
Changes in Functional Connectivity of Hippocampal Subregions in Patients with Obstructive Sleep Apnea after Six Months of Continuous Positive Airway Pressure Treatment
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Polysomnography
2.3. Clinical and Neuropsychological Assessments
2.4. Continuous Positive Airway Pressure Treatment
2.5. MRI Data Acquisition
2.6. Data Preprocessing
2.7. Definition of Regions of Interest and Functional Connectivity Calculations across Hippocampal Subregions
2.8. Statistical Analysis
3. Results
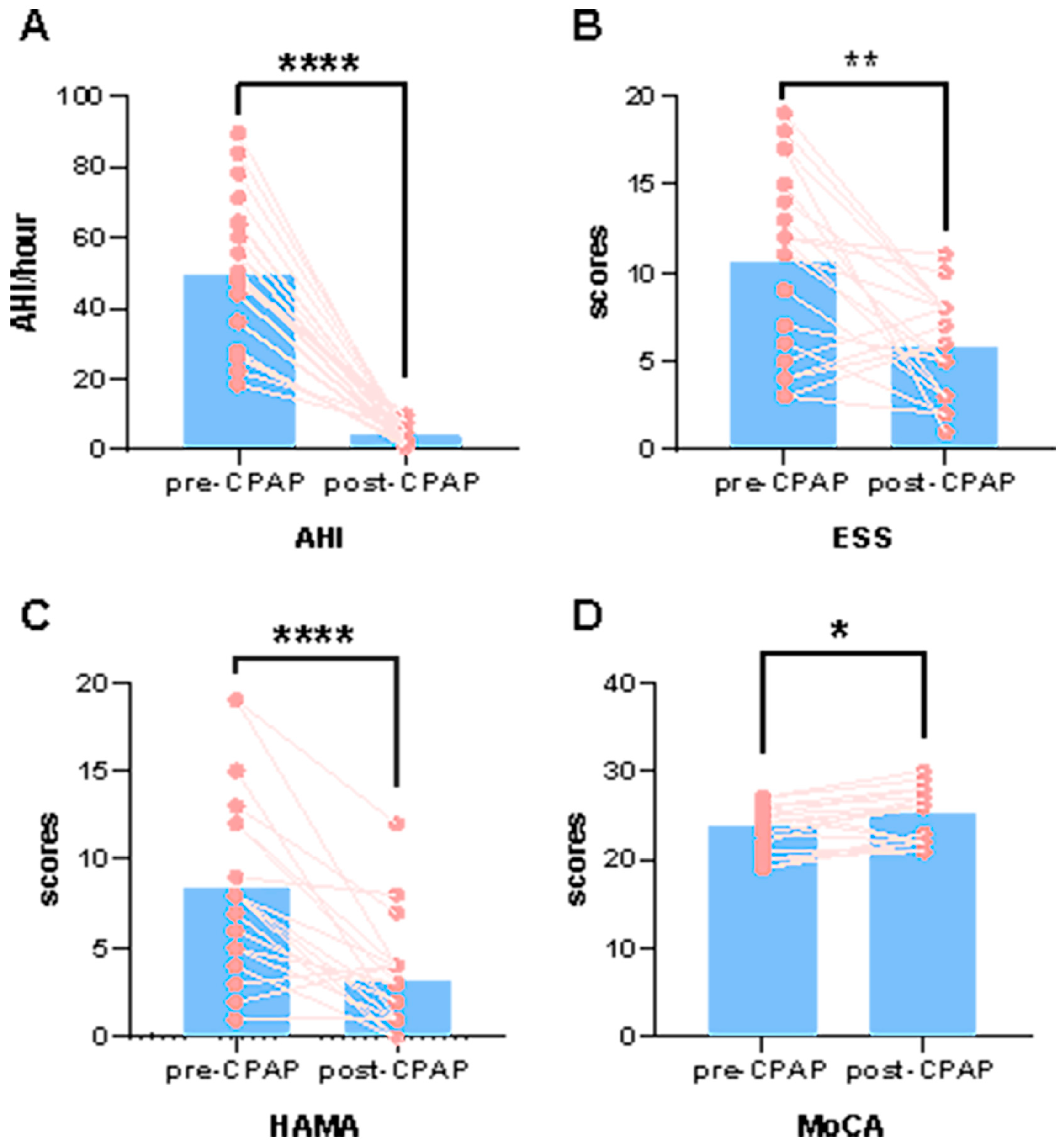
3.1. Differences in Demographic and Clinical Characteristics
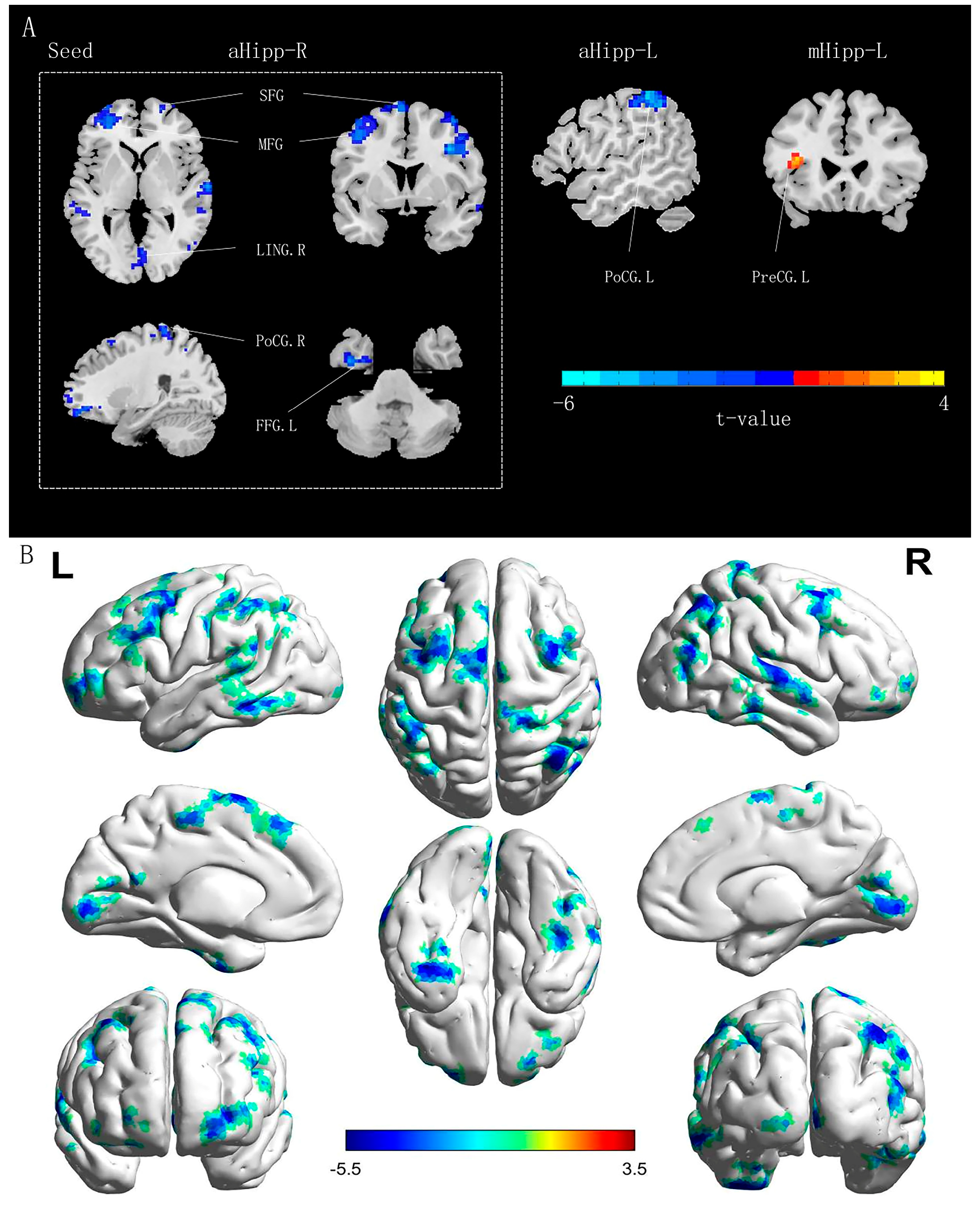
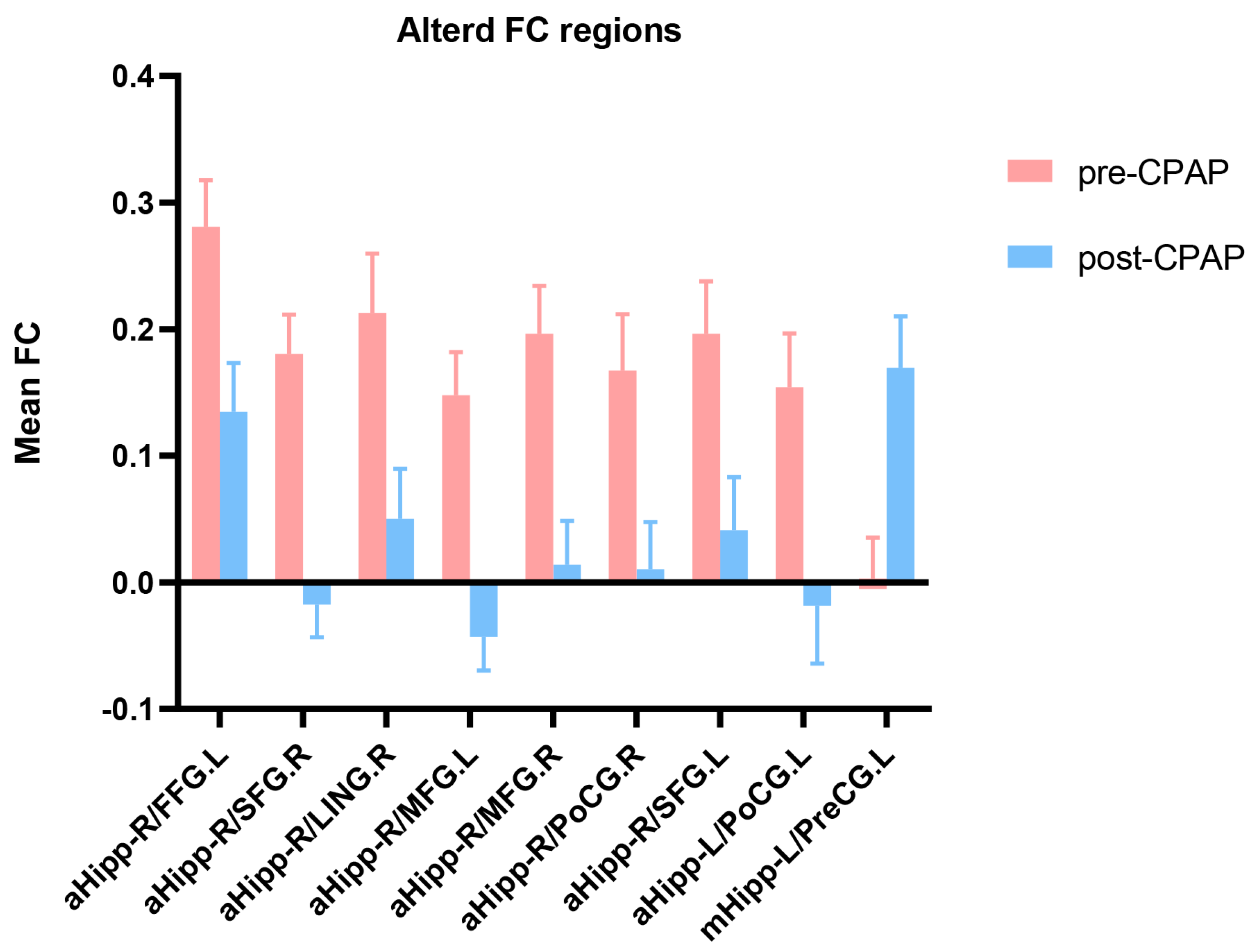
3.2. Differences in Functional Connectivity of Hippocampal Subregions in Patients with OSA before and after CPAP Treatment
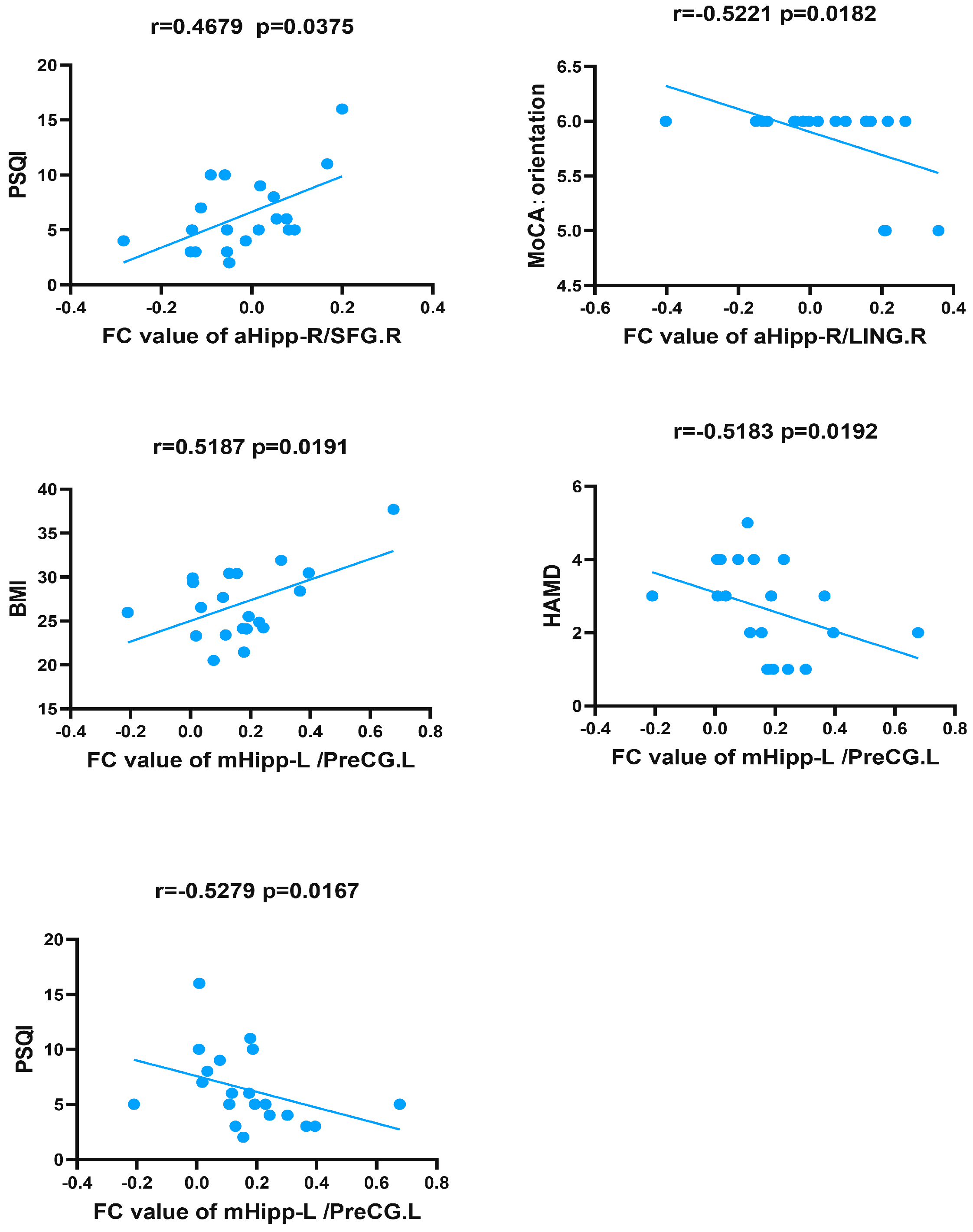
3.3. Correlations between Functional Connectivity Changes in Hippocampal Subregions and Clinical Data in Patients with OSA
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Benjafield, A.V.; Ayas, N.T.; Eastwood, P.R.; Heinzer, R.; Ip, M.S.M.; Morrell, M.J.; Nunez, C.M.; Patel, S.R.; Penzel, T.; Pépin, J.-L.; et al. Estimation of the Global Prevalence and Burden of Obstructive Sleep Apnoea: A Literature-Based Analysis. Lancet Respir. Med. 2019, 7, 687–698. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.J.; Sundar, K.M. Evaluation and Management of Adults with Obstructive Sleep Apnea Syndrome. Lung 2021, 199, 87–101. [Google Scholar] [CrossRef] [PubMed]
- Vanek, J.; Prasko, J.; Genzor, S.; Ociskova, M.; Kantor, K.; Holubova, M.; Slepecky, M.; Nesnidal, V.; Kolek, A.; Sova, M. Obstructive Sleep Apnea, Depression and Cognitive Impairment. Sleep Med. 2020, 72, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Olaithe, M.; Bucks, R.S.; Hillman, D.R.; Eastwood, P.R. Cognitive Deficits in Obstructive Sleep Apnea: Insights from a Meta-Review and Comparison with Deficits Observed in COPD, Insomnia, and Sleep Deprivation. Sleep Med. Rev. 2018, 38, 39–49. [Google Scholar] [CrossRef]
- Cha, J.; Zea-Hernandez, J.A.; Sin, S.; Graw-Panzer, K.; Shifteh, K.; Isasi, C.R.; Wagshul, M.E.; Moran, E.E.; Posner, J.; Zimmerman, M.E.; et al. The Effects of Obstructive Sleep Apnea Syndrome on the Dentate Gyrus and Learning and Memory in Children. J. Neurosci. 2017, 37, 4280–4288. [Google Scholar] [CrossRef]
- Tahmasian, M.; Rosenzweig, I.; Eickhoff, S.B.; Sepehry, A.A.; Laird, A.R.; Fox, P.T.; Morrell, M.J.; Khazaie, H.; Eickhoff, C.R. Structural and Functional Neural Adaptations in Obstructive Sleep Apnea: An Activation Likelihood Estimation Meta-Analysis. Neurosci. Biobehav. Rev. 2016, 65, 142–156. [Google Scholar] [CrossRef]
- Daulatzai, M.A. Quintessential Risk Factors: Their Role in Promoting Cognitive Dysfunction and Alzheimer’s Disease. Neurochem. Res. 2012, 37, 2627–2658. [Google Scholar] [CrossRef]
- Tatu, L.; Vuillier, F. Structure and Vascularization of the Human Hippocampus. Front. Neurol. Neurosci. 2014, 34, 18–25. [Google Scholar] [CrossRef]
- Daulatzai, M.A. Evidence of Neurodegeneration in Obstructive Sleep Apnea: Relationship between Obstructive Sleep Apnea and Cognitive Dysfunction in the Elderly. J. Neurosci. Res. 2015, 93, 1778–1794. [Google Scholar] [CrossRef]
