

A Systematic Review of Pharmacological Interventions for Apathy in Aging Neurocognitive Disorders
 , ,
, ,
Abstract
:1. Introduction
1.1. Eligibility Criteria, Information Sources, and Search Strategy
1.2. Study Selection and Quality Evaluation
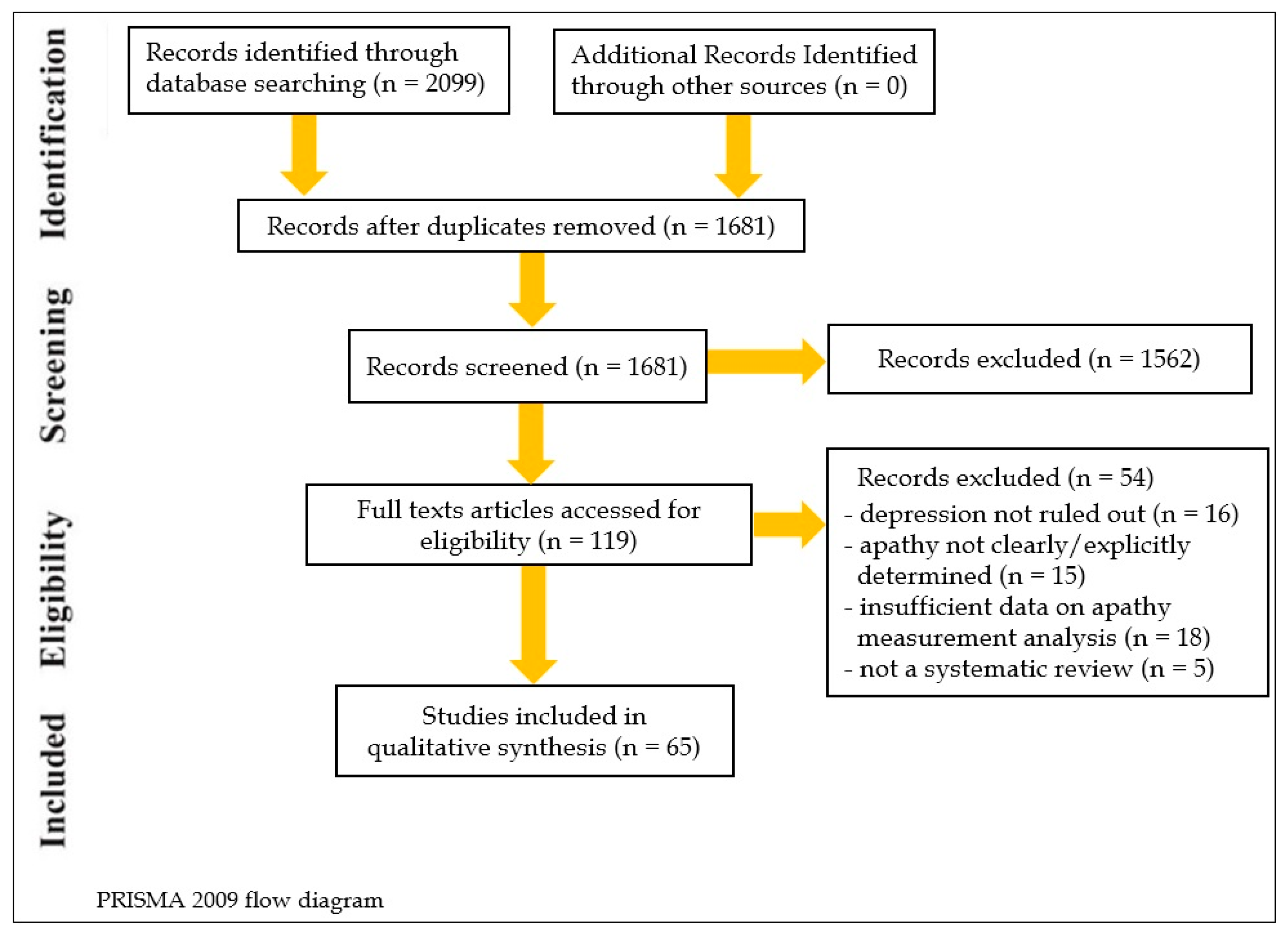
1.3. Search Results
1.4. Assessment of Apathy
2. Review of Pharmacological Treatments (Table 1)
2.1. Alzheimer’s Disease (AD)
2.1.1. Donepezil
2.1.2. Galantamine
2.1.3. Memantine
2.1.4. Ginkgo Biloba
2.1.5. Methylphenidate
2.1.6. Modafinil
2.1.7. Antidepressants
2.1.8. Atypical Antipsychotics
2.1.9. Pain Management
2.1.10. THC
2.1.11. BrainUp-10
2.2. Parkinson’s Disease (PD) and Dementia with Lewy Bodies (DLB)
2.2.1. Memantine
2.2.2. Amantadine
2.2.3. Rivastigmine
2.2.4. Rasagiline
2.2.5. Rotigotine
2.2.6. Atomoxetine
2.2.7. Methylphenidate
2.2.8. Piribedil
2.2.9. IRL752
2.2.10. Safinamide

{kind=link}
| Ref. | Compound/Apathy Measure | PEDro | PEDro | PEDro | PEDro | PEDro | PEDro | PEDro | PEDro | PEDro | PEDro | PEDro | PEDro | OCEBM |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Random Group Allocation | Allocation Concealed | Baseline Group Similarity | Blinding of All Subjects | Blinding of All Therapists | Blinding of All Assessors of At Least one Key Outcome | Less than 15% Dropouts | Intention to Treat Analysis of At Least One Key Outcome | Between-Group Statistical Comparisons Reported for At Least One Key Outcome | Point Measurements and Measurements of Variability Provided for At least One Key Outcome | Total Yes | Quality | |||
| Alzheimer’s Disease | ||||||||||||||
| Tariot et al. [35] | Donepezil/NPI | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | 9 | High | B |
| Feldman et al. [36] | Donepezil/NPI | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | 9 | High | B |
| Gauthier et al. [37] | Donepezil/NPI | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | 9 | High | B |
| Feldman et al. [38] | Donepezil/NPI | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | 9 | High | B |
| Holmes et al. [39] | Donepezil/NPI | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | 9 | High | B |
| Seltzer et al. [40] | Donepezil/AES | Y | N | N | Y | Y | Y | N | Y | N | N | 5 | Moderate | B |
| Cummings et al. [41] | Donepezil/NPI | Y | N | Y | Y | Y | Y | N | Y | Y | Y | 8 | High | B |
| Rea et al. [42] | Donepezil+choline alphoscerate/NPI | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | 9 | High | B |
| Tariot et al. [43] | Galantamine/NPI | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | 9 | High | B |
| Rockwood et al. [44] | Galantamine/NPI | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | 9 | High | B |
| Erkinjutti et al. [45] | Galantamine/NPI | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | 9 | High | B |
| Cummings et al. [46] | Galantamine/NPI | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | 9 | High | B |
| Winblad and Poritis [48] | Memantine/CGI-C | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | 9 | High | B |
| Cummings et al. [49] | Memantine/NPI | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | 9 | High | B |
| Scripnikov et al. [50] | Ginkgo Biloba/NPI | N | N | Y | Y | Y | Y | N | N | Y | Y | 7 | High | B |
| Bachinskaya et al. [51] | Ginkgo Biloba/NPI | Y | N | Y | Y | Y | Y | N | Y | Y | Y | 8 | High | B |
| Ihl et al. [52] | Ginkgo Biloba/NPI | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | 9 | High | B |
| Kaplitz et al. [53] | Methylphenydate/NOSIE | Y | N | N | Y | Y | Y | N | N | Y | Y | 6 | Moderate | C |
| Hermann et al. [54] | Methylphenydate/AES | Y | N | N | Y | Y | Y | N | N | Y | Y | 6 | Moderate | C |
| Rosenberg et al. [55] | Methylphenydate/AES, NPI | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 10 | High | A |
| Padala et al. [57] | Methylphenydate/AES-C | Y | Y | N | Y | Y | Y | Y | N | Y | Y | 8 | High | B |
| Frakey et al. [58] | Modafinil/FSBS | Y | N | Y | Y | Y | Y | Y | N | Y | Y | 8 | High | B |
| Zhou et al. [66] | Citalopram/NPI | Y | N | Y | Y | N | N | N | N | Y | Y | 5 | Moderate | B |
| Maier et al. [67] | Bupropion/AES-C | Y | N | Y | Y | Y | Y | N | Y | Y | Y | 8 | High | B |
| Nagata et al. [72] | Atypical antipsychotics/NPI | Y | N | Y | Y | N | N | Y | Y | Y | Y | 7 | High | B |
| Husebo et al. [74] | Pain treatment (paracetamol, morphine XR, buprenorphine or pregabaline)/NPI-NH | Y | Y | N | Y | Y | Y | N | N | Y | Y | 7 | High | B |
| van den Elsen et al. [75] | Tetrahydrocannabinol/NPI | Y | Y | Y | Y | Y | Y | Y | Y | N | N | 8 | High | B |
| Guzman-Martinez et al. [76] | BrainUp-10®/AES | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | 9 | High | B |
| Parkinson’s Disease | ||||||||||||||
| Emre et al. [77] | Memantine/NPI | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | 9 | High | B |
