
Effect of Anti-Interleukin-6 Agents on Psychopathology in a Sample of Patients with Post-COVID-19 Syndrome: An Observational Study
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Assessment
2.2. Statistical Analysis
3. Results
Effects of Possible Confounding Variables
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Simpson, R.J.; Hammacher, A.; Smith, D.K.; Matthews, J.M.; Ward, L.D. Interleukin-6: Structure-function relationships. Protein Sci. 1997, 6, 929–955. [Google Scholar] [CrossRef] [PubMed]
- Sehgal, P.B.; Zilberstein, A.; Ruggieri, R.M.; May, L.T.; Ferguson-Smith, A.; Slate, D.L.; Revel, M.; Ruddle, F.H. Human chromosome 7 carries the beta 2 interferon gene. Proc. Natl. Acad. Sci. USA 1986, 83, 5219–5222. [Google Scholar] [CrossRef] [PubMed]
- Grötzinger, J.; Kernebeck, T.; Kallen, K.J.; Rose-John, S. IL-6 type cytokine receptor complexes: Hexamer, tetramer or both? Biol. Chem. 1999, 380, 803–813. [Google Scholar] [CrossRef] [PubMed]
- Heinrich, P.C.; Behrmann, I.; Müller-Newen, G.; Schaper, F.; Graeve, L. Interleukin-6-type cytokine signalling through the gp130/Jak/STAT pathway. Biochem. J. 1998, 334, 297–314. [Google Scholar] [CrossRef] [PubMed]
- Hirano, T.; Yasukawa, K.; Harada, H.; Taga, T.; Watanabe, Y.; Matsuda, T.; Kashiwamura, S.; Nakajima, K.; Koyama, K.; Iwamatsu, A.; et al. Complementary DNA for a novel human interleukin (BSF-2) that induces B lymphocytes to produce immunoglobulin. Nature 1986, 324, 73–76. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Narazaki, M.; Kishimoto, T. IL-6 in inflammation, immunity, and disease. Cold Spring Harb. Perspect. Biol. 2014, 6, a016295. [Google Scholar] [CrossRef] [PubMed]
- Gubernatorova, E.O.; Gorshkova, E.A.; Namakanova, O.A.; Zvartsev, R.V.; Hidalgo, J.; Drutskaya, M.S.; Tumanov, A.V.; Nedospasov, S.A. Non-redundant functions of IL-6 produced by macrophages and dendritic cells in allergic airway inflammation. Front. Immunol. 2018, 9, 2718. [Google Scholar] [CrossRef] [PubMed]
- Scheller, J.; Chalaris, A.; Schmidt-Arras, D.; Rose-John, S. The pro- and anti-inflammatory properties of the cytokine interleukin-6. Biochim. Biophys. Acta 2011, 1813, 878–888. [Google Scholar] [CrossRef]
- Magro, G. SARS-CoV-2 and COVID-19: Is interleukin-6 (IL-6) the ‘culprit lesion’ of ARDS onset? What is there besides Tocilizumab? SGP130Fc. Cytokine X 2020, 2, 100. [Google Scholar] [CrossRef]
- Banks, W.A.; Kastin, A.J.; Gutierrez, E.G. Penetration of interleukin-6 across the murine blood-brain barrier. Neurosci. Lett. 1994, 179, 53–56. [Google Scholar] [CrossRef]
- Fernandes, G.L.; Araujo, P.; Tufik, S.; Andersen, M.L. The role of IL-6 and STAT in sleep and neuroinflammation. Clin. Immunol. 2017, 180, 58–59. [Google Scholar] [CrossRef] [PubMed]
- Castellanos, L.C.S.; Gatto, R.G.; Malnati, G.O.M.; Montes, M.M.; Uchitel, O.D.; Weissmann, C. Redistribution of ASIC1a channels triggered by IL-6: Potential role of ASIC1a in neuroinflammation. Biochim. Biophys. Acta Mol. Basis Dis. 2023, 1870, 166927. [Google Scholar] [CrossRef] [PubMed]
- Roohi, E.; Jaafari, N.; Hashemian, F. On inflammatory hypothesis of depression: What is the role of IL-6 in the middle of the chaos? J. Neuroinflamm. 2021, 18, 45. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M. Cytokine storm and immunomodulatory therapy in COVID-19: Role of chloroquine and anti-IL-6 monoclonal antibodies. Int. J. Antimicrob. Agents 2020, 55, 105982. [Google Scholar] [CrossRef] [PubMed]
- Bai, Z.; Gao, T.; Zhang, R.; Lu, Y.; Tian, J.; Wang, T.; Zhao, K.; Wang, H. Inhibition of IL-6 methylation by Saikosaponin C regulates neuroinflammation to alleviate depression. Int. Immunopharmacol. 2023, 118, 110043. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, R.R.; Amer, R.A.; Abozeid, A.A.; Elsharaby, R.M.; Shafik, N.M. Micro RNA 146a gene variant/TNF-α/IL-6/IL-1 β; A cross-link axis inbetween oxidative stress, endothelial dysfunction and neuro-inflammation in acute ischemic stroke and chronic schizophrenic patients. Arch. Biochem. Biophys. 2020, 679, 108193. [Google Scholar] [CrossRef] [PubMed]
- Mazza, M.; Caroppo, E.; De Berardis, D.; Marano, G.; Avallone, C.; Kotzalidis, G.D.; Janiri, D.; Moccia, L.; Simonetti, A.; Conte, E.; et al. Psychosis in Women: Time for Personalized Treatment. J. Pers. Med. 2021, 11, 1279. [Google Scholar] [CrossRef] [PubMed]
- Simonetti, A.; Koukopoulos, A.E.; Kotzalidis, G.D.; Janiri, D.; De Chiara, L.; Janiri, L.; Sani, G. Stabilization Beyond Mood: Stabilizing Patients with Bipolar Disorder in the Various Phases of Life. Front. Psychiatry 2020, 11, 247. [Google Scholar] [CrossRef]
- Elbadawy, H.M.; Khattab, A.; El-Agamy, D.S.; Eltahir, H.M.; Alhaddad, A.; Aljohani, F.D.; Almuzaini, T.M.; Abouzied, M.M.; Aldhafiri, A. IL-6 at the center of cytokine storm: Circulating inflammation mediators as biomarkers in hospitalized COVID-19 patients. J. Clin. Lab. Anal. 2023, 37, e24881. [Google Scholar] [CrossRef]
- Frisoni, P.; Neri, M.; D’Errico, S.; Alfieri, L.; Bonuccelli, D.; Cingolani, M.; Di Paolo, M.; Gaudio, R.M.; Lestani, M.; Marti, M.; et al. Cytokine storm and histopathological findings in 60 cases of COVID-19-related death: From viral load research to immunohistochemical quantification of major players IL-1β, IL-6, IL-15 and TNF-α. Forensic Sci. Med. Pathol. 2022, 18, 4–19. [Google Scholar] [CrossRef]
- Ganesh, R.; Grach, S.L.; Ghosh, A.K.; Bierle, D.M.; Salonen, B.R.; Collins, N.M.; Joshi, A.Y.; Boeder NDJr Anstine, C.V.; Mueller, M.R.; Wight, E.C.; et al. The female-predominant persistent immune dysregulation of the post-COVID syndrome. Mayo Clin. Proc. 2022, 97, 454–464. [Google Scholar] [CrossRef] [PubMed]
- Raveendran, A.V.; Jayadevan, R.; Sashidharan, S. Long COVID: An overview. Diabetes Metab. Syndr. 2021, 15, 869–875, Erratum in Diabetes Metab. Syndr. 2022, 16, 102504; Erratum in Diabetes Metab. Syndr. 2022, 16, 102660. [Google Scholar] [CrossRef]
- Chakraborty, C.; Sharma, A.R.; Bhattacharya, M.; Sharma, G.; Lee, S.S.; Agoramoorthy, G. COVID-19: Consider IL-6 receptor antagonist for the therapy of cytokine storm syndrome in SARS-CoV-2 infected patients. J. Med. Virol. 2020, 92, 2260–2262. [Google Scholar] [CrossRef] [PubMed]
- Oldfield, V.; Dhillon, S.; Plosker, G.L. Tocilizumab: A review of its use in the management of rheumatoid arthritis. Drugs 2009, 69, 609–632. [Google Scholar] [CrossRef] [PubMed]
- Sheppard, M.; Laskou, F.; Stapleton, P.P.; Hadavi, S.; Dasgupta, B. Tocilizumab (Actemra). Hum. Vaccines Immunother. 2017, 13, 1972–1988. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency (EMA). EMA Recommends Approval for Use of RoActemra in Adults with Severe COVID-19. News 6 December 2021. Available online: https://www.ema.europa.eu/en/news/ema-recommends-approval-use-roactemra-adults-severe-covid-19 (accessed on 22 November 2023).
