
Pre- and Post-Operative Online Prediction of Outcome in Patients Undergoing Endovascular Coiling after Aneurysmal Subarachnoid Hemorrhage: Visual and Dynamic Nomograms

Abstract
:1. Background
2. Methods
2.1. Study Population
2.2. Treatment of Ruptured Aneurysm
2.3. Data Collection and Definition
2.4. Outcome Measure
2.5. Statistical Analysis and Construction of Dynamic Nomogram
2.6. Validation of Model
3. Results
3.1. Patient Characteristic
3.2. Variable Selection (by Univariate and Multivariate Analyses)
3.3. Construction and Performance of Visualized Online Nomograms
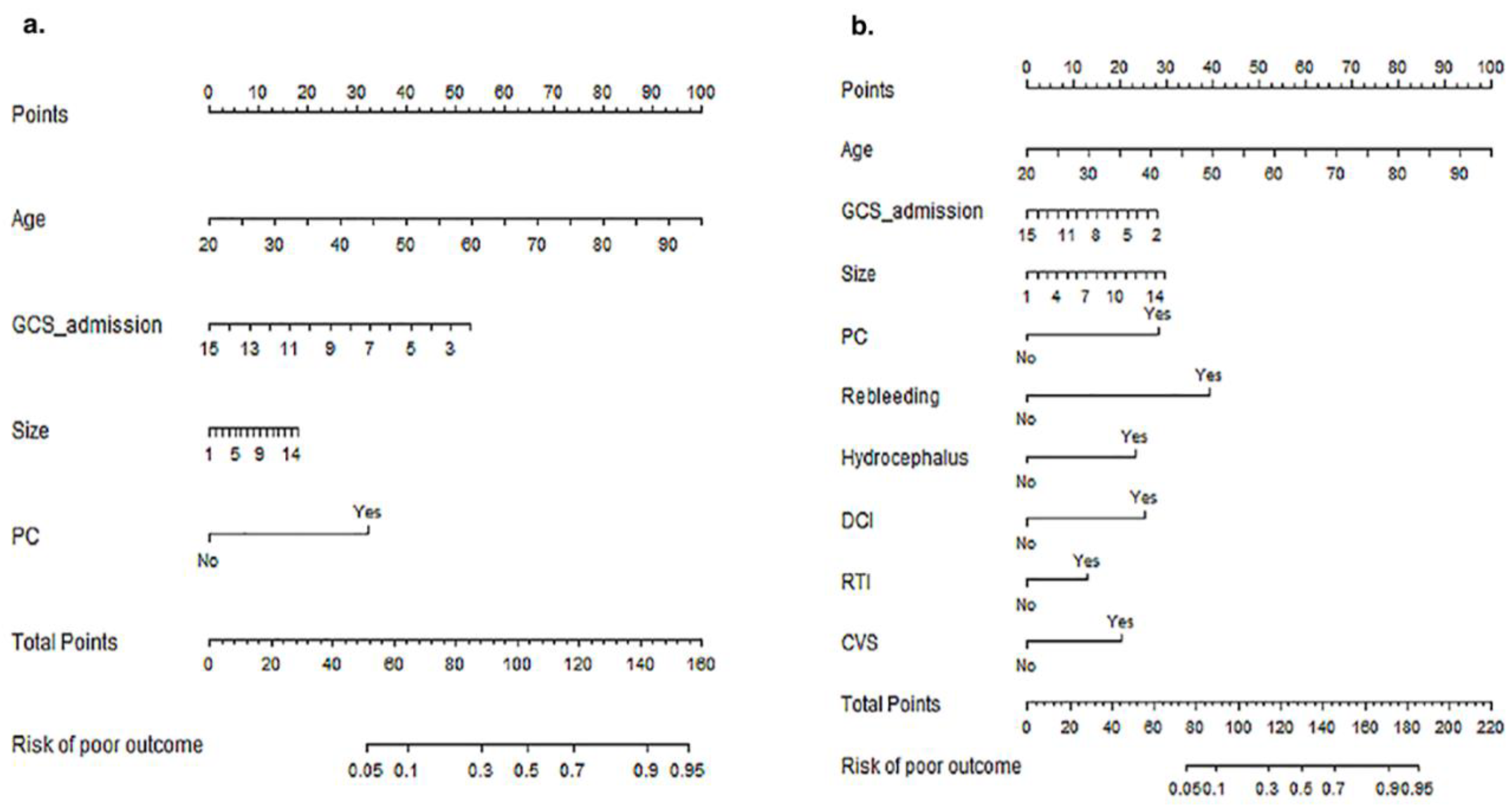
Development of Nomograms
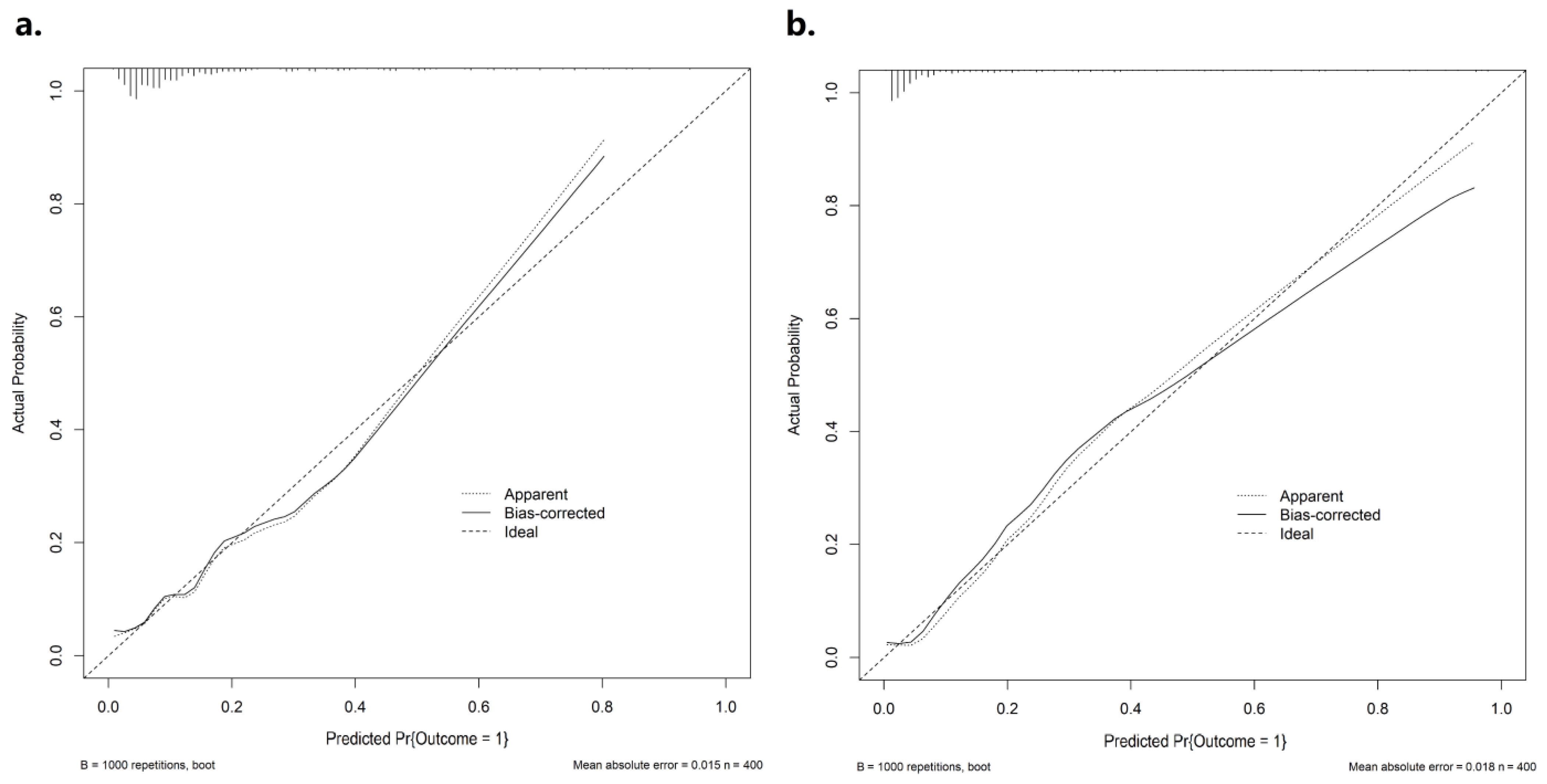
3.4. Discrimination and Calibration of Nomograms
3.5. Clinical Utility of Nomograms
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Neifert, S.N.; Chapman, E.K.; Martini, M.L.; Shuman, W.H.; Schupper, A.J.; Oermann, E.K.; Mocco, J.; Macdonald, R.L. Aneurysmal Subarachnoid Hemorrhage: The Last Decade. Transl. Stroke Res. 2021, 12, 428–446. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, R.L.; Schweizer, T.A. Spontaneous subarachnoid haemorrhage. Lancet 2017, 389, 655–666. [Google Scholar] [CrossRef] [PubMed]
- Ran, K.R.; Wang, A.C.; Nair, S.K.; Akça, O.; Xu, R. Acute Multidisciplinary Management of Aneurysmal Subarachnoid Hemorrhage (aSAH). Balk. Med. J. 2023, 40, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Al-Khindi, T.; Macdonald, R.L.; Schweizer, T.A. Cognitive and Functional Outcome after Aneurysmal Subarachnoid Hemorrhage. Stroke 2010, 41, e519–e536. [Google Scholar] [CrossRef] [Green Version]
- Nieuwkamp, D.J.; Setz, L.E.; Algra, A.; Linn, F.H.; de Rooij, N.K.; Rinkel, G.J. Changes in case fatality of aneurysmal subarachnoid haemorrhage over time, according to age, sex, and region: A meta-analysis. Lancet Neurol. 2009, 8, 635–642. [Google Scholar] [CrossRef]
- Lindgren, A.; Vergouwen, M.D.; van der Schaaf, I.; Algra, A.; Wermer, M.; Clarke, M.J.; Rinkel, G.J. Endovascular coiling versus neurosurgical clipping for people with aneurysmal subarachnoid haemorrhage. Cochrane Stroke Group, editor. Cochrane Database Syst. Rev. 2018, 8, CD003085. [Google Scholar]
- Molyneux, A.J.; Kerr, R.S.; Yu, L.M.; Clarke, M.; Sneade, M.; Yarnold, J.A.; Sandercock, P. International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: A randomised com-parison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet 2005, 366, 809–817. [Google Scholar]
