
Postoperative Cerebral Venous Sinus Thrombosis Following a Retrosigmoid Craniotomy—A Clinical and Radiological Analysis
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. CVST Classification
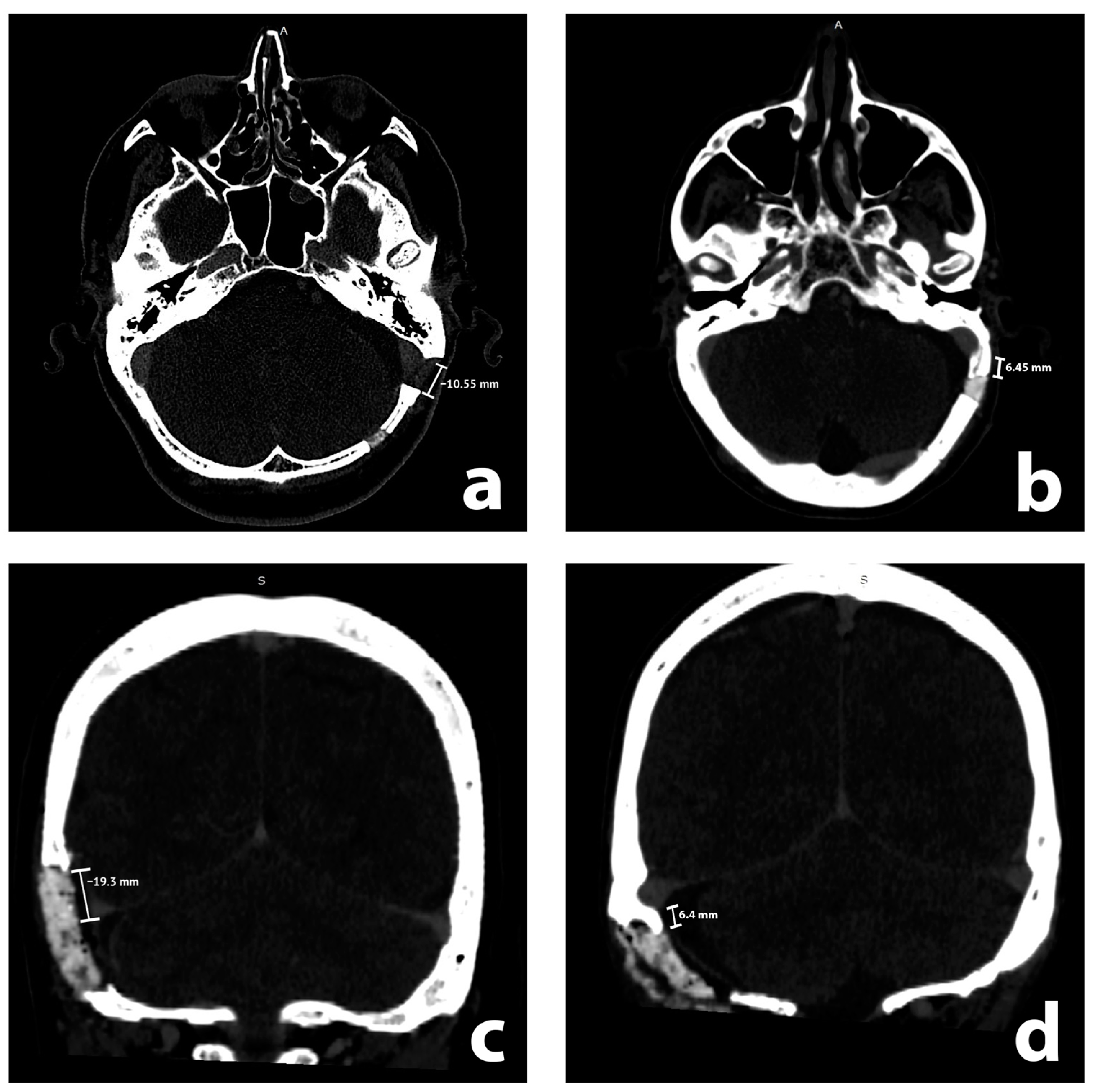
2.3. Radiological Analysis
2.4. Clinical Analysis
2.5. Statistical Analysis
3. Results
3.1. Patient Demographics
3.2. Radiological and Clinical Results
3.3. Patients with cCVST
3.4. Radiological and Clinical Analysis
4. Discussion
4.1. Mechanisms and Risk Factors
4.2. Diagnosis and Presentation
4.3. Medical Treatment
4.4. Interventional Treatment
4.5. Comparison with Other Studies
4.6. Pediatric Population
4.7. Approach Selection in CPA Surgery
4.8. Rare Case Reports
4.9. Limitations and Future Studies
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhou, C.; Evins, A.I.; Boschi, A.; Tang, Y.; Li, S.; Przepiorka, L.; Sadhwani, S.; Stieg, P.E.; Xu, T.; Bernardo, A. Preoperative identification of the initial burr hole site in retrosigmoid craniotomies: A teaching and technical note. Int. J. Med. Robot. 2019, 15, e1987. [Google Scholar] [CrossRef]
- Przepiórka, Ł.; Kunert, P.; Rutkowska, W.; Dziedzic, T.; Marchel, A. Surgery After Surgery for Vestibular Schwannoma: A Case Series. Front. Oncol. 2020, 10, 588260. [Google Scholar] [CrossRef] [PubMed]
- You, W.; Meng, J.; Yang, X.; Zhang, J.; Jiang, G.; Yan, Z.; Gu, F.; Tao, X.; Chen, Z.; Wang, Z.; et al. Microsurgical Management of Posterior Circulation Aneurysms: A Retrospective Study on Epidemiology, Outcomes, and Surgical Approaches. Brain Sci. 2022, 12, 1066. [Google Scholar] [CrossRef] [PubMed]
