
Photosensitizers for Photodynamic Therapy of Brain Cancers—A Review



Abstract
:1. Introduction
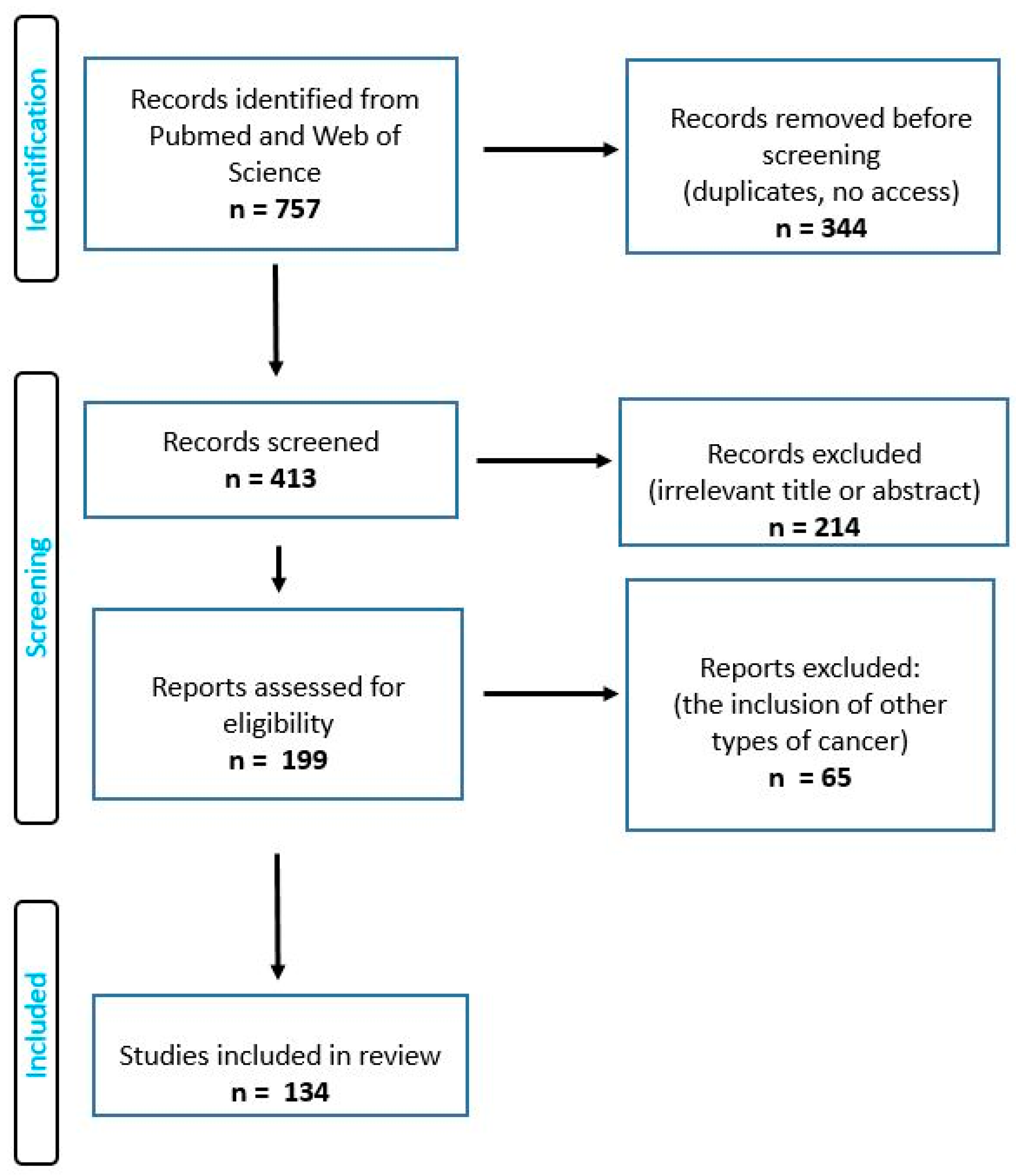
2. Materials and Methods
3. A Review of the Literature
3.1. Application of Photodynamic Therapy
3.2. Photosensitizer
3.2.1. 5-Aminolevulinic Acid
3.2.2. Temoporfin—THPC
3.2.3. Photofrin
3.2.4. Hypericin
3.2.5. Talaporfin
3.2.6. Other Photosensitizers
3.3. Third Generation Photosensitizers
3.4. Limitations of Photosensitizers
3.5. Optical Characteristics of Photosensitizers
3.6. Irradiation Conditions
3.7. Light-Delivery Systems
4. Limitations of this Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fan, Y.; Zhang, X.; Gao, C.; Jiang, S.; Wu, H.; Liu, Z.; Dou, T. Burden and trends of brain and central nervous system cancer from 1990 to 2019 at the global, regional, and country levels. Arch. Public Health 2022, 80, 209. [Google Scholar] [CrossRef] [PubMed]
- Ibarra, L.E.; Vilchez, M.L.; Caverzán, M.D.; Milla Sanabria, L.N. Understanding the glioblastoma tumor biology to optimize photodynamic therapy: From molecular to cellular events. J. Neurosci. Res. 2021, 99, 1024–1047. [Google Scholar] [CrossRef]
- Ostrom, Q.T.; Gittleman, H.; Farah, P.; Ondracek, A.; Chen, Y.; Wolinsky, Y.; Stroup, N.E.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS statistical report: Primary brain and central nervous system tumors diagnosed in the United States in 2006-2010. Neuro Oncol. 2013, 5, 2. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [PubMed]
- Ostrom, Q.T.; Bauchet, L.; Davis, F.G.; Deltour, I.; Fisher, J.L.; Langer, C.E.; Pekmezci, M.; Schwartzbaum, J.A.; Turner, M.C.; Walsh, K.M.; et al. The epidemiology of glioma in adults: A “state of the science” review. Neuro-Oncology 2014, 16, 896–913. [Google Scholar] [CrossRef]
- Claes, A.; Idema, A.J.; Wesseling, P. Diffuse glioma growth: A guerilla war. Acta Neuropathol. 2007, 114, 443–458. [Google Scholar] [CrossRef]
- Madsen, S.J.; Sun, C.-H.; Tromberg, B.J.; Cristini, V.; De Magalhães, N.; Hirschberg, H. Multicell tumor spheroids in photodynamic therapy. Lasers in Surg. Med. 2006, 38, 555–564. [Google Scholar] [CrossRef]
- Jeising, S.; Geerling, G.; Guthoff, R.; Hänggi, D.; Sabel, M.; Rapp, M.; Nickel, A.-C. In-Vitro Use of Verteporfin for Photodynamic Therapy in Glioblastoma. Photodiagn. Photodyn. Ther. 2022, 40, 103049. [Google Scholar] [CrossRef]
- Zavadskaya, T.S. Photodynamic therapy in the treatment of glioma. Exp. Oncol. 2015, 37, 234–241. [Google Scholar] [CrossRef]
- Kolarikova, M.; Hosikova, B.; Dilenko, H.; Barton-Tomankova, K.; Valkova, L.; Bajgar, R.; Malina, L.; Kolarova, H. Photodynamic therapy: Innovative approaches for antibacterial and anticancer treatments. Med. Res. Rev. 2023, 43, 717–774. [Google Scholar] [CrossRef]
- Quach, S.; Schwartz, C.; Aumiller, M.; Foglar, M.; Schmutzer, M.; Katzendobler, S.; El Fahim, M.; Forbrig, R.; Bochmann, K.; Egensperger, R.; et al. Interstitial photodynamic therapy for newly diagnosed glioblastoma. J. Neurooncol. 2023, 162, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Chiba, K.; Aihara, Y.; Oda, Y.; Fukui, A.; Tsuzuk, S.; Saito, T.; Nitta, M.; Muragaki, Y.; Kawamata, T. Photodynamic therapy for malignant brain tumors in children and young adolescents. Front. Oncol. 2022, 12, 957267. [Google Scholar] [CrossRef] [PubMed]
- Aldosari, L.I.N.; Hassan, S.A.B.; Alshadidi, A.A.F.; Rangaiah, G.C.; Divakar, D.D. Short-term influence of antimicrobial photodynamic therapy as an adjuvant to mechanical debridement in reducing soft-tissue inflammation and subgingival yeasts colonization in patients with peri-implant mucositis. Photodiagn. Photodyn. Ther. 2023, 42, 103320. [Google Scholar] [CrossRef]
- de Paiva, A.C.M.; Ferreira, M.D.C.; da Fonseca, A.S. Photodynamic therapy for treatment of bacterial keratitis. Photodiagn. Photodyn. Ther. 2022, 37, 102717. [Google Scholar] [CrossRef]
- Gil-Pallares, P.; Navarro-Bielsa, A.; Almenara-Blasco, M.; Gracia-Cazaña, T.; Gilaberte, Y. Photodynamic Therapy, a successful treatment for granular parakeratosis. Photodiagn. Photodyn. Ther. 2023, 42, 103562. [Google Scholar] [CrossRef]
- Alexiades-Armenakas, M. Laser-mediated photodynamic therapy. Clin. Dermatol. 2006, 24, 16–25. [Google Scholar] [CrossRef]
- Kessel, D. Photodynamic Therapy: Critical PDT Theory. Photochem. Photobiol. 2023, 99, 199–203. [Google Scholar] [CrossRef]
- Maharjan, P.S.; Bhattarai, H.K. Singlet Oxygen, Photodynamic Therapy, and Mechanisms of Cancer Cell Death. J. Oncol. 2022, 2022, 7211485. [Google Scholar] [CrossRef]
