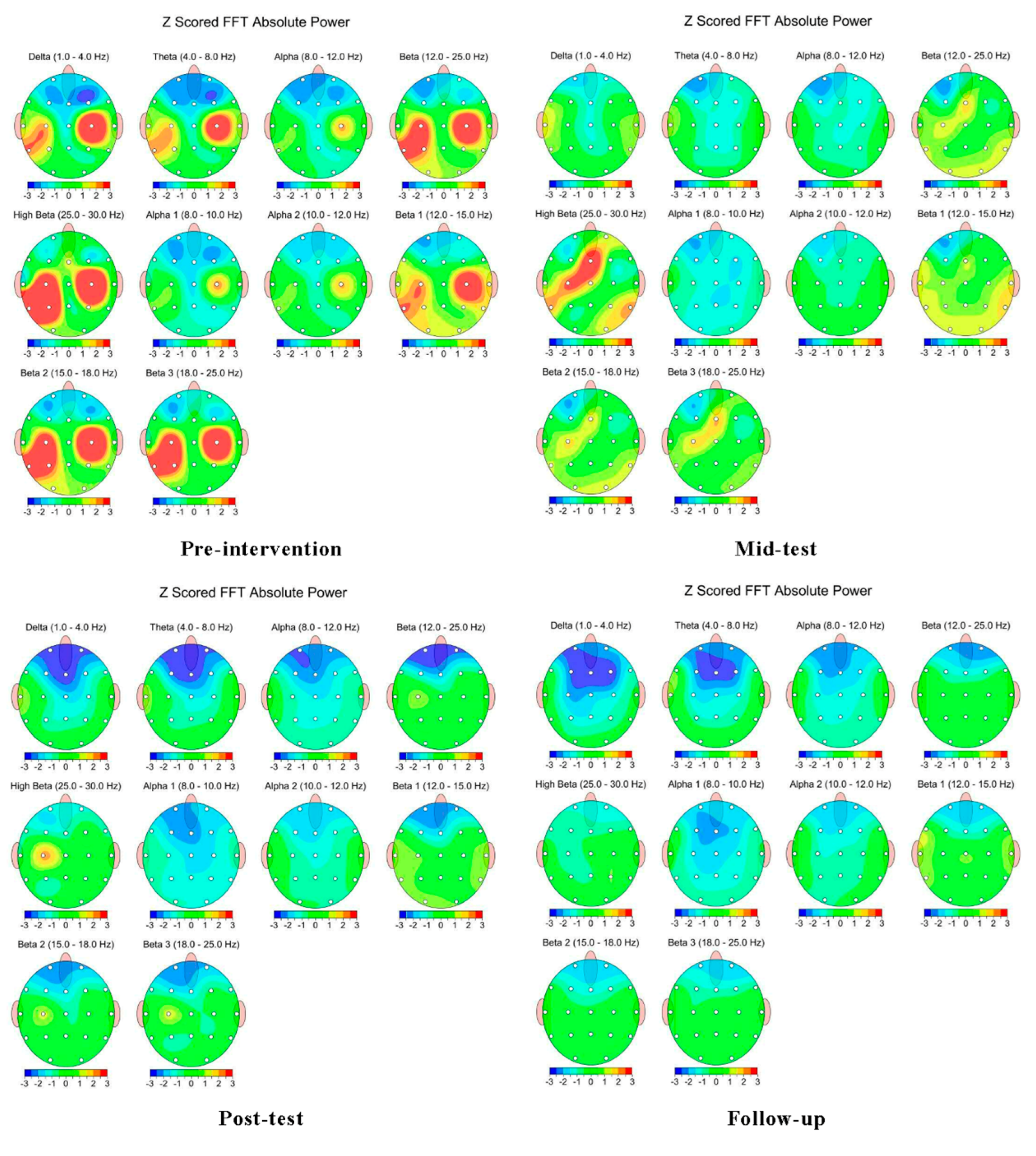
3.2. Quantitative Electroencephalography (qEEG)
3.3. Dizziness Handicap Inventory (DHI)
3.4. Visual Vertigo Analog Scale (VVAS)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wipperman, J. Dizziness and Vertigo. Prim. Care Clin. Off. Pract. 2014, 41, 115–131. [Google Scholar] [CrossRef] [PubMed]
- Sloane, P.D.; Baloh, R.W. Persistent Dizziness in Geriatric Patients. J. Am. Geriatr. Soc. 1989, 37, 1031–1038. [Google Scholar] [CrossRef]
- Bisdorff, A.; Von Brevern, M.; Lempert, T.; Newman-Toker, D.E. Classification of vestibular symptoms: Towards an international classification of vestibular disorders. J. Vestib. Res. 2009, 19, 1–13. [Google Scholar] [CrossRef]
- Sloane, P.D.; Coeytaux, R.R.; Beck, R.S.; Dallara, J. Dizziness: State of the Science. Ann. Intern. Med. 2001, 134, 823–832. [Google Scholar] [CrossRef] [PubMed]
- Formeister, E.J.; Rizk, H.G.; Kohn, M.A.; Sharon, J.D. The Epidemiology of Vestibular Migraine: A Population-based Survey Study. Otol. Neurotol. 2018, 39, 1037–1044. [Google Scholar] [CrossRef]
- Neuhauser, H.K.; Radtke, A.; von Brevern, M.; Feldmann, M.; Lezius, F.; Ziese, T.; Lempert, T. Migrainous vertigo: Prevalence and impact on quality of life. Neurology 2006, 67, 1028–1033. [Google Scholar] [CrossRef] [PubMed]
- Baloh, R.W. Vestibular Migraine I: Mechanisms, Diagnosis, and Clinical Features. Semin. Neurol. 2020, 40, 76–82. [Google Scholar] [CrossRef]
- Neuhauser, H.; Lempert, T. Vertigo and Dizziness Related to Migraine: A Diagnostic Challenge. Cephalalgia 2004, 24, 83–91. [Google Scholar] [CrossRef]
- Koganemaru, S.; Goto, F.; Arai, M.; Toshikuni, K.; Hosoya, M.; Wakabayashi, T.; Yamamoto, N.; Minami, S.; Ikeda, S.; Ikoma, K.; et al. Effects of vestibular rehabilitation combined with transcranial cerebellar direct current stimulation in patients with chronic dizziness: An exploratory study. Brain Stimul. 2017, 10, 576–578. [Google Scholar] [CrossRef]
- Eggers, S.D.Z. Migraine-related vertigo: Diagnosis and treatment. Curr. Pain Headache Rep. 2007, 11, 217–226. [Google Scholar] [CrossRef]
- Dunlap, P.M.; Holmberg, J.M.; Whitney, S.L. Vestibular rehabilitation: Advances in peripheral and central vestibular disorders. Curr. Opin. Neurol. 2019, 32, 137–144. [Google Scholar] [CrossRef]