- Zhou, L.; Liu, G.; Luo, H.; Li, H.; Peng, Y.; Zong, D.; Ouyang, R. Aberrant Hippocampal Network Connectivity Is Associated With Neurocognitive Dysfunction in Patients With Moderate and Severe Obstructive Sleep Apnea. Front. Neurol. 2020, 11, 580408. [Google Scholar] [CrossRef]
- Bartlett, D.J.; Rae, C.; Thompson, C.H.; Byth, K.; Joffe, D.A.; Enright, T.; Grunstein, R.R. Hippocampal Area Metabolites Relate to Severity and Cognitive Function in Obstructive Sleep Apnea. Sleep Med. 2004, 5, 593–596. [Google Scholar] [CrossRef]
- Liu, X.; Wei, Z.; Chen, L.; Duan, W.; Li, H.; Kong, L.; Shu, Y.; Li, P.; Li, K.; Xie, W.; et al. Effects of 3-Month CPAP Therapy on Brain Structure in Obstructive Sleep Apnea: A Diffusion Tensor Imaging Study. Front. Neurol. 2022, 13, 913193. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Chavez, A.S.; Macey, P.M.; Woo, M.A.; Yan-Go, F.L.; Harper, R.M. Altered Global and Regional Brain Mean Diffusivity in Patients with Obstructive Sleep Apnea. J. Neurosci. Res. 2012, 90, 2043–2052. [Google Scholar] [CrossRef]
- Canessa, N.; Castronovo, V.; Cappa, S.F.; Aloia, M.S.; Marelli, S.; Falini, A.; Alemanno, F.; Ferini-Strambi, L. Obstructive Sleep Apnea: Brain Structural Changes and Neurocognitive Function before and after Treatment. Am. J. Respir. Crit. Care Med. 2011, 183, 1419–1426. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Macey, P.M.; Cross, R.L.; Woo, M.A.; Yan-Go, F.L.; Harper, R.M. Neural Alterations Associated with Anxiety Symptoms in Obstructive Sleep Apnea Syndrome. Depress Anxiety 2009, 26, 480–491. [Google Scholar] [CrossRef]
- Alkan, A.; Sharifov, R.; Akkoyunlu, M.E.; Kiliçarslan, R.; Toprak, H.; Aralasmak, A.; Kart, L. MR Spectroscopy Features of Brain in Patients with Mild and Severe Obstructive Sleep Apnea Syndrome. Clin. Imaging 2013, 37, 989–992. [Google Scholar] [CrossRef]
- Halbower, A.C.; Degaonkar, M.; Barker, P.B.; Earley, C.J.; Marcus, C.L.; Smith, P.L.; Prahme, M.C.; Mahone, E.M. Childhood Obstructive Sleep Apnea Associates with Neuropsychological Deficits and Neuronal Brain Injury. PLoS Med. 2006, 3, e301. [Google Scholar] [CrossRef] [PubMed]
- Rajah, M.N.; Kromas, M.; Han, J.E.; Pruessner, J.C. Group Differences in Anterior Hippocampal Volume and in the Retrieval of Spatial and Temporal Context Memory in Healthy Young versus Older Adults. Neuropsychologia 2010, 48, 4020–4030. [Google Scholar] [CrossRef]
- Strange, B.A.; Witter, M.P.; Lein, E.S.; Moser, E.I. Functional Organization of the Hippocampal Longitudinal Axis. Nat. Rev. Neurosci. 2014, 15, 655–669. [Google Scholar] [CrossRef]
- Poppenk, J.; Evensmoen, H.R.; Moscovitch, M.; Nadel, L. Long-Axis Specialization of the Human Hippocampus. Trends Cogn. Sci. 2013, 17, 230–240. [Google Scholar] [CrossRef]
- Poppenk, J.; Moscovitch, M. A Hippocampal Marker of Recollection Memory Ability among Healthy Young Adults: Contributions of Posterior and Anterior Segments. Neuron 2011, 72, 931–937. [Google Scholar] [CrossRef] [PubMed]
- Kensinger, E.A. Remembering the Details: Effects of Emotion. Emot. Rev. 2009, 1, 99–113. [Google Scholar] [CrossRef] [PubMed]
