
The Comorbidity of Depression and Anxiety Symptoms in Tinnitus Sufferers: A Network Analysis
 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Evaluating Depression and Anxiety Symptoms
2.3. Network Analysis
2.3.1. Network Estimation and Visualization
2.3.2. Expected Influence and Predictability Analysis
2.3.3. Network Accuracy and Stability
3. Results
3.1. Basic Descriptive Characteristics of Depression and Anxiety Severity in Tinnitus Sufferers
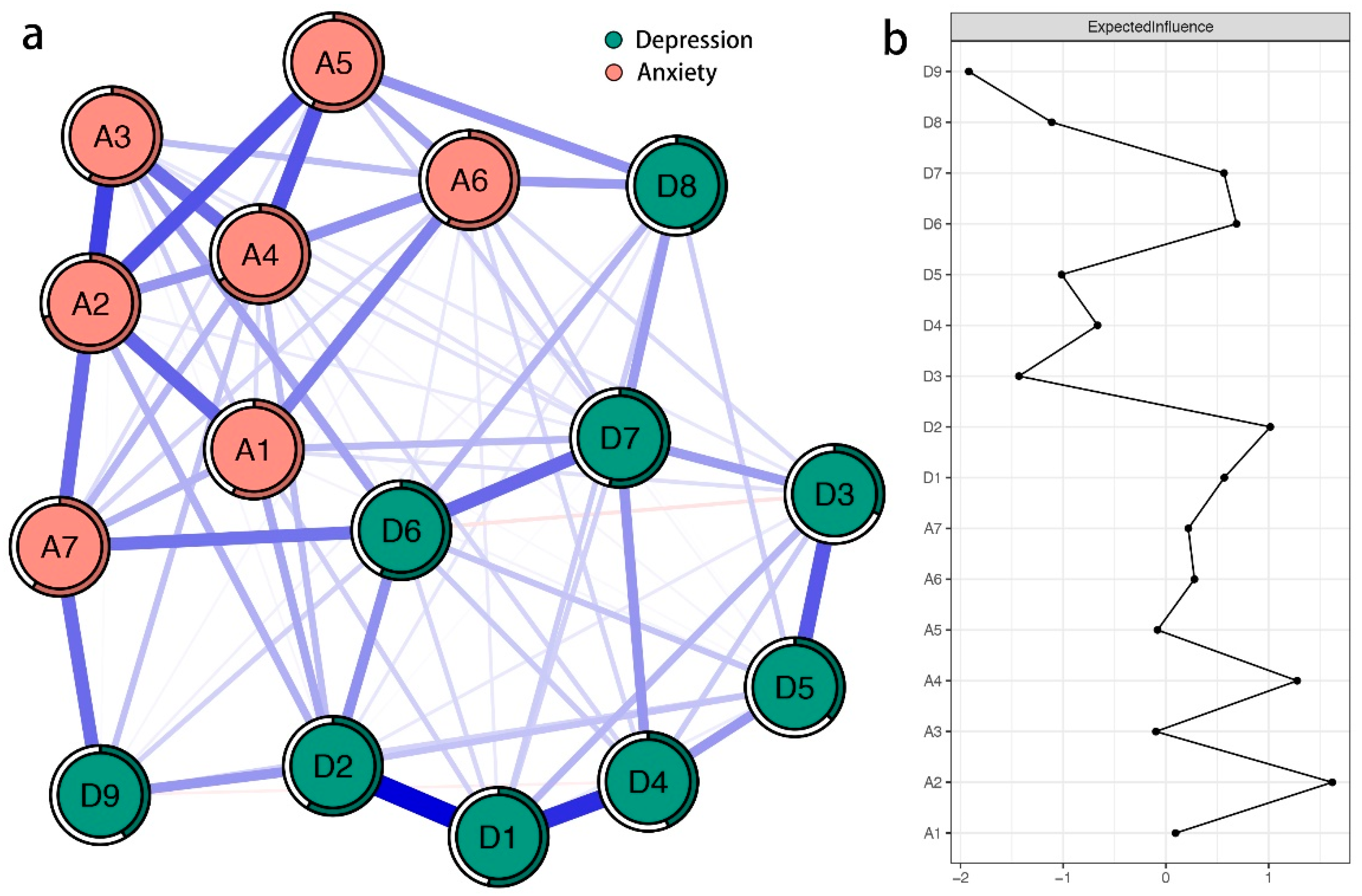
3.2. Network Structure of Depression and Anxiety Symptoms in Tinnitus Sufferers
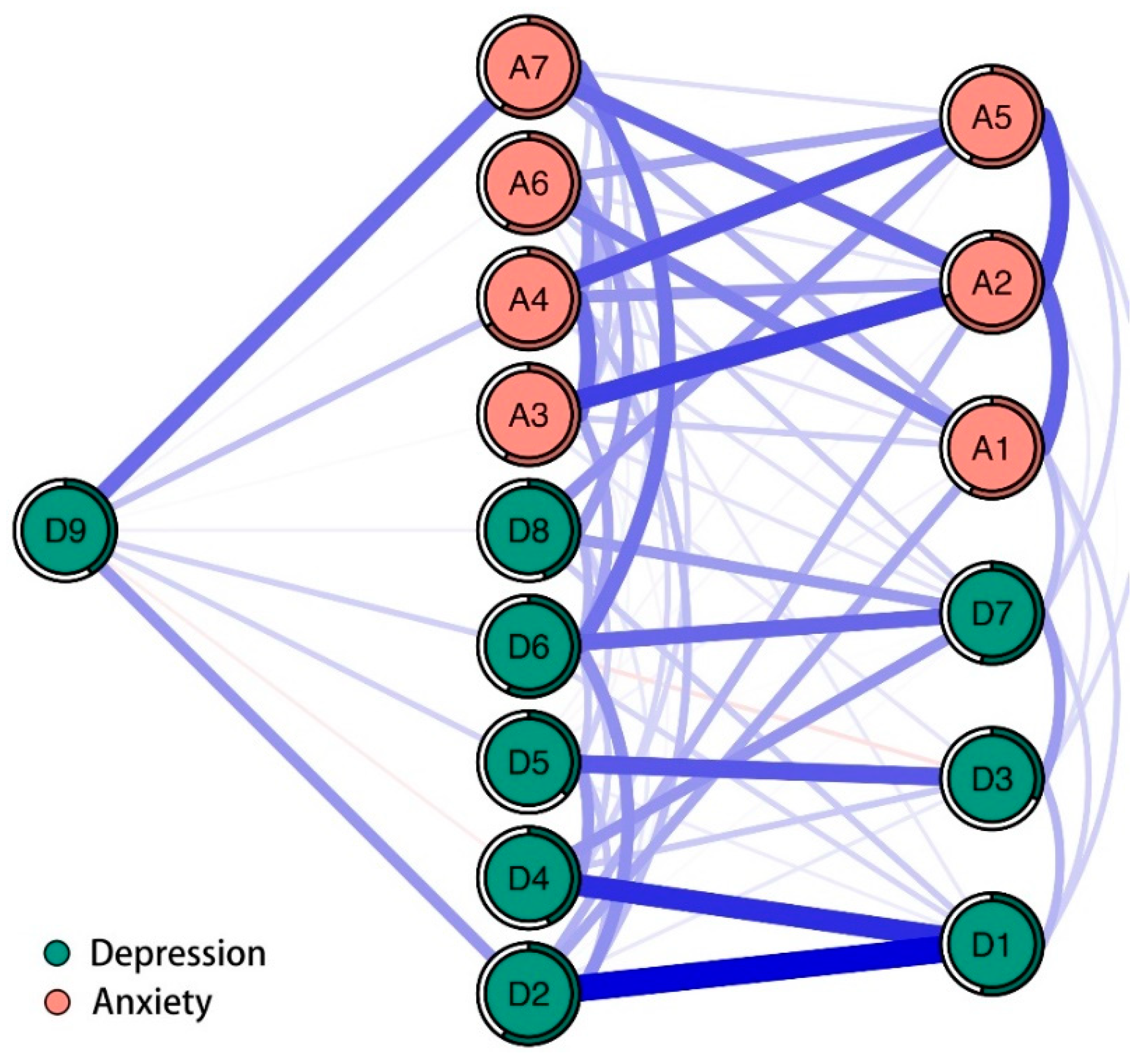
3.3. Bridge Symptoms of Depression and Anxiety in Tinnitus Sufferers
3.4. Flow Network of Suicidal Ideation with Depression and Anxiety Symptoms in Tinnitus Sufferers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baguley, D.; McFerran, D.; Hall, D. Tinnitus. Lancet 2013, 382, 1600–1607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCormack, A.; Edmondson-Jones, M.; Somerset, S.; Hall, D. A Systematic Review of the Reporting of Tinnitus Prevalence and Severity. Hear. Res. 2016, 337, 70–79. [Google Scholar] [CrossRef] [PubMed]
- Parving, A.; Hein, H.O.; Suadicani, P.; Ostri, B.; Gyntelberg, F. Epidemiology of Hearing Disorders. Some Factors Affecting Hearing. The Copenhagen Male Study. Scand. Audiol. 1993, 22, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Fujii, K.; Nagata, C.; Nakamura, K.; Kawachi, T.; Takatsuka, N.; Oba, S.; Shimizu, H. Prevalence of Tinnitus in Community-Dwelling Japanese Adults. J. Epidemiol. 2011, 21, 299–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCormack, A.; Edmondson-Jones, M.; Fortnum, H.; Dawes, P.; Middleton, H.; Munro, K.J.; Moore, D.R. The Prevalence of Tinnitus and the Relationship with Neuroticism in a Middle-Aged UK Population. J. Psychosom. Res. 2014, 76, 56–60. [Google Scholar] [CrossRef]
- Tang, D.; Li, H.; Chen, L. Advances in Understanding, Diagnosis, and Treatment of Tinnitus. Adv. Exp. Med. Biol. 2019, 1130, 109–128. [Google Scholar]
- Mantello, E.B.; Lupoli, L.M.; Rodrigues, P.C.P.; Cavalcante, J.M.S.; Massuda, E.T.; Anastasio, A.R.T. Functional Impact of Tinnitus in Patients with Hearing Loss. Int. Arch. Otorhinolaryngol. 2020, 24, e191–e197. [Google Scholar] [CrossRef] [Green Version]
- Cheng, Y.F.; Xirasagar, S.; Kuo, N.W.; Lin, H.C. Tinnitus and risk of attempted suicide: A one year follow-up study. J. Affect. Disord. 2023, 322, 141–145. [Google Scholar] [CrossRef]
- Tailor, B.V.; Thompson, R.E.; Nunney, I.; Agius, M.; Phillips, J.S. Suicidal ideation in people with tinnitus: A systematic review and meta-analysis. J. Laryngol. Otol. 2021, 135, 1042–1050. [Google Scholar] [CrossRef]
- Fox-Thomas, L.G. Suicidal ideation among patients with chronic tinnitus. Hear. J. 2016, 69, 10. [Google Scholar] [CrossRef]