| Leroi et al. [78] | Memantine/NPI | Y | N | N | Y | Y | N | Y | N | Y | Y | 6 | Moderate | B |
| Ory-Magne et al. [79] | Amantadine/AI | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 10 | High | A |
| Devos et al. [81] | Rivastigmine/LARS | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 10 | High | A |
| Smith et al. [82] | Rasagiline/UPDRS | Y | N | Y | Y | Y | Y | N | N | Y | Y | 7 | High | B |
| Antonini et al. [83] | Rotigotine/NMSS | Υ | Ν | Υ | Υ | Υ | Υ | Ν | Υ | Υ | Υ | 8 | High | B |
| Castriotto et al. [84] | Rotigotine/LARS | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 10 | High | A |
| Chaudhuri et al. [85] | Rotigotine/NMSS | Y | N | Y | Y | Y | Y | Y | N | Y | Y | 8 | High | B |
| Hauser et al. [86] | Rotigotine/UPDRS | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | 9 | High | B |
| Chung et al. [87] | Rotigotine/AES | Y | N | Y | Y | Y | Y | N | Y | Y | Y | 8 | High | B |
| Weintraub et al. [88] | Atomoxetine/AES | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | 9 | High | B |
| Moreau et al. [89] | Methylphenydate/UPDRS, LARS | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 10 | High | A |
| Thobois et al. [90] | Piribedil/AES | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 10 | High | A |
| Sveningson et al. [91] | IRL752/UPDRS, NPI | Y | N | N | Y | Y | Y | Y | Y | Y | Y | 8 | High | B |
| Hattori et al. [94] | Safinamide/UPDRS | Y | N | Y | Y | Y | Y | Y | N | Y | Y | 8 | High | B |
| Kulisevsky et al. [92] | Safinamide/NPI, AES | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | 9 | High | B |
| Dementia with Lewy Bodies | ||||||||||||||
| McKeith et al. [80] | Rivastigmine/NPI | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | 9 | High | B |
| Frontotemporal Dementia | ||||||||||||||
| Jesso et al. [95] | Oxytocin/NPI | Υ | N | N | Υ | Υ | Υ | Y | N | Y | Y | 7 | High | B |
| Finger et al. [96] | Oxytocin/NPI, FBI | Y | N | Y | Y | Y | Y | Y | N | Y | Y | 8 | High | B |
| Huey et al. [97] | Dextroamphetamine vs. Quetiapine/NPI | Y | N | Y | Y | Y | Y | Y | N | Y | N | 7 | High | B |
| Callegari et al. [98] | Melatonin/AES-C, NPI | Y | N | Y | Y | Y | Y | Y | N | Y | Y | 9 | High | B |
| Huntington’s Disease | ||||||||||||||
| Gelderblom et al. [99] | Bupropion/AES, NPI, UPDRS | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 10 | High | A |
2.3. Frontotemporal Dementia (FTD)
2.3.1. Oxytocin
2.3.2. Dextroamphetamine
2.3.3. Agomelatine
2.4. Huntington’s Disease
Bupropion
3. Discussion
3.1. Principal Findings
3.2. Strengths and Weaknesses
3.2.1. Appraisal of Methodological Quality of the Review
3.2.2. Preceding Pharmacological Reviews
3.3. General Implications for Future Research
3.4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Winblad, B.; Engedal, K.; Soininen, H.; Verhey, F.; Waldemar, G.; Wimo, A.; Wetterholm, A.-L.; Zhang, R.; Haglund, A.; Subbiah, P.; et al. A 1-year, randomized, placebo-controlled study of donepezil in patients with mild to moderate AD. Neurology 2001, 57, 489–495. [Google Scholar] [CrossRef]
- Cummings, J.L.; Diaz, C.; Levy, M.; Binetti, G.; Litvan, I.I. Behavioral syndromes in Neurodegenerative Diseases: Frequency and Significance. Semin. Clin. Neuropsychiatry 1996, 1, 241–247. [Google Scholar]
- Mega, M.S.; Cummings, J.L.; Fiorello, T.; Gornbein, J. The spectrum of behavioral changes in Alzheimer’s disease. Neurology 1996, 46, 130–135. [Google Scholar] [CrossRef]
- Lyketsos, C.G.; Steinberg, M.; Tschanz, J.T.; Norton, M.C.; Steffens, D.C.; Breitner, J.C. Mental and Behavioral Disturbances in Dementia: Findings From the Cache County Study on Memory in Aging. Am. J. Psychiatry 2000, 157, 708–714. [Google Scholar] [CrossRef]
- Lyketsos, C.G.; Carrillo, M.C.; Ryan, J.M.; Khachaturian, A.S.; Trzepacz, P.; Amatniek, J.; Cedarbaum, J.; Brashear, R.; Miller, D.S. Neuropsychiatric symptoms in Alzheimer’s disease. Alzheimers Dement. 2011, 7, 532–539. [Google Scholar] [CrossRef] [Green Version]
- Cummings, J.L. The Neuropsychiatric Inventory: Assessing psychopathology in dementia patients. Neurology 1997, 48 (Suppl. S6), S10–S16. [Google Scholar] [CrossRef] [Green Version]
- Marin, R.S. Differential diagnosis and classification of apathy. Am. J. Psychiatry 1990, 147, 22–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levy, R.; Dubois, B. Apathy and the Functional Anatomy of the Prefrontal Cortex–Basal Ganglia Circuits. Cereb. Cortex 2006, 16, 916–928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyketsos, C.G.; Rosenblatt, A.; Rabins, P. Forgotten frontal lobe syndrome or “Executive Dysfunction Syndrome”. Psychosomatics 2004, 45, 247–255. [Google Scholar] [CrossRef]
- Theleritis, C.; Politis, A.; Siarkos, K.; Lyketsos, C.G. A review of neuroimaging findings of apathy in Alzheimer’s disease. Int. Psychogeriatr. 2014, 26, 195–207. [Google Scholar] [CrossRef] [Green Version]