- Saki, N.; Saki, N.; Bayat, A.; Bayat, A.; Nikakhlagh, S.; Nikakhlagh, S.; Mirmomeni, G.; Mirmomeni, G. Vestibular rehabilitation therapy in combination with transcranial direct current stimulation (tDCS) for treatment of chronic vestibular dysfunction in the elderly: A double-blind randomized controlled trial. Braz. J. Otorhinolaryngol. 2022, 88, 758–766. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Cohen, L.G.; Wassermann, E.M.; Priori, A.; Lang, N.; Antal, A.; Paulus, W.; Hummel, F.; Boggio, P.S.; Fregni, F.; et al. Transcranial direct current stimulation: State of the art 2008. Brain Stimul. 2008, 1, 206–223. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Paulus, W. Transcranial direct current stimulation—Update 2011. Restor. Neurol. Neurosci. 2011, 29, 463–492. [Google Scholar] [CrossRef]
- Ziemann, U.; Paulus, W.; Nitsche, M.A.; Pascual-Leone, A.; Byblow, W.D.; Berardelli, A.; Siebner, H.R.; Classen, J.; Cohen, L.G.; Rothwell, J.C. Consensus: Motor cortex plasticity protocols. Brain Stimul. 2008, 1, 164–182. [Google Scholar] [CrossRef] [PubMed]
- Hordacre, B.; Moezzi, B.; Ridding, M.C. Neuroplasticity and network connectivity of the motor cortex following stroke: A transcranial direct current stimulation study. Hum. Brain Mapp. 2018, 39, 3326–3339. [Google Scholar] [CrossRef] [PubMed]
- Hoppes, C.W.; Sparto, P.J.; Whitney, S.L.; Furman, J.M.; Huppert, T.J. Changes in cerebral activation in individuals with and without visual vertigo during optic flow: A functional near-infrared spectroscopy study. NeuroImage Clin. 2018, 20, 655–663. [Google Scholar] [CrossRef]
- Lopez, C.; Blanke, O.; Mast, F. The human vestibular cortex revealed by coordinate-based activation likelihood estimation meta-analysis. Neuroscience 2012, 212, 159–179. [Google Scholar] [CrossRef] [PubMed]
- Bense, S.; Stephan, T.; Yousry, T.A.; Brandt, T.; Dieterich, M.; Dlugaiczyk, J.; Gensberger, K.D.; Straka, H.; Frank, S.M.; Greenlee, M.W.; et al. Multisensory Cortical Signal Increases and Decreases During Vestibular Galvanic Stimulation (fMRI). J. Neurophysiol. 2001, 85, 886–899. [Google Scholar] [CrossRef] [PubMed]
- Dieterich, M.; Brandt, T. The parietal lobe and the vestibular system. Handb. Clin. Neurol. 2018, 151, 119–140. [Google Scholar] [CrossRef] [PubMed]
- Frank, S.M.; Greenlee, M.W. The parieto-insular vestibular cortex in humans: More than a single area? J. Neurophysiol. 2018, 120, 1438–1450. [Google Scholar] [CrossRef] [PubMed]
- Indovina, I.; Riccelli, R.; Chiarella, G.; Petrolo, C.; Augimeri, A.; Giofrè, L.; Lacquaniti, F.; Staab, J.P.; Passamonti, L. Role of the Insula and Vestibular System in Patients with Chronic Subjective Dizziness: An fMRI Study Using Sound-Evoked Vestibular Stimulation. Front. Behav. Neurosci. 2015, 9, 334. [Google Scholar] [CrossRef] [PubMed]
- Lempert, T.; Olesen, J.; Furman, J.; Waterston, J.; Seemungal, B.; Carey, J.; Bisdorff, A.; Versino, M.; Evers, S.; Newman-Toker, D. Vestibular migraine: Diagnostic criteria. J. Vestib. Res. 2012, 22, 167–172. [Google Scholar] [CrossRef]