- Peris-Celda, M.; Graffeo, C.S.; Perry, A.; Carlstrom, L.P.; Link, M.J. Trigeminal Nerve Schwannoma of the Cerebellopontine Angle. J. Neurol. Surg. B Skull Base. 2018, 79 (Suppl. S5), S389–S390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsushima, K.; Kohno, M.; Komune, N.; Miki, K.; Matsushima, T.; Rhoton, A.L. Suprajugular extension of the retrosigmoid approach: Microsurgical anatomy. J. Neurosurg. 2014, 121, 397–407. [Google Scholar] [CrossRef]
- Li, Q.; Yu, Y.; Zhang, L.; Liu, J.; Ren, H.; Zhen, X. Staged Surgery for Intra-Extracranial Communicating Jugular Foramen Paraganglioma: A Case Report and Systematic Review. Brain Sci. 2022, 12, 1257. [Google Scholar] [CrossRef] [PubMed]
- Abou-Al-Shaar, H.; Gozal, Y.M.; Alzhrani, G.; Karsy, M.; Shelton, C.; Couldwell, W.T. Cerebral venous sinus thrombosis after vestibular schwannoma surgery: A call for evidence-based management guidelines. Neurosurg. Focus. 2018, 45, E4. [Google Scholar] [CrossRef] [Green Version]
- Gogu, A.E.; Jianu, D.C.; Dumitrascu, V.; Ples, H.; Stroe, A.Z.; Axelerad, D. MTHFR Gene Polymorphisms and Cardiovascular Risk Factors, Clinical-Imagistic Features and Outcome in Cerebral Venous Sinus Thrombosis. Brain Sci. 2020, 11, 23. [Google Scholar] [CrossRef]
- Pacchioni, A. Dissertatio Epistolaris de Glandulis Conglobatis Durae Meningis Humanae, Indeque Ortis Lymphaticis ad Piam Meningem Productis; Buagni: Rome, Italy, 1705. [Google Scholar]
- Brunori, A.; Vagnozzi, R.; Giuffrè, R. Antonio Pacchioni (1665–1726): Early studies of the dura mater. J. Neurosurg. 1993, 78, 515–518. [Google Scholar] [CrossRef] [Green Version]
- López-Ratón, M.; Rodríguez-Álvarez, M.X.; Cadarso-Suárez, C.; Gude-Sampedro, F. OptimalCutpoints: An R Package for Selecting Optimal Cutpoints in Diagnostic Tests. J. Stat. Softw. 2014, 61, 1–36. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing [Internet]. Vienna, Austria: R Foundation for Statistical Computing. 2021. Available online: https://www.R-project.org/ (accessed on 10 September 2022).
