
Altered Resting-State Functional Networks in Nondialysis Patients with Stage 5 Chronic Kidney Disease: A Graph–Theoretical Analysis
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
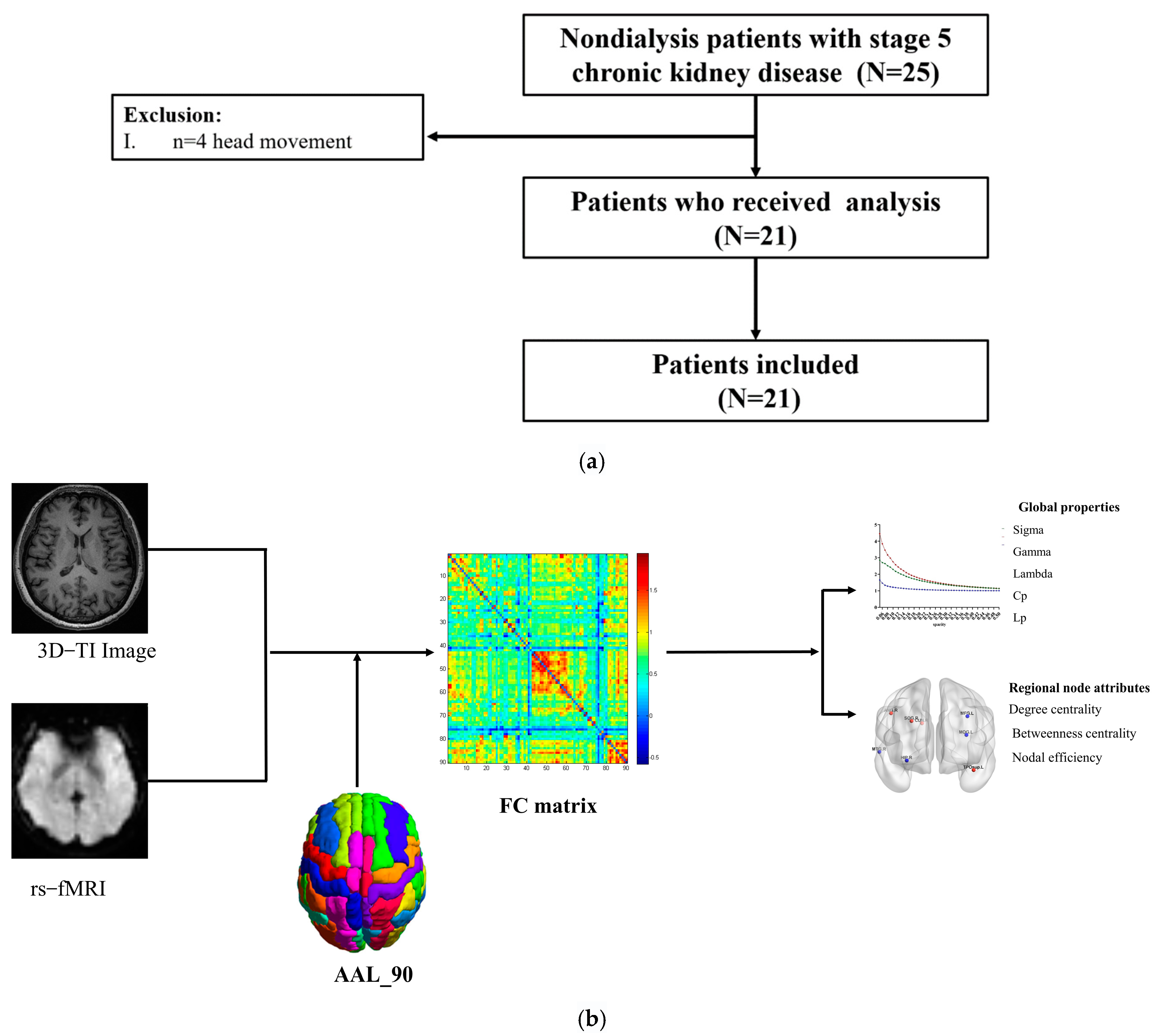
2.1. Participants
2.2. Clinical Evaluations and Laboratory Examination
2.3. MRI Data Acquisition
2.4. Data Preprocessing
2.5. Functional Network Construction
2.6. Network Analysis
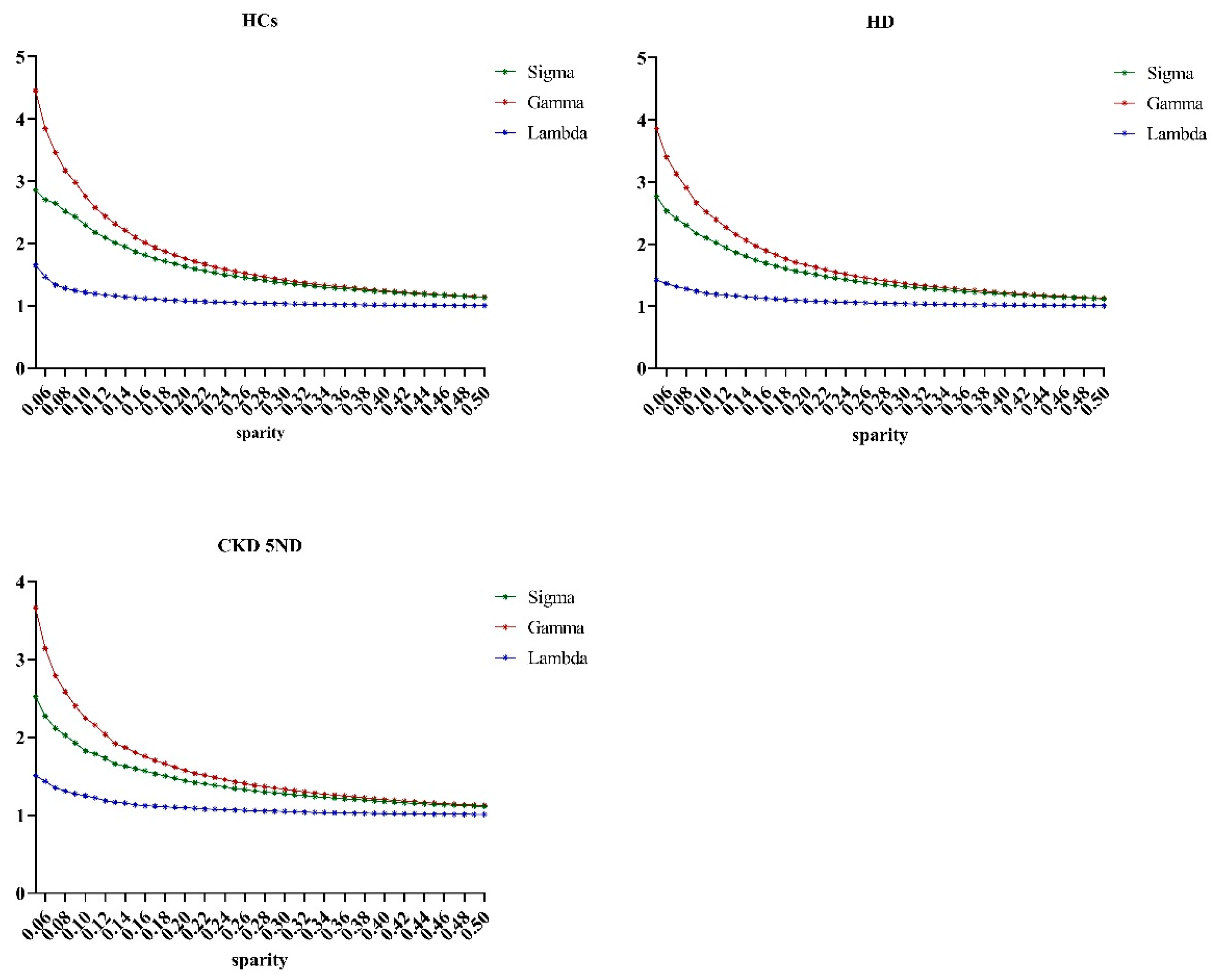
2.6.1. Threshold Selection
2.6.2. Network Metrics
2.7. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics
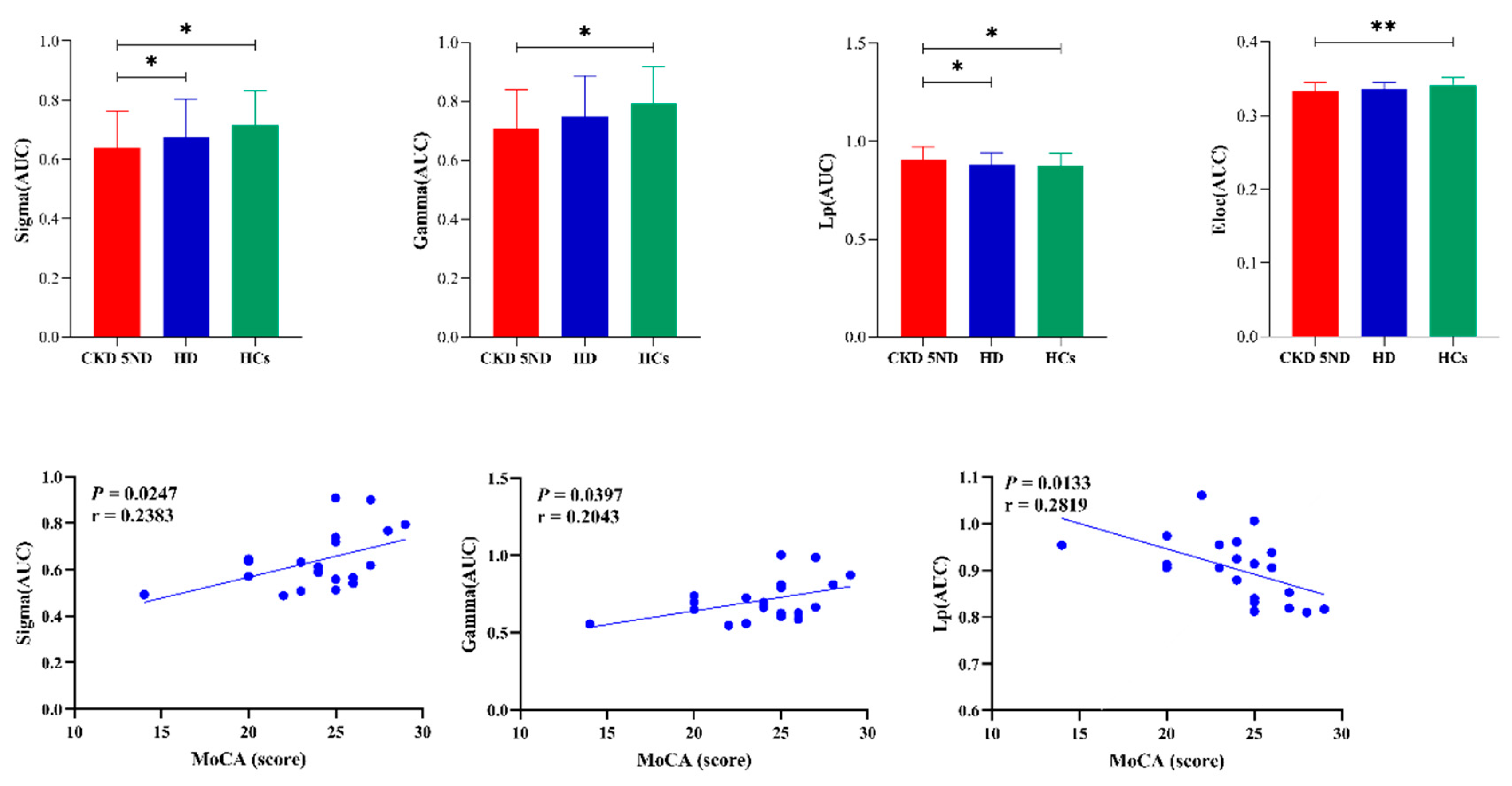
3.2. Alterations in Global Properties
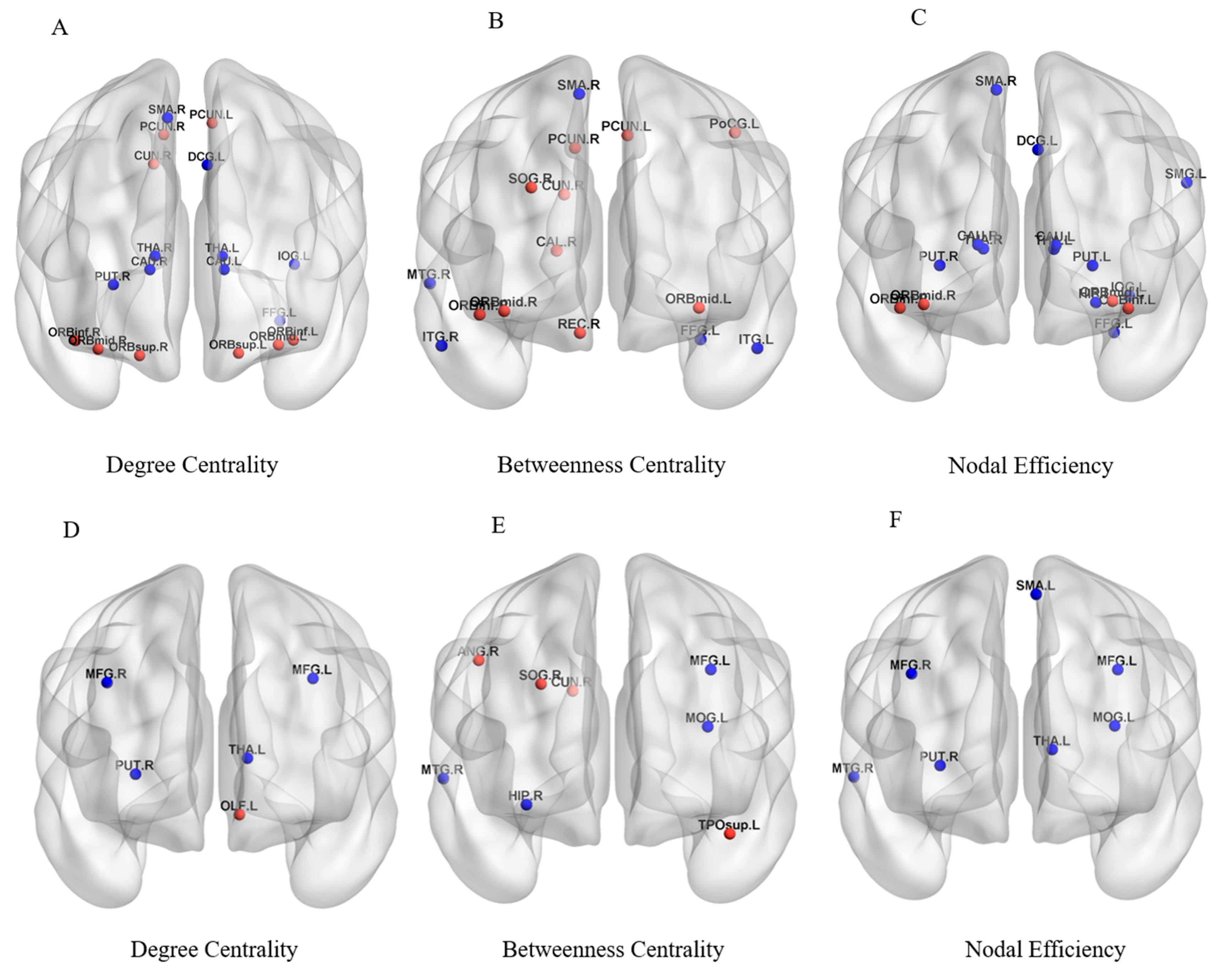
3.3. Alterations in Regional Node Attributes
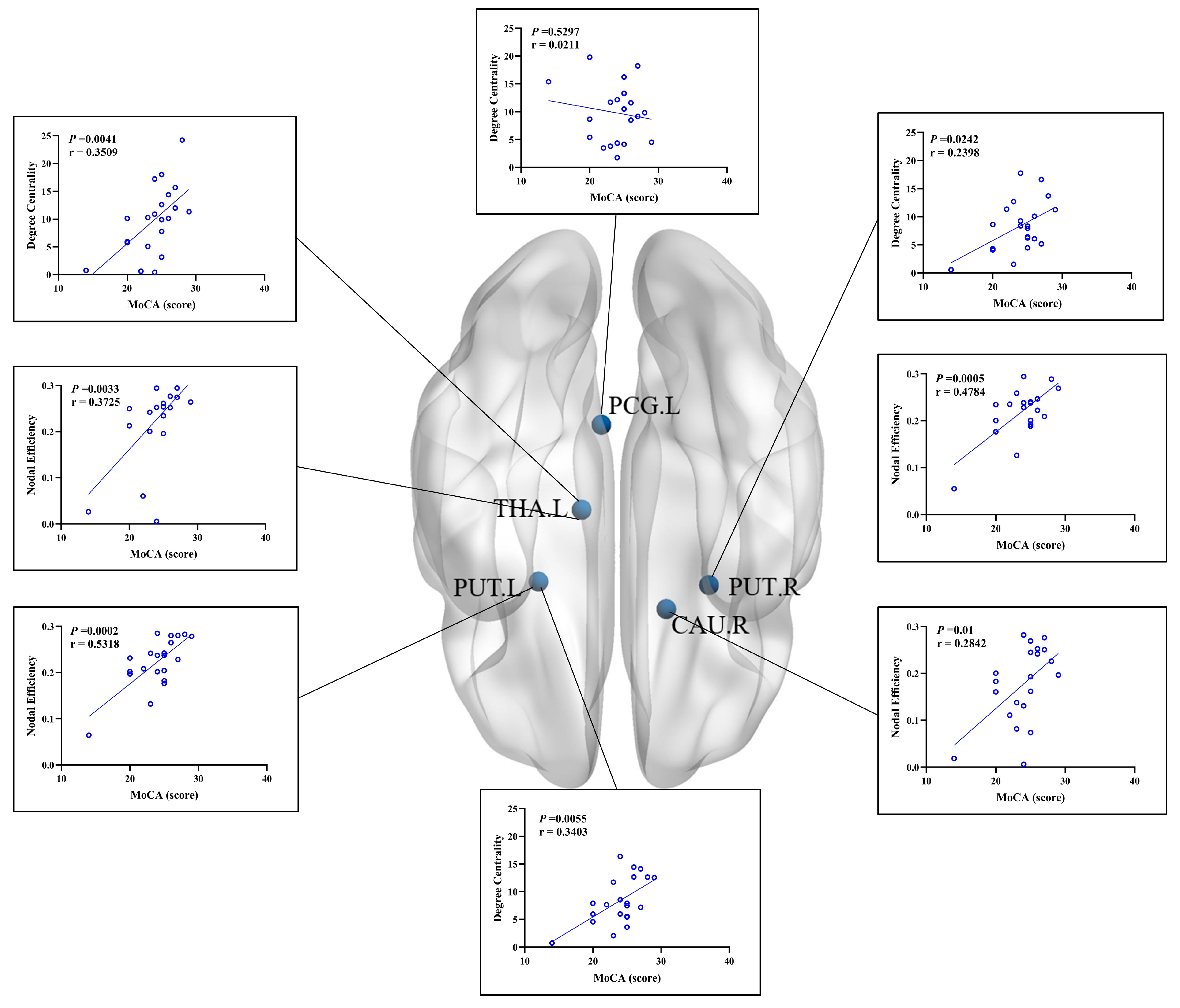
3.4. Relationships between Network Indicators and Clinical Variables
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| Abbreviation | Full Name |
| CKD5 ND | non-dialysis patients with stage 5 chronic kidney disease |
| HD | hemodialysis |
| HCs | healthy controls |
| ESRD | end-stage renal disease |
| CI | cognitive impairment |
| ASL | arterial spin labeling |
| QSM | quantitative susceptibility mapping |
| rs-fMRI | resting-state functional magnetic resonance imaging |
| MoCA | montreal cognitive assessment |
| AAL | automated anatomical labeling |
| Lp | characteristic path length |
| Cp | clustering coefficients |
| gamma | normalized clustering coefficient |
| lambda | normalized characteristic path length |
| AUC | area under the receiver-operating characteristic curve |
| sigma | small-worldness |
| Eg | Global efficiency |
| Eloc | local efficiency |
| SMG | supramarginal gyrus |
| OLF | olfactory cortex |
| TPOsup | superior temporal gyrus pars temporal pole |
| DCG | Median cingulate and paracingulate gyri |
| SMA | supplementary motor area |
| IOG | inferior occipital gyrus |
| FFG | fusiform gyrus |
| CAU | caudate nucleus |
| PUT | lenticular nucleus, putamen |
| THA | thalamus |
| ORBsup | orbital superior frontal gyrus |
| ORBmid | orbital middle frontal gyrus |
| ORBinf | orbital inferior frontal gyrus |
| PCUN | precuneus |
| CUN | cuneus |
| MTG | middle temporal gyrus |
| ITG | inferior temporal gyrus |
| REC | right gyrus rectus |
| HIP | hippocampus |
| CAL | surrounding cortex |