- Olesen, J. Headache classification committee of the international headache society (IHS) the international classification of headache disorders. Cephalalgia 2018, 38, 1–211. [Google Scholar]
- Piper, S.K.; Krueger, A.; Koch, S.P.; Mehnert, J.; Habermehl, C.; Steinbrink, J.; Obrig, H.; Schmitz, C.H. A wearable multi-channel fNIRS system for brain imaging in freely moving subjects. NeuroImage 2014, 85 Pt 1, 64–71. [Google Scholar] [CrossRef]
- Morais, G.A.Z.; Balardin, J.B.; Sato, J.R. fNIRS Optodes’ Location Decider (fOLD): A toolbox for probe arrangement guided by brain regions-of-interest. Sci. Rep. 2018, 8, 3341. [Google Scholar] [CrossRef]
- Yeo, S.S.; Kwon, J.W.; Park, S.Y. EEG-based analysis of various sensory stimulation effects to reduce visually induced motion sickness in virtual reality. Sci. Rep. 2022, 12, 18043. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.M.; Ferreira, M.M.; Manso, A.; Ganança, M.M.; Caovilla, H.H.; Grigol, T.A.d.A.e.S. Dizziness Handicap Inventory and Visual Vertigo Analog Scale in Vestibular Dysfunction. Int. Arch. Otorhinolaryngol. 2016, 20, 241–243. [Google Scholar] [CrossRef]
- Dannenbaum, E.; Chilingaryan, G.; Fung, J. Visual vertigo analogue scale: An assessment questionnaire for visual vertigo. J. Vestib. Res. 2011, 21, 153–159. [Google Scholar] [CrossRef]
- Johkura, K.; Takahashi, K.; Kudo, Y.; Soma, T.; Asakawa, S.; Hasegawa, N.; Imamichi, S.; Kurihara, K. Cerebral perfusion changes in chronic dizziness: A single-photon emission computed tomography study. eNeurologicalSci 2021, 25, 100367. [Google Scholar] [CrossRef]
- Berger, A.; Horst, F.; Müller, S.; Steinberg, F.; Doppelmayr, M. Current State and Future Prospects of EEG and fNIRS in Robot-Assisted Gait Rehabilitation: A Brief Review. Front. Hum. Neurosci. 2019, 13, 172. [Google Scholar] [CrossRef] [PubMed]
- Abtahi, M.; Borgheai, S.B.; Jafari, R.; Constant, N.; Diouf, R.; Shahriari, Y.; Mankodiya, K. Merging fNIRS-EEG Brain Monitoring and Body Motion Capture to Distinguish Parkinsons Disease. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 1246–1253. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Session | Brain Region (Brodmann Area) | HbO | HbT | |
|---|---|---|---|---|
| Baseline | Rt | Superior Temporal Gyrus (BA 22) | 25 | 25 |
| Middle Temporal Gyrus (BA 21) | 6, 24, 26, 33 | 6, 24, 26, 33 | ||
| Inferior Temporal Gyrus (BA 20) | 20, 35 | 35 | ||
| Lt | Middle Temporal Gyrus (BA 21) | 23, 34 | 23, 34 | |
| Inferior Temporal Gyrus (BA 20) | 17 | - | ||