- Rubbert, C.; Patil, K.R.; Beseoglu, K.; Mathys, C.; May, R.; Kaschner, M.G.; Sigl, B.; Teichert, N.A.; Boos, J.; Turowski, B.; et al. Prediction of outcome after aneurysmal subarachnoid haemorrhage using data from patient admission. Eur. Radiol. 2018, 28, 4949–4958. [Google Scholar] [CrossRef]
- Jaja, B.N.R.; Saposnik, G.; Lingsma, H.F.; Macdonald, E.; Thorpe, K.E.; Mamdani, M.; Steyerberg, E.W.; Molyneux, A.; Manoel, A.L.d.O.; Schatlo, B.; et al. Development and validation of outcome prediction models for aneurysmal subarachnoid haemorrhage: The SAHIT multinational cohort study. BMJ 2018, 360, j5745. [Google Scholar] [CrossRef] [Green Version]
- Van Donkelaar, C.E.; Bakker, N.; Birks, J. Prediction of Outcome After Aneurysmal Subarachnoid Hemorrhage: Development and validation of the SAFIRE grading scale. Stroke 2019, 50, 837–844. [Google Scholar] [CrossRef]
- Stienen, M.N.; Germans, M.; Burkhardt, J.K.; Neidert, M.C.; Fung, C.; Bervini, D.; Zumofen, D.; Roethlisberger, M.; Marbacher, S.; Maduri, R.; et al. Predictors of In-Hospital Death After Aneurysmal Subarachnoid Hemorrhage: Analysis of a Nationwide Database (Swiss SOS [Swiss Study on Aneurysmal Subarachnoid Hem-orrhage]). Stroke 2018, 49, 333–340. [Google Scholar] [CrossRef]
- Neidert, M.C.; Maldaner, N.; Stienen, M.N.; Roethlisberger, M.; Zumofen, D.W.; Marbacher, S.; Maduri, R.; Hostettler, I.C.; Schatlo, B.; Schneider, M.M.; et al. The Barrow Neurological Institute Grading Scale as a Predictor for Delayed Cerebral Ischemia and Outcome After Aneurysmal Subarachnoid Hemorrhage: Data From a Nationwide Patient Registry (Swiss SOS). Neurosurgery 2018, 83, 1286–1293. [Google Scholar] [CrossRef]
- Washington, C.W.; Derdeyn, C.P.; Dacey, R.G.; Dhar, R.; Zipfel, G.J. Analysis of subarachnoid hemorrhage using the Nationwide Inpatient Sample: The NIS-SAH Severity Score and Outcome Measure: Clinical article. J. Neurosurg. 2014, 121, 482–489. [Google Scholar] [CrossRef] [PubMed]
- Maldaner, N.; Zeitlberger, A.M.; Sosnova, M.; Goldberg, J.; Fung, C.; Bervini, D.; May, A.; Bijlenga, P.; Schaller, K.; Roethlisberger, M.; et al. Development of a Complication- and Treat-ment-Aware Prediction Model for Favorable Functional Outcome in Aneurysmal Subarachnoid Hemorrhage Based on Machine Learning. Neurosurgery 2021, 88, E150–E157. [Google Scholar] [CrossRef]