- Aazh, H.; Landgrebe, M.; Danesh, A.A. Parental mental illness in childhood as a risk factor for suicidal and self-harm ideations in adults seeking help for tinnitus and/or hyperacusis. Am. J. Audiol. 2019, 28, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Peng, Z.; Yu, S.; Song, Q.L.; Qu, T.F.; He, L.; Liu, K.; Gong, S.S. Loss of Cochlear Ribbon Synapse Is a Critical Contributor to Chronic Salicylate Sodium Treatment-Induced Tinnitus without Change Hearing Threshold. Neural. Plast. 2020, 2020, 3949161. [Google Scholar] [CrossRef] [PubMed]
- Liberman, M.C.; Kujawa, S.G. Cochlear Synaptopathy in Acquired Sensorineural Hearing Loss: Manifestations and Mechanisms. Hear. Res. 2017, 349, 138–147. [Google Scholar] [CrossRef] [PubMed]
- Jastreboff, P.J.; Hazell, J.W. A Neurophysiological Approach to Tinnitus: Clinical Implications. Br. J. Audiol. 1993, 27, 7–17. [Google Scholar] [CrossRef]
- Kalappa, B.I.; Brozoski, T.J.; Turner, J.G.; Caspary, D.M. Single Unit Hyperactivity and Bursting in the Auditory Thalamus of Awake Rats Directly Correlates with Behavioural Evidence of Tinnitus. J. Physiol. 2014, 592, 5065–5078. [Google Scholar] [CrossRef] [Green Version]
- Piccirillo, J.F.; Rodebaugh, T.L.; Lenze, E.J. Tinnitus. JAMA 2020, 323, 1497–1498. [Google Scholar] [CrossRef]
- Leaver, A.M.; Renier, L.; Chevillet, M.A.; Morgan, S.; Kim, H.J.; Rauschecker, J.P. Dysregulation of Limbic and Auditory Networks in Tinnitus. Neuron 2011, 69, 33–43. [Google Scholar] [CrossRef] [Green Version]
- Rauschecker, J.P.; Leaver, A.M.; Muhlau, M. Tuning out the Noise: Limbic-Auditory Interactions in Tinnitus. Neuron 2010, 66, 819–826. [Google Scholar] [CrossRef] [Green Version]
- Jackson, P. A Comparison of the Effects of Eighth Nerve Section with Lidocaine on Tinnitus. J. Laryngol. Otol. 1985, 99, 663–666. [Google Scholar] [CrossRef]
- Norena, A.J. An Integrative Model of Tinnitus Based on a Central Gain Controlling Neural Sensitivity. Neurosci. Biobehav. Rev. 2011, 35, 1089–1109. [Google Scholar] [CrossRef]
- Sheppard, A.; Stocking, C.; Ralli, M.; Salvi, R. A Review of Auditory Gain, Low-Level Noise and Sound Therapy for Tinnitus and Hyperacusis. Int. J. Audiol. 2020, 59, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Besteher, B.; Gaser, C.; Ivansic, D.; Guntinas-Lichius, O.; Dobel, C.; Nenadic, I. Chronic Tinnitus and the Limbic System: Reappraising Brain Structural Effects of Distress and Affective Symptoms. Neuroimage Clin. 2019, 24, 101976. [Google Scholar] [CrossRef] [PubMed]
- Kleinjung, T.; Langguth, B. Avenue for Future Tinnitus Treatments. Otolaryngol. Clin. N. Am. 2020, 53, 667–683. [Google Scholar] [CrossRef]
- Langguth, B.; Elgoyhen, A.B.; Cederroth, C.R. Therapeutic Approaches to the Treatment of Tinnitus. Annu. Rev. Pharmacol. Toxicol. 2019, 59, 291–313. [Google Scholar] [CrossRef]
- Andersson, G. Clinician-Supported Internet-Delivered Psychological Treatment of Tinnitus. Am. J. Audiol. 2015, 24, 299–301. [Google Scholar] [CrossRef]
- Sereda, M.; Xia, J.; El Refaie, A.; Hall, D.A.; Hoare, D.J. Sound Therapy (Using Amplification Devices and/or Sound Generators) for Tinnitus. Cochrane Database Syst. Rev. 2018, 12, CD013094. [Google Scholar] [PubMed]