- Sabino, C.P.; Ribeiro, M.S.; Wainwright, M.; Dos Anjos, C.; Sellera, F.P.; Dropa, M.; Nunes, N.B.; Brancini, G.T.P.; Braga, G.U.L.; Arana-Chavez, V.E.; et al. The Biochemical Mechanisms of Antimicrobial Photodynamic Therapy †. Photochem. Photobiol. 2023, 99, 742–750. [Google Scholar] [CrossRef]
- Lima, E.; Reis, L.V. Photodynamic Therapy: From the Basics to the Current Progress of N-Heterocyclic-Bearing Dyes as Effective Photosensitizers. Molecules 2023, 28, 5092. [Google Scholar] [CrossRef]
- Collin, F. Chemical Basis of Reactive Oxygen Species Reactivity and Involvement in Neurodegenerative Diseases. Int. J. Mol. Sci. 2019, 20, 2407. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Song, J.; Nie, L.; Chen, X. Reactive oxygen species generating systems meeting challenges of photodynamic cancer therapy. Chem. Soc. Rev. 2016, 45, 6597–6626. [Google Scholar] [CrossRef] [PubMed]
- Fujii, J.; Soma, Y.; Matsuda, Y. Biological Action of Singlet Molecular Oxygen from the Standpoint of Cell Signaling, Injury and Death. Molecules 2023, 28, 4085. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Bartusik-Aebisher, D.; Żołyniak, A.; Barnaś, E.; Machorowska-Pieniążek, A.; Oleś, P.; Kawczyk-Krupka, A.; Aebisher, D. The Use of Photodynamic Therapy in the Treatment of Brain Tumors-A Review of the Literature. Molecules 2022, 27, 6847. [Google Scholar] [CrossRef]
- Correia, J.H.; Rodrigues, J.A.; Pimenta, S.; Dong, T.; Yang, Z. Photodynamic Therapy Review: Principles, Photosensitizers, Applications, and Future Directions. Pharmaceutics 2021, 13, 1332. [Google Scholar] [CrossRef] [PubMed]
- Mishchenko, T.; Balalaeva, I.; Gorokhova, A.; Vedunova, M.; Krysko, D.V. Which cell death modality wins the contest for photodynamic therapy of cancer? Cell Death Dis. 2022, 13, 455. [Google Scholar] [CrossRef]
- Bacellar, I.O.L.; Baptista, M.S. Mechanisms of Photosensitized Lipid Oxidation and Membrane Permeabilization. ACS Omega 2019, 4, 21636–21646. [Google Scholar] [CrossRef]
- Ray, P.D.; Huang, B.W.; Tsuji, Y. Reactive oxygen species (ROS) homeostasis and redox regulation in cellular signaling. Cell Signal. 2012, 24, 981–990. [Google Scholar] [CrossRef]
- Murotomi, K.; Umeno, A.; Shichiri, M.; Tanito, M.; Yoshida, Y. Significance of Singlet Oxygen Molecule in Pathologies. Int. J. Mol. Sci. 2023, 24, 2739. [Google Scholar] [CrossRef]
- Gunaydin, G.; Gedik, M.E.; Ayan, S. Photodynamic Therapy-Current Limitations and Novel Approaches. Front. Chem. 2021, 9, 691697. [Google Scholar] [CrossRef]
- Dynarowicz, K. Naturally occurring photosensitizers and photodynamic therapy: Laser or sun? Eur. J. Clin. Exp. Med. 2021, 19, 174–178. [Google Scholar] [CrossRef]
- Queirós, C.; Garrido, P.M.; Maia Silva, J.; Filipe, P. Photodynamic therapy in dermatology: Beyond current indications. Dermatol. Ther. 2020, 33, e13997. [Google Scholar] [CrossRef] [PubMed]
- Mazur, A.; Koziorowska, K.; Dynarowicz, K.; Aebisher, D.; Bartusik-Aebisher, D. Vitamin D and Vitamin D3 Supplementation during Photodynamic Therapy: A Review. Nutrients 2022, 14, 3805. [Google Scholar] [CrossRef]
- Pariser, D.M.; Lowe, N.J.; Stewart, D.M.; Jarratt, M.T.; Lucky, A.W.; Pariser, R.J.; Yamauchi, P.S. Photodynamic therapy with topical methyl aminolevulinate for actinic keratosis: Results of a prospective randomized multicenter trial. J. Am. Acad. Dermatol. 2003, 48, 227–232. [Google Scholar] [CrossRef]
- Rynda, A.Y.; Olyushin, V.E.; Rostovtsev, D.M.; Zabrodskaya, Y.M.; Ulitin, A.Y.; Papayan, G.V. Intraoperative photodynamic therapy in complex treatment of malignant gliomas. Zh. Vopr. Neirokhir. Im. N. N. Burdenko 2023, 87, 25–34. (In Russian) [Google Scholar] [CrossRef]
- Mahmoudi, K.; Garvey, K.L.; Bouras, A.; Cramer, G.; Stepp, H.; Jesu Raj, J.G.; Bozec, D.; Busch, T.M.; Hadjipanayis, C.G. 5-aminolevulinic acid photodynamic therapy for the treatment of high-grade gliomas. J. Neurooncol. 2019, 141, 595–607. [Google Scholar] [CrossRef] [PubMed]
- Casas, A. Clinical uses of 5-aminolaevulinic acid in photodynamic treatment and photodetection of cancer: A review. Cancer Lett. 2020, 490, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Feng, H.; Li, F. Progression of basic research, clinical application of photodynamic therapy and fluorescence-guided surgery in glioma treatment. Zhong Nan Da Xue Xue Bao Yi Xue Ban 2018, 43, 360–367. [Google Scholar] [CrossRef]
- Friesen, S.A.; Hjortland, G.O.; Madsen, S.J.; Hirschberg, H.; Engebraten, O.; Nesland, J.M.; Peng, Q. 5-Aminolevulinic acid-based photodynamic detection and therapy of brain tumors (review). Int. J. Oncol. 2002, 21, 577–582. [Google Scholar] [CrossRef]
