

The Relationship between Paresthesia and the Presence of Cardiac Dysautonomia in Patients with Post-COVID-19 Syndrome: A Preliminary Observational Study


 ,
,
Abstract
:1. Introduction
2. Subjects and Methods
2.1. Place of Study and Participants
2.2. Autonomic Tests
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bellavia, S.; Scala, I.; Luigetti, M.; Brunetti, V.; Gabrielli, M.; Verme, L.Z.D.; Servidei, S.; Calabresi, P.; Frisullo, G.; Della Marca, G. Instrumental Evaluation of COVID-19 Related Dysautonomia in Non-Critically-Ill Patients: An Observational, Cross-Sectional Study. J. Clin. Med. 2021, 10, 5861. [Google Scholar] [CrossRef] [PubMed]
- Kaliyaperumal, D.; Rk, K.; Alagesan, M.; Ramalingam, S. Characterization of cardiac autonomic function in COVID-19 using heart rate variability: A hospital based preliminary observational study. J. Basic Clin. Physiol. Pharmacol. 2021, 32, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini, L.; Albecka, A.; Mallery, D.L.; Kellner, M.J.; Paul, D.; Carter, A.P.; James, L.C.; Lancaster, M.A. SARS-CoV-2 Infects the Brain Choroid Plexus and Disrupts the Blood-CSF Barrier in Human Brain Organoids. Cell Stem Cell 2020, 27, 951–961.e5. [Google Scholar] [CrossRef] [PubMed]
- Keyhanian, K.; Umeton, R.P.; Mohit, B.; Davoudi, V.; Hajighasemi, F.; Ghasemi, M. SARS-CoV-2 and nervous system: From pathogenesis to clinical manifestation. J. Neuroimmunol. 2021, 350, 577436. [Google Scholar] [CrossRef] [PubMed]
- Lanza, G.A. Autonomic dysfunction and post-COVID-19 syndrome: A still elusive link. Heart Rhythm 2022, 19, 621–622. [Google Scholar] [CrossRef] [PubMed]
- Dani, M.; Dirksen, A.; Taraborrelli, P.; Torocastro, M.; Panagopoulos, D.; Sutton, R.; Lim, P.B. Autonomic dysfunction in ‘long COVID’: Rationale, physiology and management strategies. Clin. Med. 2021, 21, e63–e67. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.; Yu, Z.; Yuan, Y.; Han, J.; Wang, Z.; Chen, H.; Wang, S.; Wang, Z.; Hu, H.; Zhou, L.; et al. Alteration of Autonomic Nervous System Is Associated With Severity and Outcomes in Patients with COVID-19. Front. Physiol. 2021, 12, 630038. [Google Scholar] [CrossRef] [PubMed]
- Becker, R.C. Autonomic dysfunction in SARS-CoV-2 infection acute and long-term implications COVID-19 editor’s page series. J. Thromb. Thrombolysis 2021, 52, 692–707. [Google Scholar] [CrossRef] [PubMed]
- Hinduja, A.; Moutairou, A.; Calvet, J.-H. Sudomotor dysfunction in patients recovered from COVID-19. Neurophysiol. Clin. 2021, 51, 193–196. [Google Scholar] [CrossRef] [PubMed]
- Shah, B.; Kunal, S.; Bansal, A.; Jain, J.; Poundrik, S.; Shetty, M.K.; Batra, V.; Chaturvedi, V.; Yusuf, J.; Mukhopadhyay, S.; et al. Heart rate variability as a marker of cardiovascular dysautonomia in post-COVID-19 syndrome using artificial intelligence. Indian Pacing Electrophysiol. J. 2022, 22, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Wirth, K.J.; Löhn, M. Orthostatic Intolerance after COVID-19 Infection: Is Disturbed Microcirculation of the Vasa Vasorum of Capacitance Vessels the Primary Defect? Medicina 2022, 58, 1807. [Google Scholar] [CrossRef] [PubMed]
- Soliński, M.; Pawlak, A.; Petelczyc, M.; Buchner, T.; Aftyka, J.; Gil, R.; Król, Z.; Żebrowski, J. Heart Rate Variability Changes in Mild-Symptomatic, Physically Fit Male in 4–6 Weeks from the End of SARS-CoV-2 Infection. 2021. Available online: https://www.researchsquare.com/article/rs-909431/v1 (accessed on 23 April 2023).
