
Effects of Long-Term Oral Administration of N-Palmitoylethanolamine in Subjects with Mild Cognitive Impairment: Study Protocol
 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
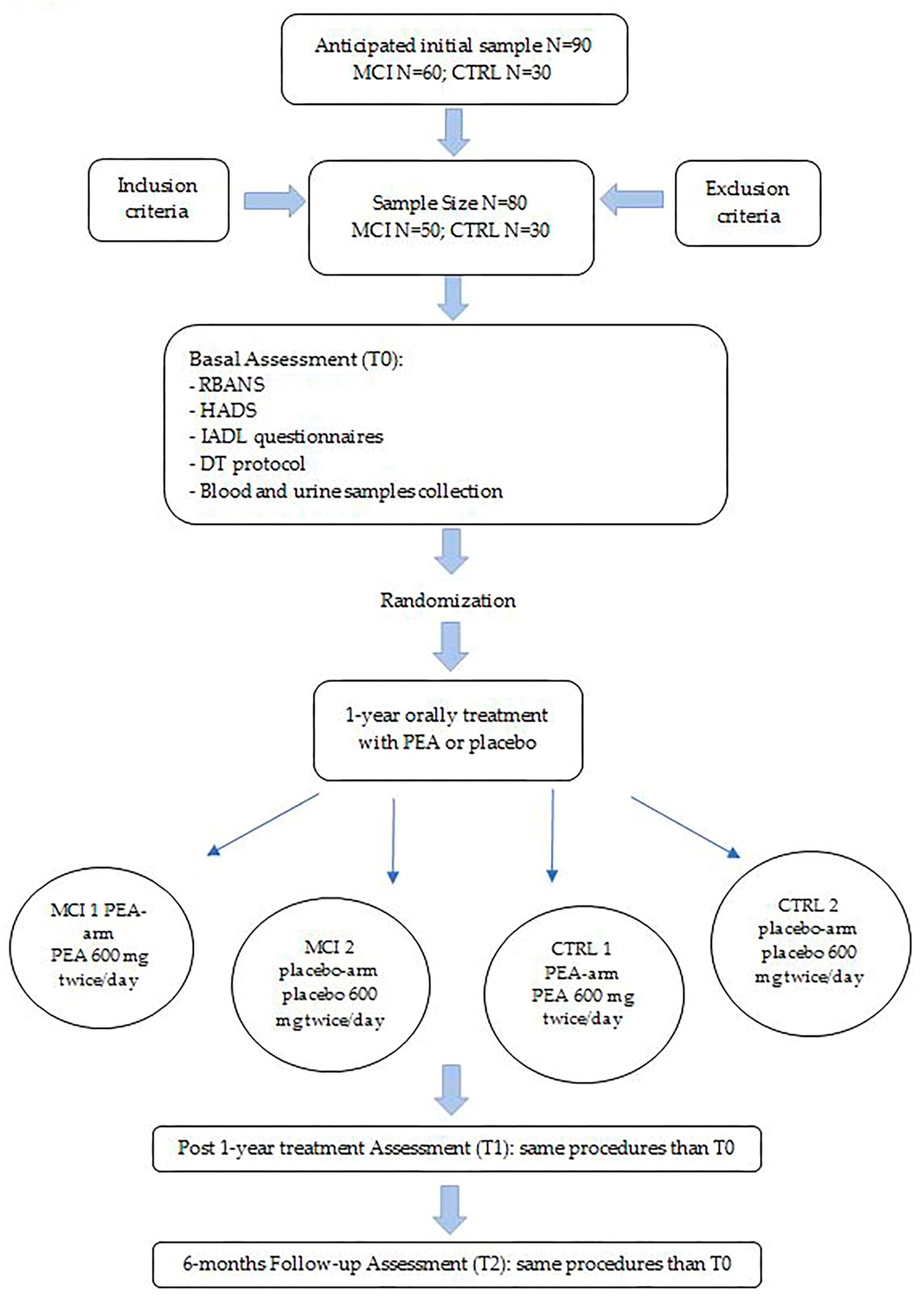
2.1. Aims, Design and Setting of the Study
- Aim 1: To determine if PEA has any effect on neuropsychological, behavioral and functional assessment scores after one-year treatment by comparing treated and placebo arms, both in MCI and control groups;
- Aim 2: To determine if PEA modifies inflammatory and neuronal damage markers, both at the blood and urine levels in MCI subjects;
- Aim 3: To determine if these changes correlate with clinical scores in all study participants.