- Le Heron, C.; Apps, M.; Husain, M. The anatomy of apathy: A neurocognitive framework for amotivated behaviour. Neuropsychologia 2018, 118 Pt B, 54–67. [Google Scholar] [CrossRef]
- Starkstein, S.E.; Petracca, G.; Chemerinski, E.; Kremer, J. Syndromic Validity of Apathy in Alzheimer’s Disease. Am. J. Psychiatry 2001, 158, 872–877. [Google Scholar] [CrossRef] [PubMed]
- Robert, P.; Lanctôt, K.; Agüera-Ortiz, L.; Aalten, P.; Bremond, F.; DeFrancesco, M.; Hanon, C.; David, R.; Dubois, B.; Dujardin, K.; et al. Is it time to revise the diagnostic criteria for apathy in brain disorders? The 2018 international consensus group. Eur. Psychiatry 2018, 54, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Mulin, E.; Leone, E.; Dujardin, K.; Delliaux, M.; Leentjens, A.; Nobili, F.; Dessi, B.; Tible, O.; Agüera-Ortiz, L.; Osorio, R.S.; et al. Diagnostic criteria for apathy in clinical practice. Int. J. Geriatr. Psychiatry 2011, 26, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Miller, D.S.; Robert, P.; Ereshefsky, L.; Adler, L.; Bateman, D.; Cummings, J.; DeKosky, S.T.; Fischer, C.E.; Husain, M.; Ismail, Z.; et al. Diagnostic criteria for apathy in neurocognitive disorders. Alzheimers Dement. 2021, 17, 1892–1904. [Google Scholar] [CrossRef]
- Drijgers, R.L.; Verhey, F.R.J.; Leentjens, A.F.G.; Köhler, S.; Aalten, P. Neuropsychological correlates of apathy in mild cognitive impairment and Alzheimer’s disease: The role of executive functioning. Int. Psychogeriatr. 2011, 23, 1327–1333. [Google Scholar] [CrossRef]
- Onyike, C.U.; Sheppard, J.-M.E.; Tschanz, J.T.; Norton, M.C.; Green, R.C.; Steinberg, M.; Welsh-Bohmer, K.A.; Breitner, J.C.; Lyketsos, C.G. Epidemiology of Apathy in Older Adults: The Cache County Study. Am. J. Geriatr. Psychiatry 2007, 15, 365–375. [Google Scholar] [CrossRef]
- Ma, A.M.L.; Ma, S.D.S.; Strauss, M.E.; Geldmacher, D.S. Apathy in Alzheimer’s Disease. J. Am. Geriatr. Soc. 2001, 49, 1700–1707. [Google Scholar] [CrossRef]
- Politis, A.M.; Mayer, L.S.; Passa, M.; Maillis, A.; Lyketsos, C.G. Validity and reliability of the newly translated Hellenic Neuropsychiatric Inventory(H-NPI) applied to Greek outpatients with Alzheimer’s disease: A study of disturbing behaviors among referrals to a memory clinic. Int. J. Geriatr. Psychiatry 2004, 19, 203–208. [Google Scholar] [CrossRef]
- Ruthirakuhan, M.; Herrmann, N.; Vieira, D.; Gallagher, D.; Lanctôt, K.L. The Roles of Apathy and Depression in Predicting Alzheimer Disease: A Longitudinal Analysis in Older Adults With Mild Cognitive Impairment. Am. J. Geriatr. Psychiatry 2019, 27, 873–882. [Google Scholar] [CrossRef]
- Grossman, H.T.; Sano, M.; Aloysi, A.; Elder, G.A.; Neugroschl, J.; Schimming, C.; Soleimani, L.; Zhu, C.W. Prevalent, persistent, and impairing: Longitudinal course and impact of apathy in Alzheimer’s disease. Alzheimers Dement. 2022, 13, e12169. [Google Scholar] [CrossRef]
- Harrison, F.; Aerts, L.; Brodaty, H. Apathy in Dementia: Systematic Review of Recent Evidence on Pharmacological Treatments. Curr. Psychiatry Rep. 2016, 18, 103. [Google Scholar] [CrossRef] [PubMed]
- Spalletta, G.; Fagioli, S.; Caltagirone, C.; Piras, F. Brain microstructure of subclinical apathy phenomenology in healthy individuals. Hum. Brain Mapp. 2013, 12, 3193–3203. [Google Scholar] [CrossRef] [PubMed]
- Stuss, D.T.; van Reekum, R.; Murphy, K.J. Differentiation of states and causes of apathy. In The Neuropsychology of Emotion; Borod, J., Ed.; Oxford University Press: New York, NY, USA, 2000; pp. 340–363. [Google Scholar]
- Theleritis, C.; Siarkos, K.; Katirtzoglou, E.; Politis, A. Pharmacological and Nonpharmacological Treatment for Apathy in Alzheimer’s Disease. A systematic review across modalities. J. Geriatr. Psychiatry Neurol. 2017, 30, 26–49. [Google Scholar] [CrossRef] [PubMed]
- Theleritis, C.; Siarkos, K.; Politis, A.A.; Katirtzoglou, E.; Politis, A. A systematic review of non-pharmacological treatments for apathy in dementia. Int. J. Geriatr. Psychiatry 2018, 33, e177–e192. [Google Scholar] [CrossRef]
- Theleritis, C.G.; Siarkos, K.T.; Politis, A.M. Unmet Needs in Pharmacological Treatment of Apathy in Alzheimer’s Disease: A Systematic Review. Front. Pharmacol. 2019, 10, 1108. [Google Scholar] [CrossRef]
- Trifiró, G.; Sultana, J.; Spina, E. Are the Safety Profiles of Antipsychotic Drugs Used in Dementia the Same? An Updated Review of Observational Studies. Drug Saf. 2014, 37, 501–520. [Google Scholar] [CrossRef]
- Medicine OCfE-b. Levels of Evidence and Grades of Recommendation. Oxford Centre for Evidence-Based Medicine. University of Oxford. 2009. Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/oxford-centre-for-evidence-based-medicine-levels-of-evidence-march-2009 (accessed on 30 May 2021).