- Pienkowski, M. Rationale and Efficacy of Sound Therapies for Tinnitus and Hyperacusis. Neuroscience 2019, 407, 120–134. [Google Scholar] [CrossRef]
- Ogata, Y.; Sekitani, T.; Moriya, K.; Watanabe, K. Biofeedback Therapy in the Treatment of Tinnitus. Auris Nasus Larynx 1993, 20, 95–101. [Google Scholar] [CrossRef]
- Vernon, J.A.; Meikle, M.B. Masking Devices and Alprazolam Treatment for Tinnitus. Otolaryngol. Clin. N. Am. 2003, 36, 307–320. [Google Scholar] [CrossRef]
- Karaaslan, O.; Kantekin, Y.; Hacimusalar, Y.; Dagistan, H. Anxiety Sensitivities, Anxiety and Depression Levels, and Personality Traits of Patients with Chronic Subjective Tinnitus: A Case-Control Study. Int. J. Psychiatry Clin. Pract. 2020, 24, 264–269. [Google Scholar] [CrossRef]
- Van Munster, J.J.; van der Valk, W.H.; Stegeman, I.; Lieftink, A.F.; Smit, A.L. The Relationship of Tinnitus Distress with Personality Traits: A Systematic Review. Front. Neurol. 2020, 11, 225. [Google Scholar] [CrossRef] [PubMed]
- Waechter, S. Association between Hearing Status and Tinnitus Distress. Acta Otolaryngol. 2021, 141, 381–385. [Google Scholar] [CrossRef]
- Bhatt, J.M.; Bhattacharyya, N.; Lin, H.W. Relationships between Tinnitus and the Prevalence of Anxiety and Depression. Laryngoscope 2017, 127, 466–469. [Google Scholar] [CrossRef] [Green Version]
- Belli, S.; Belli, H.; Bahcebasi, T.; Ozcetin, A.; Alpay, E.; Ertem, U. Assessment of Psychopathological Aspects and Psychiatric Comorbidities in Patients Affected by Tinnitus. Eur. Arch. Otorhinolaryngol. 2008, 265, 279–285. [Google Scholar] [CrossRef]
- Budd, R.J.; Pugh, R. The Relationship between Locus of Control, Tinnitus Severity, and Emotional Distress in a Group of Tinnitus Sufferers. J. Psychosom. Res. 1995, 39, 1015–1018. [Google Scholar] [CrossRef]
- Hebert, S.; Canlon, B.; Hasson, D.; Hanson, L.L.M.; Westerlund, H.; Theorell, T. Tinnitus Severity Is Reduced with Reduction of Depressive Mood—A Prospective Population Study in Sweden. PLoS ONE 2012, 7, e37733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pattyn, T.; Van Den Eede, F.; Vanneste, S.; Cassiers, L.; Veltman, D.J.; Van De Heyning, P.; Sabbe, B.C.G. Tinnitus and Anxiety Disorders: A Review. Hear. Res. 2016, 333, 255–265. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, N.C.; Newman, M.G. Anxiety and Depression as Bidirectional Risk Factors for One Another: A Meta-Analysis of Longitudinal Studies. Psychol. Bull. 2017, 143, 1155–1200. [Google Scholar] [CrossRef]
- Lamers, F.; van Oppen, P.; Comijs, H.C.; Smit, J.H.; Spinhoven, P.; van Balkom, A.J.; Nolen, W.A.; Zitman, F.G.; Beekman, A.T.; Penninx, B.W. Comorbidity Patterns of Anxiety and Depressive Disorders in a Large Cohort Study: The Netherlands Study of Depression and Anxiety (Nesda). J. Clin. Psychiatry 2011, 72, 341–348. [Google Scholar] [CrossRef]
- Wittchen, H.U.; Kessler, R.C.; Pfister, H.; Lieb, M. Why Do People with Anxiety Disorders Become Depressed? A Prospective-Longitudinal Community Study. Acta Psychiatr. Scand. 2000, 102, 14–23. [Google Scholar] [CrossRef]