- Teasdale, G.; Jennett, B. Assessment of coma and impaired consciousness. A practical scale. Lancet 1974, 2, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Brennan, P.M.; Murray, G.D.; Teasdale, G.M. A practical method for dealing with missing Glasgow Coma Scale verbal component scores. J. Neurosurg. 2020, 135, 214–219. [Google Scholar] [CrossRef]
- Van Calster, B.; Wynants, L.; Verbeek, J.F.; Verbakel, J.Y.; Christodoulou, E.; Vickers, A.J.; Roobol, M.J.; Steyerberg, E.W. Reporting and Interpreting Decision Curve Analysis: A Guide for Investigators. Eur. Urol. 2018, 74, 796–804. [Google Scholar] [CrossRef] [PubMed]
- Vickers, A.J.; Elkin, E.B. Decision curve analysis: A novel method for evaluating prediction models. Med. Decis. Mak. 2006, 26, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Risselada, R.; Lingsma, H.F.; Bauer-Mehren, A.; Friedrich, C.M.; Molyneux, A.J.; Kerr, R.S.C.; Yarnold, J.; Sneade, M.; Steyerberg, E.W.; Sturkenboom, M.C.J.M. Prediction of 60 day case-fatality after aneurysmal subarachnoid haemorrhage: Results from the International Subarachnoid Aneurysm Trial (ISAT). Eur. J. Epidemiol. 2010, 25, 261–266. [Google Scholar] [CrossRef]
- Schuss, P.; Hadjiathanasiou, A.; Borger, V.; Wispel, C.; Vatter, H.; Güresir, E. Poor-Grade Aneurysmal Subarachnoid Hemorrhage: Factors Influencing Functional Outcome—A Single-Center Series. World Neurosurg. 2016, 85, 125–129. [Google Scholar] [CrossRef]
- Park, S.Y. Nomogram: An analogue tool to deliver digital knowledge. J. Thorac. Cardiovasc. Surg. 2018, 155, 1793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, L.; Xie, J.; Wu, W.; Chen, H.; Li, S.; He, H.; Yu, Y.; Hu, M.; Li, J.; Zheng, R.; et al. A simple nomogram for predicting failure of non-invasive respiratory strategies in adults with COVID-19: A retrospective multicentre study. Lancet Digit. Health 2021, 3, e166–e174. [Google Scholar] [CrossRef] [PubMed]
- Jia, X.; Chu, X.; Jiang, L.; Li, Y.; Zhang, Y.; Mao, Z.; Liang, T.; Du, Y.; Xu, L.; Shen, Y.; et al. Predicting checkpoint inhibitors pneumonitis in non-small cell lung cancer using a dynamic online hypertension nomogram. Lung Cancer 2022, 170, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Jalali, A.; Alvarez-Iglesias, A.; Roshan, D.; Newell, J. Visualising statistical models using dynamic nomograms. Calabrese R, editor. PLoS ONE 2019, 14, e0225253. [Google Scholar] [CrossRef]