- Johansson, A.; Palte, G.; Schnell, O.; Tonn, J.C.; Herms, J.; Stepp, H. 5-Aminolevulinic acid-induced protoporphyrin IX levels in tissue of human malignant brain tumors. Photochem. Photobiol. 2010, 86, 1373–1378. [Google Scholar] [CrossRef] [PubMed]
- Stepp, H.; Stummer, W. 5-ALA in the management of malignant glioma. Lasers Surg. Med. 2018, 50, 399–419. [Google Scholar] [CrossRef] [PubMed]
- Tetard, M.C.; Vermandel, M.; Mordon, S.; Lejeune, J.P.; Reyns, N. Experimental use of photodynamic therapy in high grade gliomas: A review focused on 5-aminolevulinic acid. Photodiagn. Photodyn. Ther. 2014, 11, 319–330. [Google Scholar] [CrossRef] [PubMed]
- Vilchez, M.L.; Rodríguez, L.B.; Palacios, R.E.; Prucca, C.G.; Caverzán, M.D.; Caputto, B.L.; Rivarola, V.A.; Milla Sanabria, L.N. Isolation and initial characterization of human glioblastoma cells resistant to photodynamic therapy. Photodiagn. Photodyn. Ther. 2021, 33, 102097. [Google Scholar] [CrossRef]
- Yi, W.; Xu, H.T.; Tian, D.F.; Wu, L.Q.; Zhang, S.Q.; Wang, L.; Ji, B.W.; Zhu, X.N.; Okechi, H.; Liu, G.; et al. Photodynamic therapy mediated by 5-aminolevulinic acid suppresses gliomas growth by decreasing the microvessels. Journal of Huazhong University of Science and Technology. Medical sciences = Hua zhong ke ji da xue xue bao. Yi xue Ying De wen ban = Huazhong keji daxue xuebao. Yixue Yingdewen Ban 2015, 35, 259–264. [Google Scholar]
- Kamoshima, Y.; Terasaka, S.; Kuroda, S.; Iwasaki, Y. Morphological and histological changes of glioma cells immediately after 5-aminolevulinic acid mediated photodynamic therapy. Neurol. Res. 2011, 33, 739–746. [Google Scholar] [CrossRef]
- Schwake, M.; Nemes, A.; Dondrop, J.; Schroeteler, J.; Schipmann, S.; Senner, V.; Stummer, W.; Ewelt, C. In-Vitro Use of 5-ALA for Photodynamic Therapy in Pediatric Brain Tumors. Neurosurgery 2018, 83, 1328–1337. [Google Scholar] [CrossRef]
- Fontana, L.C.; Pinto, J.G.; Vitorio, G.D.S.; Ferreira, I.; Pacheco-Soares, C.; Mamone, L.A.; Strixino, J.F. Photodynamic effect of protoporphyrin IX in gliosarcoma 9l/lacZ cell line. Photodiagn. Photodyn. Ther. 2022, 37, 102669. [Google Scholar] [CrossRef]
- Inoue, H.; Kajimoto, Y.; Shibata, M.A.; Miyoshi, N.; Ogawa, N.; Miyatake, S.; Otsuki, Y.; Kuroiwa, T. Massive apoptotic cell death of human glioma cells via a mitochondrial pathway following 5-aminolevulinic acid-mediated photodynamic therapy. J. Neuro-Oncol. 2007, 83, 223–231. [Google Scholar] [CrossRef]
- Howley, R.; Chandratre, S.; Chen, B. 5-Aminolevulinic Acid as a Theranostic Agent for Tumor Fluorescence Imaging and Photodynamic Therapy. Bioengineering 2023, 10, 496. [Google Scholar] [CrossRef]
- Hirschberg, H.; Spetalen, S.; Carper, S.; Hole, P.; Tillung, T.; Madsen, S. Minimally invasive photodynamic therapy (PDT) for ablation of experimental rat glioma. Minim. Invasive Neurosurg. 2006, 49, 135–142. [Google Scholar] [CrossRef]
- Coupienne, I.; Bontems, S.; Dewaele, M.; Rubio, N.; Habraken, Y.; Fulda, S.; Agostinis, P.; Piette, J. NF-kappaB inhibition improves the sensitivity of human glioblastoma cells to 5-aminolevulinic acid-based photodynamic therapy. Biochem. Pharmacol. 2011, 81, 606–616. [Google Scholar] [CrossRef]
- Madsen, S.J.; Sun, C.H.; Tromberg, B.J.; Hirschberg, H. Repetitive 5-aminolevulinic acid-mediated photodynamic therapy on human glioma spheroids. J Neurooncol. 2003, 62, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Tetard, M.C.; Vermandel, M.; Leroy, H.A.; Leroux, B.; Maurage, C.A.; Lejeune, J.P.; Mordon, S.; Reyns, N. Interstitial 5-ALA photodynamic therapy and glioblastoma: Preclinical model development and preliminary results. Photodiagn. Photodyn. Ther. 2016, 13, 218–224. [Google Scholar] [CrossRef]
- Fujishiro, T.; Nonoguchi, N.; Pavliukov, M.; Ohmura, N.; Kawabata, S.; Park, Y.; Kajimoto, Y.; Ishikawa, T.; Nakano, I.; Kuroiwa, T. 5-Aminolevulinic acid-mediated photodynamic therapy can target human glioma stem-like cells refractory to antineoplastic agents. Photodiagn. Photodyn. Ther. 2018, 24, 58–68. [Google Scholar] [CrossRef]
- Fettweis, G.; Di Valentin, E.; L′homme, L.; Lassence, C.; Dequiedt, F.; Fillet, M.; Coupienne, I.; Piette, J. RIP3 antagonizes a TSC2-mediated pro-survival pathway in glioblastoma cell death. Biochimica et biophysica acta. Mol. Cell Res. 2017, 1864, 113–124. [Google Scholar]
- Fisher, C.J.; Niu, C.; Foltz, W.; Chen, Y.; Sidorova-Darmos, E.; Eubanks, J.H.; Lilge, L. ALA-PpIX mediated photodynamic therapy of malignant gliomas augmented by hypothermia. PLoS ONE 2017, 12, e0181654. [Google Scholar] [CrossRef]