- Food and Drug Administration (FDA). Frequently Asked Questions on the Emergency Use Authorization for Actemra (Tocilizumab) for Treatment of COVID-19. Available online: https://www.fda.gov/media/150345/download (accessed on 22 November 2023).
- Scott, L.J. Sarilumab: First global approval. Drugs 2017, 77, 705–712. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency (EMA). Committee for Medicinal Products for Human Use (CHMP), Assessment report Kevzara, International Non-Proprietary Name: Sarilumab. Procedure No. EMEA/H/C/004254/0000. EMA/292840/2017. 21 April 2017. Available online: https://www.ema.europa.eu/en/documents/assessment-report/kevzara-epar-public-assessment-report_en.pdf (accessed on 23 November 2023).
- Huizinga, T.W.; Fleischmann, R.M.; Jasson, M.; Radin, A.R.; van Adelsberg, J.; Fiore, S.; Huang, X.; Yancopoulos, G.D.; Stahl, N.; Genovese, M.C. Sarilumab, a fully human monoclonal antibody against IL-6Rα in patients with rheumatoid arthritis and an inadequate response to methotrexate: Efficacy and safety results from the randomised SARIL-RA-MOBILITY Part A trial. Ann. Rheum. Dis. 2014, 73, 1626–1634. [Google Scholar] [CrossRef]
- Genovese, M.C.; Fleischmann, R.; Kivitz, A.J.; Rell-Bakalarska, M.; Martincova, R.; Fiore, S.; Rohane, P.; van Hoogstraten, H.; Garg, A.; Fan, C.; et al. Sarilumab plus methotrexate in patients with active rheumatoid arthritis and inadequate response to methotrexate: Results of a phase III study. Arthritis Rheumatol. 2015, 67, 1424–1437. [Google Scholar] [CrossRef]
- Burmester, G.R.; Lin, Y.; Patel, R.; van Adelsberg, J.; Mangan, E.K.; Graham, N.M.; van Hoogstraten, H.; Bauer, D.; Ignacio Vargas, J.; Lee, E.B. Efficacy and safety of sarilumab monotherapy versus adalimumab monotherapy for the treatment of patients with active rheumatoid arthritis (MONARCH): A randomised, double-blind, parallel-group phase III trial. Ann. Rheum. Dis. 2017, 76, 840–847. [Google Scholar] [CrossRef]
- Boyce, E.G.; Rogan, E.L.; Vyas, D.; Prasad, N.; Mai, Y. Sarilumab: Review of a second IL-6 receptor antagonist indicated for the treatment of rheumatoid arthritis. Ann. Pharmacother. 2018, 52, 780–791. [Google Scholar] [CrossRef]
- Spiera, R.F.; Unizony, S.; Warrington, K.J.; Sloane, J.; Giannelou, A.; Nivens, M.C.; Akinlade, B.; Wong, W.; Bhore, R.; Lin, Y.; et al. Sarilumab for relapse of polymyalgia rheumatica during glucocorticoid taper. N. Engl. J. Med. 2023, 389, 1263–1272. [Google Scholar] [CrossRef] [PubMed]
- Chamlagain, R.; Shah, S.; Sharma Paudel, B.; Dhital, R.; Kandel, B. Efficacy and safety of sarilumab in COVID-19: A systematic review. Interdiscip. Perspect. Infect. Dis. 2021, 2021, 8903435. [Google Scholar] [CrossRef] [PubMed]
- Lescure, F.X.; Honda, H.; Fowler, R.A.; Lazar, J.S.; Shi, G.; Wung, P.; Patel, N.; Hagino, O.; Sarilumab COVID-19 Global Study Group. Sarilumab in patients admitted to hospital with severe or critical COVID-19: A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Respir. Med. 2021, 9, 522–532. [Google Scholar] [CrossRef] [PubMed]
- Sivapalasingam, S.; Lederer, D.J.; Bhore, R.; Hajizadeh, N.; Criner, G.; Hosain, R.; Mahmood, A.; Giannelou, A.; Somersan-Karakaya, S.; O’Brien, M.P.; et al. Efficacy and Safety of Sarilumab in Hospitalized Patients with Coronavirus Disease 2019: A Randomized Clinical Trial. Clin. Infect. Dis. 2022, 75, e380–e388. [Google Scholar] [CrossRef] [PubMed]
- Mastrorosa, I.; Gagliardini, R.; Segala, F.V.; Mondi, A.; Lorenzini, P.; Cerva, C.; Taddei, E.; Bai, F.; Vergori, A.; Marcantonio, N.; et al. Sarilumab plus standard of care vs standard of care for the treatment of severe COVID-19: A phase 3, randomized, open-labeled, multi-center study (ESCAPE study). EClinicalMedicine 2023, 57, 101895. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Therapeutics and COVID-19. Living Guideline 6 July 2021; WHO Reference Number: WHO/2019-nCoV/therapeutics/2021.2; World Health Organization: Geneva, Switzerland, 2021; Available online: https://iris.who.int/bitstream/handle/10665/342368/WHO-2019-nCoV-therapeutics-2021.2-eng.pdf (accessed on 23 November 2023).
- Agenzia Italiana del Farmaco (AIFA), Sarilumab Nella Terapia Dei Pazienti Adulti con COVID-19, Linee Guida AIFA, 2021; CTS. 23 September 2021. Available online: https://www.aifa.gov.it/documents/20142/1123276/Sarilumab_28.09.2021.pdf (accessed on 21 November 2023).