- Moore, J.; Thomas, P.; Cousins, V.; Rosenfeld, J.V. Diagnosis and Management of Dural Sinus Thrombosis following Resection of Cerebellopontine Angle Tumors. J. Neurol. Surg. B Skull Base. 2014, 75, 402–408. [Google Scholar] [PubMed] [Green Version]
- Benjamin, C.G.; Sen, R.D.; Golfinos, J.G.; Sen, C.; Roland, J.T.; McMenomey, S.; Pacione, D. Postoperative cerebral venous sinus thrombosis in the setting of surgery adjacent to the major dural venous sinuses. J. Neurosurg. 2018, 1, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerges, C.; Malloy, P.; Rabah, N.; Defta, D.; Duan, Y.; Wright, C.H.; van Keulen, M.; Wright, J.; Mowry, S.; Megerian, C.A.; et al. Functional Outcomes and Postoperative Cerebral Venous Sinus Thrombosis after Translabyrinthine Approach for Vestibular Schwannoma Resection: A Radiographic Demonstration of Anatomic Predictors. J. Neurol. Surg. B Skull Base. 2022, 83 (Suppl. 2), e89–e95. [Google Scholar] [CrossRef] [PubMed]
- Apra, C.; Kotbi, O.; Turc, G.; Corns, R.; Pagès, M.; Souillard-Scémama, R.; Dezamis, E.; Parraga, E.; Meder, J.-F.; Sauvageon, X. Presentation and management of lateral sinus thrombosis following posterior fossa surgery. J. Neurosurg. 2017, 126, 8–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Izzo, A.; Stifano, V.; Della Pepa, G.M.; Di Domenico, M.; D’Alessandris, Q.G.; Menna, G.; D’Ercole, M.; Lauretti, L.; Olivi, A.; Montano, N. Tailored Approach and Multimodal Intraoperative Neuromonitoring in Cerebellopontine Angle Surgery. Brain Sci. 2022, 12, 1167. [Google Scholar] [CrossRef]
- Guazzo, E.; Panizza, B.; Lomas, A.; Wood, M.; Amato, D.; Alalade, A.; Gandhi, M.; Bowman, J. Cerebral Venous Sinus Thrombosis After Translabyrinthine Vestibular Schwannoma-A Prospective Study and Suggested Management Paradigm. Otol. Neurotol. 2020, 41, e273–e279. [Google Scholar] [CrossRef] [PubMed]
- Aliprandi, A.; Borelli, P.; Polonia, V.; Salmaggi, A. Headache in cerebral venous thrombosis. Neurol. Sci. 2020, 41 (Suppl. S2), 401–406. [Google Scholar] [CrossRef]
- Ohata, K.; Haque, M.; Morino, M.; Nagai, K.; Nishio, A.; Nishijima, Y.; Hakuba, A. Occlusion of the sigmoid sinus after surgery via the presigmoidal-transpetrosal approach. J. Neurosurg. 1998, 89, 575–584. [Google Scholar] [CrossRef] [Green Version]
- Vogl, T.J.; Bergman, C.; Villringer, A.; Einhäupl, K.; Lissner, J.; Felix, R. Dural sinus thrombosis: Value of venous MR angiography for diagnosis and follow-up. AJR Am. J. Roentgenol. 1994, 162, 1191–1198. [Google Scholar] [CrossRef]
- Rodallec, M.H.; Krainik, A.; Feydy, A.; Hélias, A.; Colombani, J.M.; Jullès, M.C.; Marteau, V.; Zins, M. Cerebral venous thrombosis and multidetector CT angiography: Tips and tricks. Radiographics 2006, 26 (Suppl. S1), S5–S18; discussion S42–S43. [Google Scholar] [CrossRef]
- Salgado-Lopez, L.; Custozzo, A.; Raviv, N.; Abdelhak, T.; Peris-Celda, M. Cerebral sinus thrombosis as an initial symptom of acute promyelocytic leukemia: Case report and literature review. Surg. Neurol. Int. 2022, 13, 89. [Google Scholar] [CrossRef]