- Cornelius, J.F.; Slotty, P.J.; El Khatib, M.; Giannakis, A.; Senger, B.; Steiger, H.J. Enhancing the effect of 5-aminolevulinic acid based photodynamic therapy in human meningioma cells. Photodiagn. Photodyn Ther. 2014, 11, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Leroy, H.A.; Guérin, L.; Lecomte, F.; Baert, G.; Vignion, A.S.; Mordon, S.; Reyns, N. Is interstitial photodynamic therapy for brain tumors ready for clinical practice? A systematic review. Photodiagn. Photodyn Ther. 2021, 36, 102492. [Google Scholar] [CrossRef] [PubMed]
- Demyanenko, S.V.; Uzdensky, A.B.; Sharifulina, S.A.; Lapteva, T.O.; Polyakova, L.P. PDT-induced epigenetic changes in the mouse cerebral cortex: A protein microarray study. Biochim. Biophys. Acta 2014, 1840, 262–270. [Google Scholar] [CrossRef]
- Kimura, S.; Kuroiwa, T.; Ikeda, N.; Nonoguchi, N.; Kawabata, S.; Kajimoto, Y.; Ishikawa, T. Assessment of safety of 5-aminolevulinic acid-mediated photodynamic therapy in rat brain. Photodiagn. Photodyn. Ther. 2018, 21, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Madsen, S.J.; Angell-Petersen, E.; Spetalen, S.; Carper, S.W.; Ziegler, S.A.; Hirschberg, H. Photodynamic therapy of newly implanted glioma cells in the rat brain. Lasers Surg. Med. 2006, 38, 540–548. [Google Scholar] [CrossRef]
- Ishikawa, T.; Kajimoto, Y.; Inoue, Y.; Ikegami, Y.; Kuroiwa, T. Critical role of ABCG2 in ALA-photodynamic diagnosis and therapy of human brain tumor. Adv. Cancer Res. 2015, 125, 197–216. [Google Scholar] [PubMed]
- Müller, P.; Abdel Gaber, S.A.; Zimmermann, W.; Wittig, R.; Stepp, H. ABCG2 influence on the efficiency of photodynamic therapy in glioblastoma cells. J. Photochem. Photobiol. B 2020, 210, 111963. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Kajimoto, Y.; Inoue, H.; Miyatake, S.; Ishikawa, T.; Kuroiwa, T. Gefitinib enhances the efficacy of photodynamic therapy using 5-aminolevulinic acid in malignant brain tumor cells. Photodiagn. Photodyn. Ther. 2013, 10, 42–50. [Google Scholar] [CrossRef]
- Girotti, A.W.; Fahey, J.M.; Korytowski, W. Multiple Means by Which Nitric Oxide can Antagonize Photodynamic Therapy. Curr. Med. Chem. 2016, 23, 2754–2769. [Google Scholar] [CrossRef] [PubMed]
- Wiehe, A.; Senge, M.O. The Photosensitizer Temoporfin (mTHPC)—Chemical, Pre-clinical and Clinical Developments in the Last Decade. Photochem. Photobiol. 2022. advance online publication. [Google Scholar] [CrossRef]
- Senge, M.O.; Brandt, J.C. Temoporfin (Foscan®, 5,10,15,20-tetra(m-hydroxyphenyl)chlorin)—A second-generation photosensitizer. Photochem. Photobiol. 2011, 87, 1240–1296. [Google Scholar] [CrossRef] [PubMed]
- Mattioli, E.J.; Ulfo, L.; Marconi, A.; Pellicioni, V.; Costantini, P.E.; Marforio, T.D.; Di Giosia, M.; Danielli, A.; Fimognari, C.; Turrini, E.; et al. Carrying Temoporfin with Human Serum Albumin: A New Perspective for Photodynamic Application in Head and Neck Cancer. Biomolecules 2022, 13, 68. [Google Scholar] [CrossRef]
- Mannino, S.; Molinari, A.; Sabatino, G.; Ciafrè, S.A.; Colone, M.; Maira, G.; Anile, C.; Arancia, G.; Mangiola, A. Intratumoral vs systemic administration of meta-tetrahydroxyphenylchlorin for photodynamic therapy of malignant gliomas: Assessment of uptake and spatial distribution in C6 rat glioma model. Int. J. Immunopathol. Pharmacol. 2008, 21, 227–231. [Google Scholar] [CrossRef]
- Molinari, A.; Bombelli, C.; Mannino, S.; Stringaro, A.; Toccacieli, L.; Calcabrini, A.; Colone, M.; Mangiola, A.; Maira, G.; Luciani, P.; et al. m-THPC-mediated photodynamic therapy of malignant gliomas: Assessment of a new transfection strategy. Int. J. Cancer 2007, 121, 1149–1155. [Google Scholar] [CrossRef] [PubMed]
- Ng, J.; Henriquez, N.; MacRobert, A.; Kitchen, N.; Williams, N.; Bown, S. Bioluminescence-activated photodynamic therapy for luciferase transfected, grade 4 astrocytoma cells in vitro. Photodiagn. Photodyn. Ther. 2022, 38, 102856. [Google Scholar] [CrossRef] [PubMed]
- Varon, E.; Blumrosen, G.; Sinvani, M.; Haimov, E.; Polani, S.; Natan, M.; Shoval, I.; Jacob, A.; Atkins, A.; Zitoun, D.; et al. An Engineered Nanocomplex with Photodynamic and Photothermal Synergistic Properties for Cancer Treatment. Int. J. Mol. Sci. 2022, 23, 2286. [Google Scholar] [CrossRef]
- Jiang, F.; Chopp, M.; Katakowski, M.; Cho, K.K.; Yang, X.; Hochbaum, N.; Tong, L.; Mikkelsen, T. Photodynamic therapy with photofrin reduces invasiveness of malignant human glioma cells. Lasers Med. Sci. 2002, 17, 280–288. [Google Scholar] [CrossRef]