- Lesmana, M.H.S.; Le, N.Q.K.; Chiu, W.C.; Chung, K.H.; Wang, C.Y.; Irham, L.M.; Chung, M.H. Genomic-analysis-oriented drug repurposing in the search for novel antidepressants. Biomedicines 2022, 10, 1947. [Google Scholar] [CrossRef] [PubMed]
- Khandaker, G.M.; Oltean, B.P.; Kaser, M.; Dibben, C.R.M.; Ramana, R.; Jadon, D.R.; Dantzer, R.; Coles, A.J.; Lewis, G.; Jones, P.B. Protocol for the insight study: A randomised controlled trial of single-dose tocilizumab in patients with depression and low-grade inflammation. BMJ Open 2018, 8, e025333. [Google Scholar] [CrossRef]
- Traki, L.; Rostom, S.; Tahiri, L.; Bahiri, R.; Harzy, T.; Abouqal, R.; Hajjaj-Hassouni, N. Responsiveness of the EuroQol EQ-5D and Hospital Anxiety and Depression Scale (HADS) in rheumatoid arthritis patients receiving tocilizumab. Clin. Rheumatol. 2014, 33, 1055–1060. [Google Scholar] [CrossRef]
- Tiosano, S.; Yavne, Y.; Watad, A.; Langevitz, P.; Lidar, M.; Feld, J.; Tishler, M.; Aamar, S.; Elkayam, O.; Balbir-Gurman, A.; et al. The impact of tocilizumab on anxiety and depression in patients with rheumatoid arthritis. Eur. J. Clin. Investig. 2020, 50, e13268. [Google Scholar] [CrossRef]
- Behrens, F.; Burmester, G.R.; Feuchtenberger, M.; Kellner, H.; Kuehne, C.; Liebhaber, A.; Wassenberg, S.; Gerlach, J.; Zortel, M.; Hofmann, M.W.; et al. Characterisation of depressive symptoms in rheumatoid arthritis patients treated with tocilizumab during routine daily care. Clin. Exp. Rheumatol. 2022, 40, 551–559. [Google Scholar] [CrossRef]
- Knight, J.M.; Costanzo, E.S.; Singh, S.; Yin, Z.; Szabo, A.; Pawar, D.S.; Hillard, C.J.; Rizzo, J.D.; D’Souza, A.; Pasquini, M.; et al. The IL-6 antagonist tocilizumab is associated with worse depression and related symptoms in the medically ill. Transl. Psychiatry 2021, 11, 58. [Google Scholar] [CrossRef] [PubMed]
- Chakravarty, R.; Jyani, G.; Paul, S.; Mohindra, R.; Goyal, M.; Suri, V.; Bhalla, A.; Singh, S.M. Depression, anxiety, and quality of life in patients treated with single infusion tocilizumab for COVID-19: A follow-up, controlled study. Indian J. Psychol. Med. 2023, 45, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Strand, V.; Boklage, S.H.; Kimura, T.; Joly, F.; Boyapati, A.; Msihid, J. High levels of interleukin-6 in patients with rheumatoid arthritis are associated with greater improvements in health-related quality of life for sarilumab compared with adalimumab. Arthritis Res. Ther. 2020, 22, 250. [Google Scholar] [CrossRef] [PubMed]
- Munblit, D.; Nicholson, T.R.; Needham, D.M.; Seylanova, N.; Parr, C.; Chen, J.; Kokorina, A.; Sigfrid, L.; Buonsenso, D.; Bhatnagar, S.; et al. Studying the post-COVID-19 condition: Research challenges, strategies, and importance of Core Outcome Set development. BMC Med. 2022, 20, 50. [Google Scholar] [CrossRef] [PubMed]
- Ventura, J.; Green, M.F.; Shaner, A.; Liberman, R.P. Training and quality assurance with the Brief Psychiatric Rating Scale: “The drift busters”. Int. J. Methods Psychiatr. Res. 1993, 3, 221–244. [Google Scholar]
- Roncone, R.; Ventura, J.; Impallomeni, M.; Falloon, I.R.; Morosini, P.L.; Chiaravalle, E.; Casacchia, M. Reliability of an Italian standardized and expanded Brief Psychiatric Rating Scale (BPRS 4.0) in raters with high vs. low clinical experience. Acta Psychiatr. Scand. 1999, 100, 229–236. [Google Scholar] [CrossRef]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef]
- Hamilton, M. The assessment of anxiety states by rating. Br. J. Med. Psychol. 1959, 32, 50–55. [Google Scholar] [CrossRef]
- Weathers, F.W.; Bovin, M.J.; Lee, D.J.; Sloan, D.M.; Schnurr, P.P.; Kaloupek, D.G.; Keane, T.M.; Marx, B.P. The Clinician-Administered PTSD Scale for DSM-5 (CAPS-5): Development and initial psychometric evaluation in military veterans. Psychol. Assess. 2018, 30, 383–395. [Google Scholar] [CrossRef]
- Koukopoulos, A.E.; Simonetti, A.; Janiri, D.; De Chiara, L.; Kotzalidis, G.D.; Sani, G. Validazione della versione italiana della Koukopoulos Mixed Depression Rating Scale (KMDRS) in un campione di pazienti italiani affetti da disturbi dell’umore [Validation of the Italian version of the Koukopoulos Mixed Depression Rating Scale (KMDRS) in an Italian sample of subjects with mood disorders]. Riv. Psichiatr. 2020, 55, 281–291. (In Italian) [Google Scholar] [CrossRef]
- Connor, K.M.; Davidson, J.R. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Weissman, A.; Lester, D.; Trexler, L. The measurement of pessimism: The hopelessness scale. J. Consult. Clin. Psychol. 1974, 42, 861–865. [Google Scholar] [CrossRef] [PubMed]
- Gratz, K.L.; Roemer, L. Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the difficulties in emotion regulation scale. J. Psychopathol. Behav. Assess. 2004, 26, 41–54. [Google Scholar] [CrossRef]
- Sighinolfi, C.; Pala, A.N.; Chiri, L.R.; Marchetti, I.; Sica, C. Difficulties in Emotion Regulation Scale (DERS): Traduzione e adattamento Italiano [Difficulties in Emotion Regulation Scale (DERS): The Italian translation and adaptation]. Psicoter. Cogn. Comport. 2010, 16, 141–170. [Google Scholar]