- Galderisi, S.; Rucci, P.; Kirkpatrick, B.; Mucci, A.; Gibertoni, D.; Rocca, P.; Rossi, A.; Bertolino, A.; Strauss, G.P.; Aguglia, E.; et al. Interplay among Psychopathologic Variables, Personal Resources, Context-Related Factors, and Real-Life Functioning in Individuals with Schizophrenia: A Network Analysis. JAMA Psychiatry 2018, 75, 396–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beard, C.; Millner, A.J.; Forgeard, M.J.; Fried, E.I.; Hsu, K.J.; Treadway, M.T.; Leonard, C.V.; Kertz, S.J.; Bjorgvinsson, T. Network Analysis of Depression and Anxiety Symptom Relationships in a Psychiatric Sample. Psychol. Med. 2016, 46, 3359–3369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boccaletti, S.; Bianconi, G.; Criado, R.; Del Genio, C.I.; Gomez-Gardenes, J.; Romance, M.; Sendina-Nadal, I.; Wang, Z.; Zanin, M. The Structure and Dynamics of Multilayer Networks. Phys. Rep. 2014, 544, 1–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borsboom, D. A Network Theory of Mental Disorders. World Psychiatry 2017, 16, 5–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cramer, A.O.J.; Waldorp, L.J.; van der Maas, H.L.J.; Borsboom, D. Complex Realities Require Complex Theories: Refining and Extending the Network Approach to Mental Disorders. Behav. Brain Sci. 2010, 33, 178–193. [Google Scholar] [CrossRef]
- Lucchesi, C.; Baldacci, F.; Cafalli, M.; Dini, E.; Giampietri, L.; Siciliano, G.; Gori, S. Fatigue, Sleep-Wake Pattern, Depressive and Anxiety Symptoms and Body-Mass Index: Analysis in a Sample of Episodic and Chronic Migraine Patients. Neurol. Sci. 2016, 37, 987–989. [Google Scholar] [CrossRef]
- Kroenke, K.; RSpitzer, L.; Williams, J.B.; Lowe, B. The Patient Health Questionnaire Somatic, Anxiety, and Depressive Symptom Scales: A Systematic Review. Gen. Hosp. Psychiatry 2010, 32, 345–359. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The Phq-9: Validity of a Brief Depression Severity Measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.; Monahan, P.O.; Lowe, B. Anxiety Disorders in Primary Care: Prevalence, Impairment, Comorbidity, and Detection. Ann. Intern. Med. 2007, 146, 317–325. [Google Scholar] [CrossRef]
- Epskamp, S.; Waldorp, L.J.; Mottus, R.; Borsboom, D. The Gaussian Graphical Model in Cross-Sectional and Time-Series Data. Multivar. Behav. Res. 2018, 53, 453–480. [Google Scholar] [CrossRef] [Green Version]
- Epskamp, S.; Fried, E.I. A Tutorial on Regularized Partial Correlation Networks. Psychol. Methods 2018, 23, 617–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedman, J.; Hastie, T.; Tibshirani, R. Sparse Inverse Covariance Estimation with the Graphical Lasso. Biostatistics 2008, 9, 432–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.H.; Chen, Z.H. Extended Bayesian Information Criteria for Model Selection with Large Model Spaces. Biometrika 2008, 95, 759–771. [Google Scholar] [CrossRef] [Green Version]
- Fruchterman, T.M.J.; Reingold, E.M. Graph Drawing by Force-Directed Placement. Software Pract. Exper. 1991, 21, 1129–1164. [Google Scholar] [CrossRef]