- Kurtoğlu, E.; Afsin, A.; Aktaş, İ.; Aktürk, E.; Kutlusoy, E.; Çağaşar, Ö. Altered cardiac autonomic function after recovery from COVID-19. Ann. Noninvasive Electrocardiol. 2021, 27, e12916. [Google Scholar] [CrossRef] [PubMed]
- Asarcikli, L.D.; Hayiroglu, M.İ.; Osken, A.; Keskin, K.; Kolak, Z.; Aksu, T. Heart rate variability and cardiac autonomic functions in post-COVID period. J. Interv. Card. Electrophysiol. 2022, 63, 715–721. [Google Scholar] [CrossRef] [PubMed]
- Townsend, L.; Moloney, D.; Finucane, C.; McCarthy, K.; Bergin, C.; Bannan, C.; Kenny, R.-A. Fatigue following COVID-19 infection is not associated with autonomic dysfunction. PLoS ONE 2021, 16, e0247280. [Google Scholar] [CrossRef] [PubMed]
- Azabou, E.; Bao, G.; Bounab, R.; Heming, N.; Annane, D. Vagus Nerve Stimulation: A Potential Adjunct Therapy for COVID-19. Front. Med. 2021, 8, 625836. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical Power Analyses Using G*Power 3.1: Tests for Correlation and Regression Analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Machado García, A. Optimización de los Métodos para Estudiar la Variabilidad de la Frecuencia Cardiaca y su Aplicación a Grupos de Sujetos Sanos y Enfermos [Internet]. [Cuba]: Repositorio de Tesis en Ciencias Biomédicas y de la Salud de Cuba. 2008. Available online: http://tesis.sld.cu/index.php?P=FullRecord&ID=539 (accessed on 23 April 2023).