| SOG | superior occipital gyrus |
| PoCG | postcentral gyrus |
| MOG | middle occipital gyrus |
| ANG | angular gyrus |
| PCG.L | posterior cingulate gyrus |
References
- Stevens, P.E.; Levin, A.; Kidney Disease: Improving Global Outcomes Chronic Kidney Disease Guideline Development Work Group Members. Evaluation and Management of Chronic Kidney Disease: Synopsis of the Kidney Disease: Improving Global Outcomes 2012 Clinical Practice Guideline. Ann. Intern. Med. 2013, 158, 825–830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viggiano, D.; Wagner, C.A.; Martino, G.; Nedergaard, M.; Zoccali, C.; Unwin, R.; Capasso, G. Mechanisms of cognitive dysfunction in CKD. Nat. Rev. Nephrol. 2020, 16, 452–469. [Google Scholar] [CrossRef] [PubMed]
- Harhay, M.N.; Xie, D.; Zhang, X.; Hsu, C.Y.; Vittinghoff, E.; Go, A.S.; Sozio, S.M.; Blumenthal, J.; Seliger, S.; Chen, J.; et al. Cognitive Impairment in Non-Dialysis-Dependent CKD and the Transition to Dialysis: Findings From the Chronic Renal Insufficiency Cohort (CRIC) Study. Am. J. Kidney Dis. 2018, 72, 499–508. [Google Scholar] [CrossRef] [Green Version]
- Jha, V.; Garcia-Garcia, G.; Iseki, K.; Li, Z.; Naicker, S.; Plattner, B.; Saran, R.; Wang, A.Y.-M.; Yang, C.-W. Chronic kidney disease: Global dimension and perspectives. Lancet 2013, 382, 260–272. [Google Scholar] [CrossRef]
- Watts, D.J.; Strogatz, S.H. Collective dynamics of ‘small-world’ networks. Nature 1998, 393, 440–442. [Google Scholar] [CrossRef]
- Jin, M.; Wang, L.; Wang, H.; Han, X.; Diao, Z.; Guo, W.; Yang, Z.; Ding, H.; Wang, Z.; Zhang, P.; et al. Structural and Functional Alterations in Hemodialysis Patients: A Voxel-Based Morphometry and Functional Connectivity Study. Front. Hum. Neurosci. 2020, 14, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, R.; Liu, K.; Yang, L.; Zhou, T.; Qian, S.; Li, B.; Peng, Z.; Li, M.; Sang, S.; Jiang, Q.; et al. Reduced white matter integrity and cognitive deficits in maintenance hemodialysis ESRD patients: A diffusion-tensor study. Eur. Radiol. 2015, 25, 661–668. [Google Scholar] [CrossRef]