- Epskamp, S.; Cramer, A.O.J.; Waldorp, L.J.; Schmittmann, V.D.; Borsboom, D. Qgraph: Network Visualizations of Relationships in Psychometric Data. J. Stat. Softw. 2012, 48, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Jones, P.J.; Ma, R.; McNally, R.J. Bridge Centrality: A Network Approach to Understanding Comorbidity. Multivar. Behav. Res. 2021, 56, 353–367. [Google Scholar] [CrossRef] [PubMed]
- Haslbeck, J.M.B.; Fried, E.I. How predictable are symptoms in psychopathological networks? A reanalysis of 18 published datasets. Psychol. Med. 2017, 47, 2767–2776. [Google Scholar] [CrossRef] [Green Version]
- Epskamp, S.; Borsboom, D.; Fried, E.I. Estimating Psychological Networks and Their Accuracy: A Tutorial Paper. Behav. Res. Methods 2018, 50, 195–212. [Google Scholar] [CrossRef] [Green Version]
- Ren, L.; Wang, Y.; Wu, L.; Wei, Z.; Cui, L.B.; Wei, X.; Hu, X.; Peng, J.; Jin, Y.; Li, F.; et al. Network structure of depression and anxiety symptoms in Chinese female nursing students. BMC Psychiatry 2021, 21, 279. [Google Scholar] [CrossRef]
- Groen, R.N.; Ryan, O.; Wigman, J.T.W.; Riese, H.; Penninx, B.W.J.H.; Giltay, E.J.; Wichers, M.; Hartman, C.A. Comorbidity between Depression and Anxiety: Assessing the Role of Bridge Mental States in Dynamic Psychological Networks. BMC Med. 2020, 18, 308. [Google Scholar] [CrossRef]
- Everaert, J.; Joormann, J. Emotion Regulation Difficulties Related to Depression and Anxiety: A Network Approach to Model Relations among Symptoms, Positive Reappraisal, and Repetitive Negative Thinking. Clin. Psychol. Sci. 2019, 7, 1304–1318. [Google Scholar] [CrossRef] [Green Version]
- McElroy, E.; Fearon, P.; Belsky, J.; Fonagy, P.; Patalay, P. Networks of Depression and Anxiety Symptoms across Development. J. Am. Acad. Child Adolesc. Psychiatry 2018, 57, 964–973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dobson, E.T.; Croarkin, P.E.; Schroeder, H.K.; Varney, S.T.; Mossman, S.A.; Cecil, K.; Strawn, J.R. Bridging Anxiety and Depression: A Network Approach in Anxious Adolescents. J. Affect. Disord. 2021, 280 Pt A, 305–314. [Google Scholar] [CrossRef]
- Park, S.C.; Kim, D. The Centrality of Depression and Anxiety Symptoms in Major Depressive Disorder Determined Using a Network Analysis. J. Affect. Disord. 2020, 271, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Natalini, E.; Fioretti, A.; Riedl, D.; Moschen, R.; Eibenstein, A. Tinnitus and Metacognitive Beliefs-Results of a Cross-Sectional Observational Study. Brain Sci. 2020, 11, 3. [Google Scholar] [CrossRef] [PubMed]
- Moritz, S.; Klein, J.P.; Lysaker, P.H.; Mehl, S. Metacognitive and Cognitive-Behavioral Interventions for Psychosis: New Developments. Dialogues Clin. Neurosci. 2019, 21, 309–317. [Google Scholar] [CrossRef]
- McEvoy, P.M. Metacognitive Therapy for Anxiety Disorders: A Review of Recent Advances and Future Research Directions. Curr. Psychiatry Rep. 2019, 21, 29. [Google Scholar] [CrossRef]
- Solem, S.; Wells, A.; Kennair, L.E.O.; Hagen, R.; Nordahl, H.; Hjemdal, O. Metacognitive Therapy Versus Cognitive-Behavioral Therapy in Adults with Generalized Anxiety Disorder: A 9-Year Follow-up Study. Brain Behav. 2021, 11, e32358. [Google Scholar] [CrossRef]