- Lewek, J.; Jatczak-Pawlik, I.; Maciejewski, M.; Jankowski, P.; Banach, M. COVID-19 and cardiovascular complications—Preliminary results of the LATE-COVID study. Arch. Med. Sci. 2021, 17, 818–822. [Google Scholar] [CrossRef] [PubMed]
- Bourdillon, N.; Yazdani, S.; Schmitt, L.; Millet, G.P. Effects of COVID-19 lockdown on heart rate variability. PLoS ONE 2020, 15, e0242303. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | COVID+ (n = 29) | COVID− (n = 15) | Statistic |
|---|---|---|---|
| Gender, female, n (%) | 23 (79.31) | 7 (46.66) | χ2 = 4.856 p = 0.028 |
| (±SD) | (±SD) | ||
| Age | 45.21 (±12.1) | 44.80 (±8.7) | t = 0.693 p = 0.492 |
| BMI | 25.75 (±5.0) | 25.94 (±3.5) | t = −0.123 p = 0.902 |
| HR | 70.14 (±10.9) | 68.66 (±6.5) | t = 0.477 p = 0.635 |
| SBP | 120.77 (±17.6) | 124.60(±22.3) | t = −0.610 p = 0.544 |
| DBP | 78.70 (±8.9) | 82.46 (±15.5) | t = −0.999 p = 0.323 |
| MBP | 92.72 (10.73) | 96.50 (17.50705) | t = −0.870 p = 0.389 |
| Active stand SBP | 131.48 (±18.9) | 143.33 (±23.5) | t = −1.783 p = 0.082 |
| Active stand DBP | 90.74 (±13.7) | 98.33 (±17.07) | t = −1.570 p = 0.124 |
| Active stand MBP | 104.31(±14.6) | 113.28 (±18.5) | t = −1.725 p = 0.092 |
| SDNN | 45.96 (±27.4) | 44.73 (±17.8) | t = 0.155 p = 0.877 |
| CV | 5.08 (±2.4) | 5.01 (±1.7) | t = 0.104 p = 0.917 |
| RMSSD | 39.57 (±35.4) | 37.55 (±24.4) | t = 0.195 p = 0.845 |
| log LF | −1.756 (±0.51) | −1.535 (±0.35) | t = −1.476 p = 0.147 |
| log HF | −1.801 (±0.52) | −1.602 (±0.36) | t = −1.302 p = 0.200 |