- Cheng, B.C.; Chen, P.C.; Chen, P.C.; Lu, C.H.; Huang, Y.C.; Chou, K.H.; Li, S.H.; Lin, A.N.; Lin, W.C. Decreased cerebral blood flow and improved cognitive function in patients with end-stage renal disease after peritoneal dialysis: An arterial spin-labelling study. Eur. Radiol. 2019, 29, 1415–1424. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Han, X.; Jin, M.; Wang, L.Y.; Diao, Z.L.; Guo, W.; Zhang, P.; Wang, Z.; Ding, H.Y.; Lv, H.; et al. Different iron deposition patterns in hemodialysis patients with and without restless legs syndrome: A quantitative susceptibility mapping study. Sleep Med. 2020, 69, 34–40. [Google Scholar] [CrossRef]
- Chen, H.J.; Qiu, J.; Fu, Q.; Chen, F. Alterations of Spontaneous Brain Activity in Hemodialysis Patients. Front. Hum. Neurosci. 2020, 14, 278. [Google Scholar] [CrossRef]
- Gu, Z.; Lu, H.; Zhou, H.; Zhang, J.; Xing, W. The relationship between abnormal cortical activity in the anterior cingulate gyrus and cognitive dysfunction in patients with end-stage renal disease: A fMRI study on the amplitude of low-frequency fluctuations. Ann. Palliat. Med. 2020, 9, 4187–4193. [Google Scholar] [CrossRef]
- Guo, H.; Liu, W.; Li, H.; Yang, J. Structural and Functional Brain Changes in Hemodialysis Patients with End-Stage Renal Disease: DTI Analysis Results and ALFF Analysis Results. Int. J. Nephrol. Renov. Dis. 2021, 14, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Su, H.; Fu, S.; Liu, M.; Yin, Y.; Hua, K.; Meng, S.; Jiang, G.; Quan, X. Altered Spontaneous Brain Activity and Functional Integration in Hemodialysis Patients With End-Stage Renal Disease. Front. Neurol. 2021, 12, 801336. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.J.; Qi, R.F.; Kong, X.; Wen, J.Q.; Liang, X.; Zhang, Z.; Li, X.; Lu, G.M.; Zhang, L.J. The impact of hemodialysis on cognitive dysfunction in patients with end-stage renal disease: A resting-state functional MRI study. Metab. Brain Dis. 2015, 30, 1247–1256. [Google Scholar] [CrossRef]
- Wu, B.; Li, X.; Zhang, M.; Zhang, F.; Long, X.; Gong, Q.; Jia, Z. Disrupted brain functional networks in patients with end-stage renal disease undergoing hemodialysis. J. Neurosci. Res. 2020, 98, 2566–2578. [Google Scholar] [CrossRef]
- Park, B.S.; Kim, S.E.; Lee, H.J.; Kim, Y.W.; Kim, I.H.; Park, J.H.; Park, S.H.; Lee, Y.J.; Seo, S.A.; Park, K.M. Alterations in Structural and Functional Connectivities in Patients with End-Stage Renal Disease. J. Clin. Neurol. 2020, 16, 390–400. [Google Scholar] [CrossRef]