- Shew, M.; Kavookjian, H.; Dahlstrom, K.; Muelleman, T.; Lin, J.; Camarata, P.; Ledbetter, L.; Staecker, H. Incidence and Risk Factors for Sigmoid Venous Thrombosis Following CPA Tumor Resection. Otol. Neurotol. 2018, 39, e376–e380. [Google Scholar] [CrossRef] [PubMed]
- Orlev, A.; Jackson, C.M.; Luksik, A.; Garzon-Muvdi, T.; Yang, W.; Chien, W.; Harnof, S.; Tamargo, R.J. Natural History of Untreated Transverse/Sigmoid Sinus Thrombosis Following Posterior Fossa Surgery: Case Series and Literature Review. Oper. Neurosurg. 2020, 19, 109–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kow, C.Y.; Caldwell, J.; Mchugh, F.; Sillars, H.; Bok, A. Dural venous sinus thrombosis after cerebellopontine angle surgery: Should it be treated? J. Clin. Neurosci. 2020, 75, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Manzoor, N.F.; Ray, A.; Singer, J.; Nord, R.; Sunshine, J.; Megerian, C.A.; Bambakidis, N.C.; Semaan, M.T. Successful endovascular management of venous sinus thrombosis complicating trans-labyrinthine removal of vestibular schwanomma. Am. J. Otolaryngol. 2016, 37, 379–382. [Google Scholar] [CrossRef]
- Teping, F.; Linsler, S.; Zemlin, M.; Oertel, J. The semisitting position in pediatric neurosurgery: Pearls and pitfalls of a 10-year experience. J. Neurosurg. Pediatr. 2021, 28, 724–733. [Google Scholar] [CrossRef]
- Petrov, D.; Uohara, M.Y.; Ichord, R.; Ali, Z.; Jastrzab, L.; Lang, S.S.; Billinghurst, L. Pediatric cerebral sinovenous thrombosis following cranial surgery. Childs Nerv. Syst. 2017, 33, 491–497. [Google Scholar] [CrossRef]
- Sawarkar, D.P.; Verma, S.K.; Singh, P.K.; Doddamani, R.; Kumar, A.; Sharma, B.S. Fatal Superior Sagittal Sinus and Torcular Thrombosis After Vestibular Schwannoma Surgery: Report of a Rare Complication and Review of the Literature. World Neurosurg. 2016, 96, e19–e607. [Google Scholar] [CrossRef]
- Nadkarni, T.D.; Dindorkar, K.S.; Desai, K.; Goel, A. Cavernous sinus thrombosis and air embolism following surgery for acoustic neurinoma: A case report. Neurol. India. 2002, 50, 201–203. [Google Scholar]
- Wong, A.K.; Wong, R.H. Successful treatment of superior sagittal sinus thrombosis after translabyrinthine resection of metastatic neuroendocrine tumor: A case report and review of literature. Surg. Neurol. Int. 2020, 11, 410. [Google Scholar] [CrossRef]
- Keiper, G.L.; Sherman, J.D.; Tomsick, T.A.; Tew, J.M. Dural sinus thrombosis and pseudotumor cerebri: Unexpected complications of suboccipital craniotomy and translabyrinthine craniectomy. J. Neurosurg. 1999, 91, 192–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jean, W.C.; Felbaum, D.R.; Stemer, A.B.; Hoa, M.; Kim, H.J. Venous sinus compromise after pre-sigmoid, transpetrosal approach for skull base tumors: A study on the asymptomatic incidence and report of a rare dural arteriovenous fistula as symptomatic manifestation. J. Clin. Neurosci. 2017, 39, 114–117. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, A.; El-Kouri, N.; Dymon, Z.; Serrano, D.; Bashir, M.; Anderson, D.; Leonetti, J. Sigmoid Sinus Patency following Vestibular Schwannoma Resection via Retrosigmoid versus Translabyrinthine Approach. J. Neurol. Surg. B Skull Base. 2021, 82, 461–465. [Google Scholar] [CrossRef] [PubMed]