- Muller, P.J.; Wilson, B.C. Photodynamic therapy of brain tumors—A work in progress. Lasers Surg. Med. 2006, 38, 384–389. [Google Scholar] [CrossRef]
- Zhang, X.; Jiang, F.; Kalkanis, S.N.; Zhang, Z.; Hong, X.; Yang, H.; Chopp, M. Post-acute response of 9L gliosarcoma to Photofrin-mediated PDT in athymic nude mice. Lasers Med. Sci. 2007, 22, 253–259. [Google Scholar] [CrossRef]
- Chopp, M.; Madigan, L.; Dereski, M.; Jiang, F.; Li, Y. Photodynamic therapy of human glioma (U87) in the nude rat. Photochem. Photobiol. 1996, 64, 707–711. [Google Scholar] [CrossRef]
- deCarvalho, A.C.; Zhang, X.; Roberts, C.; Jiang, F.; Kalkanis, S.N.; Hong, X.; Lu, M.; Chopp, M. Subclinical photodynamic therapy treatment modifies the brain microenvironment and promotes glioma growth. Glia 2007, 55, 1053–1060. [Google Scholar] [CrossRef]
- Jiang, F.; Lilge, L.; Grenier, J.; Li, Y.; Wilson, M.D.; Chopp, M. Photodynamic therapy of U87 human glioma in nude rat using liposome-delivered photofrin. Lasers Surg. Med. 1998, 22, 74–80. [Google Scholar] [CrossRef]
- Jiang, F.; Lilge, L.; Logie, B.; Li, Y.; Chopp, M. Photodynamic therapy of 9L gliosarcoma with liposome-delivered photofrin. Photochem. Photobiol. 1997, 65, 701–706. [Google Scholar] [CrossRef]
- Aziz, F.; Telara, S.; Moseley, H.; Goodman, C.; Manthri, P.; Eljamel, M.S. Photodynamic therapy adjuvant to surgery in metastatic carcinoma in brain. Photodiagn. Photodyn. Ther. 2009, 6, 227–230. [Google Scholar] [CrossRef] [PubMed]
- Jiang, F.; Lilge, L.; Belcuig, M.; Singh, G.; Grenier, J.; Li, Y.; Chopp, M. Photodynamic therapy using Photofrin in combination with buthionine sulfoximine (BSO) to treat 9L gliosarcoma in rat brain. Lasers Surg. Med. 1998, 23, 161–166. [Google Scholar] [CrossRef]
- Jiang, F.; Cho, K.K.; Mikkelse, T.; Tong, L.; Lew, Y.S.; Hochbaum, N.; Shargorodsky, J.; Chop, M. Tamoxifen increases photodynamic therapeutic response of U87 and U25ln human glioma cells. J. Neuro-Oncol. 2002, 56, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Tsukagoshi, S. Gan to kagaku ryoho. Cancer Chemother. 1995, 22, 1271–1278. [Google Scholar]
- Cole, C.D.; Liu, J.K.; Sheng, X.; Chin, S.S.; Schmidt, M.H.; Weiss, M.H.; Couldwell, W.T. Hypericin-mediated photodynamic therapy of pituitary tumors: Preclinical study in a GH4C1 rat tumor model. J. Neuro-Oncol. 2008, 87, 255–261. [Google Scholar] [CrossRef]
- Ritz, R.; Wein, H.T.; Dietz, K.; Schenk, M.; Roser, F.; Tatagiba, M.; Strauss, W.S. Photodynamic therapy of malignant glioma with hypericin: Comprehensive in vitro study in human glioblastoma cell lines. Int. J. Oncol. 2007, 30, 659–667. [Google Scholar] [CrossRef]
- Nakajima, N.; Kawashima, N. A basic study on hypericin-PDT in vitro. Photodiagn. Photodyn. Ther. 2012, 9, 196–203. [Google Scholar] [CrossRef]
- Bassler, M.C.; Rammler, T.; Wackenhut, F.; Zur Oven-Krockhaus, S.; Secic, I.; Ritz, R.; Meixner, A.J.; Brecht, M. Accumulation and penetration behavior of hypericin in glioma tumor spheroids studied by fluorescence microscopy and confocal fluorescence lifetime imaging microscopy. Anal. Bioanal. Chem. 2022, 414, 4849–4860. [Google Scholar] [CrossRef]
- Kessel, D. Hypericin Accumulation as a Determinant of PDT Efficacy. Photochem. Photobiol. 2020, 96, 1144–1147. [Google Scholar] [CrossRef]
- Muragaki, Y.; Akimoto, J.; Maruyama, T.; Iseki, H.; Ikuta, S.; Nitta, M.; Maebayashi, K.; Saito, T.; Okada, Y.; Kaneko, S.; et al. Phase II clinical study on intraoperative photodynamic therapy with talaporfin sodium and semiconductor laser in patients with malignant brain tumors. J. Neurosurg. 2013, 119, 845–852. [Google Scholar] [CrossRef]
- Akimoto, J.; Haraoka, J.; Aizawa, K. Preliminary clinical report on safety and efficacy of photodynamic therapy using talaporfin sodium for malignant gliomas. Photodiagn. Photodyn. Ther. 2012, 9, 91–99. [Google Scholar] [CrossRef]
- Hiramatsu, R.; Kawabata, S.; Tanaka, H.; Sakurai, Y.; Suzuki, M.; Ono, K.; Miyatake, S.; Kuroiwa, T.; Hao, E.; Vicente, M.G. Tetrakis(p-carboranylthio-tetrafluorophenyl)chlorin (TPFC): Application for photodynamic therapy and boron neutron capture therapy. J. Pharm. Sci. 2015, 104, 962–970. [Google Scholar] [CrossRef] [PubMed]
- Munegowda, M.A.; Fisher, C.; Molehuis, D.; Foltz, W.; Roufaiel, M.; Bassan, J.; Nitz, M.; Mandel, A.; Lilge, L. Efficacy of ruthenium coordination complex-based Rutherrin in a preclinical rat glioblastoma model. Neurooncol. Adv. 2019, 1, vdz006. [Google Scholar] [CrossRef] [PubMed]