- Snaith, R.P.; Hamilton, M.; Morley, S.; Humayan, A.; Hargreaves, D.; Trigwell, P. A scale for the assessment of hedonic tone the Snaith-Hamilton Pleasure Scale. Br. J. Psychiatry 1995, 167, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Santangelo, G.; Morgante, L.; Savica, R.; Marconi, R.; Grasso, L.; Antonini, A.; De Gaspari, D.; Ottaviani, D.; Tiple, D.; Simoni, L.; et al. Anhedonia and cognitive impairment in Parkinson’s disease: Italian validation of the Snaith-Hamilton Pleasure Scale and its application in the clinical routine practice during the PRIAMO study. Park. Relat. Disord. 2009, 15, 576–581. [Google Scholar] [CrossRef]
- Agenzia Italiana del Farmaco (AIFA). Tocilizumab Nella Terapia Dei Pazienti Adulti Con COVID-19, Linee Guida AIFA, 2021; CTS. 9 June 2021. Available online: https://www.aifa.gov.it/documents/20142/1267737/Tocilizumab_09.06.2021.pdf (accessed on 21 November 2023).
- Salama, C.; Han, J.; Yau, L.; Reiss, W.G.; Kramer, B.; Neidhart, J.D.; Criner, G.J.; Kaplan-Lewis, E.; Baden, R.; Pandit, L.; et al. Tocilizumab in patients hospitalized with COVID-19 pneumonia. N. Engl. J. Med. 2021, 384, 20–30. [Google Scholar] [CrossRef]
- Rosas, I.O.; Bräu, N.; Waters, M.; Go, R.C.; Hunter, B.D.; Bhagani, S.; Skiest, D.; Aziz, M.S.; Cooper, N.; Douglas, I.S.; et al. Tocilizumab in hospitalized patients with severe COVID-19 pneumonia. N. Engl. J. Med. 2021, 384, 1503–1516. [Google Scholar] [CrossRef]
- RECOVERY Collaborative Group. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2021, 397, 1637–1645. [Google Scholar] [CrossRef]
- Writing Committee for the REMAP-CAP Investigators; Higgins, A.M.; Berry, L.R.; Lorenzi, E.; Murthy, S.; McQuilten, Z.; Mouncey, P.R.; Al-Beidh, F.; Annane, D.; Arabi, Y.M.; et al. Long-term (180-day) outcomes in critically ill patients with COVID-19 in the REMAP-CAP randomized clinical trial. JAMA 2023, 329, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Emery, P.; Rondon, J.; Parrino, J.; Lin, Y.; Pena-Rossi, C.; van Hoogstraten, H.; Graham, N.M.H.; Liu, N.; Paccaly, A.; Wu, R.; et al. Safety and tolerability of subcutaneous sarilumab and intravenous tocilizumab in patients with rheumatoid arthritis. Rheumatology 2019, 58, 849–858. [Google Scholar] [CrossRef] [PubMed]
- Emery, P.; van Hoogstraten, H.; Thangavelu, K.; Mangan, E.; St John, G.; Verschueren, P. Subcutaneous sarilumab in patients with rheumatoid arthritis who previously received subcutaneous sarilumab or intravenous tocilizumab: An open-label extension of a randomized clinical trial. ACR Open Rheumatol. 2020, 2, 672–680. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.Y.; Koh, D.H.; Choi, M.; Ryoo, S.; Huh, K.; Yeom, J.S.; Yoon, Y.K. Clinical efficacy and safety of interleukin-6 receptor antagonists (tocilizumab and sarilumab) in patients with COVID-19: A systematic review and meta-analysis. Emerg. Microbes Infect. 2022, 11, 1154–1165. [Google Scholar] [CrossRef]
- Godolphin, P.J.; Fisher, D.J.; Berry, L.R.; Derde, L.P.G.; Diaz, J.V.; Gordon, A.C.; Lorenzi, E.; Marshall, J.C.; Murthy, S.; Shankar-Hari, M.; et al. Association between tocilizumab, sarilumab and all-cause mortality at 28 days in hospitalised patients with COVID-19: A network meta-analysis. PLoS ONE 2022, 17, e0270668. [Google Scholar] [CrossRef]
- Albuquerque, A.M.; Eckert, I.; Tramujas, L.; Butler-Laporte, G.; McDonald, E.G.; Brophy, J.M.; Lee, T.C. Effect of tocilizumab, sarilumab, and baricitinib on mortality among patients hospitalized for COVID-19 treated with corticosteroids: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2023, 29, 13–21. [Google Scholar] [CrossRef]
- Swets, M.C.; Moss, R.J.; Kor, F.; Hilarius, D.; Moes, D.J.A.R.; Berkhout, W.E.; van den Toorn, L.M.; van den Oever, N.C.G.; de Valk, R.; Rosendaal, F.R.; et al. A comparison of the effectiveness of different doses of tocilizumab and sarilumab in the treatment of severe COVID-19: A natural experiment due to drug shortages. Int. J. Infect. Dis. 2023, 129, 57–62. [Google Scholar] [CrossRef]
- Zeraatkar, D.; Cusano, E.; Martínez, J.P.D.; Qasim, A.; Mangala, S.; Kum, E.; Bartoszko, J.J.; Devji, T.; Agoritsas, T.; Guyatt, G.; et al. Use of tocilizumab and sarilumab alone or in combination with corticosteroids for COVID-19: Systematic review and network meta-analysis. BMJ Med. 2022, 1, e000036. [Google Scholar] [CrossRef]
- Wang, J.; Levi, J.; Ellis, L.; Hill, A. Minimum Manufacturing Costs, National Prices, and Estimated Global Availability of New Repurposed Therapies for Coronavirus Disease 2019. Open Forum Infect. Dis. 2021, 9, ofab581. [Google Scholar] [CrossRef]
- Saito, S.; Suzuki, K.; Yoshimoto, K.; Kondo, Y.; Kikuchi, J.; Hanaoka, H.; Kaneko, Y.; Takeuchi, T. Differences in the strength of inhibition of interleukin-6 signalling by subcutaneous sarilumab and tocilizumab in rheumatoid arthritis patients. Clin. Exp. Rheumatol. 2023, 41, 1451–1455. [Google Scholar] [CrossRef]
- Xu, C.; Rafique, A.; Potocky, T.; Paccaly, A.; Nolain, P.; Lu, Q.; Iglesias-Rodriguez, M.; St John, G.; Nivens, M.C.; Kanamaluru, V.; et al. Differential binding of sarilumab and tocilizumab to IL-6Rα and effects of receptor occupancy on clinical parameters. J. Clin. Pharmacol. 2021, 61, 714–724. [Google Scholar] [CrossRef] [PubMed]