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro Scale for Rating Quality of Randomized Controlled Trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Lai, C.K. The merits and problems of Neuropsychiatric Inventory as an assessment tool in people with dementia and other neurological disorders. Clin. Interv. Aging. 2014, 9, 1051–1061. [Google Scholar] [CrossRef] [Green Version]
- Marin, R.S.; Biedrzycki, R.C.; Firinciogullari, S. Reliability and validity of the apathy evaluation scale. Psychiatry Res. 1991, 38, 143–162. [Google Scholar] [CrossRef]
- Starkstein, S.E.; Mayberg, H.S.; Preziosi, T.J.; Andrezejewski, P.; Leiguarda, R.; Robinson, R.G. Reliability, validity, and clinical correlates of apathy in Parkinson’s disease. J. Neuropsychiatry Clin. Neurosci. 1992, 2, 134–139. [Google Scholar] [CrossRef]
- Tariot, P.N.; Cummings, J.L.; Katz, I.R.; Mintzer, J.; Perdomo, C.A.; Schwam, E.M.; Whalen, E. A Randomized, Double-Blind, Placebo-Controlled Study of the Efficacy and Safety of Donepezil in Patients with Alzheimer’s Disease in the Nursing Home Setting. J. Am. Geriatr. Soc. 2001, 49, 1590–1599. [Google Scholar] [CrossRef] [PubMed]
- Feldman, H.; Gauthier, S.; Hecker, J.; Vellas, B.; Xu, Y.; Ieni, J.R.; Schwam, E.M.; The Donepezil MSAD Study Investigators Group. Efficacy and safety of donepezil in patients with more severe Alzheimer’s disease: A subgroup analysis from a randomized, placebo-controlled trial. Int. J. Geriatr. Psychiatry 2005, 20, 559–569. [Google Scholar] [CrossRef]
- The Donepezil MSAD Study Investigators Group; Gauthier, S.; Feldman, H.; Hecker, J.; Vellas, B.; Ames, D.; Subbiah, P.; Whalen, E.; Emir, B. Efficacy of Donepezil on Behavioral Symptoms in Patients With Moderate to Severe Alzheimer’s Disease. Int. Psychogeriatr. 2002, 14, 389–404. [Google Scholar] [CrossRef]
- Feldman, H.; Gauthier, S.; Hecker, J.; Vellas, B.; Subbiah, P.; Whalen, E.; Donepezil MSAD Study Investigators Group. A 24-week, randomized, double-blind study of donepezil in moderate to severe Alzheimer’s disease. Neurology 2001, 57, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Holmes, C.; Wilkinson, D.; Dean, C.; Vethanayagam, S.; Olivieri, S.; Langley, A.; Pandita-Gunawardena, N.D.; Hogg, F.; Clare, C.; Damms, J. The efficacy of donepezil in the treatment of neuropsychiatric symptoms in Alzheimer disease. Neurology 2004, 63, 214–219. [Google Scholar] [CrossRef]
- Seltzer, B.; Zolnouni, P.; Nuñez, M.; Goldman, R.; Kumar, D.; Ieni, J.; Richardson, S.; Donepezil “402” Study Group. Efficacy of Donepezil in Early-Stage Alzheimer Disease: A randomized placebo-controlled trial. Arch. Neurol. 2004, 61, 1852–1856. [Google Scholar] [CrossRef] [Green Version]
- Cummings, J.L.; McRae, T.; Zhang, R.; Donepezil-Sertraline Study Group. Effects of Donepezil on Neuropsychiatric Symptoms in Patients With Dementia and Severe Behavioral Disorders. Am. J. Geriatr. Psychiatry 2006, 14, 605–612. [Google Scholar] [CrossRef] [Green Version]
- Rea, R.; Carotenuto, A.; Traini, E.; Fasanaro, A.M.; Manzo, V.; Amenta, F. Apathy Treatment in Alzheimer’s Disease: Interim Results of the ASCOMALVA Trial. J. Alzheimers Dis. 2015, 48, 377–383. [Google Scholar] [CrossRef]
- Tariot, P.; Solomon, P.; Morris, J.; Kershaw, P.; Lilienfeld, S.; Ding, C.; The Galantamine USA-10 Study Group. A 5-month, randomized, placebo-controlled trial of galantamine in AD. Neurology 2000, 54, 2269–2276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rockwood, K.; Mintzer, J.; Truyen, L.; Wessel, T.; Wilkinson, D. Effects of a flexible galantamine dose in Alzheimer’s disease: A randomized, controlled trial. J. Neurol. Neurosurg. Psychiatry 2001, 71, 589–595. [Google Scholar] [CrossRef] [Green Version]
- Erkinjuntti, T.; Kurz, A.; Gauthier, S.; Bullock, R.; Lilienfeld, S.; Damaraju, C.V. Efficacy of galantamine in probable vascular dementia and Alzheimer’s disease combined with cerebrovascular disease: A randomised trial. Lancet 2002, 359, 1283–1290. [Google Scholar] [CrossRef]
- Cummings, J.L.; Schneider, L.; Tariot, P.N.; Kershaw, P.R.; Yuan, W. Reduction of Behavioral Disturbances and Caregiver Distress by Galantamine in Patients With Alzheimer’s Disease. Am. J. Psychiatry 2004, 161, 532–538. [Google Scholar] [CrossRef] [PubMed]
- Pantev, M.; Ritter, R.; Gortelmeyer, R. Clinical and behavioural eveluation in long-term care patients with mild to moderate dementia under memantine treatment. Z. Gerontopsychol. Psychiatr. 1993, 6, S103–S117. [Google Scholar]
- Winblad, B.; Poritis, N. Memantine in severe dementia: Results of the9M-best study (benefit and efficacy in severly demented patients during treatment with memantine). Int. J. Geriatr. Psychiatry 1999, 14, 135–146. [Google Scholar] [CrossRef]
- Cummings, J.L.; Schneider, E.; Tariot, P.N.; Graham, S.M.; The Memantine MEM-MD-02 Stu1dy Group. Behavioral effects of memantine in Alzheimer disease patients receiving donepezil treatment. Neurology 2006, 67, 57–63. [Google Scholar] [CrossRef]
- Scripnikov, A.; Khomenko, A.; Napryeyenko, O.; The GINDEM-NP Study Group. Effects of Ginkgo biloba Extract EGb 761® on neuropsychiatric symptoms of dementia: Findings from a randomised controlled trial. Wien. Med. Wochenschr. 2007, 157, 295–300. [Google Scholar] [CrossRef]
- Hoerr, R.; Bachinskaya, N.; Ihl, R. Alleviating neuropsychiatric symptoms in dementia: The effects of Ginkgo biloba extract EGb 761®. Findings from a randomized controlled trial. Neuropsychiatr. Dis. Treat. 2011, 7, 209–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ihl, R.; Bachinskaya, N.; Korczyn, A.D.; Vakhapova, V.; Tribanek, M.; Hoerr, R.; Napryeyenko, O.; GOTADAY Study Group. Efficacy and safety of a once-daily formulation of Ginkgo biloba extract EGb 761 in dementia with neuropsychiatric features: A randomized controlled trial. Int. J. Geriatr. Psychiatry 2011, 26, 1186–1194. [Google Scholar] [CrossRef]
- Kaplitz, S.E. Withdrawn, Apathetic Geriatric Patients Responsive to Methylphenidate. J. Am. Geriatr. Soc. 1975, 23, 271–276. [Google Scholar] [CrossRef]