- Hambsch, P.; Istomin, Y.P.; Tzerkovsky, D.A.; Patties, I.; Neuhaus, J.; Kortmann, R.D.; Schastak, S.; Glasow, A. Efficient cell death induction in human glioblastoma cells by photodynamic treatment with Tetrahydroporphyrin-Tetratosylat (THPTS) and ionizing irradiation. Oncotarget 2017, 8, 72411–72423. [Google Scholar] [CrossRef]
- Milla, L.N.; Yslas, E.I.; Cabral, A.; Durantini, E.N.; Romanini, S.; Rivarola, V.; Bertuzzi, M. Pharmacokinetic, toxicological and phototherapeutic studies of phthalocyanine ZnPcCF3. Biomed. Pharmacother. 2009, 63, 209–215. [Google Scholar] [CrossRef]
- Castilho-Fernandes, A.; Lopes, T.G.; Primo, F.L.; Pinto, M.R.; Tedesco, A.C. Photodynamic process induced by chloro-aluminum phthalocyanine nanoemulsion in glioblastoma. Photodiagn. Photodyn. Ther. 2017, 19, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Fontana, L.C.; Pinto, J.G.; Pereira AH, C.; Soares, C.P.; Raniero, L.J.; Ferreira-Strixino, J. Photodithazine photodynamic effect on viability of 9L/lacZ gliosarcoma cell line. Lasers Surg. Med. 2017, 32, 1245–1252. [Google Scholar] [CrossRef]
- Santos Vitorio, G.D.; de Almeida RM, S.; Pinto, J.G.; Fontana, L.C.; Ferreira-Strixino, J. Analysis of the effects of Photodynamic therapy with Photodithazine on the treatment of 9l/lacZ cells, in vitro study. Photodiagn. Photodyn. Ther. 2021, 34, 102233. [Google Scholar] [CrossRef]
- Klimenko, A.; Rodina, E.E.; Silachev, D.; Begun, M.; Babenko, V.A.; Benditkis, A.S.; Kozlov, A.S.; Krasnovsky, A.A.; Khotimchenko, Y.S.; Katanaev, V.L. Chlorin Endogenous to the North Pacific Brittle Star Ophiura sarsii for Photodynamic Therapy Applications in Breast Cancer and Glioblastoma Models. Biomedicines 2022, 10, 134. [Google Scholar] [CrossRef]
- Lobel, J.; MacDonald, I.J.; Ciesielski, M.J.; Barone, T.; Potter, W.R.; Pollina, J.; Plunkett, R.J.; Fenstermaker, R.A.; Dougherty, T.J. 2-[1-hexyloxyethyl]-2-devinyl pyropheophorbide-a (HPPH) in a nude rat glioma model: Implications for photodynamic therapy. Lasers Surg. Med. 2001, 29, 397–405. [Google Scholar] [CrossRef]
- Fujishima, I.; Sakai, T.; Tanaka, T.; Ryu, H.; Uemura, K.; Fujishima, Y.; Horiuchi, K.; Daikuzono, N.; Sekiguchi, Y. Photodynamic therapy using pheophorbide a and Nd:YAG laser. Neurol. Medico-Chir. 1991, 31, 257–263. [Google Scholar] [CrossRef]
- Cai, X.; Wang, M.; Mu, P.; Jian, T.; Liu, D.; Ding, S.; Luo, Y.; Du, D.; Song, Y.; Chen, C.L.; et al. Sequence-Defined Nanotubes Assembled from IR780-Conjugated Peptoids for Chemophototherapy of Malignant Glioma. Research 2021, 2021, 9861384. [Google Scholar] [CrossRef]
- Olivier, D.; Bourré, L.; El-Sabbagh, E.; Loussouarn, D.; Simonneaux, G.; Valette, F.; Patrice, T. Photodynamic effects of SIM01, a new sensitizer, on experimental brain tumors in rats. Surg. Neurol. 2007, 68, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, J.; Hirano, T.; Li, S.; Koide, M.; Kohno, E.; Inenaga, C.; Tokuyama, T.; Yokota, N.; Yamamoto, S.; Terakawa, S.; et al. Selective accumulation and strong photodynamic effects of a new photosensitizer, ATX-S10.Na (II), in experimental malignant glioma. Int. J. Oncol. 2005, 27, 1207–1213. [Google Scholar] [CrossRef] [PubMed]
- Xu, D.; Chen, X.; Chen, K.; Peng, Y.; Li, Y.; Ke, Y.; Gan, D. Tetra-sulfonate phthalocyanine zinc-bovine serum albumin conjugate-mediated photodynamic therapy of human glioma. J. Biomater. Appl. 2014, 29, 378–385. [Google Scholar] [CrossRef]
- Xu, D.; Ke, Y.; Jiang, X.; Cai, Y.; Peng, Y.; Li, Y. In vitro photodynamic therapy on human U251 glioma cells with a novel photosensitiser ZnPcS4-BSA. Br. J. Neurosurg. 2010, 24, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Xu, D.; Baidya, A.; Deng, K.; Li, Y.S.; Wu, B.; Xu, H.B. Multifunctional nanoparticle PEG-Ce6-Gd for MRI-guided photodynamic therapy. Oncol. Rep. 2021, 45, 547–556. [Google Scholar] [CrossRef]
- Xu, H.Z.; Li, T.F.; Ma, Y.; Li, K.; Zhang, Q.; Xu, Y.H.; Zhang, Y.C.; Zhao, L.; Chen, X. Targeted photodynamic therapy of glioblastoma mediated by platelets with photo-controlled release property. Biomaterials 2022, 290, 121833. [Google Scholar] [CrossRef]
- Ince, M.; Er, O.; Ocakoglu, K.; Lambrecht, F.Y.; Colak, S.G.; Soylu, H.M.; Kayabasi, C.; Gunduz, C. Investigation of In vitro PDT Activities and In vivo Biopotential of Zinc Phthalocyanines Using (131)I Radioisotope. Chem. Biol. Drug Des. 2016, 87, 224–232. [Google Scholar] [CrossRef]
- De Groof, T.W.M.; Mashayekhi, V.; Fan, T.S.; Bergkamp, N.D.; Sastre Toraño, J.; van Senten, J.R.; Heukers, R.; Smit, M.J.; Oliveira, S. Nanobody-Targeted Photodynamic Therapy Selectively Kills Viral GPCR-Expressing Glioblastoma Cells. Mol. Pharm. 2019, 16, 3145–3156. [Google Scholar] [CrossRef]