- Aim 1:
- Aims 2 and 3:
2.2. Recruitment and Screening of Participants
2.3. Assessment Procedures
2.3.1. Humans Cognitive, Behavioral and Functional Disability Assessment
- The RBANS battery [23] will be used for cognitive assessment. This neuropsychological battery measures cognitive decline, even in very mild dementia, or improvement across different domains: Immediate Memory, Visuospatial/Constructional Abilities, Language, Attention, Delayed Memory.
- HADS [24] will be used for behavioral assessment. It is useful in identifying the anxiety and depression levels of participants.
- IADL [25] is an appropriate instrument to assess independent living skills at a functional level.
- The DT [26] protocol assesses the cognitive–motor efficiency when simultaneously performing a cognitive and a motor task. It seems to be a reliable tool even in pre-dementia stages and consists of performing three 2 min tasks, two neutrals (motor task, cognitive task) and the other one with the concurrent tasks.
2.3.2. Biochemical Analyses
- Apolipoprotein (apo) E genotyping: ApoE genotype of each participant will be determined via PCR, according to standard procedures. Humans have three versions of the APOE gene: ε2, ε3 and ε4 alleles. ApoE genotyping can help estimate a patient’s risk of converting from MCI to AD. In fact, in precedent studies, the epsilon4 allele of apolipoprotein E was considered as the major genetic risk factor for AD onset [27] and conversion to dementia in MCI patients [28].
- Central and peripheral inflammation: Selected inflammatory markers, specifically altered in MCI and possibly providing predictive information in AD progression, namely, C-reactive protein, interleukin (IL)-6, IL-8, IL-10, monocyte chemotactic protein-1, macrophage inflammatory protein-1beta and soluble triggering receptor expressed on myeloid cells 2, will be evaluated via ELISA and/or the Luminex platform.
- Amyloid-β, tau and neurofilament light chain: To monitor disease progression and treatment response, neurofilament light-chain protein, Aβ42, total and phosphorylated tau will be quantified via ELISA or using the multiplex Luminex platform.
- Oxidative stress: The effects of PEA treatment on oxidative/nitrosative stress that occurs at an early stage in AD will be assessed by measuring the presence of 3-nitrotyrosine and 4-hydroxynonenal (two end products of peroxynitrite), through ELISA [29].
- PEA, AEA and their main catabolic enzymes: The levels of PEA and AEA will be assessed via state-of-the-art liquid chromatography/mass spectrometry. In parallel, enzymatic activity of FAAH and NAAA [5] will be measured via radiometric assays.
3. Statistics and Outcomes
3.1. Data Analysis
3.2. Outcomes
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Soria Lopez, J.A.; González, H.M.; Léger, G.C. Alzheimer’s Disease. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2019; Volume 167, pp. 231–255. ISBN 978-0-12-804766-8. [Google Scholar]
- Petersen, R.C. Mild cognitive impairment. Contin. Lifelong Learn. Neurol. 2016, 22, 404–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, W.-S.; Barrett, D.A.; Randall, M.D. ‘Entourage’ Effects of N-Palmitoylethanolamide and N-Oleoylethanolamide on Vasorelaxation to Anandamide Occur through TRPV1 Receptors: Effect of Congeners on Anandamide Vasorelaxation. Br. J. Pharmacol. 2008, 155, 837–846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ueda, N.; Tsuboi, K.; Uyama, T. Metabolism of Endocannabinoids and Related N-Acylethanolamines: Canonical and Alternative Pathways. FEBS J. 2013, 280, 1874–1894. [Google Scholar] [CrossRef] [PubMed]