- Ferraro, L.; La Barbera, D.; Messina, A.; Galioto, S.; Marinaro, A.M.; Caruso, C.; Rizzo, R.; La Cascia, C. Metacognitive Therapy in Patients with Tinnitus: A Single Group Study. J. Contemp. Psychother. 2019, 49, 133–140. [Google Scholar] [CrossRef]
- Ost, L.G. Applied Relaxation: Description of a Coping Technique and Review of Controlled Studies. Behav. Res. Ther. 1987, 25, 397–409. [Google Scholar] [CrossRef]
- Kreuzer, P.M.; Goetz, M.; Holl, M.; Schecklmann, M.; Landgrebe, M.; Staudinger, S.; Langguth, B. Mindfulness-and Body-Psychotherapy-Based Group Treatment of Chronic Tinnitus: A Randomized Controlled Pilot Study. BMC Complement. Altern. Med. 2012, 12, 235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arif, M.; Sadlier, M.; Rajenderkumar, D.; James, J.; Tahir, T. A Randomised Controlled Study of Mindfulness Meditation Versus Relaxation Therapy in the Management of Tinnitus. J. Laryngol. Otol. 2017, 131, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Philippot, P.; Nef, F.; Clauw, L.; de Romree, M.; Segal, Z. A Randomized Controlled Trial of Mindfulness-Based Cognitive Therapy for Treating Tinnitus. Clin. Psychol. Psychother. 2012, 19, 411–419. [Google Scholar] [CrossRef]
- Heinecke, K.; Weise, C.; Rief, W. Psychophysiological Effects of Biofeedback Treatment in Tinnitus Sufferers. Br. J. Clin. Psychol. 2009, 48 Pt 3, 223–239. [Google Scholar] [CrossRef]
- Fuller, T.; Cima, R.; Langguth, B.; Mazurek, B.; Vlaeyen, J.W.; Hoare, D.J. Cognitive Behavioural Therapy for Tinnitus. Cochrane Database Syst. Rev. 2020, 1, CD012614. [Google Scholar] [CrossRef] [PubMed]
- Cima, R.F.; Maes, I.H.; Joore, M.A.; Scheyen, D.J.; El Refaie, A.; Baguley, D.M.; Anteunis, L.J.; van Breukelen, G.J.; Vlaeyen, J.W. Specialised Treatment Based on Cognitive Behaviour Therapy versus Usual Care for Tinnitus: A Randomised Controlled Trial. Lancet 2012, 379, 1951–1959. [Google Scholar] [CrossRef] [PubMed]
- Hesser, H.; Weise, C.; Westin, V.Z.; Andersson, G. A Systematic Review and Meta-Analysis of Randomized Controlled Trials of Cognitive-Behavioral Therapy for Tinnitus Distress. Clin. Psychol. Rev. 2011, 31, 545–553. [Google Scholar] [CrossRef]
- Yuan, T.; Yadollahpour, A.; Salgado-Ramirez, J.; Robles-Camarillo, D.; Ortega-Palacios, R. Transcranial Direct Current Stimulation for the Treatment of Tinnitus: A Review of Clinical Trials and Mechanisms of Action. BMC Neurosci. 2018, 19, 66. [Google Scholar] [CrossRef] [Green Version]
- Schwippel, T.; Schroeder, P.A.; Fallgatter, A.J.; Plewnia, C. Clinical Review: The Therapeutic Use of Theta-Burst Stimulation in Mental Disorders and Tinnitus. Prog. Neuropsychopharmacol. Biol. Psychiatry 2019, 92, 285–300. [Google Scholar] [CrossRef]
- Aazh, H.; Moore, B.C.J. Thoughts About Suicide and Self-Harm in Patients with Tinnitus and Hyperacusis. J. Am. Acad. Audiol. 2018, 29, 255–261. [Google Scholar] [CrossRef]