- Herrmann, N.; Rothenburg, L.S.; Black, S.E.; Ryan, M.; Liu, B.A.; Busto, U.E.; Lanctôt, K.L. Methylphenidate for the Treatment of Apathy in Alzheimer Disease: Prediction of response using dextroamphetamine. J. Clin. Psychopharmacol. 2008, 28, 296–301. [Google Scholar] [CrossRef]
- Rosenberg, P.B.; Lanctôt, K.L.; Drye, L.T.; Herrmann, N.; Scherer, R.W.; Bachman, D.L.; Mintzer, J.E. ADMET Investigators. Safety and Efficacy of Methylphenidate for Apathy in Alzheimer’s Disease: A randomized, placebo-controlled trial. J. Clin. Psychiatry 2013, 74, 810–816. [Google Scholar] [CrossRef] [Green Version]
- Lanctôt, K.L.; Chau, S.A.; Herrmann, N.; Drye, L.T.; Rosenberg, P.B.; Scherer, R.W.; Black, S.E.; Vaidya, V.; Bachman, D.L.; Mintzer, J.E. Effect of methylphenidate on attention in apathetic AD patients in a randomized, placebo-controlled trial. Int. Psychogeriatr. 2013, 26, 239–246. [Google Scholar] [CrossRef]
- Padala, P.; Padala, K.P.; Lensing, S.Y.; Ramirez, D.; Monga, V.; Bopp, M.M.; Roberson, P.K.; Dennis, R.A.; Petty, F.; Sullivan, D.H.; et al. Methylphenidate for Apathy in Community-Dwelling Older Veterans With Mild Alzheimer’s Disease: A Double-Blind, Randomized, Placebo-Controlled Trial. Am. J. Psychiatry 2017, 175, 159–168. [Google Scholar] [CrossRef]
- Frakey, L.L.; Salloway, S.; Buelow, M.; Malloy, P. A Randomized, Double-Blind, Placebo-Controlled Trial of Modafinil for the Treatment of Apathy in Individuals With Mild-to-Moderate Alzheimer’s Disease. J. Clin. Psychiatry 2012, 73, 796–801. [Google Scholar] [CrossRef]
- Tariot, P.N.; Cohen, R.M.; Sunderland, T.; Newhouse, P.A.; Yount, D.; Mellow, A.M.; Weingartner, H.; Mueller, E.A.; Murphy, D.L. L-Deprenyl in Alzheimer’s Disease. Preliminary evidence for behavioral change with monoamine oxidase B inhibition. Arch. Gen. Psychiatry 1987, 44, 427–433. [Google Scholar] [CrossRef]
- Nyth, A.L.; Gottfries, C.G.; Lyby, K.; Smedegaard-Andersen, L.; Gylding-Sabroe, J.; Kristensen, M.; Refsum, H.-E.; Öfsti, E.; Eriksson, S.; Syversen, S. A controlled multicenter clinical study of citalopram and placebo in elderly depressed patients with and without concomitant dementia. Acta Psychiatr. Scand. 1992, 86, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Freedman, M.; Rewilak, D.; Xerri, T.; Cohen, S.; Gordon, A.S.; Shandling, M.; Logan, A.G. L-deprenyl in Alzheimer’s disease: Cognitive and behavioral effects. Neurology 1998, 50, 660–668. [Google Scholar] [CrossRef]
- Pollock, B.G.; Mulsant, B.H.; Rosen, J.; Sweet, R.A.; Mazumdar, S.; Bharucha, A.; Marin, R.; Jacob, N.J.; Huber, K.A.; Kastango, K.B.; et al. Comparison of Citalopram, Perphenazine, and Placebo for the Acute Treatment of Psychosis and Behavioral Disturbances in Hospitalized, Demented Patients. Am. J. Psychiatry 2002, 159, 460–465. [Google Scholar] [CrossRef]
- Lyketsos, C.G.; DelCampo, L.; Steinberg, M.; Miles, Q.; Steele, C.D.; Munro, C.; Baker, A.S.; Sheppard, J.-M.E.; Frangakis, C.; Brandt, J.; et al. Treating Depression in Alzheimer Disease: Efficacy and safety of sertraline therapy, and the benefits of depression reduction: The DIADS. Arch. Gen. Psychiatry 2003, 60, 737–746. [Google Scholar] [CrossRef]
- Siddique, H.; Hynan, L.S.; Weiner, M.F. Effect of a Serotonin Reuptake Inhibitor on Irritability, Apathy, and Psychotic Symptoms in Patients With Alzheimer’s Disease. J. Clin. Psychiatry 2009, 70, 915–918. [Google Scholar] [CrossRef]
- Porsteinsson, A.P.; Drye, L.T.; Pollock, B.G.; Devanand, D.P.; Frangakis, C.; Ismail, Z.; Marano, C.; Meinert, C.L.; Mintzer, J.E.; Munro, C.A.; et al. Effect of Citalopram on Agitation in Alzheimer’s Disease—The CitAD Randomized Controlled Trial. JAMA 2014, 311, 682–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, T.; Wang, J.; Xin, C.; Kong, L.; Wang, C. Effect of memantine combined with citalopram on cognition of BPSD and moderate Alzheimer’s disease: A clinical trial. Exp. Ther. Med. 2019, 17, 1625–1630. [Google Scholar] [CrossRef] [Green Version]
- Maier, F.; Spottke, A.; Bach, J.-P.; Bartels, C.; Buerger, K.; Dodel, R.; Fellgiebel, A.; Fliessbach, K.; Frölich, L.; Hausner, L.; et al. Bupropion for the Treatment of Apathy in Alzheimer Disease: A Randomized Clinical Trial. JAMA Netw. Open 2020, 5, e206027. [Google Scholar] [CrossRef]
- Oberholzer, A.F.; Hendriksen, C.; Monsch, A.U.; Heierli, B.; Stähelin, H.B. Safety and Effectiveness of Low-Dose Clozapine in Psychogeriatric Patients: A Preliminary Study. Int. Psychogeriatr. 1992, 4, 187–195. [Google Scholar] [CrossRef]
- Negrón, A.E.; Reichman, W.E. Risperidone in the Treatment of Patients With Alzheimer’s Disease With Negative Symptoms. Int. Psychogeriatr. 2000, 12, 527–536. [Google Scholar] [CrossRef] [PubMed]
- De Deyn, P.P.; Carrasco, M.M.; Deberdt, W.; Jeandel, C.; Hay, D.P.; Feldman, P.D.; Young, C.A.; Lehman, D.L.; Breier, A. Olanzapine versus placebo in the treatment of psychosis with or without associated behavioral disturbances in patients with Alzheimer’s disease. Int. J. Geriatr. Psychiatry 2004, 19, 115–126. [Google Scholar] [CrossRef]
- Onor, M.L.; Saina, M.; Trevisiol, M.; Cristante, T.; Aguglia, E. Clinical experience with risperidone in the treatment of behavioral and psychological symptoms of dementia. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2007, 31, 205–209. [Google Scholar] [CrossRef] [PubMed]
- Nagata, T.; Shinagawa, S.; Yoshida, K.; Noda, Y.; Shigeta, M.; Mimura, M.; Nakajima, S. Early Improvements of Individual Symptoms With Antipsychotics Predict Subsequent Treatment Response of Neuropsychiatric Symptoms in Alzheimer’s Disease: A re-analysis of the CATIE-AD Study. J. Clin. Psychiatry 2020, 81, 19m12961. [Google Scholar] [CrossRef] [Green Version]
- FDA. Deaths with Antipsychotics in Elderly Patients with Behavioral Disturbances; U.S. Food and Drug Administration; FDA Public Health Advisory; Centre for Drug Evaluation & Research, 2005. Available online: http://www.fda.gov/cder/drug/advisory/antipsychotics.htm (accessed on 26 April 2023).