- Liu, J.; Xiong, Y.; Zhong, M.; Yang, Y.; Guo, X.; Tan, X.; Zhao, B. Predicting Long-Term Outcomes After Poor-Grade Aneurysmal Subarachnoid Hemorrhage Using Decision Tree Modeling. Neurosurgery 2020, 87, 523–529. [Google Scholar] [CrossRef]
- Gotoh, O.; Tamura, A.; Yasui, N.; Suzuki, A.; Hadeishi, H.; Sano, K. Glasgow Coma Scale in the Prediction of Outcome after Early Aneurysm Surgery. Neurosurgery 1996, 39, 19–25; 24–25. [Google Scholar] [CrossRef] [PubMed]
- Zheng, K.; Zhong, M.; Zhao, B.; Chen, S.-Y.; Tan, X.-X.; Li, Z.-Q.; Xiong, Y.; Duan, C.-Z. Poor-Grade Aneurysmal Subarachnoid Hemorrhage: Risk Factors Affecting Clinical Outcomes in Intracranial Aneurysm Patients in a Multi-Center Study. Front. Neurol. 2019, 10, 123. [Google Scholar] [CrossRef] [Green Version]
- Oshiro, E.M.; Walter, K.A.; Piantadosi, S.; Witham, T.F.; Tamargo, R.J. A New Subarachnoid Hemorrhage Grading System Based on the Glasgow Coma Scale: A Comparison with the Hunt and Hess and World Federation of Neurological Surgeons Scales in a Clinical Series. Neurosurgery 1997, 41, 140–148; 147–148; [Google Scholar] [CrossRef]
- Ban, V.S.; El Ahmadieh, T.Y.; Aoun, S.G.; Plitt, A.R.; Lyon, K.A.; Eddleman, C.; Beecher, J.; McDougall, C.M.; Reisch, J.; Welch, B.G.; et al. Prediction of Outcomes for Ruptured Aneurysm Surgery: The Southwestern Aneurysm Severity Index. Stroke 2019, 50, 595–601. [Google Scholar] [CrossRef]
- Wang, Y.; Xie, Y.; Wang, H.; Zhang, J.; Li, C.; Chen, F.; Ren, C.; Xu, Z.; Liu, M.; Li, L.; et al. Development and Clinical Translation of a Perioperative Nomogram Incorporating Free Fatty Acids to Predict Poor Outcome of Aneurysmal Subarachnoid Hemorrhage Following Endovascular Treatment. Front. Neurol. 2021, 12, 629997. [Google Scholar] [CrossRef]
- Li, S.; Zhang, J.; Li, N.; Wang, D.; Zhao, X. Predictive nomogram models for unfavorable prognosis after aneurysmal subarachnoid hemorrhage: Analysis from a prospective, observational cohort in China. CNS Neurosci. Ther. 2023; online ahead of print. [Google Scholar] [CrossRef]