- Pridmore, S.; Walter, G.; Friedland, P. Tinnitus and Suicide: Recent Cases on the Public Record Give Cause for Reconsideration. Otolaryngol. Head Neck Surg. 2012, 147, 193–195. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.E.; Stephens, S.D.; McKenna, L. Tinnitus and Suicide. Clin. Otolaryngol. Allied Sci. 1994, 19, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.H.; Kang, J.M.; Hwang, S.H.; Han, K.D.; Joo, Y.H. Relationship between Tinnitus and Suicidal Behaviour in Korean Men and Women: A Cross-Sectional Study. Clin. Otolaryngol. 2016, 41, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Gijzen, M.W.M.; Rasing, S.P.A.; Creemers, D.H.M.; Smit, F.; Engels, R.C.M.E.; De Beurs, D. Suicide Ideation as a Symptom of Adolescent Depression. A Network Analysis. J. Affect. Disord. 2021, 278, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Hawton, K.; Casanas, I.C.C.; Haw, C.; Saunders, K. Risk Factors for Suicide in Individuals with Depression: A Systematic Review. J. Affect. Disord. 2013, 147, 17–28. [Google Scholar] [CrossRef] [PubMed]
- Sala, R.; Goldstein, B.I.; Morcillo, C.; Liu, S.M.; Castellanos, M.; Blanco, C. Course of Comorbid Anxiety Disorders among Adults with Bipolar Disorder in the U.S. Population. J. Psychiatr. Res. 2012, 46, 865–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolton, J.M.; Pagura, J.; Enns, M.W.; Grant, B.; Sareen, J. A Population-Based Longitudinal Study of Risk Factors for Suicide Attempts in Major Depressive Disorder. J. Psychiatr. Res. 2010, 44, 817–826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanley, I.H.; Boffa, J.W.; Rogers, M.L.; Hom, M.A.; Albanese, B.J.; Chu, C.; Capron, D.W.; Schmidt, N.B.; Joiner, T.E. Anxiety Sensitivity and Suicidal Ideation/Suicide Risk: A Meta-Analysis. J. Consult. Clin. Psychol. 2018, 86, 946–960. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, A.; Gendron, A.; McIntyre, A. Quetiapine Adjunct to Selective Serotonin Reuptake Inhibitors or Venlafaxine in Patients with Major Depression, Comorbid Anxiety, and Residual Depressive Symptoms: A Randomized, Placebo-Controlled Pilot Study. Depress. Anxiety 2007, 24, 487–494. [Google Scholar] [CrossRef] [PubMed]
- Hirschfeld, R.M.; Weisler, R.H.; Raines, S.R.; Macfadden, W.; Bolder Study Group. Quetiapine in the Treatment of Anxiety in Patients with Bipolar I or Ii Depression: A Secondary Analysis from a Randomized, Double-Blind, Placebo-Controlled Study. J. Clin. Psychiatry 2006, 67, 355–362. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Mean | SD |
|---|---|---|
| Age | 44.74 | 14.33 |
| Number | Percentage | |
| Gender | ||
| Male | 284 | 50.18% |
| Female | 282 | 49.82% |
| Education | ||
| Junior high school and below | 107 | 18.90% |
| Senior high school or technical secondary school | 107 | 18.90% |
| Junior college | 114 | 20.14% |
| Undergraduate | 179 | 31.63% |
| Master | 51 | 9.01% |
| Doctor | 8 | 1.41% |
| Duration of tinnitus | ||
| <3 months | 202 | 35.69% |
| 3–6 months | 63 | 11.13% |
| 6–12 months | 71 | 12.54% |
| >12 months | 230 | 40.64% |
| Family history | ||