- Biswal, B.B.; Mennes, M.; Zuo, X.N.; Gohel, S.; Kelly, C.; Smith, S.M.; Beckmann, C.F.; Adelstein, J.S.; Buckner, R.L.; Colcombe, S.; et al. Toward discovery science of human brain function. Proc. Natl. Acad. Sci. USA 2010, 107, 4734–4739. [Google Scholar] [CrossRef] [Green Version]
- Azeem, M.; Nadeem, M.F. Metric-based resolvability of polycyclic aromatic hydrocarbons. Eur. Phys. J. Plus 2021, 136, 395. [Google Scholar] [CrossRef]
- Azeem, M.; Jamil, M.K.; Shang, Y. Notes on the Localization of Generalized Hexagonal Cellular Networks. Mathematics 2023, 11, 844. [Google Scholar] [CrossRef]
- Zhao, X.; Liu, Y.; Wang, X.; Liu, B.; Xi, Q.; Guo, Q.; Jiang, H.; Jiang, T.; Wang, P. Disrupted small-world brain networks in moderate Alzheimer’s disease: A resting-state FMRI study. PLoS ONE 2012, 7, e33540. [Google Scholar] [CrossRef] [Green Version]
- Liu, F.; Zhuo, C.; Yu, C. Altered Cerebral Blood Flow Covariance Network in Schizophrenia. Front. Neurosci. 2016, 10, 308. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.F.; Gu, P.; Zhang, J.; Qi, R.; de Veer, M.; Zheng, G.; Xu, Q.; Liu, Y.; Lu, G.M.; Zhang, L.J. Deteriorated functional and structural brain networks and normally appearing functional-structural coupling in diabetic kidney disease: A graph theory-based magnetic resonance imaging study. Eur. Radiol. 2019, 29, 5577–5589. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wang, X.; Xia, M.; Liao, X.; Evans, A.; He, Y. GRETNA: A graph theoretical network analysis toolbox for imaging connectomics. Front. Hum. Neurosci. 2015, 9, 386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashburner, J. A fast diffeomorphic image registration algorithm. Neuroimage 2007, 38, 95–113. [Google Scholar] [CrossRef] [PubMed]
- Tzourio-Mazoyer, N.; Landeau, B.; Papathanassiou, D.; Crivello, F.; Etard, O.; Delcroix, N.; Mazoyer, B.; Joliot, M. Automated anatomical labeling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject brain. Neuroimage 2002, 15, 273–289. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Wang, J.; Wu, Q.; Kuang, W.; Huang, X.; He, Y.; Gong, Q. Disrupted brain connectivity networks in drug-naive, first-episode major depressive disorder. Biol. Psychiatry 2011, 70, 334–342. [Google Scholar] [CrossRef]