- Moscovitch, M.; Cabeza, R.; Winocur, G.; Nadel, L. Episodic Memory and Beyond: The Hippocampus and Neocortex in Transformation. Annu. Rev. Psychol. 2016, 67, 105–134. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.H.M.; Chuah, L.Y.M.; Sim, S.K.Y.; Chee, M.W.L. Hippocampal Region-Specific Contributions to Memory Performance in Normal Elderly. Brain Cogn. 2010, 72, 400–407. [Google Scholar] [CrossRef]
- Travis, S.G.; Huang, Y.; Fujiwara, E.; Radomski, A.; Olsen, F.; Carter, R.; Seres, P.; Malykhin, N.V. High Field Structural MRI Reveals Specific Episodic Memory Correlates in the Subfields of the Hippocampus. Neuropsychologia 2014, 53, 233–245. [Google Scholar] [CrossRef] [PubMed]
- DeMaster, D.; Pathman, T.; Lee, J.K.; Ghetti, S. Structural Development of the Hippocampus and Episodic Memory: Developmental Differences along the Anterior/Posterior Axis. Cereb. Cortex 2014, 24, 3036–3045. [Google Scholar] [CrossRef]
- Zarei, M.; Beckmann, C.F.; Binnewijzend, M.A.A.; Schoonheim, M.M.; Oghabian, M.A.; Sanz-Arigita, E.J.; Scheltens, P.; Matthews, P.M.; Barkhof, F. Functional Segmentation of the Hippocampus in the Healthy Human Brain and in Alzheimer’s Disease. Neuroimage 2013, 66, 28–35. [Google Scholar] [CrossRef]
- Dean, D.J.; Orr, J.M.; Bernard, J.A.; Gupta, T.; Pelletier-Baldelli, A.; Carol, E.E.; Mittal, V.A. Hippocampal Shape Abnormalities Predict Symptom Progression in Neuroleptic-Free Youth at Ultrahigh Risk for Psychosis. Schizophr. Bull. 2016, 42, 161–169. [Google Scholar] [CrossRef]
- Tamnes, C.K.; Bos, M.G.N.; van de Kamp, F.C.; Peters, S.; Crone, E.A. Longitudinal Development of Hippocampal Subregions from Childhood to Adulthood. Dev. Cogn. Neurosci. 2018, 30, 212–222. [Google Scholar] [CrossRef]
- Thompson, D.K.; Omizzolo, C.; Adamson, C.; Lee, K.J.; Stargatt, R.; Egan, G.F.; Doyle, L.W.; Inder, T.E.; Anderson, P.J. Longitudinal Growth and Morphology of the Hippocampus through Childhood: Impact of Prematurity and Implications for Memory and Learning. Hum. Brain Mapp. 2014, 35, 4129–4139. [Google Scholar] [CrossRef]
- Xiong, Y.; Zhou, X.J.; Nisi, R.A.; Martin, K.R.; Karaman, M.M.; Cai, K.; Weaver, T.E. Brain White Matter Changes in CPAP-Treated Obstructive Sleep Apnea Patients with Residual Sleepiness. J. Magn. Reson. Imaging JMRI 2017, 45, 1371–1378. [Google Scholar] [CrossRef] [PubMed]
- Henderson, L.A.; Fatouleh, R.H.; Lundblad, L.C.; McKenzie, D.K.; Macefield, V.G. Effects of 12 Months Continuous Positive Airway Pressure on Sympathetic Activity Related Brainstem Function and Structure in Obstructive Sleep Apnea. Front. Neurosci. 2016, 10, 90. [Google Scholar] [CrossRef] [PubMed]
- Dalmases, M.; Solé-Padullés, C.; Torres, M.; Embid, C.; Nuñez, M.D.; Martínez-Garcia, M.Á.; Farré, R.; Bargalló, N.; Bartrés-Faz, D.; Montserrat, J.M. Effect of CPAP on Cognition, Brain Function, and Structure Among Elderly Patients With OSA: A Randomized Pilot Study. Chest 2015, 148, 1214–1223. [Google Scholar] [CrossRef]
- Zhao, Y.Y.; Wang, R.; Gleason, K.J.; Lewis, E.F.; Quan, S.F.; Toth, C.M.; Morrical, M.; Rueschman, M.; Weng, J.; Ware, J.H.; et al. Effect of Continuous Positive Airway Pressure Treatment on Health-Related Quality of Life and Sleepiness in High Cardiovascular Risk Individuals With Sleep Apnea: Best Apnea Interventions for Research (BestAIR) Trial. Sleep 2017, 40, zsx040. [Google Scholar] [CrossRef]