| Yes | 90 | 15.90% |
| No | 476 | 84.10% |
| Tinnitus perception at onset | ||
| Gradual | 177 | 31.27% |
| Abrupt | 389 | 68.73% |
| Tinnitus location | ||
| Right ear | 166 | 29.33% |
| Left ear | 177 | 31.27% |
| Both ears | 209 | 36.93% |
| Inside the head | 14 | 2.47% |
| Tinnitus manifestation | ||
| Intermittent | 121 | 21.38% |
| Constant | 445 | 78.62% |
| Visual analog scale (VAS) score | ||
| Minimal symptoms (range = 0–3) | 186 | 32.86% |
| Mild symptoms (range = 4–6) | 217 | 38.34% |
| Severe symptoms (range = 7–10) | 163 | 28.80% |
| Depression symptoms (PHQ-9) | ||
| Minimal symptoms (range = 0–4) | 241 | 42.58% |
| Mild symptoms (range = 5–9) | 164 | 28.96% |
| Moderate symptoms (range = 10–14) | 102 | 18.02% |
| Moderately severe symptoms (range = 15–19) | 39 | 6.89% |
| Severe symptoms (range = 20–27) | 20 | 3.53% |
| Anxiety symptoms (GAD-7) | ||
| Minimal symptoms (range = 0–4) | 288 | 50.88% |
| Mild symptoms (range = 5–9) | 169 | 29.86% |
| Moderate symptoms (range = 10–14) | 68 | 12.01% |
| Severe symptoms (range = 15–21) | 41 | 7.24% |
| Symptoms | Mean | SD | Predictability |
|---|---|---|---|
| Depression symptoms (PHQ-9) | 6.83 | 5.65 | |
| PHQ-1: Anhedonia (D1) | 0.99 | 1.01 | 0.53 |
| PHQ-2: Feeling depressed or hopeless (D2) | 0.84 | 0.94 | 0.59 |
| PHQ-3: Sleep problems (D3) | 1.2 | 1.05 | 0.32 |
| PHQ-4: Energy loss (D4) | 1.15 | 1.03 | 0.43 |
| PHQ-5: Appetite changes (D5) | 0.58 | 0.83 | 0.36 |
| PHQ-6: Feeling of worthlessness (D6) | 0.55 | 0.82 | 0.57 |
| PHQ-7: Trouble concentrating (D7) | 0.78 | 0.92 | 0.53 |
| PHQ-8: Psychomotor issues (D8) | 0.56 | 0.82 | 0.45 |
| PHQ-9: Suicidal ideation (D9) | 0.18 | 0.47 | 0.41 |
| Anxiety symptoms (GAD-7) | 5.52 | 5.12 | |
| GAD-1: Feeling nervous or anxious (A1) | 0.94 | 0.91 | 0.57 |
| GAD-2: Unable to control worry (A2) | 0.77 | 0.90 | 0.70 |
| GAD-3: Excessive worry (A3) | 0.95 | 0.95 | 0.58 |
| GAD-4: Relaxation difficulty (A4) | 0.89 | 0.94 | 0.66 |
| GAD-5: Too restless to sit still (A5) | 0.52 | 0.80 | 0.57 |
| GAD-6: Easily annoyed or irritable (A6) | 0.97 | 0.94 | 0.57 |
| GAD-7: Afraid something awful might happen (A7) | 0.48 | 0.76 | 0.59 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, X.; Ren, L.; Xue, X.; Yu, N.; Liu, P.; Shen, W.; Zhou, H.; Wang, B.; Zhou, J.; Yang, S.; et al. The Comorbidity of Depression and Anxiety Symptoms in Tinnitus Sufferers: A Network Analysis. Brain Sci. 2023, 13, 583. https://doi.org/10.3390/brainsci13040583
Chen X, Ren L, Xue X, Yu N, Liu P, Shen W, Zhou H, Wang B, Zhou J, Yang S, et al. The Comorbidity of Depression and Anxiety Symptoms in Tinnitus Sufferers: A Network Analysis. Brain Sciences. 2023; 13(4):583. https://doi.org/10.3390/brainsci13040583
Chicago/Turabian StyleChen, Xuemin, Lei Ren, Xinmiao Xue, Ning Yu, Peng Liu, Weidong Shen, Hanwen Zhou, Ben Wang, Jingcheng Zhou, Shiming Yang, and et al. 2023. "The Comorbidity of Depression and Anxiety Symptoms in Tinnitus Sufferers: A Network Analysis" Brain Sciences 13, no. 4: 583. https://doi.org/10.3390/brainsci13040583