- Maccarrone, M. Missing Pieces to the Endocannabinoid Puzzle. Trends Mol. Med. 2020, 26, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Solorzano, C.; Zhu, C.; Battista, N.; Astarita, G.; Lodola, A.; Rivara, S.; Mor, M.; Russo, R.; Maccarrone, M.; Antonietti, F.; et al. Selective N-Acylethanolamine-Hydrolyzing Acid Amidase Inhibition Reveals a Key Role for Endogenous Palmitoylethanolamide in Inflammation. Proc. Natl. Acad. Sci. USA 2009, 106, 20966–20971. [Google Scholar] [CrossRef]
- Mattace Raso, G.; Russo, R.; Calignano, A.; Meli, R. Palmitoylethanolamide in CNS Health and Disease. Pharmacol. Res. 2014, 86, 32–41. [Google Scholar] [CrossRef]
- Esposito, E.; Cuzzocrea, S. Palmitoylethanolamide in Homeostatic and Traumatic Central Nervous System Injuries. CNS Neurol. Disord. Drug Targets 2013, 12, 55–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Agostino, G.; Russo, R.; Avagliano, C.; Cristiano, C.; Meli, R.; Calignano, A. Palmitoylethanolamide Protects against the Amyloid-Β25-35-Induced Learning and Memory Impairment in Mice, an Experimental Model of Alzheimer Disease. Neuropsychopharmacology 2012, 37, 1784–1792. [Google Scholar] [CrossRef] [Green Version]
- Scuderi, C.; Stecca, C.; Valenza, M.; Ratano, P.; Bronzuoli, M.R.; Bartoli, S.; Steardo, L.; Pompili, E.; Fumagalli, L.; Campolongo, P.; et al. Palmitoylethanolamide Controls Reactive Gliosis and Exerts Neuroprotective Functions in a Rat Model of Alzheimer’s Disease. Cell Death Dis. 2014, 5, e1419. [Google Scholar] [CrossRef] [Green Version]
- Tomasini, M.C.; Borelli, A.C.; Beggiato, S.; Ferraro, L.; Cassano, T.; Tanganelli, S.; Antonelli, T. Differential Effects of Palmitoylethanolamide against Amyloid-β Induced Toxicity in Cortical Neuronal and Astrocytic Primary Cultures from Wild-Type and 3xTg-AD Mice. J. Alzheimers Dis. 2015, 46, 407–421. [Google Scholar] [CrossRef]
- Di Paola, R.; Impellizzeri, D.; Fusco, R.; Cordaro, M.; Siracusa, R.; Crupi, R.; Esposito, E.; Cuzzocrea, S. Ultramicronized Palmitoylethanolamide (PEA-Um®) in the Treatment of Idiopathic Pulmonary Fibrosis. Pharmacol. Res. 2016, 111, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Petrosino, S.; Schiano Moriello, A.; Cerrato, S.; Fusco, M.; Puigdemont, A.; De Petrocellis, L.; Di Marzo, V. The Anti-Inflammatory Mediator Palmitoylethanolamide Enhances the Levels of 2-Arachidonoyl-Glycerol and Potentiates Its Actions at TRPV1 Cation Channels: Novel Palmitoylethanolamide ‘Entourage Effects’. Br. J. Pharmacol. 2016, 173, 1154–1162. [Google Scholar] [CrossRef] [Green Version]
- Ueda, N. Endocannabinoid hydrolases. Prostaglandins Other Lipid Mediat. 2002, 68, 521–534. [Google Scholar] [CrossRef] [PubMed]
- Paladini, A.; Fusco, M.; Cenacchi, T.; Schievano, C.; Piroli, A.; Varrassi, G. Palmitoylethanolamide, a Special Food for Medical Purposes, in the Treatment of Chronic Pain: A Pooled Data Meta-Analysis. Pain. Physician 2016, 19, 11–24. [Google Scholar] [PubMed]
- Bacci, C.; Cassetta, G.; Emanuele, B.; Berengo, M. Randomized split-mouth study on postoperative effects of palmitoylethanolamide for impacted lower third molar surgery. ISRN Surg. 2011, 2011, 917350. [Google Scholar] [CrossRef] [Green Version]
- Chiurchiù, V.; Scipioni, L.; Arosio, B.; Mari, D.; Oddi, S.; Maccarrone, M. Anti-Inflammatory Effects of Fatty Acid Amide Hydrolase Inhibition in Monocytes/Macrophages from Alzheimer’s Disease Patients. Biomolecules 2021, 11, 502. [Google Scholar] [CrossRef]
- Petersen, R.C.; Smith, G.E.; Waring, S.C.; Ivnik, R.J.; Tangalos, E.G.; Kokmen, E. Mild Cognitive Impairment: Clinical Characterization and Outcome. Arch. Neurol. 1999, 56, 303. [Google Scholar] [CrossRef]