- Krystkiewicz, K.; Wrona, D.; Tosik, M.; Birski, M.; Szylberg, Ł.; Morawska, A.; Furtak, J.; Wałęsa, C.; Stopa, K.; Harat, M. Dural sinus thrombosis after resection of vestibular schwannoma using suboccipital retrosigmoid approach-thrombosis classification and management proposal. Neurosurg. Rev. 2022, 45, 2211–2219. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Data | Measurement | p-Value |
|---|---|---|
| Distance to the sigmoid sinus (mm) | N/A | |
| median (range) | −1.75 (−10.55, 7.45) | |
| 1st, 3rd quartile | −5.23, 0.95 | |
| Exposure of the sigmoid sinus | 0.01 | |
| exposed | 79 (60.77%) | |
| hidden | 51 (39.23%) | |
| Distance to the transverse sinus (mm) | N/A | |
| median (range) | −6.60 (−23.15, 9.2) | |
| 1st, 3rd quartile | −10.13, −2.76 | |
| Exposure of the transverse sinus | <0.0001 | |
| exposed | 108 (83.1%) | |
| hidden | 22 (16.9%) | |
| Radiologic features of CVST | 0.48 | |
| present | 61 (46.9%) | |
| none | 69 (53.1%) | |
| Transverse sinus thrombosis | 0.01 | |
| present | 40 (30.8%) | |
| absent | 21 (16.2%) | |
| Sigmoid sinus thrombosis | 0.1 | |
| present | 37 (28.5%) | |
| absent | 24 (18.5%) | |
| Junctions of sinuses thrombosis | 0.7 | |
| present | 32 (24.6%) | |
| absent | 29 (22.3%) | |
| Intraparenchymal hemorrhage | <0.0001 | |
| present | 2 (1.5%) | |
| absent | 128 (98.5%) | |
| Sinus dominance | <0.0001 | |
| right | 94 (72.3%) | |
| left | 32 (24.6%) | |
| none | 4 (3.1%) |
| Data | Measurement |
|---|---|
| Clinical diagnosis of CVST | |
| present | 4 (3.1%) |
| absent | 126 (96.9%) |
| Intraoperative injuries of the sinuses | |
| present | 6 (4.6%) |
| absent | 124 (95.4%) |
| Clinical risk factors | |
| Overweight/obesity | 23 (17.7%) |
| Oncologic past medical history | 10 (7.7%) |
| Deep venous thrombosis | 2 (1.5%) |
| Chronic venous insufficiency | 3 (2.3%) |
| Other | 14 (10.8%) |
| Length of stay (days) | |
| median (range) | 11 (8–48) |
| 1st, 3rd quartile | 10, 14 |
| Postoperative headaches refractory to regular medical treatment | |
| present | 12 (9.2%) |
| absent | 115 (88.5%) |
| not applicable/patient unconscious | 1 (0.8%) |
| no data | 2 (1.5%) |
| Exposure of the transverse sinus | |
| exposed | 108 (83.1%) |
| hidden | 22 (16.9%) |
| Analyzed Factor | Value | rCVST Present | rCVST Absent | p-Value |
|---|---|---|---|---|
| Sex | male | 19 (37.3%) | 32 (62.7%) | 0.076 |
| female | 42 (53.2%) | 37 (46.8%) | ||
| Age (years) | median (range) | 48 (22–76) | 43 (20–82) | 0.774 |
| 1st, 3rd quartile | 40, 58 | 33, 57 | ||
| Side | right | 26 (40.6%) | 38 (59.4%) | 0.157 |
| left | 35 (53.0%) | 31 (47.0%) | ||
| Tumor maximal size (mm) | median (range) | 31 (12–50) | 32 (9–57) | 0.810 |
| 1st, 3rd quartile | 24, 39 | 22, 38 | ||
| Tumor volume (cm3) | median (range) | 11 (0.26–41.89) | 11.73 (0.18–59.9) | 0.493 |
| 1st, 3rd quartile | 3.78, 18.25 | 3.94, 18.38 | ||