- He, Y.; Dagher, A.; Chen, Z.; Charil, A.; Zijdenbos, A.; Worsley, K.; Evans, A. Impaired small-world efficiency in structural cortical networks in multiple sclerosis associated with white matter lesion load. Brain 2009, 132, 3366–3379. [Google Scholar] [CrossRef] [Green Version]
- Bassett, D.S.; Bullmore, E.T. Small-World Brain Networks Revisited. Neuroscientist 2017, 23, 499–516. [Google Scholar] [CrossRef] [Green Version]
- Achard, S.; Bullmore, E. Efficiency and cost of economical brain functional networks. PLoS Comput. Biol. 2007, 3, e17. [Google Scholar] [CrossRef]
- Sporns, O.; Honey, C.J. Small worlds inside big brains. Proc. Natl. Acad. Sci. USA 2006, 103, 19219–19220. [Google Scholar] [CrossRef] [Green Version]
- Latora, V.; Marchiori, M. Efficient behavior of small-world networks. Phys. Rev. Lett. 2001, 87, 198701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bassett, D.S.; Bullmore, E. Small-world brain networks. Neuroscientist 2006, 12, 512–523. [Google Scholar] [CrossRef]
- Rubinov, M.; Sporns, O. Complex network measures of brain connectivity: Uses and interpretations. Neuroimage 2010, 52, 1059–1069. [Google Scholar] [CrossRef] [PubMed]
- Miglinas, M.; Cesniene, U.; Janusaite, M.M.; Vinikovas, A. Cerebrovascular Disease and Cognition in Chronic Kidney Disease Patients. Front. Cardiovasc. Med. 2020, 7, 96. [Google Scholar] [CrossRef]
- Ghandili, M.; Munakomi, S. Neuroanatomy, Putamen. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Chai, C.; Yan, S.; Chu, Z.; Wang, T.; Wang, L.; Zhang, M.; Zuo, C.; Haacke, E.M.; Xia, S.; Shen, W. Quantitative measurement of brain iron deposition in patients with haemodialysis using susceptibility mapping. Metab. Brain Dis. 2015, 30, 563–571. [Google Scholar] [CrossRef]
- Jin, M.; Wang, L.; Wang, H.; Han, X.; Diao, Z.; Guo, W.; Yang, Z.; Ding, H.; Wang, Z.; Zhang, P.; et al. Altered resting-state functional networks in patients with hemodialysis: A graph-theoretical based study. Brain Imaging Behav. 2021, 15, 833–845. [Google Scholar] [CrossRef]
- Chou, M.C.; Ko, C.H.; Chang, J.M.; Hsieh, T.J. Disruptions of brain structural network in end-stage renal disease patients with long-term hemodialysis and normal-appearing brain tissues. J. Neuroradiol. 2019, 46, 256–262. [Google Scholar] [CrossRef] [PubMed]