- Chen, M.H.; Jenh, Y.J.; Wu, S.K.; Chen, Y.S.; Hanagata, N.; Lin, F.H. Non-invasive Photodynamic Therapy in Brain Cancer by Use of Tb3+-Doped LaF3 Nanoparticles in Combination with Photosensitizer Through X-ray Irradiation: A Proof-of-Concept Study. Nanoscale Res. Lett. 2017, 12, 62. [Google Scholar] [CrossRef] [PubMed]
- Mishchenko, T.A.; Turubanova, V.D.; Mitroshina, E.V.; Alzeibak, R.; Peskova, N.N.; Lermontova, S.A.; Klapshina, L.G.; Balalaeva, I.V.; Vedunova, M.V.; Krysko, D.V. Effect of novel porphyrazine photosensitizers on normal and tumor brain cells. J. Biophotonics 2020, 13, e201960077. [Google Scholar] [CrossRef] [PubMed]
- Savyuk, M.O.; Turubanova, V.D.; Mishchenko, T.A.; Lermontova, S.A.; Klapshina, L.G.; Krysko, D.V.; Vedunova, M.V. Unraveling of Functional Activity of Primary Hippocampal Neuron-Glial Networks in Photodynamic Therapy Based on Tetracyanotetra(aryl)porphyrazines. Cells 2022, 11, 1212. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Seo, M.; Park, T.E.; Lee, D.Y. A novel therapeutic strategy of multimodal nanoconjugates for state-of-the-art brain tumor phototherapy. J. Nanobiotechnol. 2022, 20, 14. [Google Scholar] [CrossRef]
- Mfouo-Tynga, I.S.; Dias, L.D.; Inada, N.M.; Kurachi, C. Features of third generation photosensitizers used in anticancer photodynamic therapy: Review. Photodiagn. Photodyn. Ther. 2021, 34, 102091. [Google Scholar] [CrossRef]
- Paszko, E.; Ehrhardt, C.; Senge, M.O.; Kelleher, D.P.; Reynolds, J.V. Nanodrug applications in photodynamic therapy. Photodiagn. Photodyn. Ther. 2011, 8, 14–29. [Google Scholar] [CrossRef]
- Narumi, A.; Tsuji, T.; Shinohara, K.; Yamazaki, H.; Kikuchi, M.; Kawaguchi, S.; Mae, T.; Ikeda, A.; Sakai, Y.; Kataoka, H.; et al. Maltotriose-conjugation to a fluorinated chlorin derivative generating a PDT photosensitizer with improved water-solubility. Org. Biomol. Chem. 2016, 14, 3608–3613. [Google Scholar] [CrossRef]
- Waite, C.L.; Roth, C.M. Nanoscale drug delivery systems for enhanced drug penetration into solid tumors: Current progress and opportunities. Crit. Rev. Biomed. Eng. 2012, 40, 21–41. [Google Scholar] [CrossRef]
- Natesan, S.; Krishnaswami, V.; Ponnusamy, C.; Madiyalakan, M.; Woo, T.; Palanisamy, R. Hypocrellin B and nano silver loaded polymeric nanoparticles: Enhanced generation of singlet oxygen for improved photodynamic therapy. Mater. Sci. Eng. C Mater. Biol. Appl. 2017, 77, 935–946. [Google Scholar] [CrossRef]
- Temizel, E.; Sagir, T.; Ayan, E.; Isik, S.; Ozturk, R. Delivery of lipophilic porphyrin by liposome vehicles: Preparation and photodynamic therapy activity against cancer cell lines. Photodiagn. Photodyn. Ther. 2014, 11, 537–545. [Google Scholar] [CrossRef]
- Cramer, S.W.; Chen, C.C. Photodynamic Therapy for the Treatment of Glioblastoma. Front. Surg. 2020, 6, 81. [Google Scholar] [CrossRef]
- Ibarra, L.E.; Beaugé, L.; Arias-Ramos, N.; Rivarola, V.A.; Chesta, C.A.; López-Larrubia, P.; Palacios, R.E. Trojan horse monocyte-mediated delivery of conjugated polymer nanoparticles for improved photodynamic therapy of glioblastoma. Nanomedicine 2020, 15, 1687–1707. [Google Scholar] [CrossRef]
- Caverzán, M.D.; Beaugé, L.; Chesta, C.A.; Palacios, R.E.; Ibarra, L.E. Photodynamic therapy of Glioblastoma cells using doped conjugated polymer nanoparticles: An in vitro comparative study based on redox status. J. Photochem. Photobiol. B 2020, 212, 112045. [Google Scholar] [CrossRef]
- Ibarra, L.E.; Porcal, G.V.; Macor, L.P.; Ponzio, R.A.; Spada, R.M.; Lorente, C.; Chesta, C.A.; Rivarola, V.A.; Palacios, R.E. Metallated porphyrin-doped conjugated polymer nanoparticles for efficient photodynamic therapy of brain and colorectal tumor cells. Nanomedicine 2018, 13, 605–624. [Google Scholar] [CrossRef] [PubMed]
- Caverzán, M.D.; Oliveda, P.M.; Beaugé, L.; Palacios, R.E.; Chesta, C.A.; Ibarra, L.E. Metronomic Photodynamic Therapy with Conjugated Polymer Nanoparticles in Glioblastoma Tumor Microenvironment. Cells 2023, 12, 1541. [Google Scholar] [CrossRef]
- Sun, B.; Bte Rahmat, J.N.; Zhang, Y. Advanced techniques for performing photodynamic therapy in deep-seated tissues. Biomaterials 2022, 291, 121875. [Google Scholar] [CrossRef]
- Udrea, A.M.; Smarandache, A.; Dinache, A.; Mares, C.; Nistorescu, S.; Avram, S.; Staicu, A. Photosensitizers-Loaded Nanocarriers for Enhancement of Photodynamic Therapy in Melanoma Treatment. Pharmaceutics 2023, 15, 2124. [Google Scholar] [CrossRef] [PubMed]