- Reid, M.L.; Gleason, K.J.; Bakker, J.P.; Wang, R.; Mittleman, M.A.; Redline, S. The Role of Sham Continuous Positive Airway Pressure as a Placebo in Controlled Trials: Best Apnea Interventions for Research Trial. Sleep 2019, 42, zsz099. [Google Scholar] [CrossRef] [PubMed]
- Labarca, G.; Saavedra, D.; Dreyse, J.; Jorquera, J.; Barbe, F. Efficacy of CPAP for Improvements in Sleepiness, Cognition, Mood, and Quality of Life in Elderly Patients With OSA: Systematic Review and Meta-Analysis of Randomized Controlled Trials. Chest 2020, 158, 751–764. [Google Scholar] [CrossRef]
- Wang, G.; Goebel, J.R.; Li, C.; Hallman, H.G.; Gilford, T.M.; Li, W. Therapeutic Effects of CPAP on Cognitive Impairments Associated with OSA. J. Neurol. 2020, 267, 2823–2828. [Google Scholar] [CrossRef]
- Castronovo, V.; Scifo, P.; Castellano, A.; Aloia, M.S.; Iadanza, A.; Marelli, S.; Cappa, S.F.; Strambi, L.F.; Falini, A. White Matter Integrity in Obstructive Sleep Apnea before and after Treatment. Sleep 2014, 37, 1465–1475. [Google Scholar] [CrossRef]
- Kim, J.S.; Seo, J.H.; Kang, M.-R.; Seong, M.J.; Lee, W.G.; Joo, E.Y.; Hong, S.B. Effect of Continuous Positive Airway Pressure on Regional Cerebral Blood Flow in Patients with Severe Obstructive Sleep Apnea Syndrome. Sleep Med. 2017, 32, 122–128. [Google Scholar] [CrossRef]
- Liu, X.; Chen, L.; Duan, W.; Li, H.; Kong, L.; Shu, Y.; Li, P.; Li, K.; Xie, W.; Zeng, Y.; et al. Abnormal Functional Connectivity of Hippocampal Subdivisions in Obstructive Sleep Apnea: A Resting-State Functional Magnetic Resonance Imaging Study. Front. Neurosci. 2022, 16, 850940. [Google Scholar] [CrossRef]
- Kapur, V.K.; Auckley, D.H.; Chowdhuri, S.; Kuhlmann, D.C.; Mehra, R.; Ramar, K.; Harrod, C.G. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2017, 13, 479–504. [Google Scholar] [CrossRef]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for Scoring Respiratory Events in Sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2012, 8, 597–619. [Google Scholar] [CrossRef]
- Zimmerman, M.; Martinez, J.H.; Young, D.; Chelminski, I.; Dalrymple, K. Severity Classification on the Hamilton Depression Rating Scale. J. Affect. Disord. 2013, 150, 384–388. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Yan, C.-G.; Cheung, B.; Kelly, C.; Colcombe, S.; Craddock, R.C.; Di Martino, A.; Li, Q.; Zuo, X.-N.; Castellanos, F.X.; Milham, M.P. A Comprehensive Assessment of Regional Variation in the Impact of Head Micromovements on Functional Connectomics. Neuroimage 2013, 76, 183–201. [Google Scholar] [CrossRef]
- Van Dijk, K.R.A.; Sabuncu, M.R.; Buckner, R.L. The Influence of Head Motion on Intrinsic Functional Connectivity MRI. Neuroimage 2012, 59, 431–438. [Google Scholar] [CrossRef]
- Zhu, D.; Yuan, T.; Gao, J.; Xu, Q.; Xue, K.; Zhu, W.; Tang, J.; Liu, F.; Wang, J.; Yu, C. Correlation between Cortical Gene Expression and Resting-State Functional Network Centrality in Healthy Young Adults. Hum. Brain Mapp. 2021, 42, 2236–2249. [Google Scholar] [CrossRef] [PubMed]