- Charpentier Mora, S.; Bastianoni, C.; Cavanna, D.; Bizzi, F. Emerging adults facing the COVID-19 pandemic: Emotion dysregulation, mentalizing, and psychological symptoms. Curr. Psychol. 2022, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Sani, G.; Janiri, D.; Moccia, L.; Albert, U.; Carrà, G.; Carmassi, C.; Cirulli, F.; Dell’Osso, B.; Menculini, G.; Nanni, M.G.; et al. Psychopathological burden and coping strategies among frontline and second-line Italian healthcare workers facing the COVID-19 emergency: Findings from the COMET collaborative network. J. Affect. Disord. 2022, 311, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Velotti, P.; Rogier, G.; Beomonte Zobel, S.; Castellano, R.; Tambelli, R. Loneliness, emotion dysregulation, and internalizing symptoms during Coronavirus Disease 2019: A structural equation modeling approach. Front. Psychiatry 2021, 11, 581494. [Google Scholar] [CrossRef] [PubMed]
- Simonetti, A.; Lijffijt, M.; Kahlon, R.S.; Gandy, K.; Arvind, R.P.; Amin, P.; Arciniegas, D.B.; Swann, A.C.; Soares, J.C.; Saxena, K. Early and late cortical reactivity to passively viewed emotional faces in pediatric bipolar disorder. J. Affect. Disord. 2019, 253, 240–247. [Google Scholar] [CrossRef] [PubMed]
- Moccia, L.; Janiri, D.; Giuseppin, G.; Agrifoglio, B.; Monti, L.; Mazza, M.; Caroppo, E.; Fiorillo, A.; Sani, G.; Di Nicola, M.; et al. Reduced hedonic tone and emotion dysregulation predict depressive symptoms severity during the COVID-19 outbreak: An observational study on the Italian general population. Int. J. Environ. Res. Public Health 2020, 18, 255. [Google Scholar] [CrossRef]
- Patel, H.; Easterbrook, B.; D’Alessandro-Lowe, A.M.; Andrews, K.; Ritchie, K.; Hosseiny, F.; Rodrigues, S.; Malain, A.; O’Connor, C.; Schielke, H.; et al. Associations between trauma and substance use among healthcare workers and public safety personnel during the SARS-CoV-2 (COVID-19) pandemic: The mediating roles of dissociation and emotion dysregulation. Eur. J. Psychotraumatol. 2023, 14, 2180706. [Google Scholar] [CrossRef]
- Gadient, R.A.; Otten, U. Expression of interleukin-6 (IL-6) and interleukin-6 receptor (IL-6R) mRNAs in rat brain during postnatal development. Brain Res. 1994, 637, 10–14. [Google Scholar] [CrossRef]
- Schöbitz, B.; de Kloet, E.R.; Sutanto, W.; Holsboer, F. Cellular localization of interleukin 6 mRNA and interleukin 6 receptor mRNA in rat brain. Eur. J. Neurosci. 1993, 5, 1426–1435. [Google Scholar] [CrossRef]
- LeMay, L.G.; Vander, A.J.; Kluger, M.J. The effects of psychological stress on plasma interleukin-6 activity in rats. Physiol. Behav. 1990, 47, 957–961. [Google Scholar] [CrossRef]
- Wu, T.H.; Lin, C.H. IL-6 mediated alterations on immobile behavior of rats in the forced swim test via ERK1/2 activation in specific brain regions. Behav. Brain Res. 2008, 193, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Roberts, A.J.; Khom, S.; Bajo, M.; Vlkolinsky, R.; Polis, I.; Cates-Gatto, C.; Roberto, M.; Gruol, D.L. Increased IL-6 expression in astrocytes is associated with emotionality, alterations in central amygdala GABAergic transmission, and excitability during alcohol withdrawal. Brain Behav. Immun. 2019, 82, 188–202. [Google Scholar] [CrossRef] [PubMed]
- Gilpin, N.W.; Herman, M.A.; Roberto, M. The central amygdala as an integrative hub for anxiety and alcohol use disorders. Biol. Psychiatry 2015, 77, 859–869. [Google Scholar] [CrossRef] [PubMed]
- Mihara, M.; Kasutani, K.; Okazaki, M.; Nakamura, A.; Kawai, S.; Sugimoto, M.; Matsumoto, Y.; Ohsugi, Y. Tocilizumab inhibits signal transduction mediated by both mIL-6R and sIL-6R, but not by the receptors of other members of IL-6 cytokine family. Int. Immunopharmacol. 2005, 5, 1440–1731. [Google Scholar] [CrossRef] [PubMed]
- Baier, P.C.; May, U.; Scheller, J.; Rose-John, S.; Schiffelholz, T. Impaired hippocampus-dependent and -independent learning in IL-6 deficient mice. Behav. Brain Res. 2009, 200, 192–196. [Google Scholar] [CrossRef] [PubMed]
- Erta, M.; Giralt, M.; Esposito, F.L.; Fernandez-Gayol, O.; Hidalgo, J. Astrocytic IL-6 mediates locomotor activity, exploration, anxiety, learning and social behavior. Horm. Behav. 2015, 73, 64–74. [Google Scholar] [CrossRef]
- Janiri, D.; Sani, G.; Rossi, P.; Piras, F.; Iorio, M.; Banaj, N.; Giuseppin, G.; Spinazzola, E.; Maggiora, M.; Ambrosi, E.; et al. Amygdala and hippocampus volumes are differently affected by childhood trauma in patients with bipolar disorders and healthy controls. Bipolar Disord. 2017, 19, 353–362. [Google Scholar] [CrossRef]
- De Filippis, S.; Cuomo, I.; Lionetto, L.; Janiri, D.; Simmaco, M.; Caloro, M.; De Persis, S.; Piazzi, G.; Simonetti, A.; Telesforo, C.L.; et al. Intramuscular aripiprazole in the acute management of psychomotor agitation. Pharmacotherapy 2013, 33, 603–614. [Google Scholar] [CrossRef]


{kind=link}
| Ctrl (N = 158) | Anti-IL-6-R (N = 88) | U or χ2 | p-Value | |
|---|---|---|---|---|
| Sociodemographic and clinical characteristics | ||||
| Age (y), mean ± SD | 56.66 ± 10.30 | 56.90 ± 12.12 | 6640 | 0.56 |