- Husebo, B.S.; Ballard, C.; Fritze, F.; Sandvik, R.K.; Aarsland, D. Efficacy of pain treatment on mood syndrome in patients with dementia: A randomized clinical trial. Int. J. Geriatr. Psychiatry 2014, 29, 828–836. [Google Scholar] [CrossRef] [Green Version]
- Elsen, G.A.v.D.; Ahmed, A.I.; Verkes, R.-J.; Kramers, C.; Feuth, T.; Rosenberg, P.B.; van der Marck, M.A.; Rikkert, M.G.O. Tetrahydrocannabinol for neuropsychiatric symptoms in dementia: A randomized controlled trial. Neurology 2015, 84, 2338–2346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guzman-Martinez, L.; Farías, G.A.; Tapia, J.P.; Sánchez, M.P.; Fuentes, P.; Gloger, S.; Maccioni, R.B. Interventional Study to Evaluate the Clinical Effects and Safety of the Nutraceutical Compound BrainUp-10® in a Cohort of Patients with Alzheimer’s Disease: A Multicenter, Randomized, Double-Blind, and Placebo-Controlled Trial. J. Alzheimers Dis. 2021, 81, 1231–1241. [Google Scholar] [CrossRef]
- Emre, M.; Tsolaki, M.; Bonuccelli, U.; Destée, A.; Tolosa, E.; Kutzelnigg, A.; Ceballos-Baumann, A.; Zdravkovic, S.; Bladström, A.; Jones, R. Memantine for patients with Parkinson’s disease dementia or dementia with Lewy bodies: A randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2010, 9, 969–977. [Google Scholar] [CrossRef]
- Leroi, I.; Overshott, R.; Byrne, E.J.; Daniel, E.; Burns, A. Randomized controlled trial of memantine in dementia associated with Parkinson’s disease. Mov. Disord. 2009, 24, 1217–1221. [Google Scholar] [CrossRef]
- Ory-Magne, F.; Corvol, J.-C.; Azulay, J.-P.; Bonnet, A.-M.; Brefel-Courbon, C.; Damier, P.; Dellapina, E.; Destée, A.; Durif, F.; Galitzky, M.; et al. Withdrawing amantadine in dyskinetic patients with Parkinson disease: The AMANDYSK trial. Neurology 2014, 82, 300–307. [Google Scholar] [CrossRef]
- McKeith, I.; Del Ser, T.; Spano, P.; Emre, M.; Wesnes, K.; Anand, R.; Cicin-Sain, A.; Ferrara, R.; Spiegel, R. Efficacy of rivastigmine in dementia with Lewy bodies: A randomised, double-blind, placebo-controlled international study. Lancet 2000, 356, 2031–2036. [Google Scholar] [CrossRef]
- Devos, D.; Moreau, C.; Maltete, D.; Lefaucheur, R.; Kreisler, A.; Eusebio, A.; Defer, G.; Ouk, T.; Azulay, J.-P.; Krystkowiak, P.; et al. Rivastigmine in apathetic but dementia and depression-free patients with Parkinson’s disease: A double-blind, placebo-controlled, randomized clinical trial. J. Neurol. Neurosurg. Psychiatry 2014, 85, 668–674. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.M.; Eyal, E.; Weintraub, D.; ADAGIO Investigators. Combined Rasagiline and Antidepressant Use in Parkinson Disease in the ADAGIO Study: Effects on nonmotor symptoms and tolerability. JAMA Neurol. 2015, 72, 88–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antonini, A.; Bauer, L.; Dohin, E.; Oertel, W.H.; Rascol, O.; Reichmann, H.; Schmid, M.; Singh, P.; Tolosa, E.; Chaudhuri, K.R. Effects of rotigotine transdermal patch in patients with Parkinson’s disease presenting with non-motor symptoms—Results of a double-blind, randomized, placebo-controlled trial. Eur. J. Neurol. 2015, 22, 1400–1407. [Google Scholar] [CrossRef]
- Castrioto, A.; Thobois, S.; Anheim, M.; Quesada, J.L.; Lhommée, E.; Klinger, H.; Bichon, A.; Schmitt, E.; Durif, F.; Azulay, J.P.; et al. A randomized controlled double-blind study of rotigotine on neuropsychiatric symptoms in de novo PD. npj Park. Dis. 2020, 6, 41. [Google Scholar] [CrossRef]
- Chaudhuri, K.R.; Martinez-Martin, P.; Antonini, A.; Brown, R.G.; Friedman, J.H.; Onofrj, M.; Surmann, E.; Ghys, L.; Trenkwalder, C. Rotigotine and specific non-motor symptoms of Parkinson’s disease: Post hoc analysis of RECOVER. Park. Relat. Disord. 2013, 19, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Hauser, R.A.; Slawek, J.; Barone, P.; Dohin, E.; Surmann, E.; Asgharnejad, M.; Bauer, L. Evaluation of rotigotine transdermal patch for the treatment of apathy and motor symptoms in Parkinson’s disease. BMC Neurol. 2016, 16, 90. [Google Scholar] [CrossRef] [Green Version]
- Chung, S.J.; Asgharnejad, M.; Bauer, L.; Ramirez, F.; Jeon, B. Evaluation of rotigotine transdermal patch for the treatment of depressive symptoms in patients with Parkinson’s disease. Expert Opin. Pharmacother. 2016, 17, 1453–1461. [Google Scholar] [CrossRef]
- Weintraub, D.; Mavandadi, S.; Mamikonyan, E.; Siderowf, A.D.; Duda, J.E.; Hurtig, H.I.; Colcher, A.; Horn, S.S.; Nazem, S.; Have, T.R.T.; et al. Atomoxetine for depression and other neuropsychiatric symptoms in Parkinson disease. Neurology 2010, 75, 448–455. [Google Scholar] [CrossRef] [Green Version]
- Moreau, C.; Delval, A.; Defebvre, L.; Dujardin, K.; Duhamel, A.; Petyt, G.; Vuillaume, I.; Corvol, J.-C.; Brefel-Courbon, C.; Ory-Magne, F.; et al. Methylphenidate for gait hypokinesia and freezing in patients with Parkinson’s disease undergoing subthalamic stimulation: A multicentre, parallel, randomised, placebo-controlled trial. Lancet Neurol. 2012, 11, 589–596. [Google Scholar] [CrossRef] [PubMed]
- Thobois, S.; Lhommée, E.; Klinger, H.; Ardouin, C.; Schmitt, E.; Bichon, A.; Kistner, A.; Castrioto, A.; Xie, J.; Fraix, V.; et al. Parkinsonian apathy responds to dopaminergic stimulation of D2/D3 receptors with piribedil. Brain 2013, 136 Pt 5, 1568–1577. [Google Scholar] [CrossRef] [Green Version]
- Svenningsson, P.; Odin, P.; Dizdar, N.; Johansson, A.; Grigoriou, S.; Tsitsi, P.; Wictorin, K.; Bergquist, F.; Nyholm, D.; Rinne, J.; et al. A Phase 2a Trial Investigating the Safety and Tolerability of the Novel Cortical Enhancer IRL752 in Parkinson’s Disease Dementia. Mov. Disord. 2020, 35, 1046–1054. [Google Scholar] [CrossRef]
- Kulisevsky, J.; Martínez-Horta, S.; Campolongo, A.; Pascual-Sedano, B.; Marín-Lahoz, J.; Bejr-Kasem, H.; Aracil-Bolaños, I.; Horta-Barba, A.; Puig-Davi, A.; Pagonabarraga, J. A Randomized Clinical Trial to Evaluate the Effects of Safinamide on Apathetic Non-demented Patients With Parkinson’s Disease. Front. Neurol. 2022, 13, 866502. [Google Scholar] [CrossRef]