- Hostettler, I.C.; Sebök, M.; Ambler, G.; Muroi, C.; Prömmel, P.; Neidert, M.C.; Richter, J.K.; Pangalu, A.; Regli, L.; Germans, M.R. Validation and Optimization of Barrow Neurological Institute Score in Prediction of Adverse Events and Functional Outcome After Subarachnoid Hemorrhage-Creation of the HATCH (Hemorrhage, Age, Treatment, Clinical State, Hydrocephalus) Score. Neurosurgery 2020, 88, 96–105. [Google Scholar] [CrossRef]
- Lu, V.M.; Graffeo, C.S.; Perry, A.; Carlstrom, L.P.; Rangel-Castilla, L.; Lanzino, G.; Brinjikji, W.; Wijdicks, E.F.M.; Rabinstein, A.A. Rebleeding drives poor outcome in aneurysmal subarachnoid hemorrhage independent of delayed cerebral ischemia: A propensity-score matched cohort study. J. Neurosurg. 2019, 133, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Samuels, O.B.; Sadan, O.; Feng, C.; Martin, K.; Medani, K.; Mei, Y.; Barrow, D.L. Aneurysmal Subarachnoid Hemorrhage: Trends, Out-comes, and Predictions From a 15-Year Perspective of a Single Neurocritical Care Unit. Neurosurgery 2021, 88, 574–583. [Google Scholar] [CrossRef] [PubMed]
- Boulouis, G.; Labeyrie, M.A.; Raymond, J.; Rodriguez-Régent, C.; Lukaszewicz, A.C.; Bresson, D.; Ben Hassen, W.; Trystram, D.; Meder, J.F.; Oppenheim, C.; et al. Treatment of cerebral vasospasm following aneurysmal subarachnoid haemorrhage: A systematic review and meta-analysis. Eur. Radiol. 2016, 27, 3333–3342. [Google Scholar] [CrossRef]
- Lucke-Wold, B.P.; Logsdon, A.F.; Manoranjan, B.; Turner, R.C.; McConnell, E.; Vates, G.E.; Huber, J.D.; Rosen, C.L.; Simard, J.M. Aneurysmal Subarachnoid Hemorrhage and Neuroinflammation: A Comprehensive Review. Int. J. Mol. Sci. 2016, 17, 497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DI Vergouwen, M.; Etminan, N.; Ilodigwe, D.; Macdonald, R.L. Lower incidence of cerebral infarction correlates with improved functional outcome after aneurysmal subarachnoid hemorrhage. J. Cereb. Blood Flow Metab. 2011, 31, 1545–1553. [Google Scholar] [CrossRef] [Green Version]
- van der Harst, J.J.; Elting, J.W.J.; Bokkers, R.P.H.; Veeger, N.J.G.M.; van Donkelaar, C.E.; van den Bergh, W.M.; Metzemaekers, J.D.M.; Groen, R.J.M.; Mazuri, A.; Luijckx, G.R.; et al. The Diagnostic Value of Near-Infrared Spectroscopy to Predict Delayed Cerebral Ischemia and Unfavorable Outcome After Subarachnoid Hemorrhage. World Neurosurg. 2023; online ahead of print. [Google Scholar]