- Hunerli, D.; Emek-Savas, D.D.; Cavusoglu, B.; Donmez Colakoglu, B.; Ada, E.; Yener, G.G. Mild cognitive impairment in Parkinson’s disease is associated with decreased P300 amplitude and reduced putamen volume. Clin. Neurophysiol. 2019, 130, 1208–1217. [Google Scholar] [CrossRef]
- Chai, C.; Wang, H.; Liu, S.; Chu, Z.Q.; Li, J.; Qian, T.; Haacke, E.M.; Xia, S.; Shen, W. Increased iron deposition of deep cerebral gray matter structures in hemodialysis patients: A longitudinal study using quantitative susceptibility mapping. J. Magn. Reson. Imaging 2019, 49, 786–799. [Google Scholar] [CrossRef]
- Gu, W.; He, R.; Su, H.; Ren, Z.; Zhang, L.; Yuan, H.; Zhang, M.; Ma, S. Changes in the Shape and Volume of Subcortical Structures in Patients With End-Stage Renal Disease. Front. Hum. Neurosci. 2021, 15, 778807. [Google Scholar] [CrossRef]
- Wang, Z.; Jia, X.; Liang, P.; Qi, Z.; Yang, Y.; Zhou, W.; Li, K. Changes in thalamus connectivity in mild cognitive impairment: Evidence from resting state fMRI. Eur. J. Radiol. 2012, 81, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Coleman, K.K.; Coleman, B.L.; MacKinley, J.D.; Pasternak, S.H.; Finger, E.C. Detection and Differentiation of Frontotemporal Dementia and Related Disorders From Alzheimer Disease Using the Montreal Cognitive Assessment. Alzheimer Dis. Assoc. Disord. 2016, 30, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Dalrymple-Alford, J.C.; MacAskill, M.R.; Nakas, C.T.; Livingston, L.; Graham, C.; Crucian, G.P.; Melzer, T.R.; Kirwan, J.; Keenan, R.; Wells, S.; et al. The MoCA: Well-suited screen for cognitive impairment in Parkinson disease. Neurology 2010, 75, 1717–1725. [Google Scholar] [CrossRef]
- Zietemann, V.; Georgakis, M.K.; Dondaine, T.; Müller, C.; Mendyk, A.M.; Kopczak, A.; Hénon, H.; Bombois, S.; Wollenweber, F.A.; Bordet, R.; et al. Early MoCA predicts long-term cognitive and functional outcome and mortality after stroke. Neurology 2018, 91, e1838–e1850. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CKD5 ND (n = 21) | HD (n = 32) | HCs (n = 32) | p-Value | |
|---|---|---|---|---|
| Age (years) | 48.9 ± 14.9 (21–76) | 53.4 ± 9.7(32–66) | 51.2 ± 10.3(30–65) | 0.533 a |
| Gender (male/female) | 15/6 | 21/11 | 17/15 | 0.359 b |
| Education (years) | 11.9 ± 3.3 (5–20) | 11.1 ± 3.5 (5–17) | 12.3 ± 3.2 (6–19) | 0.283 a |