- Hattori, N.; Kogo, Y.; Koebis, M.; Ishida, T.; Suzuki, I.; Tsuboi, Y.; Nomoto, M. The Effects of Safinamide Adjunct Therapy on Depression and Apathy in Patients With Parkinson’s Disease: Post-hoc Analysis of a Japanese Phase 2/3 Study. Front. Neurol. 2022, 12, 752632. [Google Scholar] [CrossRef]
- Hattori, N.; Tsuboi, Y.; Yamamoto, A.; Sasagawa, Y.; Nomoto, M.; ME2125-3 Study Group. Efficacy and safety of safinamide as an add-on therapy to L-DOPA for patients with Parkinson’s disease: A randomized, double-blind, placebo-controlled, phase II/III study. Park. Relat. Disord. 2020, 75, 17–23. [Google Scholar] [CrossRef]
- Jesso, S.; Morlog, D.; Ross, S.; Pell, M.D.; Pasternak, S.H.; Mitchell, D.G.V.; Kertesz, A.; Finger, E.C. The effects of oxytocin on social cognition and behaviour in frontotemporal dementia. Brain 2011, 134 Pt 9, 2493–2501. [Google Scholar] [CrossRef] [Green Version]
- Finger, E.C.; MacKinley, J.; Blair, M.; Oliver, L.D.; Jesso, S.; Tartaglia, M.C.; Borrie, M.; Wells, J.; Dziobek, I.; Pasternak, S.; et al. Oxytocin for frontotemporal dementia: A randomized dose-finding study of safety and tolerability. Neurology 2015, 84, 174–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huey, E.D.; Garcia, C.; Wassermann, E.M.; Tierny, M.C.; Grafman, J.; Tierney, M.C. Stimulant Treatment of Frontotemporal Dementia in 8 Patients. J. Clin. Psychiatry 2008, 69, 1981–1982. [Google Scholar] [CrossRef] [Green Version]
- Callegari, I.; Mattei, C.; Benassi, F.; Krueger, F.; Grafman, J.; Yaldizli, Ö.; Sassos, D.; Massucco, D.; Scialò, C.; Nobili, F.; et al. Agomelatine Improves Apathy in Frontotemporal Dementia. Neurodegener. Dis. 2016, 16, 352–356. [Google Scholar] [CrossRef]
- Gelderblom, H.; Wüstenberg, T.; McLean, T.; Mütze, L.; Fischer, W.; Saft, C.; Hoffmann, R.; Süssmuth, S.; Schlattmann, P.; van Duijn, E.; et al. Bupropion for the treatment of apathy in Huntington’s disease: A multicenter, randomised, double-blind, placebo-controlled, prospective crossover trial. PLoS ONE 2017, 12, e0173872. [Google Scholar] [CrossRef] [Green Version]
- Mega, M.S.; Cummings, J.L.; Salloway, S.; Malloy, P. The limbic system: An anatomic, phylogenetic, and clinical perspective. J. Neuropsychiatry Clin. Neurosci. 1997, 9, 315–330. [Google Scholar] [CrossRef] [PubMed]
- Cummings, J.L.; Mackell, J.; Kaufer, D. Behavioral effects of current Alzheimer’s disease treatments: A descriptive review. Alzheimers Dement. 2008, 4, 49–60. [Google Scholar] [CrossRef]
- Matsuzono, K.; Yamashita, T.; Ohta, Y.; Hishikawa, N.; Sato, K.; Kono, S.; Deguchi, K.; Nakano, Y.; Abe, K. Clinical Benefits for Older Alzheimer’s Disease Patients: Okayama Late Dementia Study (OLDS). J. Alzheimers Dis. 2015, 46, 687–693. [Google Scholar] [CrossRef] [PubMed]
- Drijgers, R.L.; Aalten, P.; Winogrodzka, A.; Verhey, F.R.; Leentjens, A.F. Pharmacological Treatment of Apathy in Neurodegenerative Diseases: A Systematic Review. Dement. Geriatr. Cogn. Disord. 2009, 28, 13–22. [Google Scholar] [CrossRef]
- Berman, K.; Brodaty, H.; Withall, A.; Seeher, K. Pharmacologic Treatment of Apathy in Dementia. Am. J. Geriatr. Psychiatry 2012, 20, 104–122. [Google Scholar] [CrossRef]
- Azhar, L.; Kusumo, R.W.; Marotta, G.; Lanctôt, K.L.; Herrmann, N. Pharmacological Management of Apathy in Dementia. CNS Drugs 2022, 36, 143–165. [Google Scholar] [CrossRef] [PubMed]
- Waldemar, G.; Gauthier, S.; Jones, R.; Wilkinson, D.; Cummings, J.; Lopez, O.; Zhang, R.; Xu, Y.; Sun, Y.; Knox, S.; et al. Effect of donepezil on emergence of apathy in mild to moderate Alzheimer’s disease. Int. J. Geriatr. Psychiatry 2011, 26, 150–157. [Google Scholar] [CrossRef]
- Sherman, C.; Liu, C.S.; Herrmann, N.; Lanctôt, K.L. Prevalence, neurobiology, and treatments for apathy in prodromal dementia. Int. Psychogeriatr. 2018, 30, 177–184. [Google Scholar] [CrossRef]
- Ruthirakuhan, M.T.; Herrmann, N.; Abraham, E.H.; Chan, S.; Lanctôt, K.L. Pharmacological interventions for apathy in Alzheimer’s disease. Cochrane Database Syst. Rev. 2018, 5, CD012197. [Google Scholar] [CrossRef]
- Sepehry, A.A.; Sarai, M.; Hsiung, G.-Y.R. Pharmacological Therapy for Apathy in Alzheimer’s Disease: A Systematic Review and Meta-Analysis. Can. J. Neurol. Sci. 2017, 44, 267–275. [Google Scholar] [CrossRef] [Green Version]
- Rektorova, I. Current treatment of behavioral and cognitive symptoms of Parkinson’s disease. Park. Relat. Disord. 2019, 59, 65–73. [Google Scholar] [CrossRef] [Green Version]
- Mele, B.; Van, S.; Holroyd-Leduc, J.; Ismail, Z.; Pringsheim, T.; Goodarzi, Z. Diagnosis, treatment and management of apathy in Parkinson’s disease: A scoping review. BMJ Open 2020, 10, e037632. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.-T.; Wang, L.; He, Y.; Yu, G. Rotigotine transdermal patch for the treatment of neuropsychiatric symptoms in Parkinson’s disease: A meta-analysis of randomized placebo-controlled trials. J. Neurol. Sci. 2018, 393, 31–38. [Google Scholar] [CrossRef]
- Herrmann, N.; Rabheru, K.; Wang, J.; Binder, C. Galantamine Treatment of Problematic Behavior in Alzheimer’s Disease: Post-Hoc Analysis of Pooled Data From Three Large Trials. Am. J. Geriatr. Psychiatry 2005, 13, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Gauthier, S.; Wirth, Y.; Möbius, H.J. Effects of memantine on behavioural symptoms in Alzheimer’s disease patients: An analysis of the Neuropsychiatric Inventory (NPI) data of two randomised, controlled studies. Int. J. Geriatr. Psychiatry 2005, 20, 459–464. [Google Scholar] [CrossRef]
- Reisberg, B.; Doody, R.; Stöffler, A.; Schmitt, F.; Ferris, S.; Möbius, H.J.; Memantine Study Group. Memantine in Moderate-to-Severe Alzheimer’s Disease. N. Engl. J. Med. 2003, 348, 1333–1341. [Google Scholar] [CrossRef]