| Female, n (%) | 58 (36.7) | 26 (29.5) | 1.29 | 0.26 |
| Marital Status (%) | ||||
| Never married | 18 (11.5) | 15 (17) | 4.94 | 0.29 |
| Married | 101 (63.9) | 61 (69.3) | ||
| Partner | 7 (4.4) | 2 (2.3) | ||
| Divorced | 7 (4.4) | 2 (2.3) | ||
| Widowed | 25 (15.8) | 8 (9.1) | ||
| Occupation (%) | ||||
| Unemployed | 9 (5.6) | 7 (7.9) | 1.85 | 0.60 |
| Employed | 117 (74.1) | 62 (70.5) | ||
| Retired | 32 (20.3) | 19 (21.6) | ||
| BMI, mean ± SD | 28.0 ± 4.57 | 28.23 ± 4.65 | 6597 | 0.66 |
| Education (y), mean ± SD | 12.80 ± 3.93 | 13.76 ± 4.13 | 5723 | 0.07 |
| Clinical history prior to COVID-19 | ||||
| Comorbidities prior to COVID-19, mean ± SD | 2.69 ± 2.40 | 2.36 ± 2.30 | 6292 | 0.21 |
| Psychiatric treatments prior to COVID-19, mean ± SD | 0.07 ± 0.30 | 0.10 ± 0.37 | 6793 | 0.49 |
| Pneumological comorbidities, n (%) | 31 (19.6) | 8 (9.1) | 4.70 | 0.03 |
| Antibiotics prior to admission | 89 (56.3) | 52 (59.1) | 0.18 | 0.67 |
| Cortisone prior to admission | 67 (42.4) | 26 (29.5) | 3.97 | 0.05 |
| Drug treatments prior to admission (n), mean ± SD | 1.27 ± 1.64 | 1.13 ± 1.67 | 6206 | 0.15 |
| COVID-19 | ||||
| Psychiatric symptoms/delirium during hospitalization, n (%) | 8 (5.1) | 11 (12.5) | 6435 | 0.04 |
| Psychiatric treatments during hospitalization (n), mean ± SD | 0.17 ± 2.33 | 0.18 ± 1.97 | 6880 | 0.82 |
| Number of total symptoms during COVID-19, mean ± SD | 7.59 ± 3.96 | 6.76 ± 3.44 | 6086 | 0.11 |
| Fever, n (%) | 142 (89.9) | 81 (92.0) | 0.31 | 0.57 |
| Cough, n (%) | 97 (61.4) | 56 (63.6) | 0.12 | 0.73 |
| Asthenia/fatigue/weakness, n (%) | 133 (84.7) | 62 (70.5) | 7.06 | <0.01 |
| Diarrhea, n (%) | 40 (25.3) | 16 (18.2) | 1.64 | 0.20 |
| Headache, n (%) | 81 (51.3) | 30 (34.1) | 6.73 | 0.01 |
| Anosmia/Dysosmia, n (%) | 62 (39.2) | 39 (44.3) | 0.60 | 0.44 |
| Dysgeusia, n (%) | 65 (41.1) | 40 (45.5) | 0.43 | 0.51 |
| Red eyes, n (%) | 27 (17.1) | 14 (15.9) | 0.06 | 0.81 |
| Reduction in eyesight, n (%) | 25 (15.8) | 12 (13.6) | 0.21 | 0.65 |
| Reduction in eyesight, n (%) | 15 (9.5) | 7 (8.0) | 0.16 | 0.68 |
| Syncope, n (%) | 46 (29.1) | 15 (17.0) | 4.41 | 0.04 |
| Vertigo, n (%) | 95 (60.1) | 42 (47.7) | 3.52 | 0.06 |
| Arthralgia, n (%) | 25 (15.8) | 4 (4.5) | 6.91 | 0.01 |
| Cutaneous and mucosal lesions, n (%) | 38 (24.1) | 14 (15.9) | 2.25 | 0.13 |
| Sicca Syndrome, n (%) | 2 (1.3) | 0 (0.0) | 1.12 | 0.29 |
| Raynaud’s phenomenon, n (%) | 95 (60.1) | 39 (44.3) | 5.69 | 0.02 |
| Myalgia, n (%) | 56 (35.4) | 25 (28.4) | 1.27 | 0.26 |
| Sore throat, n (%) | 35 (22.2) | 21 (23.9) | 0.09 | 0.76 |
| Sputum, n (%) | 32 (20.3) | 17 (19.3) | 0.03 | 0.86 |
| Rhinitis, n (%) | 20 (12.7) | 14 (15.9) | 0.50 | 0.48 |
| Loss of appetite, n (%) | 69 (43.9) | 47 (53.4) | 2.02 | 0.15 |
| Days of hospitalization, mean ± SD | 22.35 ± 25.10 | 26.47 ± 19.83 | 1.76 | 0.19 |
| Oxygen therapy, n (%) | 141 (89.2) | 69 (78.4) | 5.31 | 0.02 |
| Drugs during hospitalization (n), mean ± SD | 2.44 ± 2.54 | 2.06 ± 2.39 | 1.32 | 0.25 |
| Intensive Care Unit admission, n (%) | 113 (71.5) | 57 (60.8) | 1.20 | 0.27 |
| Ctrl | Anti-IL-6-R | U or χ2 | p | |
|---|---|---|---|---|
| Number of total post-COVID-19 symptoms, mean ± SD | 3.88 ± 2.78 | 3.23 ± 2.63 | 5714 | 0.02 |
| Asthenia/fatigue Post-COVID, n (%) | 102 (64.6) | 50 (56.8) | 1.43 | 0.23 |
| Cough Post-COVID, n (%) | 28 (17.7) | 6 (6.8) | 5.64 | 0.02 |
| Diarrhea Post-COVID, n (%) | 7 (4.4) | 0 (0) | 4.01 | 0.04 |
| Headache Post-COVID, n (%) | 35 (22.2) | 9 (10.2) | 5.47 | 0.02 |
| Anosmia/dysosmia Post-COVID, n (%) | 17 (10.8) | 9 (10.2) | 0.02 | 0.90 |
| Dysgeusia Post-COVID, n (%) | 22 (13.9) | 7 (8.0) | 1.94 | 0.16 |
| Red eyes Post-COVID, n (%) | 8 (5.1) | 5 (5.7) | 0.04 | 0.83 |
| Reduction in eyesight Post-COVID, n (%) | 26 (16.5) | 16 (18.2) | 0.12 | 0.73 |
| Syncope Post-COVID, n (%) | 0 (0) | 0 (0) | – | – |
| Vertigo Post-COVID, n (%) | 22 (13.9) | 7 (8.0) | 1.94 | 0.16 |
| Arthralgia and arthritis Post-COVID, n (%) | 62 (39.2) | 31 (35.2) | 0.39 | 0.53 |
| Cutaneous and mucosal lesions Post-COVID, n (%) | 12 (7.6) | 7 (8.0) | 0.01 | 0.92 |
| Sicca Syndrome Post-COVID, n (%) | 19 (12.0) | 9 (10.2) | 0.18 | 0.67 |
| Raynaud’s phenomenon Post-COVID, n (%) | 1 (0.6) | 0 (0) | 0.56 | 0.45 |
| Myalgia Post-COVID, n (%) | 63 (39.9) | 30 (34.1) | 0.80 | 0.37 |
| Exertional dyspnea Post-COVID, n (%) | 127 (80.4) | 57 (64.8) | 7.30 | 0.01 |
| Chest pain Post-COVID, n (%) | 28 (17.7) | 16 (18.2) | 0.01 | 0.93 |
| Sore throat Post-COVID, n (%) | 4 (2.5) | 5 (5.7) | 1.59 | 0.21 |
| Sputum Post-COVID, n (%) | 12 (7.6) | 7 (8.0) | 0.01 | 0.92 |
| Rhinitis Post-COVID, n (%) | 8 (5.1) | 8 (9.1) | 1.51 | 0.22 |
| Loss of appetite Post-COVID, n (%) | 10 (6.3) | 5 (5.7) | 0.04 | 0.84 |
| Days from COVID onset, mean ± SD | 173.38 ± 96.78 | 155.42 ± 88.23 | 2.07 | 0.15 |
| SpO2, mean± SD | 96.83 ± 5.46 | 96.67 ± 3.69 | 5902 | 0.41 |
| HAM-D, mean ± SD | 3,74 ± 4.25 | 3.89 ± 4.48 | 6764 | 0.72 |
| HAM-A, mean ± SD | 4.78 ± 4.96 | 4.86 ± 6.52 | 6409 | 0.31 |
| YMRS, mean ± SD | 0.89 ± 1.44 | 0.89 ± 1,43 | 6810 | 0.77 |
| KMRSD, mean ± SD | 6.49 ± 2.32 | 6.65 ± 2.38 | 6949 | 0.99 |
| BPRS, mean ± SD | 26.51 ± 4.70 | 26.59 ± 3.46 | 6631 | 0.53 |