| HD duration (months) | NA | 101.2 ± 21.3 (41–200) | NA | NA |
| Urea (mmol/L) | 32.47 ± 9.15 | 20.34 ±4.57 | NA | 0.001 c |
| Creatinine (μmol/L) | 858.7.1 ± 317.6 | 391.3 ± 73.32 | NA | 0.001 c |
| Phosphate (mmol/L) | 2.06 ± 0.55 | 1.99 ± 0.52 | NA | 0.604 c |
| Ca2+ (mmol/L) | 2.09 ± 0.25 | 2.22 ± 0.25 | NA | 0.003 c |
| Parathyroid hormone (pg/mL) | 192.9 ± 146.2 | 237.8 ± 212.3 | NA | 0.375 c |
| Hemoglobin (g/L) | 94.3 ± 16.4 | 117.1 ± 12.2 | NA | 0.001 c |
| Ferritin (ng/mL) | 117.9 ± 121.3 | 199.6 ± 142.4 | NA | 0.055 c |
| Serum iron (μmol/L) | 14.1 ± 8.5 | 14.2 ± 5.2 | NA | 0.988 c |
| MoCA scores | 24.5 ± 4.1 | 22.4 ± 2.8 | NA | 0.041 c |
| Brain Regions | Degree Centrality | Nodal Betweenness Centrality | Nodal Efficiency | |||
|---|---|---|---|---|---|---|
| t Values | p Values | t Values | p Values | t Values | p Values | |
| CKD5 ND > HCs | ||||||
| ORBsup.L | 2.0886 | 0.0418 | 7.7503 | 0.4419 | 1.4607 | 0.1502 |
| ORBsup.R | 2.4089 | 0.0197 | 1.5116 | 0.1368 | 1.9220 | 0.0602 |
| ORBmid.L | 4.3239 | 0.0001 | 2.6948 | 0.0095 | 3.1636 | 0.0026 |
| ORBmid.R | 3.7782 | 0.0004 | 2.1214 | 0.0388 | 2.8810 | 0.0058 |
| ORBinf.L | 3.0087 | 0.0041 | 1.3395 | 0.1863 | 2.1590 | 0.0356 |
| ORBinf.R | 2.9957 | 0.0042 | 3.2584 | 0.0020 | 2.1744 | 0.0343 |
| REC.R | 1.9195 | 0.0605 | 2.1339 | 0.0377 | 1.1891 | 0.2399 |
| CAL.R | 1.8520 | 0.0698 | 2.6670 | 0.0102 | 1.5296 | 0.1323 |
| CUN.R | 2.1206 | 0.0388 | 2.9363 | 0.0050 | 1.7570 | 0.0849 |
| SOG.R | 1.2791 | 0.2067 | 2.0377 | 0.0468 | 6.4938 | 0.5190 |
| PoCG.L | 1.3888 | 0.1709 | 2.7223 | 0.0088 | 1.2125 | 0.2309 |
| PCUN.L | 2.1500 | 0.0363 | 2.6462 | 0.0108 | 1.3741 | 0.1754 |
| PCUN.R | 2.9052 | 0.0054 | 2.7126 | 0.0091 | 1.9510 | 0.0566 |
| CKD5 ND < HCs | ||||||
| SMA.R | −2.4378 | 0.0183 | −2.8074 | 0.0071 | −2.9118 | 0.0053 |
| DCG.L | −2.0138 | 0.0493 | −1.7628 | 0.0839 | −2.4969 | 0.0158 |
| HIP.L | −1.6497 | 0.1051 | −8.8442 | 0.3806 | −2.0812 | 0.0425 |
| IOG.L | −2.1583 | 0.0356 | −8.6682 | 0.3901 | −2.3987 | 0.0201 |
| FFG.L | −2.3614 | 0.0221 | −2.2797 | 0.0268 | −2.8041 | 0.0071 |
| SMG.L | −1.4213 | 0.1613 | −8.1156 | 0.4208 | −2.0512 | 0.0454 |
| CAU.L | −2.5745 | 0.0130 | 1.7117 | 0.8648 | −3.2442 | 0.0021 |
| CAU.R | −2.1955 | 0.0327 | −1.4915 | 0.1420 | −2.9940 | 0.0042 |