- Ormond, A.B.; Freeman, H.S. Dye Sensitizers for Photodynamic Therapy. Materials 2013, 6, 817–840. [Google Scholar] [CrossRef] [PubMed]
- Quirk, B.J.; Brandal, G.; Donlon, S.; Vera, J.C.; Mang, T.S.; Foy, A.B.; Lew, S.M.; Girotti, A.W.; Jogal, S.; LaViolette, P.S.; et al. Photodynamic therapy (PDT) for malignant brain tumors—Where do we stand? Photodiagn. Photodyn. Ther. 2015, 12, 530–544. [Google Scholar] [CrossRef]
- Bhanja, D.; Wilding, H.; Baroz, A.; Trifoi, M.; Shenoy, G.; Slagle-Webb, B.; Hayes, D.; Soudagar, Y.; Connor, J.; Mansouri, A. Photodynamic Therapy for Glioblastoma: Illuminating the Path toward Clinical Applicability. Cancers 2023, 15, 3427. [Google Scholar] [CrossRef] [PubMed]
- Yoon, I.; Li, J.Z.; Shim, Y.K. Advance in photosensitizers and light delivery for photodynamic therapy. Clin. Endosc. 2013, 46, 7–23. [Google Scholar] [CrossRef]
- Muller, P.J.; Wilson, B.C. Photodynamic therapy for recurrent supratentorial gliomas. Semin. Surg. Oncol. 1995, 11, 346–354. [Google Scholar] [CrossRef] [PubMed]
- Vermandel, M.; Dupont, C.; Lecomte, F.; Leroy, H.A.; Tuleasca, C.; Mordon, S.; Hadjipanayis, C.G.; Reyns, N. Standardized intraoperative 5-ALA photodynamic therapy for newly diagnosed glioblastoma patients: A preliminary analysis of the INDYGO clinical trial. J. Neurooncol. 2021, 152, 501–514. [Google Scholar] [CrossRef] [PubMed]
- Hirschberg, H.; Sørensen, D.R.; Angell-Petersen, E.; Peng, Q.; Tromberg, B.; Sun, C.H.; Spetalen, S.; Madsen, S. Repetitive photodynamic therapy of malignant brain tumors. J. Environ. Pathol. Toxicol. Oncol. 2006, 25, 261–279. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Inclusion |
|---|
| The analyzed cases were brain tumors |
| Both in vivo and in vitro studies were included |
| Both review articles and research articles were included |
| Studies in which the research groups were adult patients were included in this review |
| This review included papers in which such photosensitizers were characterized as 5-ALA, Temoporfin, Photofrin, Hypericin or Talaporfin |
| Recent papers describing other types of photosensitizers and third-generation photosensitizers were also included |
| Exclusion |
| Articles in a language other than English or Polish |
| PDT for other types of cancer |
| Studies that used chemotherapy in combination with PDT were excluded |
| Studies in which magnetic resonance imaging, computed tomography or other tools were used for diagnostics were also excluded |
| Studies conducted on pregnant women or children |
| Analysis of the immune and anti-inflammatory response after PDT |
| No. | A Type of Photosensitizer | Structure | The Wavelength of the Light Source (nm) | Characteristics/ Application | Potential Side Effects | References |
|---|---|---|---|---|---|---|
| 1. | 5-ALA |  | 635 | Possible intraoperative fluorescent guidance, increase in PpIX accumulation, treatment of malignant gliomas | Minimal skin sensitization | [38,39,40,41] |
| 2. | Temoporfin —THPC |  | 650 | Squamous cell tumors of the head and neck | May cause complaints associated with high photosensitivity of the skin | [70,71] |
| 3. | Photofrin |  | 630–660 | Inhibits the invasiveness of glioblastoma cells; has the ability to induce VEGF expression in the tissue adjacent to the tumor; causes a transient increase in cell proliferation associated with strong activation of astrocytes and microglia in the treated region | Slight skin irritation may occur | [76] |
| 4. | Hypericin |  | 590–660 | Shows a promising therapeutic approach in the treatment of glioblastoma | Systemic side effects in healthy tissues | [88] |
| 5. | Talaporfin |  | 630–667 | Treatment of primary malignant brain parenchymal tumors | The possibility of side effects on the skin (rash, blisters, erythema) | [90] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bartusik-Aebisher, D.; Woźnicki, P.; Dynarowicz, K.; Aebisher, D. Photosensitizers for Photodynamic Therapy of Brain Cancers—A Review. Brain Sci. 2023, 13, 1299. https://doi.org/10.3390/brainsci13091299
Bartusik-Aebisher D, Woźnicki P, Dynarowicz K, Aebisher D. Photosensitizers for Photodynamic Therapy of Brain Cancers—A Review. Brain Sciences. 2023; 13(9):1299. https://doi.org/10.3390/brainsci13091299
Chicago/Turabian StyleBartusik-Aebisher, Dorota, Paweł Woźnicki, Klaudia Dynarowicz, and David Aebisher. 2023. "Photosensitizers for Photodynamic Therapy of Brain Cancers—A Review" Brain Sciences 13, no. 9: 1299. https://doi.org/10.3390/brainsci13091299