- Malykhin, N.V.; Bouchard, T.P.; Ogilvie, C.J.; Coupland, N.J.; Seres, P.; Camicioli, R. Three-Dimensional Volumetric Analysis and Reconstruction of Amygdala and Hippocampal Head, Body and Tail. Psychiatry Res. 2007, 155, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Evensmoen, H.R.; Lehn, H.; Xu, J.; Witter, M.P.; Nadel, L.; Håberg, A.K. The Anterior Hippocampus Supports a Coarse, Global Environmental Representation and the Posterior Hippocampus Supports Fine-Grained, Local Environmental Representations. J. Cogn. Neurosci. 2013, 25, 1908–1925. [Google Scholar] [CrossRef] [PubMed]
- Greicius, M.D.; Krasnow, B.; Reiss, A.L.; Menon, V. Functional Connectivity in the Resting Brain: A Network Analysis of the Default Mode Hypothesis. Proc. Natl. Acad. Sci. USA 2003, 100, 253–258. [Google Scholar] [CrossRef]
- Liu, F.; Wang, Y.; Li, M.; Wang, W.; Li, R.; Zhang, Z.; Lu, G.; Chen, H. Dynamic Functional Network Connectivity in Idiopathic Generalized Epilepsy with Generalized Tonic-Clonic Seizure. Hum. Brain Mapp. 2017, 38, 957–973. [Google Scholar] [CrossRef] [PubMed]
- Orrù, G.; Storari, M.; Scano, A.; Piras, V.; Taibi, R.; Viscuso, D. Obstructive Sleep Apnea, Oxidative Stress, Inflammation and Endothelial Dysfunction-An Overview of Predictive Laboratory Biomarkers. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 6939–6948. [Google Scholar] [CrossRef]
- Seda, G.; Matwiyoff, G.; Parrish, J.S. Effects of Obstructive Sleep Apnea and CPAP on Cognitive Function. Curr. Neurol. Neurosci. Rep. 2021, 21, 32. [Google Scholar] [CrossRef] [PubMed]
- Posadas, T.; Oscullo, G.; Zaldívar, E.; Garcia-Ortega, A.; Gómez-Olivas, J.D.; Monteagudo, M.; Martínez-García, M.A. Treatment with CPAP in Elderly Patients with Obstructive Sleep Apnoea. J. Clin. Med. 2020, 9, 546. [Google Scholar] [CrossRef] [PubMed]
- Adnan, A.; Barnett, A.; Moayedi, M.; McCormick, C.; Cohn, M.; McAndrews, M.P. Distinct Hippocampal Functional Networks Revealed by Tractography-Based Parcellation. Brain Struct. Funct. 2016, 221, 2999–3012. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.L.; Barron, D.S.; Kirby, L.A.J.; Bottenhorn, K.L.; Hill, A.C.; Murphy, J.E.; Katz, J.S.; Salibi, N.; Eickhoff, S.B.; Fox, P.T. Neurofunctional Topography of the Human Hippocampus. Hum. Brain Mapp. 2015, 36, 5018–5037. [Google Scholar] [CrossRef]
- Fan, L.; Li, H.; Zhuo, J.; Zhang, Y.; Wang, J.; Chen, L.; Yang, Z.; Chu, C.; Xie, S.; Laird, A.R.; et al. The Human Brainnetome Atlas: A New Brain Atlas Based on Connectional Architecture. Cereb. Cortex 2016, 26, 3508–3526. [Google Scholar] [CrossRef]
- Beebe, D.W.; Gozal, D. Obstructive Sleep Apnea and the Prefrontal Cortex: Towards a Comprehensive Model Linking Nocturnal Upper Airway Obstruction to Daytime Cognitive and Behavioral Deficits. J. Sleep Res. 2002, 11, 1–16. [Google Scholar] [CrossRef]
- Joo, E.Y.; Tae, W.S.; Lee, M.J.; Kang, J.W.; Park, H.S.; Lee, J.Y.; Suh, M.; Hong, S.B. Reduced Brain Gray Matter Concentration in Patients with Obstructive Sleep Apnea Syndrome. Sleep 2010, 33, 235–241. [Google Scholar] [CrossRef]
- Bai, J.; Wen, H.; Tai, J.; Peng, Y.; Li, H.; Mei, L.; Ji, T.; Li, X.; Li, Y.; Ni, X.; et al. Altered Spontaneous Brain Activity Related to Neurologic and Sleep Dysfunction in Children With Obstructive Sleep Apnea Syndrome. Front. Neurosci. 2021, 15, 595412. [Google Scholar] [CrossRef]