| LF/HF | 1.6554 (±1.439) | 1.2572 (±0.811) | t = 0.984 p = 0.330 |
| HRV (deep breathing) | 26.851 (±11.9) | 26.200 (±7.7) | t = 0.190 p = 0.850 |
| EI | 1.3155 (±0.1) | 1.3466 (±0.1) | t = −0.687 p = 0.495 |
| VI | 1.6707 (±0.4) | 1.5433 (±0.2) | t = 0.912 p = 0.366 |
| Active stand HR | 1.2646 (±0.5) | 1.2673 (±0.1) | t = −0.020 p = 0.984 |
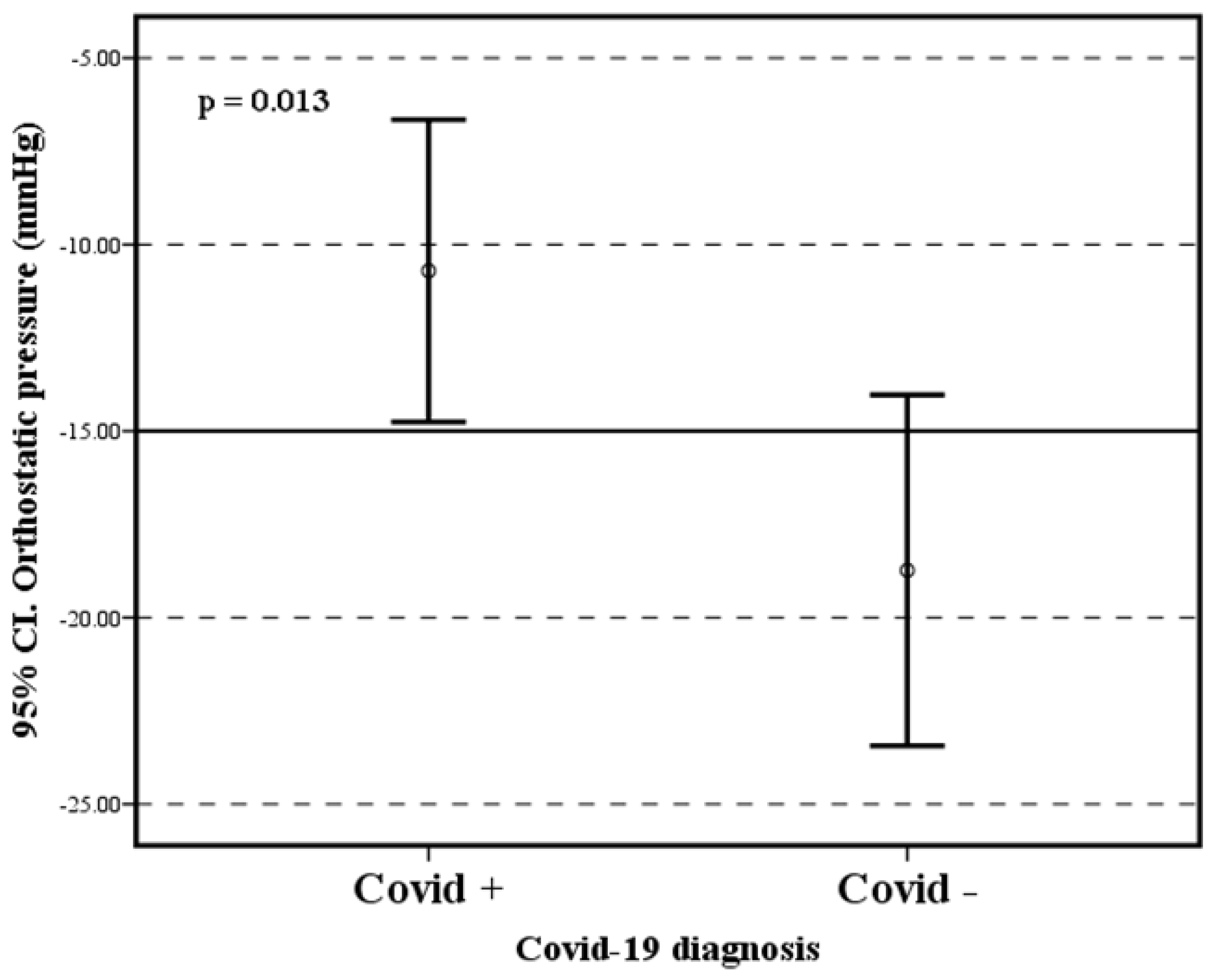
| Active stand SBP | −10.703 (±10.2) | −18.733 (±8.4) | t = 6.655 p = 0.013 |
| Variables | Paresthesia | Statistic | |
|---|---|---|---|
| Yes (n = 17) | No (n = 12) | ||
| Gender, female, n (%) | 14 (87.5) | 9 (81.8) | χ2 = 2.32 p = 0.630 |
| (±SD) | |||
| Age | 43.62 (±6.1) | 51.90 (±13.4) | t = −2.169 p = 0.039 |
| BMI | 26.10 (±5.5) | 25.25 (±4.4) | t = 0.423 p = 0.675 |
| log LF | −1.64 (±0.4) | −1.91 (±0.6) | t = 1.361 p = 0.185 |
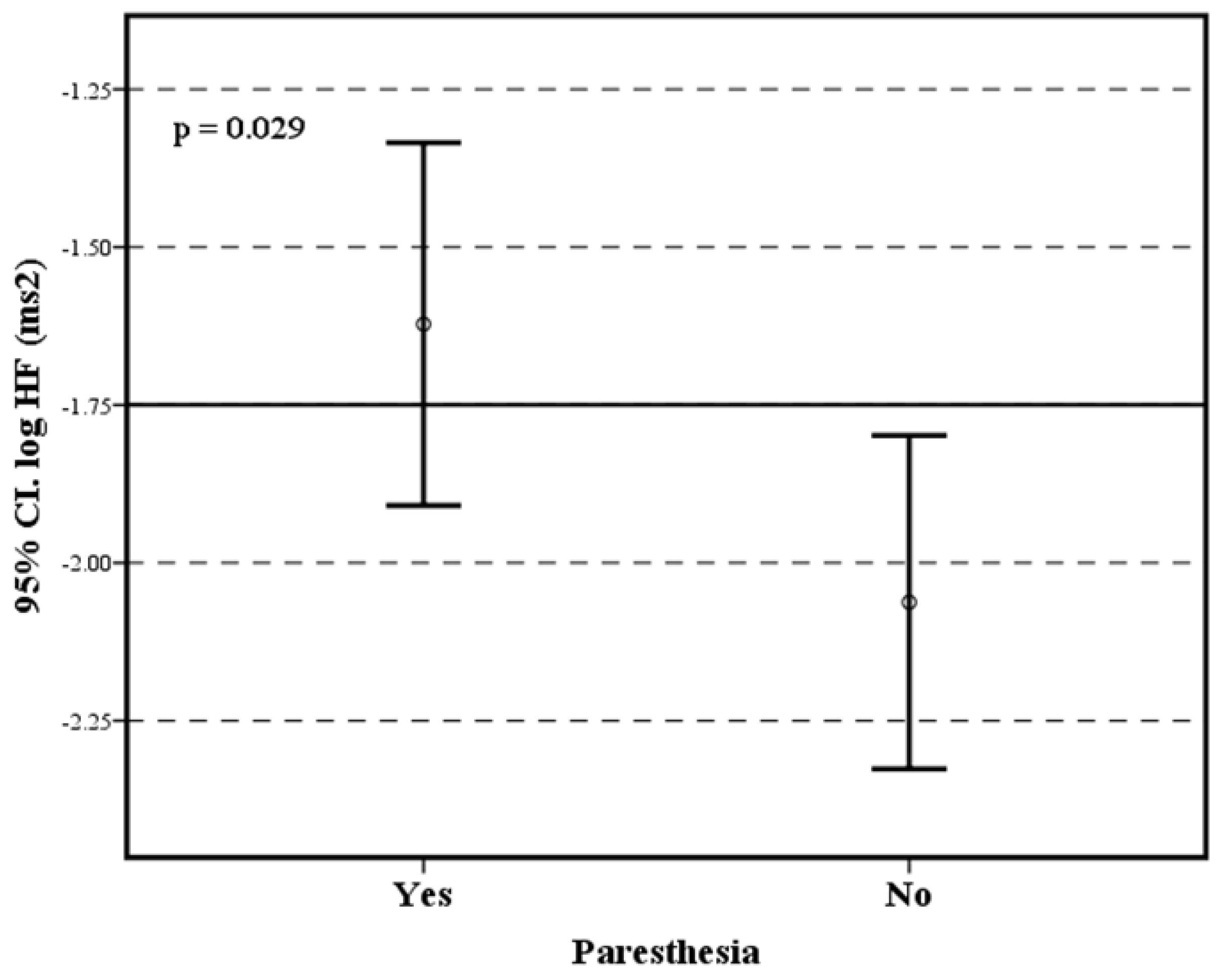
| log HF | −1.62 (±0.5) | −2.06 (±0.3) | t = 2.314 p = 0.029 |
| LF/HF | 1.22 (±0.9) | 2.28 (±1.8) | t = −1.978 p = 0.058 |
| Entropy | −4.92 (±0.6) | −4.58 (±0.7) | t = −1.270 p = 0.215 |
| HRV (deep breathing) | 28.93 (±10.8) | 23.81 (±13.3) | t = 1.101 p = 0.281 |
| EI | 1.34 (±0.1) | 1.27 (±0.1) | t = 1.176 p = 0.250 |
| VI | 1.73 (±0.5) | 1.57 (±0.3) | t = 0.809 p = 0.426 |
| HR | 71 (±11.0) | 68.90 (±11.2) | t = 0.480 p = 0.634 |
| SBP | 120 (16.5) | 120 (30) | z = −0.101 p = 0.919 |
| DBP | 80 (20) | 80 (8.7) | z = −0.167 p = 0.867 |
| Medians (IQR) | |||