- Zhao, B.; Yang, H.; Zheng, K.; Li, Z.; Xiong, Y.; Tan, X.; Zhong, M.; Je, B.; Rf, S.; Mn, H.; et al. Preoperative and postoperative predictors of long-term outcome after endovascular treatment of poor-grade aneurysmal subarachnoid hemorrhage. J. Neurosurg. 2016, 126, 1764–1771. [Google Scholar] [CrossRef]
- Molyneux, A.; Kerr, R.; Stratton, I.; Sandercock, P.; Clarke, M.; Shrimpton, J.; Holman, R. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: A randomised trial. Lancet 2002, 360, 1267–1274. [Google Scholar] [CrossRef]
- Wilson, T.J.; Davis, M.C.; Stetler, W.R.; Giles, D.A.; Chaudhary, N.; Gemmete, J.J.; Thompson, B.G.; Pandey, A.S. Endovascular treatment for aneurysmal sub-arachnoid hemorrhage in the ninth decade of life and beyond. J. NeuroIntervent. Surg. 2014, 6, 175–177. [Google Scholar] [CrossRef]
- Wiebers, D.O.; Whisnant, J.P.; Huston, J., 3rd; Meissner, I.; Brown, R.D., Jr.; Piepgras, D.G.; Forbes, G.S.; Thielen, K.; Nichols, D.; O’Fallon, W.M.; et al. Unruptured intracranial aneurysms: Natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet 2003, 362, 103–110. [Google Scholar] [CrossRef]
- Fisher, C.M.; Kistler, J.P.; Davis, J.M. Relation of Cerebral Vasospasm to Subarachnoid Hemorrhage Visualized by Computerized Tomographic Scanning. Neurosurgery 1980, 6, 1–9. [Google Scholar] [CrossRef]
- Jagger, J.; Torner, J.C.; Kassell, N.F. Neurologic assessment of subarachnoid hemorrhage in a large patient series. Surg. Neurol. 1989, 32, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, K.W.; Teasdale, G.; Knill-Jones, R.P.; Murray, L. Observer variability in grading patients with subarachnoid hemorrhage. J. Neurosurg. 1982, 56, 628–633. [Google Scholar] [CrossRef] [PubMed]
- Rosen, D.S.; Macdonald, R.L. Subarachnoid Hemorrhage Grading Scales: A Systematic Review. Neurocritical Care 2005, 2, 110–118. [Google Scholar] [CrossRef]
- Svensson, E.; Starmark, J.-E.; Ekholm, S.; von Essen, C.; Johansson, A. Analysis of interobserver disagreement in the assessment of subarachnoid blood and acute hydrocephalus on CT scans. Neurol. Res. 1996, 18, 487–494. [Google Scholar] [CrossRef]
- van der Jagt, M.; Hasan, D.; Bijvoet, H.C.; Pieterman, H.; Koudstaal, P.; Avezaat, C.J. Interobserver variability of cisternal blood on CT after aneurysmal subarachnoid hemorrhage. Neurology 2000, 54, 2156–2158. [Google Scholar] [CrossRef] [PubMed]