- Jones, K.; Harrison, Y. Frontal Lobe Function, Sleep Loss and Fragmented Sleep. Sleep Med. Rev. 2001, 5, 463–475. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Shan, X.; Peng, Y.; Liu, G.; Guo, W.; Luo, H.; Li, H.; Zong, D.; Ouyang, R. Reduced Regional Homogeneity and Neurocognitive Impairment in Patients with Moderate-to-Severe Obstructive Sleep Apnea. Sleep Med. 2020, 75, 418–427. [Google Scholar] [CrossRef] [PubMed]
- Joseph, R. Frontal Lobe Psychopathology: Mania, Depression, Confabulation, Catatonia, Perseveration, Obsessive Compulsions, and Schizophrenia. Psychiatry 1999, 62, 138–172. [Google Scholar] [CrossRef] [PubMed]
- Castronovo, V.; Canessa, N.; Strambi, L.F.; Aloia, M.S.; Consonni, M.; Marelli, S.; Iadanza, A.; Bruschi, A.; Falini, A.; Cappa, S.F. Brain Activation Changes before and after PAP Treatment in Obstructive Sleep Apnea. Sleep 2009, 32, 1161–1172. [Google Scholar] [CrossRef]
- Zhou, L.; Tian, N.; Geng, Z.-J.; Wu, B.-K.; Dong, L.-Y.; Wang, M.-R. Diffusion Tensor Imaging Study of Brain Precentral Gyrus and Postcentral Gyrus during Normal Brain Aging Process. Brain Behav. 2020, 10, e01758. [Google Scholar] [CrossRef]
- Macey, P.M.; Haris, N.; Kumar, R.; Thomas, M.A.; Woo, M.A.; Harper, R.M. Obstructive Sleep Apnea and Cortical Thickness in Females and Males. PLoS ONE 2018, 13, e0193854. [Google Scholar] [CrossRef]
- Brouillette, R.T.; Thach, B.T. Control of Genioglossus Muscle Inspiratory Activity. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1980, 49, 801–808. [Google Scholar] [CrossRef]
- Song, X.; Roy, B.; Vacas, S.; Woo, M.A.; Kang, D.W.; Aysola, R.S.; Kumar, R. Brain Regional Homogeneity Changes after Short-Term Positive Airway Pressure Treatment in Patients with Obstructive Sleep Apnea. Sleep Med. 2022, 91, 12–20. [Google Scholar] [CrossRef]
- Zhang, Q.; Wang, D.; Qin, W.; Li, Q.; Chen, B.; Zhang, Y.; Yu, C. Altered Resting-State Brain Activity in Obstructive Sleep Apnea. Sleep 2013, 36, 651–659. [Google Scholar] [CrossRef]
- Santarnecchi, E.; Sicilia, I.; Richiardi, J.; Vatti, G.; Polizzotto, N.R.; Marino, D.; Rocchi, R.; Van De Ville, D.; Rossi, A. Altered Cortical and Subcortical Local Coherence in Obstructive Sleep Apnea: A Functional Magnetic Resonance Imaging Study. J. Sleep Res. 2013, 22, 337–347. [Google Scholar] [CrossRef]
- Barton, J.J.S. Disorder of Higher Visual Function. Curr. Opin. Neurol. 2011, 24, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Passaro, A.D.; Elmore, L.C.; Ellmore, T.M.; Leising, K.J.; Papanicolaou, A.C.; Wright, A.A. Explorations of Object and Location Memory Using FMRI. Front. Behav. Neurosci. 2013, 7, 105. [Google Scholar] [CrossRef] [PubMed]
- Joo, E.Y.; Tae, W.S.; Han, S.J.; Cho, J.-W.; Hong, S.B. Reduced Cerebral Blood Flow during Wakefulness in Obstructive Sleep Apnea-Hypopnea Syndrome. Sleep 2007, 30, 1515–1520. [Google Scholar] [CrossRef] [PubMed]
- Martin, A. The Representation of Object Concepts in the Brain. Annu. Rev. Psychol. 2007, 58, 25–45. [Google Scholar] [CrossRef]