| Pre-test | Rt | Superior Temporal Gyrus (BA 22) | 25 | 25 |
| Middle Temporal Gyrus (BA 21) | 24, 26, 33 | 24, 26, 33 | ||
| Inferior Temporal Gyrus (BA 20) | 20, 35 | 35 | ||
| Lt | Middle Temporal Gyrus (BA 21) | 23, 34 | 23, 34 | |
| Inferior Temporal Gyrus (BA 20) | 17 | 17 | ||
| Mid-test | Rt | Middle Temporal Gyrus (BA 21) | 18 | 18 |
| Inferior Temporal Gyrus (BA 20) | 19 | 19 | ||
| Post-test | Rt | Middle Temporal Gyrus (BA 21) | 26 | 26 |
| Inferior Temporal Gyrus (BA 20) | 20 | 20 | ||
| Follow-up | Rt | Middle Temporal Gyrus (BA 21) | 26, 33 | 26, 33 |
| Lt | Middle Temporal Gyrus (BA 21) | 23 | - | |
| Pre-Test | Mid-Test | Post-Test | Follow-Up | ||
|---|---|---|---|---|---|
| Rt | FP2 | 0.24 | 1.13 | −1.11 | −1.32 |
| F4 | −0.99 | −0.08 | 0.05 | −0.59 | |
| C4 | 8.94 | −0.48 | −0.20 | 0.32 | |
| P4 | 1.49 | 1.03 | −0.37 | 0.52 | |
| O2 | 0.45 | 1.37 | −0.08 | 0.31 | |
| F8 | −0.49 | −0.23 | −0.59 | −0.48 | |
| T4 | −0.05 | −0.01 | −0.40 | 0.23 | |
| T6 | 0.17 | 2.30 | −0.24 | −0.30 | |
| Lt | FP1 | −0.87 | −0.73 | −1.42 | −1.09 |
| F3 | −0.74 | −0.68 | −0.88 | −0.58 | |
| C3 | 6.05 | 2.76 | 2.18 | −0.81 | |
| P3 | 7.89 | −0.08 | −0.55 | −0.48 | |
| O1 | 0.75 | 0.14 | −0.30 | 0.02 | |
| F7 | 0.04 | 0.04 | −0.77 | −0.76 | |
| T3 | −0.43 | 0.50 | −0.45 | −0.17 | |
| T5 | 8.95 | 2.28 | 0.03 | −0.28 |
| Pre-Test | Mid-Test | Post-Test | Follow-Up | ||
|---|---|---|---|---|---|
| DHI | Functional | 26 | 22 | 18 | 12 |
| Physical | 24 | 18 | 14 | 12 | |
| Emotional | 24 | 16 | 10 | 6 | |
| Total | 74 | 56 | 42 | 30 | |
| VVAS | Mild | 0 | 3 | 5 | 8 |
| Moderate | 7 | 6 | 4 | 1 | |
| Severe | 2 | 0 | 0 | 0 | |
| High | 8 | 6 | 5 | 4 | |
| Low | 6 | 3 | 2 | 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeo, S.S.; Kim, C.J.; Yun, S.H.; Son, S.M.; Kim, Y.J. Effects of Transcranial Direct Current Stimulation on Clinical Features of Dizziness and Cortical Activation in a Patient with Vestibular Migraine. Brain Sci. 2024, 14, 187. https://doi.org/10.3390/brainsci14020187
Yeo SS, Kim CJ, Yun SH, Son SM, Kim YJ. Effects of Transcranial Direct Current Stimulation on Clinical Features of Dizziness and Cortical Activation in a Patient with Vestibular Migraine. Brain Sciences. 2024; 14(2):187. https://doi.org/10.3390/brainsci14020187
Chicago/Turabian StyleYeo, Sang Seok, Chang Ju Kim, Seong Ho Yun, Sung Min Son, and Yoon Jae Kim. 2024. "Effects of Transcranial Direct Current Stimulation on Clinical Features of Dizziness and Cortical Activation in a Patient with Vestibular Migraine" Brain Sciences 14, no. 2: 187. https://doi.org/10.3390/brainsci14020187