- Gauthier, S.; Loft, H.; Cummings, J. Improvement in behavioural symptoms in patients with moderate to severe Alzheimer’s disease by memantine: A pooled data analysis. Int. J. Geriatr. Psychiatry 2008, 23, 537–545. [Google Scholar] [CrossRef]
- Tariot, P.N.; Farlow, M.R.; Grossberg, G.T.; Graham, S.M.; McDonald, S.; Gergel, I.; The Memantine Study Group. Memantine Treatment in Patients With Moderate to Severe Alzheimer Disease Already Receiving Donepezil: A randomized controlled trial. JAMA 2004, 291, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Peskind, E.R.; Potkin, S.G.; Pomara, N.; Ott, B.R.; Graham, S.M.; Olin, J.T.; McDonald, S.; The Memantine MEM-MD-10 Study Group. Memantine Treatment in Mild to Moderate Alzheimer Disease: A 24-Week Randomized, Controlled Trial. Am. J. Geriatr. Psychiatry 2006, 14, 704–715. [Google Scholar] [CrossRef]
- van Dyck, C.H.; Tariot, P.N.; Meyers, B.; Resnick, E.M.; Memantine MEM-MD-01 Study Group. A 24-week Randomized, Controlled Trial of Memantine in Patients With Moderate-to-severe Alzheimer Disease. Alzheimer Dis. Assoc. Disord. 2007, 21, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Porsteinsson, A.P.; Grossberg, G.T.; Mintzer, J.; Olin, J.T.; Memantine MEM-MD-12 Study Group. Memantine treatment in patients with mild to moderate Alzheimer’s disease already receiving a cholinesterase inhibitor: A randomized, double-blind, placebo-controlled trial. Curr. Alzheimer Res. 2008, 5, 83–89. [Google Scholar] [CrossRef]
- Bakchine, S.; Loft, H. Memantine Treatment in Patients with Mild to Moderate Alzheimer’s Disease: Results of a Randomised, Double-Blind, Placebo-Controlled 6-Month Study. J. Alzheimers Dis. 2008, 13, 97–107. [Google Scholar] [CrossRef] [Green Version]
- Mintzer, J.; Lanctôt, K.L.; Scherer, R.W.; Rosenberg, P.B.; Herrmann, N.; van Dyck, C.H.; Padala, P.R.; Brawman-Mintzer, O.; Porsteinsson, A.P.; Lerner, A.J.; et al. Effect of Methylphenidate on Apathy in Patients With Alzheimer Disease: The ADMET 2 Randomized Clinical Trial. JAMA Neurol. 2021, 78, 1324–1332. [Google Scholar] [CrossRef]
- Radakovic, R.; Harley, C.; Abrahams, S.; Starr, J.M. A systematic review of the validity and reliability of apathy scales in neurodegenerative conditions. Int. Psychogeriatr. 2015, 27, 903–923. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clarke, D.E.; Ko, J.Y.; Kuhl, E.A.; van Reekum, R.; Salvador, R.; Marin, R.S. Are the available apathy measures reliable and valid? A review of the psychometric evidence. J. Psychosom. Res. 2011, 70, 73–97. [Google Scholar] [CrossRef] [Green Version]
- Sockeel, P.; Dujardin, K.; Devos, D.; Denève, C.; Destée, A.; Defebvre, L. The Lille apathy rating scale (LARS), a new instrument for detecting and quantifying apathy: Validation in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2006, 77, 579–584. [Google Scholar] [CrossRef] [Green Version]
- Cummings, J.; Friedman, J.H.; Garibaldi, G.; Jones, M.; MacFadden, W.; Marsh, L.; Robert, P.H. Apathy in Neurodegenerative Diseases: Recommendations on the Design of Clinical Trials. J. Geriatr. Psychiatry Neurol. 2015, 28, 159–173. [Google Scholar] [CrossRef] [PubMed]
- Mortby, M.E.; Adler, L.; Agüera-Ortiz, L.; Bateman, D.R.; Brodaty, H.; Cantillon, M.; Geda, Y.E.; Ismail, Z.; Lanctôt, K.L.; Marshall, G.A.; et al. Apathy as a Treatment Target in neurocognitive disorders of the Alzheimer’s type: Implications for Clinical Trials. Am. J. Geriatr. Psychiatry 2022, 30, 119–147. [Google Scholar] [CrossRef]
- Kales, H.C.; Gitlin, L.N.; Lyketsos, C.G.; Detroit Expert Panel on Assessment and Management of Neuropsychiatric Symptoms of Dementia. Management of Neuropsychiatric Symptoms of Dementia in Clinical Settings: Recommendations from a Multidisciplinary Expert Panel. J. Am. Geriatr. Soc. 2014, 62, 762–769. [Google Scholar] [CrossRef] [Green Version]
- Rosenberg, P.B.; Lyketsos, C. Mild cognitive impairment: Searching for the prodrome of Alzheimer’s disease. World Psychiatry 2008, 7, 72–78. [Google Scholar] [CrossRef] [Green Version]

| Medication | Is It Beneficial? | Evidence Supporting RCTs/Total RCTs | Quality of Evidence |
|---|---|---|---|
| Alzheimer’s Disease | |||
| Donepezil | Yes | 6/7 | ⋆⋆⋆⋆ |
| Galantamine | Yes | 3/4 | ⋆⋆⋆⋆ |
| Memantine | Yes | 2/3 | ⋆⋆ |
| Ginkgo Biloba | Yes | 3/3 | ⋆⋆⋆⋆ |
| Methylphenidate | Yes | 4/4 | ⋆⋆⋆⋆ |
| Modafinil | No | 0/1 | -- |
| Antidepressants | No | 1/7 | -- |
| Atypical antipsychotics | Not generally advised | ||
| Pain management | Yes | 1/1 | ⋆ |
| THC | No | 0/1 | -- |
| BrainUp-10 | Yes | 1/1 | ⋆ |
| Parkinson’s Disease | |||
| Memantine | No | 0/2 | -- |
| Amantadine | No | 0/1 | -- |
| Rivastigmine | Yes | 1/1 | ⋆ |
| Rasagiline | No | 0/1 | -- |
| Rotigotine | Yes | 3/5 | ⋆⋆ |
| Atomoxetine | No | 0/1 | -- |
| Methylphenidate | Yes | 1/1 | ⋆ |
| Piribedil | Yes | 1/1 | ⋆ |
| IRL752 | Yes | 1/1 | ⋆ |
| Safinamide | No | 0/2 | -- |
| Dementia with Lewy bodies | |||
| Rivastigmine | Yes | 1/1 | ⋆ |
| Frontotemporal Dementia | |||
| Oxytocin | No | 0/2 | -- |
| Dextroamphetamine | Yes | 1/1 | ⋆ |
| Agomelatine | Yes | 1/1 | ⋆ |
| Huntington’s Disease | |||
| Bupropion | No | 0/1 | -- |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Theleritis, C.; Siarkos, K.; Politis, A.; Smyrnis, N.; Papageorgiou, C.; Politis, A.M. A Systematic Review of Pharmacological Interventions for Apathy in Aging Neurocognitive Disorders. Brain Sci. 2023, 13, 1061. https://doi.org/10.3390/brainsci13071061
Theleritis C, Siarkos K, Politis A, Smyrnis N, Papageorgiou C, Politis AM. A Systematic Review of Pharmacological Interventions for Apathy in Aging Neurocognitive Disorders. Brain Sciences. 2023; 13(7):1061. https://doi.org/10.3390/brainsci13071061
Chicago/Turabian StyleTheleritis, Christos, Kostas Siarkos, Anastasios Politis, Nikolaos Smyrnis, Charalabos Papageorgiou, and Antonios M. Politis. 2023. "A Systematic Review of Pharmacological Interventions for Apathy in Aging Neurocognitive Disorders" Brain Sciences 13, no. 7: 1061. https://doi.org/10.3390/brainsci13071061