- Op de Beeck, H.P.; Haushofer, J.; Kanwisher, N.G. Interpreting FMRI Data: Maps, Modules and Dimensions. Nat. Rev. Neurosci. 2008, 9, 123–135. [Google Scholar] [CrossRef]
- Caspers, J.; Zilles, K.; Amunts, K.; Laird, A.R.; Fox, P.T.; Eickhoff, S.B. Functional Characterization and Differential Coactivation Patterns of Two Cytoarchitectonic Visual Areas on the Human Posterior Fusiform Gyrus. Hum. Brain Mapp. 2014, 35, 2754–2767. [Google Scholar] [CrossRef]
- Zhang, W.; Wang, J.; Fan, L.; Zhang, Y.; Fox, P.T.; Eickhoff, S.B.; Yu, C.; Jiang, T. Functional Organization of the Fusiform Gyrus Revealed with Connectivity Profiles. Hum. Brain Mapp. 2016, 37, 3003–3016. [Google Scholar] [CrossRef]
- Lee, M.-H.; Sin, S.; Lee, S.; Park, H.; Wagshul, M.E.; Zimmerman, M.E.; Arens, R. Altered Cortical Structure Network in Children with Obstructive Sleep Apnea. Sleep 2022, 45, zsac030. [Google Scholar] [CrossRef]
- Luo, Y.-G.; Wang, D.; Liu, K.; Weng, J.; Guan, Y.; Chan, K.C.C.; Chu, W.C.W.; Shi, L. Brain Structure Network Analysis in Patients with Obstructive Sleep Apnea. PLoS ONE 2015, 10, e0139055. [Google Scholar] [CrossRef]
- Ji, T.; Ren, X.; Long, T.; Li, X.; Mei, L.; Ge, W.; Zhang, J.; Wang, S.; Guo, Y.; Xu, Z.; et al. Aberrant Topological Properties of Brain Functional Network in Children with Obstructive Sleep Apnea Derived from Resting-State FMRI. Brain Topogr. 2022, 36, 72–86. [Google Scholar] [CrossRef]
- Gutiérrez-Tobal, G.C.; Gomez-Pilar, J.; Kheirandish-Gozal, L.; Martín-Montero, A.; Poza, J.; Álvarez, D.; Del Campo, F.; Gozal, D.; Hornero, R. Pediatric Sleep Apnea: The Overnight Electroencephalogram as a Phenotypic Biomarker. Front. Neurosci. 2021, 15, 644697. [Google Scholar] [CrossRef] [PubMed]
- Maresky, H.S.; Shpirer, I.; Klar, M.M.; Levitt, M.; Sasson, E.; Tal, S. Continuous Positive Airway Pressure Alters Brain Microstructure and Perfusion Patterns in Patients with Obstructive Sleep Apnea. Sleep Med. 2019, 57, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Li, L.; Kong, L.; Li, P.; Zeng, Y.; Li, K.; Xie, W.; Shu, Y.; Liu, X.; Peng, D. Frequency-Specific Regional Homogeneity Alterations and Cognitive Function in Obstructive Sleep Apnea Before and After Short-Term Continuous Positive Airway Pressure Treatment. Nat. Sci. Sleep 2021, 13, 2221–2238. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Pre-CPAP | Post-CPAP | t-Value/ z-Value | p-Value |
|---|---|---|---|---|
| OSA Patients | OSA Patients | |||
| (N = 20) | (N = 20) | |||
| Sex (male/female) a | 18/2 | 18/2 | / | / |
| Age (years) a | 42.1 ± 8.2 | 42.1 ± 8.4 | / | / |
| BMI (kg/m2) a | 27.3 ± 4.2 | 27.0 ± 4.1 | 0.808 | 0.429 |
| Education (years) | 12.2 ± 3.1 | / | / | / |
| Nadir SaO2 (%) | 94.3 ± 3.5 | / | / | / |
| Mean SaO2 (%) | 97.7 ± 1.8 | / | / | / |
| SaO2 < 90% | 0.2 ± 0.2 | / | / | / |
| Sleep efficiency (%) | 89.9 ± 2.8 | / | / | / |
| AHI (events/h) a | 49.6 ± 21.3 | 4.0 ± 2.7 | 9.523 | <0.001 *** |
| PSQI, scores b | 7.3 ± 4.0 | 6.4 ± 3.4 | −0.700 | 0.484 |
| ESS, scores a | 10.6 ± 5.2 | 5.8 ± 2.8 | 3.879 | 0.001 ** |
| HAMA, scores a | 8.5 ± 5.1 | 3.2 ± 3.0 | 5.280 | <0.001 *** |
| HAMD, scores b | 4.9 ± 2.7 | 2.7 ± 1.3 | −2.562 | 0.010 * |
| MoCA, scores b | 23.8 ± 2.7 | 25.3 ± 3.1 | −2.274 | 0.013 * |