| Distance to the sigmoid sinus (quantitative) | median (range) | −2.67 (−9.4–6.2) | −1.6 (−10.6–7.5) | 0.04 |
| 1st, 3rd quartile | −5.6, 0 | −4.75, 1.95 | ||
| Exposure of the sigmoid sinus (qualitative) | exposed | 41 (51.9%) | 38 (48.1%) | 1 |
| hidden | 20 (39.2%) | 31 (60.8%) | ||
| Distance to the transverse sinus (quantitative) | median (range) | −7.3 (−21.5–9.2) | −4.9 (−23.15–7.8) | 0.028 |
| 1st, 3rd quartile | −11.4, −5.15 | −7.95, −2.5 | ||
| Exposure of the transverse sinus (qualitative) | exposed | 53 (49.1%) | 55 (50.9%) | 1 |
| hidden | 8 (36.4%) | 14 (63.6%) | ||
| Exposure of both sinuses (qualitative) | both exposed | 38 (52.1%) | 35 (47.9%) | 0.46 |
| one exposed or none | 23 (40.4%) | 34 (59.6%) | ||
| Exposure of at least one sinus (qualitative) | one or two sinuses exposed | 56 (49.1%) | 58 (50.9%) | 0.180 |
| none exposed | 5 (31.3%) | 11 (68.8%) | ||
| Sinus dominance | right | 42 (44.7%) | 52 (55.3%) | 0.46 |
| left | 18 (56.3%) | 14 (43.8%) | ||
| none | 1 (25%) | 3 (75%) | ||
| Overweight/obesity | present | 12 (52.2%) | 11 (47.8%) | 0.578 |
| absent | 49 (45.8%) | 58 (54.2%) | ||
| Oncologic past medical history | present | 6 (60%) | 4 (40%) | 0.514 |
| absent | 55 (45.8%) | 65 (54.2%) | ||
| Deep venous thrombosis | present | 1 (50%) | 1 (50%) | 1 |
| absent | 60 (49.6%) | 68 (53.1%) | ||
| Chronic venous insufficiency | present | 2 (66.7%) | 1 (33.3%) | 0.600 |
| absent | 59 (46.5%) | 68 (53.5%) | ||
| Other clinical risk factors | present | 7 (50%) | 7 (50%) | 0.807 |
| absent | 54 (46.6%) | 62 (53.4%) | ||
| Postoperative headaches refractory to regular medical treatment | present | 6 (50%) | 6 (50%) | 0.546 |
| absent | 53 (46.1%) | 62 53.9%) | ||
| not applicable/patient unconscious | 1 (100%) | 0 | ||
| no data | 1 (50%) | 1 (50%) | ||
| Surgery on the side of dominant sinus | yes | 21 (36.8%) | 36 (63.2%) | 0.042 |
| no | 40 (54.8%) | 33 (45.2%) | ||
| Intraoperative injuries of the sinus | yes | 4 (57.1%) | 3 (42.9%) | 0.705 |
| no | 57 (46.3%) | 66 (53.7%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Przepiorka, L.; Wójtowicz, K.; Camlet, K.; Jankowski, J.; Kujawski, S.; Grabowska-Derlatka, L.; Marchel, A.; Kunert, P. Postoperative Cerebral Venous Sinus Thrombosis Following a Retrosigmoid Craniotomy—A Clinical and Radiological Analysis. Brain Sci. 2023, 13, 1039. https://doi.org/10.3390/brainsci13071039
Przepiorka L, Wójtowicz K, Camlet K, Jankowski J, Kujawski S, Grabowska-Derlatka L, Marchel A, Kunert P. Postoperative Cerebral Venous Sinus Thrombosis Following a Retrosigmoid Craniotomy—A Clinical and Radiological Analysis. Brain Sciences. 2023; 13(7):1039. https://doi.org/10.3390/brainsci13071039
Chicago/Turabian StylePrzepiorka, Lukasz, Katarzyna Wójtowicz, Katarzyna Camlet, Jan Jankowski, Sławomir Kujawski, Laretta Grabowska-Derlatka, Andrzej Marchel, and Przemysław Kunert. 2023. "Postoperative Cerebral Venous Sinus Thrombosis Following a Retrosigmoid Craniotomy—A Clinical and Radiological Analysis" Brain Sciences 13, no. 7: 1039. https://doi.org/10.3390/brainsci13071039