| MBP | 93.33 (10.4) | 93.33 (10) | z = −0.100 p = 0.919 |
| SDNN | 43.50 (36.7) | 29.00 (25) | z = −1.308 p = 0.190 |
| CV | 5.05 (5.2) | 3.50 (3.1) | z = −1.777 p = 0.075 |
| RMSSD | 31.64 (53.7) | 22.63 (18.8) | z = −1.233 p = 0.217 |
| Active stand HR | 1.09 (0.2) | 1.10 (0.4) | z = −0.123 p = 0.901 |
| Active stand BP | −10.00 (13.7) | −10.00 (15.0) | z = −2.265 p = 0.178 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Galán, E.; Montoya-Pedrón, A.; Sánchez-Hechavarría, M.E.; Muñoz-Bustos, M.E.; Muñoz-Bustos, G.A. The Relationship between Paresthesia and the Presence of Cardiac Dysautonomia in Patients with Post-COVID-19 Syndrome: A Preliminary Observational Study. Brain Sci. 2023, 13, 1095. https://doi.org/10.3390/brainsci13071095
López-Galán E, Montoya-Pedrón A, Sánchez-Hechavarría ME, Muñoz-Bustos ME, Muñoz-Bustos GA. The Relationship between Paresthesia and the Presence of Cardiac Dysautonomia in Patients with Post-COVID-19 Syndrome: A Preliminary Observational Study. Brain Sciences. 2023; 13(7):1095. https://doi.org/10.3390/brainsci13071095
Chicago/Turabian StyleLópez-Galán, Erislandis, Arquímedes Montoya-Pedrón, Miguel Enrique Sánchez-Hechavarría, Mario Eugenio Muñoz-Bustos, and Gustavo Alejandro Muñoz-Bustos. 2023. "The Relationship between Paresthesia and the Presence of Cardiac Dysautonomia in Patients with Post-COVID-19 Syndrome: A Preliminary Observational Study" Brain Sciences 13, no. 7: 1095. https://doi.org/10.3390/brainsci13071095