| MoCA: visual space and execution b | 4.1 ± 1.1 | 4.7 ± 0.5 | −2.221 | 0.026 * |
| MoCA: naming b | 2.9 ± 0.3 | 2.9 ± 0.3 | / | 1.000 |
| MoCA: delayed memory b | 1.7 ± 1.2 | 2.5 ± 1.5 | −2.984 | 0.003 ** |
| MoCA: attentional function b | 5.2 ± 1.3 | 5.4 ± 1.0 | −0.586 | 0.558 |
| MoCA: language b | 2.3 ± 0.9 | 2.3 ± 0.7 | −0.577 | 0.577 |
| MoCA: abstract b | 1.6 ± 0.7 | 1.7 ± 0.6 | −0.447 | 0.655 |
| MoCA: orientation b | 5.9 ± 0.5 | 5.9 ± 0.4 | / | 1.000 |
| Condition | Hippocampal Subregions | Brain Region | Voxel | MNI Coordinates of Peak Voxel | t-Value | ||
|---|---|---|---|---|---|---|---|
| X | Y | Z | |||||
| Post-CPAP > Pre-CPAP | mHipp-L | PreCG.L | 282 | −36 | 24 | 15 | 5.325 |
| Post-CPAP < Pre-CPAP | aHipp-R | FFG.L | 171 | −39 | −9 | −42 | −5.897 |
| SFG.R | 165 | 21 | 60 | 9 | −5.335 | ||
| SFG.L | 169 | −3 | 6 | 69 | −4.700 | ||
| MFG.L | 158 | −18 | −81 | 33 | −4.800 | ||
| MFG.R | 307 | 3 | −6 | 54 | −5.261 | ||
| LING.R | 217 | 3 | −90 | −3 | −4.275 | ||
| PoCG.R | 193 | 21 | −36 | 72 | −4.992 | ||
| aHipp-L | PoCG.L | 181 | −54 | −36 | 54 | −4.570 | |
| Condition | FC Value of Brain Areas | Clinical Assessments | r-Value | p-Value |
|---|---|---|---|---|
| Post-CPAP OSA | aHipp-R/SFG.R | PSQI b | 0.468 | 0.038 |
| aHipp-R/LING.R | MoCA: orientation b | −0.522 | 0.018 | |
| mHipp-L/PreCG.L | BMI a | 0.519 | 0.019 | |
| HAMD b | −0.519 | 0.019 | ||
| PSQI b | −0.528 | 0.017 | ||
| aHipp-R/FFG.L | AHI a | −0.480 | 0.032 | |
| Pre-CPAP OSA | aHipp-R/SFG.R | Min SaO2 (%) a | 0.495 | 0.027 |
| Mean SaO2 (%) b | 0.561 | 0.010 | ||
| aHipp-R/LING.R | AHI a | −0.472 | 0.036 | |
| Min SaO2 (%) a | 0.553 | 0.011 | ||
| Mean SaO2 (%) | 0.573 | 0.008 | ||
| aHipp-R/MFG.L | Min SaO2 (%) a | 0.593 | 0.006 | |
| Mean SaO2 (%) b | 0.640 | 0.002 | ||
| aHipp-R/MFG.R | Min SaO2 (%) a | 0.447 | 0.048 | |
| Mean SaO2 (%) b | 0.634 | 0.003 | ||
| aHipp-R/PoCG.R | AHI a | −0.454 | 0.044 | |
| Min SaO2 (%) a | 0.461 | 0.041 | ||
| Mean SaO2 (%) b | 0.496 | 0.026 | ||
| aHipp-R/SFG.L | HAMD b | −0.445 | 0.049 | |
| Min SaO2 (%) a | 0.450 | 0.047 | ||
| Mean SaO2 (%) b | 0.470 | 0.037 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, L.; Li, H.; Shu, Y.; Li, K.; Xie, W.; Zeng, Y.; Long, T.; Zeng, L.; Liu, X.; Peng, D. Changes in Functional Connectivity of Hippocampal Subregions in Patients with Obstructive Sleep Apnea after Six Months of Continuous Positive Airway Pressure Treatment. Brain Sci. 2023, 13, 838. https://doi.org/10.3390/brainsci13050838
Huang L, Li H, Shu Y, Li K, Xie W, Zeng Y, Long T, Zeng L, Liu X, Peng D. Changes in Functional Connectivity of Hippocampal Subregions in Patients with Obstructive Sleep Apnea after Six Months of Continuous Positive Airway Pressure Treatment. Brain Sciences. 2023; 13(5):838. https://doi.org/10.3390/brainsci13050838
Chicago/Turabian StyleHuang, Ling, Haijun Li, Yongqiang Shu, Kunyao Li, Wei Xie, Yaping Zeng, Ting Long, Li Zeng, Xiang Liu, and Dechang Peng. 2023. "Changes in Functional Connectivity of Hippocampal Subregions in Patients with Obstructive Sleep Apnea after Six Months of Continuous Positive Airway Pressure Treatment" Brain Sciences 13, no. 5: 838. https://doi.org/10.3390/brainsci13050838