| PUT.L | −1.9589 | 0.0556 | −8.3522 | 0.4075 | −2.4671 | 0.0170 |
| PUT.R | −2.8171 | 0.0069 | −1.3416 | 0.1857 | −3.2004 | 0.0024 |
| THA.L | −2.3232 | 0.0242 | −1.3092 | 0.1963 | −2.3190 | 0.0244 |
| THA.R | −2.6136 | 0.0117 | −1.2456 | 0.2186 | −2.5073 | 0.0154 |
| MTG.R | −7.6067 | 0.4504 | −2.6950 | 0.0095 | −1.4152 | 0.1631 |
| ITG.L | −1.4478 | 0.1538 | −2.7404 | 0.0084 | −1.9122 | 0.0615 |
| ITG.R | −1.3108 | 0.1958 | −2.1112 | 0.0397 | −1.7888 | 0.0796 |
| CKD5 ND > HD | ||||||
| OLF.L | 2.0996 | 0.0407 | 1.7261 | 0.0904 | 1.7869 | 0.0799 |
| CUN.R | 1.5499 | 0.1274 | 2.0805 | 0.0425 | 1.3690 | 0.1770 |
| SOG.R | 1.3428 | 0.1853 | 2.5580 | 0.0135 | 1.1130 | 0.2709 |
| ANG.L | 2.0182 | 0.0488 | ||||
| TPOsup.L | 1.6052 | 0.1146 | 3.0474 | 0.0037 | 1.2585 | 0.2139 |
| CKD5 ND < HD | ||||||
| MFG.L | −2.2126 | 0.0314 | −2.9424 | 0.0049 | −2.6910 | 0.0096 |
| MFG.R | −2.3390 | 0.0233 | −3.4173 | 0.7340 | −2.7524 | 0.0082 |
| SMA.L | −1.6947 | 0.0962 | −1.8227 | 0.0742 | −2.1073 | 0.0400 |
| HIP.R | −2.5164 | 0.0150 | −3.6725 | 0.7150 | ||
| MOG.L | −1.8222 | 0.0743 | −2.0290 | 0.0477 | −2.1516 | 0.0362 |
| PUT.R | −2.1026 | 0.0405 | −1.1212 | 0.2675 | −2.4562 | 0.0175 |
| THA.L | −2.2948 | 0.0259 | −1.4876 | 0.1430 | −2.3097 | 0.0250 |
| MTG.R | −1.7756 | 0.0818 | −2.0977 | 0.0409 | −2.2811 | 0.0267 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, L.; Liu, X.; Yang, W.; Chen, Q.; Lv, H.; Yang, Z.; Liu, W.; Wang, H.; Wang, Z. Altered Resting-State Functional Networks in Nondialysis Patients with Stage 5 Chronic Kidney Disease: A Graph–Theoretical Analysis. Brain Sci. 2023, 13, 628. https://doi.org/10.3390/brainsci13040628
Song L, Liu X, Yang W, Chen Q, Lv H, Yang Z, Liu W, Wang H, Wang Z. Altered Resting-State Functional Networks in Nondialysis Patients with Stage 5 Chronic Kidney Disease: A Graph–Theoretical Analysis. Brain Sciences. 2023; 13(4):628. https://doi.org/10.3390/brainsci13040628
Chicago/Turabian StyleSong, Lijun, Xu Liu, Wenbo Yang, Qian Chen, Han Lv, Zhenghan Yang, Wenhu Liu, Hao Wang, and Zhenchang Wang. 2023. "Altered Resting-State Functional Networks in Nondialysis Patients with Stage 5 Chronic Kidney Disease: A Graph–Theoretical Analysis" Brain Sciences 13, no. 4: 628. https://doi.org/10.3390/brainsci13040628