- Shirao, S.; Yoneda, H.; Kunitsugu, I.; Ishihara, H.; Koizumi, H.; Suehiro, E.; Nomura, S.; Kato, S.; Fujisawa, H.; Suzuki, M. Preoperative Prediction of Outcome in 283 Poor-Grade Patients with Subarachnoid Hemorrhage: A Project of the Chugoku-Shikoku Division of the Japan Neurosurgical Society. Cerebrovasc. Dis. 2010, 30, 105–113. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | Total Cohort (n = 400) | Good Outcome (n = 341) | Poor Outcome (n = 59) | p-Value |
|---|---|---|---|---|
| Demographic data | ||||
| Age, years, mean (SD) | 58.6 (10.7) | 57.30 (10.09) | 65.88 (11.25) | <0.001 † |
| Gender (Female), n (%) | 278 (69.5) | 101 (29.6) | 21 (35.6) | 0.443 |
| Medical history, n (%) | ||||
| Hypertension | 201 (50.3) | 166 (48.7) | 35 (59.3) | 0.171 |
| Diabetes mellitus | 15 (3.8) | 12 (3.5) | 3 (5.1) | 0.831 |
| Hyperlipidemia | 4 (1.0) | 3 (0.9) | 1 (1.7) | 1.000 |
| Coronary heart disease | 30 (7.5) | 23 (6.7) | 7 (11.9) | 0.267 |
| Atrial fibrillation | 4 (1.0) | 3 (0.9) | 1 (1.7) | 1.000 |
| Smoking, n (%) | 64 (16.0) | 55 (16.1) | 9 (15.3) | 1.000 |
| Drinking, n (%) | 25 (6.3) | 21 (6.2) | 4 (6.8) | 1.000 |
| Clinical status on admission | ||||
| Hunt-Hess grade on admission, n (%) | <0.001 † | |||
| Ⅰ | 29 (7.3) | 26 (7.6) | 3 (5.1) | |
| Ⅱ | 278 (69.5) | 256 (75.1) | 22 (37.3) | |
| Ⅲ | 55 (13.8) | 39 (11.4) | 16 (27.1) | |
| Ⅳ | 38 (9.5) | 20 (5.9) | 18 (30.5) | |
| GCS on admission, mean (SD) | 13.7 (2.93) | 14.21 (2.20) | 10.93 (4.62) | <0.001 † |
| Aneurysmal characteristics | ||||
| Aneurysmal size, mm, n (%) | 5.04 (2.22) | 4.94 (2.10) | 5.62 (2.72) | 0.030 † |
| Multiple aneurysm (yes), n (%) | 115 (28.8) | 95 (27.9) | 20 (33.9) | 0.429 |
| PC location (yes), n (%) | 22 (5.5) | 14 (4.1) | 8 (13.6) | 0.008 † |
| Irregular shape (yes), n (%) | 217 (54.3) | 184 (54.0) | 33 (55.9) | 0.889 |
| Wide neck (yes), n (%) | 289 (72.3) | 245 (71.8) | 44 (74.6) | 0.784 |
| Variables | Total Cohort (n = 400) | Good Outcome (n = 341) | Poor Outcome (n = 59) | p-Value |
|---|---|---|---|---|
| Embolization technique, n (%) | 0.268 | |||
| Coiling only | 179 (44.8) | 157 (46.0) | 22 (37.3) | |
| Stent-assisted coiling | 221 (55.3) | 184 (54.0) | 37 (62.7) | |
| Immediate aneurysm occlusion, n (%) | 0.925 | |||
| Complete occlusion | 387 (96.8) | 329 (99.4) | 58 (98.3) | |