| CAPS Total; mean ± SD | 6.18 ± 9.72 | 7.74 ± 10.89 | 6525 | 0.41 |
| CD-RISC Total; mean ± SD | 67.88 ± 13.38 | 70.38 ± 12.57 | 6032 | 0.09 |
| DERS Total; mean ± SD | 83.08 ± 15.06 | 78.32 ± 15.56 | 5471 | <0.01 |
| SHAPS Total, mean ± SD | 0.82 ± 2.25 | .53 ± 2.02 | 6339 | 0.12 |
| PSQI Total; mean ± SD | 6.24 ± 5.33 | 5.76 ± 4.94 | 6659 | 0.58 |
| BHS Total; mean ± SD | 7.99 ± 4.90 | 7.41 ± 4.89 | 6193 | 0.15 |
| Ctrl | TOC | SAR | χ2 | p | Post hoc | ||||
|---|---|---|---|---|---|---|---|---|---|
| Ctrl vs. TOC | Ctrl vs. SAR | TOC vs. SAR | |||||||
| Sociodemographic and clinical characteristics | |||||||||
| Age (y), mean ± SD | 56.66 ± 10.30 | 56.00 ± 13.03 | 59.76 ± 8.21 | 1.34 | 0.51 | 0.91 | 0.25 | 0.32 | |
| BMI, mean ± SD | 28.00 ± 4.57 | 28.19 ± 4.91 | 28.35 ± 3.83 | 0.48 | 0.79 | 0.86 | 0.49 | 0.59 | |
| Female, n (%) | 58 (36.7) | 24 (35.8) | 2 (9.5) | 6.21 | 0.04 | 0.90 | 0.01 | 0.02 | |
| Marital Status (%) | |||||||||
| Never married | 18 (11.5) | 12 (17.9) | 3 (14.3) | 6.08 | 0.64 | 0.19 | 0.7 | 0.7 | |
| Married | 101 (63.9) | 45 (67.2) | 16 (76.2) | 0.64 | 0.27 | 0.44 | |||
| Partner | 7 (4.4) | 2 (3) | 0 (0) | 0.61 | 0.33 | 0.42 | |||
| Divorced | 7 (4.4) | 2 (3) | 0 (0) | 0.61 | 0.33 | 0.42 | |||
| Widowed | 25 (15.8) | 6 (9) | 2 (9.5) | 0.17 | 0.45 | 0.94 | |||
| Occupation (%) | |||||||||
| Unemployed | 9 (5.7) | 6 (9) | 1 (4.8) | 3.01 | 0.81 | 0.37 | 0.86 | 0.54 | |
| Employed | 117 (74.1) | 48 (71.6) | 14 (66.7) | 0.71 | 0.47 | 0.66 | |||
| Retired | 32 (20.3) | 13 (19.4) | 6 (28.8) | 0.88 | 0.38 | 0.37 | |||
| Education (y), mean ± SD | 12.80 ± 3.93 | 13.58 ± 4.14 | 14.35 ± 4.16 | 1.86 | 0.16 | 0.21 | 0.07 | .31 | |
| Comorbidities, mean ± SD | 2.69 ± 2.40 | 2.43 ± 2.46 | 2.14 ± 1.74 | 1.59 | 0.45 | 0.28 | 0.39 | 0.96 | |
| Psychiatric treatments prior to COVID, mean ± SD | 0.07 ± 0.30 | 0.09 ± 0.38 | 0.14 ± 0.36 | 2.15 | 0.34 | 0.91 | 0.15 | 0.25 | |
| Pneumological comorbidities, n (%) | 31(19.6) | 7(10.4) | 1 (4.8) | 5.08 | 0.08 | 0.09 | 0.09 | 0.43 | |
| COVID-19 | |||||||||
| Antibiotics prior to admission, n (%) | 89 (56.3) | 43 (64.2) | 9 (42.9) | 3.15 | 0.21 | 0.27 | 0.24 | 0.08 | |
| Cortisone prior to admission, n (%) | 67 (42.4) | 23 (34.3) | 3 (14.3) | 6.71 | 0.03 | 0.26 | 0.01 | 0.08 | |
| Drug treatments prior to admission (n), mean ± SD | 1.27 ± 1.64 | 0.99 ± 1.49 | 1.57 ± 2.13 | 2.58 | 0.28 | 0.31 | 0.17 | 0.41 | |
| Hospitalization (d), mean ± SD | 22.35 ± 25.1 | 24.75 ± 19.38 | 31.95 ± 20.74 | 1.64 | 0.20 | 0.76 | 0.18 | 0.43 | |
| Psychiatric symptoms/delirium during hospitalization, n (%) | 8 (5.1) | 8 (11.9) | 3 (14.3) | 4.49 | 0.11 | 0.07 | 0.10 | 0.78 | |
| Psychiatric treatments during hospitalization (n), mean ± SD | 0.16 ±0.46 | 0.21 ± 0.54 | 0.10 ± 0.30 | 0.55 | 0.76 | 0.62 | 0.65 | 0.49 | |
| Oxygen therapy, n (%) | 141 (89.2) | 55 (82.1) | 14 (66.7) | 8.35 | 0.01 | 0.14 | <0.01 | 0.13 | |
| Drugs during hospitalization(n), mean± SD | 2.46 ± 2.56 | 2.18 ± 2.5 | 1.67 ± 2.03 | 1.05 | 0.35 | 0.45 | 0.18 | 0.42 | |
| Intensive Care Unit admission, n (%) | 113 (71.5) | 46 (68.7) | 11 (52.4) | 3.19 | 0.2 | 0.67 | 0.07 | 0.17 | |
| Symptoms during COVID, mean ± SD | 7.59 ± 3.96 | 6.81 ± 3.63 | 6.62 ± 2.82 | 2.63 | 0.29 | 0.15 | 0.31 | 0.83 | |
| Fever, n (%) | 142 (89.9) | 60 (89.6) | 21 (100.0) | 2.37 | 0.30 | 0.94 | 0.13 | 0.12 | |
| Fatigue/Asthenia, n (%) | 133 (84.7) | 46 (68.7) | 16 (76.2) | 7.61 | 0.02 | <0.01 | 0.36 | 0.51 | |
| Cough, n (%) | 97 (61.4) | 41 (61.2) | 15 (71.4) | 0.83 | 0.66 | 0.97 | 0.37 | 0.39 | |
| Diarrhea, n (%) | 40 (25.3) | 13 (19.4) | 3 (14.3) | 1.87 | 0.39 | 0.34 | 0.27 | 0.60 | |
| Headache, n (%) | 81 (51.3) | 26 (38.8) | 4 (19.0) | 9.25 | 0.01 | 0.09 | <0.01 | 0.97 | |
| Anosmia/Dysosmia, n (%) | 62 (39.2) | 32 (47.8) | 7 (33.3) | 1.98 | 0.37 | 0.23 | 0.60 | 0.25 | |
| Dysgeusia, n (%) | 65 (41.1) | 31 (46.3) | 9 (42.9) | 0.51 | 0.78 | 0.48 | 0.88 | 0.79 | |
| Red eyes, n (%), | 27 (17.1) | 10 (14.9) | 4 (19.0) | 0.25 | 0.88 | 0.69 | 0.83 | 0.65 | |
| Reduction in eyesight, n (%) | 25 (15.8) | 9 (13.4) | 3 (14.3) | 0.22 | 0.90 | 0.65 | 0.86 | 0.92 | |
| Syncope, n (%), | 15 (9.5) | 5 (7.5) | 2 (9.5) | 0.25 | 0.88 | 0.62 | 1 | 0.76 | |
| Vertigo, n (%) | 46 (29.1) | 12 (17.9) | 3 (14.3) | 4.53 | 0.10 | 0.08 | 0.15 | 0.69 | |
| Arthralgia, n (%) | 95 (60.1) | 33 (49.3) | 9 (42.9) | 3.79 | 0.15 | 0.13 | 0.13 | 0.61 | |
| Cutaneous and mucosal lesions, n (%) | 25 (15.8) | 4 (6.0) | 0 (0.0) | 7.46 | 0.02 | 0.04 | 0.04 | 0.25 | |
| Sicca Syndrome, n (%) | 38 (24.1) | 11 (16.4) | 3 (14.3) | 2.29 | 0.32 | 0.20 | 0.32 | 0.82 | |
| Loss of appetite, n (%) | 69 (43.9) | 35 (52.2) | 12 (57.1) | 2.18 | 0.34 | 0.24 | 0.24 | 0.70 | |
| Raynaud’s phenomenon, n (%) | 2 (1.3) | 0 (0.0) | 0 (0.0) | 1.12 | 0.57 | 0.35 | 0.60 | 0.9999 | |
| Myalgia, n (%) | 95 (60.1) | 29 (43.3) | 10 (47.6) | 5.82 | 0.06 | 0.02 | 0.28 | 0.73 | |
| Chest Pain, n (%) | 56 (35.4) | 19 (28.4) | 6 (28.6) | 1.27 | 0.53 | 0.30 | 0.54 | 0.98 | |
| Sore throat, n (%) | 35 (22.2) | 16 (23.9) | 5 (23.8) | 0.09 | 0.95 | 0.78 | 0.87 | 0.99 | |