- Winblad, B.; Palmer, K.; Kivipelto, M.; Jelic, V.; Fratiglioni, L.; Wahlund, L.-O.; Nordberg, A.; Backman, L.; Albert, M.; Almkvist, O.; et al. Mild Cognitive Impairment—Beyond Controversies, towards a Consensus: Report of the International Working Group on Mild Cognitive Impairment. J. Intern. Med. 2004, 256, 240–246. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Magni, E.; Binetti, G.; Bianchetti, A.; Rozzini, R.; Trabucchi, M. Mini-Mental State Examination: A normative study in Italian elderly population. Eur. J. Neurol. 1996, 3, 198–202. [Google Scholar] [CrossRef]
- Morris, J.C. Clinical dementia rating: A reliable and valid diagnostic and staging measure for dementia of the Alzheimer type. Int. Psychogeriatr. 1997, 9, 173–176. [Google Scholar] [CrossRef] [PubMed]
- Randolph, C.; Tierney, M.C.; Mohr, E.; Chase, T.N. The Repeatable Battery for the Assessment of Neuropsychological Status (RBANS): Preliminary Clinical Validity. J. Clin. Exp. Neuropsychol. 1998, 20, 310–319. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Montero-Odasso, M.; Oteng-Amoako, A.; Speechley, M.; Gopaul, K.; Beauchet, O.; Annweiler, C.; Muir-Hunter, S.W. The Motor Signature of Mild Cognitive Impairment: Results from the Gait and Brain Study. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 1415–1421. [Google Scholar] [CrossRef]
- Kim, J.; Basak, J.M.; Holtzman, D.M. The role of apolipoprotein E in Alzheimer’s disease. Neuron 2009, 63, 287–303. [Google Scholar] [CrossRef] [Green Version]
- Valero, S.; Marquié, M.; De Rojas, I.; Espinosa, A.; Moreno-Grau, S.; Orellana, A.; Montrreal, L.; Hernández, I.; Mauleón, A.; Rosende-Roca, M.; et al. Interaction of neuropsychiatric symptoms with APOE ε4 and conversion to dementia in MCI patients in a Memory Clinic. Sci. Rep. 2021, 11, 4762. [Google Scholar] [CrossRef]
- Oddi, S.; Latini, L.; Viscomi, M.T.; Bisicchia, E.; Molinari, M.; Maccarrone, M. Distinct Regulation of NNOS and INOS by CB2 Receptor in Remote Delayed Neurodegeneration. J. Mol. Med. 2012, 90, 371–387. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Mattsson, N.; Andreasson, U.; Zetterberg, H.; Blennow, K. Association of Plasma Neurofilament Light with Neurodegeneration in Patients with Alzheimer Disease. JAMA Neurol. 2017, 74, 557. [Google Scholar] [CrossRef]


{kind=link}
| Inclusion Criteria | |
|---|---|
| Diagnosis (for MCI group) | MMSE score 23–26.9 points; CDR scale score <0.5 points |
| Age | 60–89 years |
| Cognitive status | Possess the capacity for making decisions |
| Language | Be able to read and write in Italian |
| Other conditions (for MCI group) | Have a reference person (namely, informant) |
| Exclusion criteria | |
| Pathologies | Current significant neurological disease (e.g., diagnosis of dementia, traumatic brain injury, etc.) |
| Motor limitations | Severe physical comorbidity |
| Medications | Cognitive enhancer medication |
| Other conditions | Current history of alcoholism and/or substance abuse |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bossa, M.; Argento, O.; Piacentini, C.; Manocchio, N.; Scipioni, L.; Oddi, S.; Maccarrone, M.; Nocentini, U. Effects of Long-Term Oral Administration of N-Palmitoylethanolamine in Subjects with Mild Cognitive Impairment: Study Protocol. Brain Sci. 2023, 13, 1138. https://doi.org/10.3390/brainsci13081138
Bossa M, Argento O, Piacentini C, Manocchio N, Scipioni L, Oddi S, Maccarrone M, Nocentini U. Effects of Long-Term Oral Administration of N-Palmitoylethanolamine in Subjects with Mild Cognitive Impairment: Study Protocol. Brain Sciences. 2023; 13(8):1138. https://doi.org/10.3390/brainsci13081138
Chicago/Turabian StyleBossa, Michela, Ornella Argento, Chiara Piacentini, Nicola Manocchio, Lucia Scipioni, Sergio Oddi, Mauro Maccarrone, and Ugo Nocentini. 2023. "Effects of Long-Term Oral Administration of N-Palmitoylethanolamine in Subjects with Mild Cognitive Impairment: Study Protocol" Brain Sciences 13, no. 8: 1138. https://doi.org/10.3390/brainsci13081138