| Incomplete occlusion | 3 (0.8) | 2 (0.6) | 1 (1.7) | |
| Aneurysm rebleeding, n (%) | 27 (6.75) | 13 (3.8) | 14 (23.7) | <0.001 † |
| Cerebral vasospasm, n (%) | 96 (24.0) | 60 (17.6) | 36 (61.0) | <0.001 † |
| Hydrocephalus, n (%) | 18 (4.5) | 7 (2.1) | 11 (18.6) | <0.001 † |
| EVD, n (%) | 13 (3.25) | 4 (1.2) | 9 (15.3) | <0.001 † |
| DCI, n (%) | 49 (12.3) | 25 (7.3) | 24 (40.7) | <0.001 † |
| Intracranial infection, n (%) | 6 (1.5) | 3 (0.9) | 3 (5.1) | 0.061 |
| RTI, n (%) | 119 (29.8) | 79 (23.2) | 40 (67.8) | <0.001 † |
| Predictors | Pre-Operative Model | Post-Operative Model | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Age | 1.078 | 1.044–1.115 | <0.001 | 1.074 | 1.035–1.118 | <0.001 |
| PC location | 6.188 | 2.097–17.670 | <0.001 | 4.520 | 1.239–16.448 | 0.021 |
| Size | 1.075 | 0.939–1.224 | 0.285 | 1.120 | 0.968–1.296 | 0.124 |
| GCS on admission | 0.795 | 0.731–0.862 | 0.001 | 0.891 | 0.806–0.987 | 0.026 |
| Rebleeding | 8.103 | 2.779–24.050 | <0.001 | |||
| Hydrocephalus | 3.462 | 0.937–12.707 | 0.059 | |||
| DCI | 3.843 | 1.539–9.872 | 0.004 | |||
| CVS | 2.933 | 1.311–6.569 | 0.008 | |||
| RTI | 1.982 | 0.911–4.297 | 0.082 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, Z.; Wang, F.; Chen, T.; Wei, Z.; Chen, C.; Xiang, L.; Xiang, L.; Zhang, Q.; Huang, K.; Jiang, F.; et al. Pre- and Post-Operative Online Prediction of Outcome in Patients Undergoing Endovascular Coiling after Aneurysmal Subarachnoid Hemorrhage: Visual and Dynamic Nomograms. Brain Sci. 2023, 13, 1185. https://doi.org/10.3390/brainsci13081185
Zhou Z, Wang F, Chen T, Wei Z, Chen C, Xiang L, Xiang L, Zhang Q, Huang K, Jiang F, et al. Pre- and Post-Operative Online Prediction of Outcome in Patients Undergoing Endovascular Coiling after Aneurysmal Subarachnoid Hemorrhage: Visual and Dynamic Nomograms. Brain Sciences. 2023; 13(8):1185. https://doi.org/10.3390/brainsci13081185
Chicago/Turabian StyleZhou, Zhou, Fusang Wang, Tingting Chen, Ziqiao Wei, Chen Chen, Lan Xiang, Liang Xiang, Qian Zhang, Kaizong Huang, Fuping Jiang, and et al. 2023. "Pre- and Post-Operative Online Prediction of Outcome in Patients Undergoing Endovascular Coiling after Aneurysmal Subarachnoid Hemorrhage: Visual and Dynamic Nomograms" Brain Sciences 13, no. 8: 1185. https://doi.org/10.3390/brainsci13081185