| Sputum, n (%) | 32 (20.3) | 13 (19.4) | 4 (19.0) | 0.03 | 0.98 | 0.88 | 0.90 | 0.97 | |
| Rhinitis, n (%) | 20 (12.7) | 11 (16.4) | 3 (14.3) | 0.56 | 0.75 | 0.45 | 0.83 | 0.82 | |
| Ctrl (N = 158) | TOC (N = 67) | SAR (N = 21) | χ2 | p | Post hoc | |||
|---|---|---|---|---|---|---|---|---|
| Ctrl vs. TOC | Ctrl vs. SAR | TOC vs. SAR | ||||||
| Post-COVID symptoms, mean ± SD | 3.88 ± 2.78 | 3.24 ± 2.59 | 3.19 ± 2.80 | 6.27 | 0.04 | 0.08 | 0.04 | 0.38 |
| Post-COVID Fatigue/Asthenia, n (%) | 102 (64.6) | 37 (55.2) | 13 (61.9) | 1.74 | 0.42 | 0.19 | 0.81 | 0.59 |
| Post-COVID Cough, n (%) | 28 (17.7) | 4 (6.0) | 2 (9.5) | 5.81 | 0.06 | 0.02 | 0.35 | 0.58 |
| Post-COVID Diarrhea, n (%) | 7 (4.4) | 0 (0.0) | 0 (0.0) | 4.01 | 0.13 | 0.08 | 0.33 | 0.999 |
| Post-COVID Headache, n (%) | 35 (22.2) | 7 (10.4) | 2 (9.5) | 5.48 | 0.06 | 0.04 | 0.18 | 0.90 |
| Post-COVID Anosmia/dysosmia, n (%) | 17 (10.8) | 8 (11.9) | 1 (4.8) | 0.89 | 0.64 | 0.79 | 0.39 | 0.34 |
| Post-COVID Dysgeusia, n (%) | 22 (13.9) | 6 (9.0) | 1 (4.8) | 2.20 | 0.33 | 0.30 | 0.24 | 0.53 |
| Post-COVID Red Eyes, n (%) | 8 (5.1) | 5 (7.5) | 0 (0.0) | 1.82 | 0.40 | 0.38 | 0.20 | 0.20 |
| Post-COVID Reduction in eyesight, n (%) | 26 (16.5) | 10 (14.9) | 6 (28.6) | 2.22 | 0.33 | 0.77 | 0.17 | 0.16 |
| Post-COVID Syncope, n (%) | 0 (0.0) | 0 (0.0) | 0 (0.0) | – | – | – | – | – |
| Post-COVID Vertigo, n (%) | 22 (13.9) | 5 (7.5) | 2 (9.5) | 2.0 | 0.37 | 0.17 | 0.58 | 0.76 |
| Post-COVID Arthralgia, n (%) | 62 (39.2) | 23 (34.3) | 8 (38.1) | 0.48 | 0.78 | 0.49 | 0.92 | 0.75 |
| Post-COVID Cutaneous and mucosal lesions, n (%) | 12 (7.6) | 6 (9.0) | 1 (4.8) | 0.40 | 0.82 | 0.73 | 0.64 | 0.54 |
| Post-COVID Sicca Syndrome, n (%) | 19 (12.0) | 7 (10.4) | 2 (9.5) | 0.19 | 0.91 | 0.73 | 0.74 | 0.90 |
| Post-COVID Raynaud’s phenomenon, n (%) | 1 (0.6) | 0 (0.0) | 0 (0.0) | 0.56 | 0.76 | 0.52 | 0.71 | 0.999 |
| Post-COVID Myalgia, n (%) | 63 (39.9) | 22 (32.8) | 8 (38.1) | 0.99 | 0.61 | 0.32 | 0.87 | 0.66 |
| Post-COVID Dyspnea on exertion, n (%) | 127 (80.4) | 46 (68.7) | 11 (52.4) | 9.55 | 0.01 | 0.06 | <0.01 | 0.17 |
| Post-COVID Chest Pain, n (%) | 28 (17.7) | 12 (17.9) | 4 (19.0) | 0.02 | 0.99 | 0.97 | 0.88 | 0.90 |
| Post-COVID Sore Throat, n (%) | 4 (2.5) | 5 (7.5) | 0 (0.0) | 4.12 | 0.13 | 0.08 | 0.46 | 0.20 |
| Post-COVID Sputum, n (%) | 12 (7.6) | 5 (7.5) | 2 (9.5) | 0.11 | 0.95 | 0.98 | 0.76 | 0.76 |
| Post-COVID Rhinitis, n (%) | 8 (5.1) | 6 (9.0) | 2 (9.5) | 1.52 | 0.47 | 0.27 | 0.40 | 0.94 |
| Post-COVID Loss of Appetite, n (%) | 10 (6.3) | 3 (4.5) | 2 (9.5) | 0.75 | 0.69 | 0.59 | 0.58 | 0.38 |
| Days from COVID Symptoms Onset, n (%) | 173.38 ± 96.78 | 152.96 ± 90.13 | 163.29 ± 83.48 | 1.13 | 0.32 | 0.30 | 0.89 | 0.90 |
| SpO2, mean ± SD | 96.83 ± 5.46 | 96.68 ± 4.22 | 96.62 ± 1.12 | 0.74 | 0.69 | 0.41 | 0.49 | 0.86 |
| BPRS Total, mean ± SD | 26.51 ± 4.70 | 26.49 ± 3.62 | 26.90 ± 2.95 | 1.74 | 0.42 | 0.29 | 0.55 | 0.25 |
| HAM-A Total, mean ± SD | 4.78 ± 4.96 | 4.82 ± 6.13 | 5.00 ± 7.82 | 1.15 | 0.56 | 0.42 | 0.39 | 0.76 |
| HAM-D Total, mean ± SD | 3.74 ± 4.25 | 4.03 ± 4.4 | 3.43 ± 4.83 | 0.57 | 0.75 | 0.56 | 0.75 | 0.47 |
| MRS Total, mean ± SD | 0.89 ± 1.44 | 0.85 ± 1.39 | 1.00 ± 1.58 | 0.09 | 0.96 | 0.80 | 0.84 | 0.94 |
| KMRSD Total, mean ± SD | 6.49 ± 2.32 | 6.72 ± 2.19 | 6.43 ± 2.96 | 1.64 | 0.44 | 0.59 | 0.28 | 0.23 |
| CAPS Total, mean ± SD | 6.18 ± 9.72 | 7.46 ± 10.57 | 8.62 ± 12.09 | 1.04 | 0.60 | 0.61 | 0.34 | 0.54 |
| CD-RISC Total, mean ± SD | 67.88 ± 13.38 | 69.94 ± 12.64 | 71.76 ± 12.54 | 3.04 | 0.22 | 0.15 | 0.65 | 0.23 |
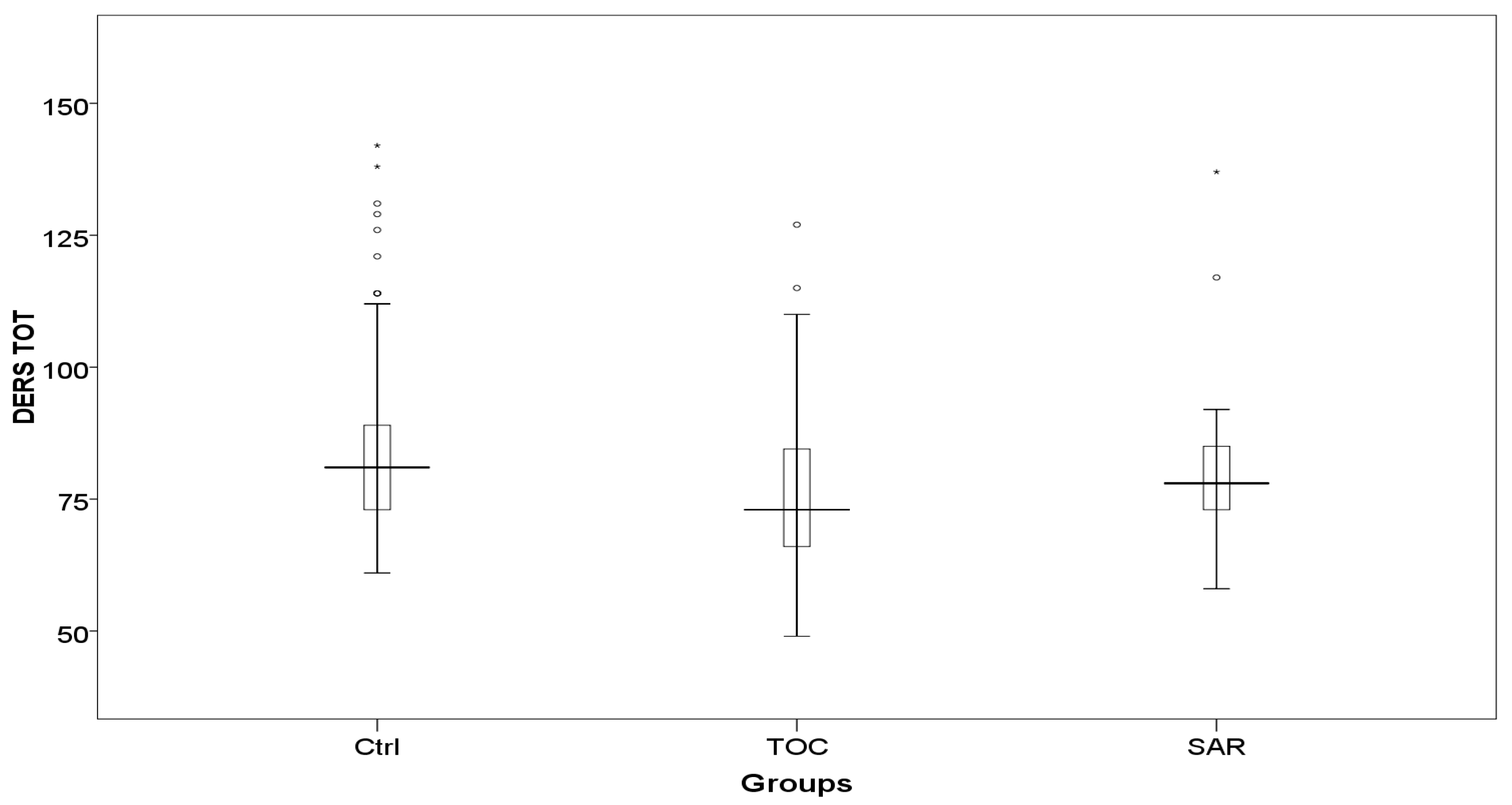
| DERS Total, mean ± SD | 83.08 ± 15.06 | 77.06 ± 14.92 | 82.33 ± 17.21 | 9.58 | <0.01 | <0.01 | 0.62 | 0.14 |
| SHAPS Total, mean ± SD | 0.82 ± 2.25 | 0.58 ± 2.26 | 0.38 ± 0.97 | 2.39 | 0.30 | 0.15 | 0.44 | 0.89 |
| PSQI Total, mean ± SD | 6.24 ± 5.33 | 5.79 ± 5.21 | 5.67 ± 4.07 | 0.34 | 0.84 | 0.57 | 0.86 | 0.81 |
| BHS Total, mean ± SD | 8.16 ± 4.78 | 7.00 ± 5.06 | 8.71 ± 4.14 | 4.38 | 0.11 | 0.05 | 0.68 | 0.12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simonetti, A.; Restaino, A.; Bernardi, E.; Ferrara, O.M.; Margoni, S.; D’Onofrio, A.M.; Ranieri, F.; Janiri, D.; Galluzzo, V.; Tosato, M.; et al. Effect of Anti-Interleukin-6 Agents on Psychopathology in a Sample of Patients with Post-COVID-19 Syndrome: An Observational Study. Brain Sci. 2024, 14, 47. https://doi.org/10.3390/brainsci14010047
Simonetti A, Restaino A, Bernardi E, Ferrara OM, Margoni S, D’Onofrio AM, Ranieri F, Janiri D, Galluzzo V, Tosato M, et al. Effect of Anti-Interleukin-6 Agents on Psychopathology in a Sample of Patients with Post-COVID-19 Syndrome: An Observational Study. Brain Sciences. 2024; 14(1):47. https://doi.org/10.3390/brainsci14010047
Chicago/Turabian StyleSimonetti, Alessio, Antonio Restaino, Evelina Bernardi, Ottavia Marianna Ferrara, Stella Margoni, Antonio Maria D’Onofrio, Federica Ranieri, Delfina Janiri, Vincenzo Galluzzo, Matteo Tosato, and et al. 2024. "Effect of Anti-Interleukin-6 Agents on Psychopathology in a Sample of Patients with Post-COVID-19 Syndrome: An Observational Study" Brain Sciences 14, no. 1: 47. https://doi.org/10.3390/brainsci14010047